
Abstract
Background:
Mandibular osteoradionecrosis (ORN) is a devastating complication of radiotherapy for oropharyngeal malignancy. Despite advancements in ORN treatment, risk of ORN recurrence remains high following surgical resection. Virtual surgical planning (VSP) for ORN treatment is an evolving application that may not only inform bony reconstruction but also therapeutic surgical margins, which remain inconclusively defined in the literature.
Methods:
A retrospective review was performed of 25 cases in which patients underwent VSP-guided resection of mandibular ORN followed by immediate free fibula flap reconstruction. Surgical margins of 1-cm from radiologically evident disease were taken. VSP accuracy was quantified by comparing measured anatomic parameters between the virtually planned outcomes and the final outcomes on postoperative imaging. Statistical analyses were performed to assess associations between preoperative factors and postoperative complications including ORN recurrence.
Results:
The mandibular body was most frequently affected by ORN in this series of patients. Among risk factors, only the presence of a preoperative orocutaneous fistula was predictive of a complication, specifically partial flap failure (β = 1.41; P = .013). Intended anatomic parameters were achieved with the exception of the intergonial distance (x difference = 0.53 cm; P = .03). Finally, there were no cases of ORN recurrence after a mean follow-up of 27.4 months.
Conclusions:
VSP of free fibula flaps for mandibular reconstruction following ORN is a valid tool for effecting accurate anatomical outcomes. Furthermore, we demonstrate that a 1-cm margin around radiographically evident ORN may effectively implement a curative outcome free from relapse.
Keywords
Introduction
Mandibular osteoradionecrosis (ORN) can be a devastating complication of radiotherapy for oropharyngeal malignancy. Despite the lack of unified diagnostic criteria, ORN is characterized as radiation-induced ischemic destruction of the bone that fails to heal over a set time period, typically 3 months, in the absence of a persistent tumor.1-8 Difficult to detect both clinically and radiographically in its early stage, ORN is a pernicious process that starts asymptomatically but may progress to substantial patient morbidity.8-10 Sequalae of ORN include severe pain, trismus, infection, fistulae, fractures, and ultimately facial collapse and deformation.11,12 While conservative and medical therapy may be sufficient for treatment of mild cases, progressive ORN often requires surgical debridement or resection of the affected bone prior to free tissue transfer for bone and soft tissue reconstruction. In recent years, advancements in targeted radiation therapy for head and neck cancers have limited the incidence of ORN. 13 However, with a frequently cited incidence of 5 to 15%, mandibular ORN remains a calamitous consequence of treating these tumors.8,14
Several staging systems of ORN have been described, each based on various criteria such as responses to hyperbaric oxygen therapy, degree of bone damage, clinical-radiological findings, duration of bone exposure, and treatment required.1,10,11,15-23 However, these systems have not led to significant reduction of residual disease following initial resection of affected bone, which has been reported to range from 11 to 53%.7,12,23-26 Persistent disease can be attributed to insufficient debridement; however, an evidence-based margin of resection that effectively prevents residual disease has not been established.26-29
Obwegeser and Sailer 30 were among the first to advise debridement to punctuate bleeding, a strategy used to the present day. Some recent authors have advocated for more extensive resection of all visibly-affected tissue. 31 However, florescence analysis of apparently healthy, bleeding bone has shown histopathology consistent with ORN. 27 Likewise, negative margins of resected specimens have been found to poorly correlate with resolution of ORN. 26 Therefore, a simple resection guided by visual examination may be inadequate to provide a wholly curative outcome, and an additional margin of healthy bone must be sacrificed to achieve this goal.
Similarly, preoperative planning for resection of ORN is challenging because imaging findings poorly correlate with disease severity.8,10,15 While ORN does present radiographically as localized extensive areas of osteolysis and sequestra, evident disease often underestimates the extent of radiation exposure to the mandible.8,10,15,32,33 A recent case series found greater than 1 cm3 of high-dose irradiated mandible left after resection with non-dosimetry virtual surgical planning (VSP) in 3 of 5 patients. 33 However, few studies present large series of patients having undergone VSP-assisted mandibular reconstruction specifically for cancer treatment-induced ORN.27-29,34
Nevertheless, VSP has become commonplace in the practice for free flap mandibular reconstruction due to demonstrated reduction in operative time, ischemia time, and improved reconstructive accuracy without differences in complication rates.34-42 To our knowledge, no studies report using this technique to implement a defined margin of resection of affected bone. As such, this study aims to (1) examine the anatomic accuracy of virtual surgical planning in fibula free flap reconstruction of the mandible for ORN, (2) identify variables associated with post-surgical morbidity in these cases, and (3) evaluate the application of a defined 1-cm surgical margin for resection of ORN using VSP.
Methods
Following institutional review board approval, a retrospective chart review was conducted of consecutive patients at our institution who underwent VSP-assisted resection of ORN followed by immediate reconstruction with a fibula free flap from August 2011 to February 2019 (Figure 1).
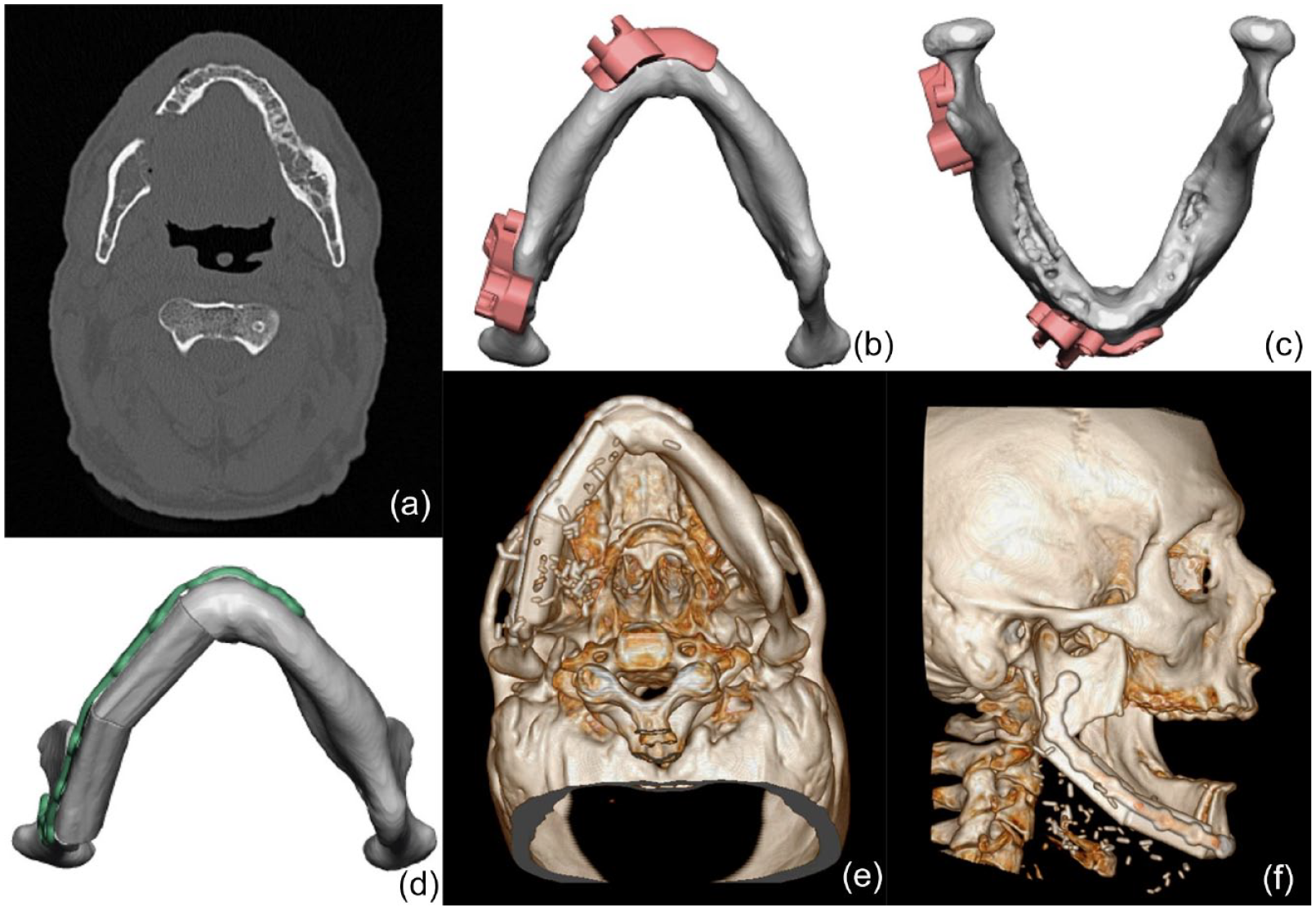
Resection and reconstruction of mandibular osteoradionecrosis using virtual surgical planning to define the margin of resection for a 47-year-old male with stage III right osteoradionecrosis (Case 11 from Table 1). (a) Axial computerized tomography scan demonstrating osteoradionecrosis of the right mandibular parasymphysis, body, and angle. (b) Inferior and (c) superior axial views of the mandible with virtually planned cutting jugs demonstrating 1-cm margins of resection based on radiographic evidence of involved bone. (d) Virtually planned reconstructive outcome. (e) Axial and (f) sagittal views of three-dimensional model demonstrating final reconstructive result.
Maxillofacial computerized tomography (CT) scans, with standard 1 mm cuts in axial, sagittal, and coronal planes, were used to perform preoperative planning. Osteotomy guides for resection of the diseased segment of bone were based on extent of evident disease plus a 1 cm margin of healthy-appearing bone. Osteotomy guides were also created for the fibula to facilitate accuracy and efficiency of the reconstruction. Lastly, preoperative planning included evaluation of risk for soft-tissue insufficiency for primary closure, indicating a need for an anterolateral thigh (ALT) or similar free flap for coverage. Study eligibility was contingent upon a minimum of 6 months of clinical follow-up.
Demographics, comorbidities, and preoperative data were extracted from electronic medical records. Of note, characteristics of radiation exposure could not be collected because most patients underwent radiotherapy at outside institutions in the remote past. Severity of ORN was classified based on radiographic appearance of the bone and evidence of soft tissue defects as described by He et al. 23 Location of disease was categorized into 8 anatomic segments: left and right ramus (including the condyle), angle, body, and symphysis/parasymphysis, respectively. Morbid features recorded on initial presentation were also extracted, including skin involvement on the face, presence of a fistula, exposed hardware, and exposed bone. Preoperative plans were characterized by 6 anatomic dimensions: anterior-posterior (AP) distance; condyle height; intergonial distance; gonial angle; condyle:AP distance ratio; and condyle:intergonial distance ratio, as measured on VSP images using open-access graphical analysis software ImageJ (Figure 2). 43
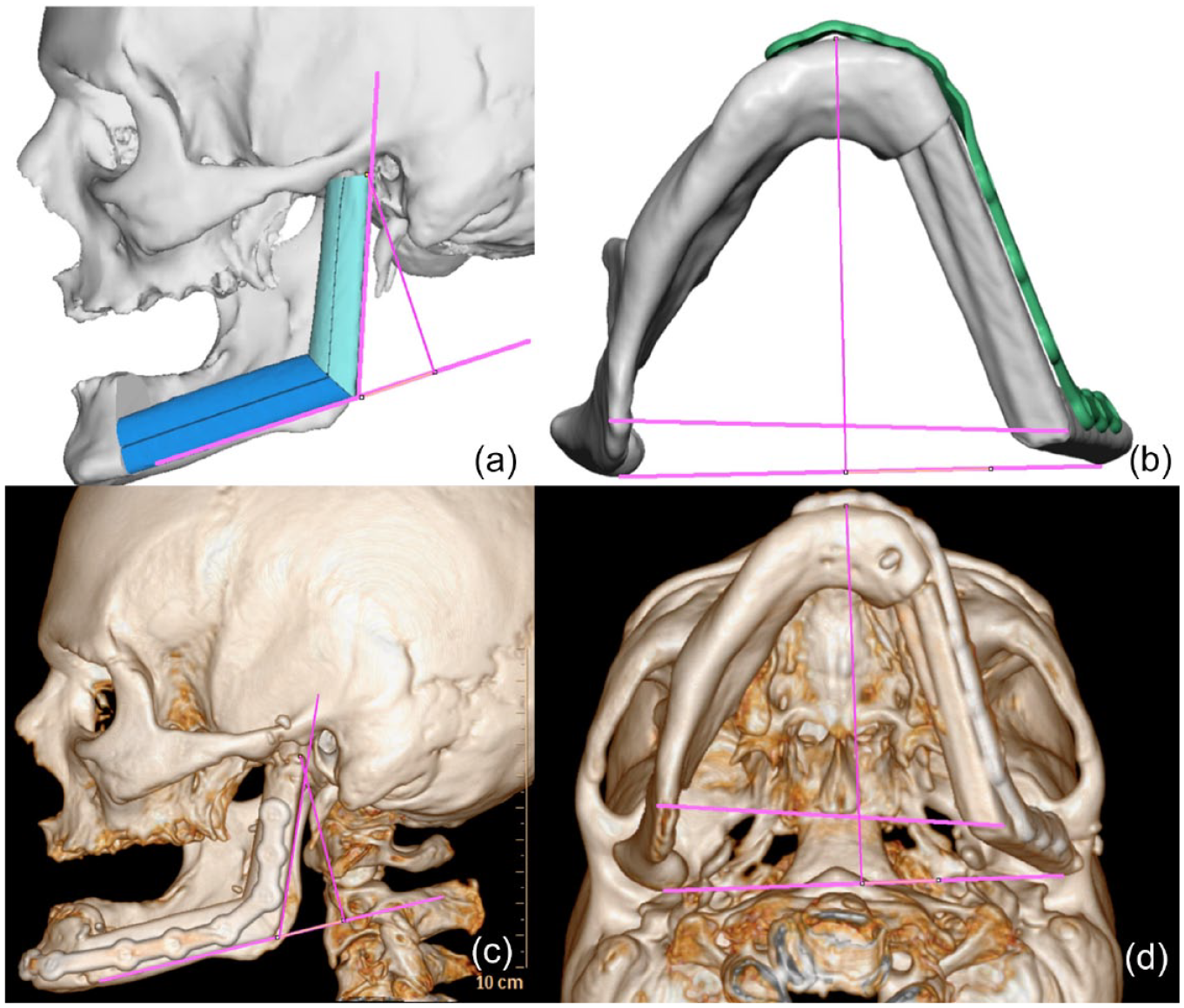
Comparison of preoperative virtual surgical planning and actual postoperative outcome of free fibula flap reconstruction of stage III osteoradionecrosis of the mandible in a 62-year-old male (Case 2 in Table 1). (a) Sagittal view of planned fibula construct. Lines representing the condyle height and gonial angle can be seen. (b) Axial view of reconstructed mandible with custom plating. The vertical line extending to the posterior (bottom) horizontal line represents the anterior-posterior distance, while the anterior (top) horizontal line represents the intergonial distance. (c) Sagittal and (d) axial views of three-dimensional model demonstrating the reconstructed mandible and collection of final anatomic measurements.
Outcome variables were chosen to evaluate accuracy of VSP and postoperative morbidity in the context of fibula free flap reconstruction of the mandible for ORN. Analogous to the preoperative planning variables, accuracy outcomes included 6 anatomical dimensions measured on CT scans in the acute postoperative period, using Horos™ 3.0 software (Horos Project, Annapolis, MD, USA) (Figure 2). Postoperative morbidity variables included partial and total flap failure as well as incidence of ORN persistence at any time during follow-up. Evaluation of recurrence or persistence of ORN postoperatively was primarily performed via thorough history taking and physical exam during clinical visits; all patients in this series were followed clinically for at least 6 months. Noncontrast maxillofacial CT was commonly performed within 1 week of surgery and served as a useful adjunct to the history and physical. However, imaging timing was not uniform and varied based on surgeon preference and the specific clinical scenario. Partial flap failure was defined as any complication leading to a return to the operating room with sub-total debridement of the free fibula flap. Total flap failure was defined as complications leading to complete removal of the free fibula flap.
Statistical Analysis
All study data was entered into a statistical database for analysis (IBM SPSS Version 23; IBM Corp., Armonk, N.Y.). T-tests were used to compare the preoperative planned anatomical measurements to those obtained postoperatively. Predictors evaluated in all regression analyses included: age, sex, hypertension, diabetes, smoking status, ORN stage, orocutaneous fistula, exposed hardware, and exposed bone. Stepwise regression analysis was used to model the final number of mandibular segments requiring resection as well as the need for an additional free flap for soft tissue coverage. Stepwise logistic regression analysis was also conducted to model occurrence of total flap failure or partial flap failure.
Results
A total of 25 patients (20 males, 80%) with mandibular reconstruction using free fibula flaps in the setting of ORN were included in this series. A total of 26 free fibula flaps are included, as 1 patient with bilateral ORN underwent staged reconstruction with individual fibula flaps on each side. The sample mean age was 59.4 (±9.8) years (range: 40-78). Five patients (21%) had hypertension; 4 (17%) had diabetes mellitus; and 16 (67%) smoked tobacco cigarettes at the time of ORN development.
All patients in the series had cancer of the head and neck region as the indication for radiation treatment. Fifteen patients had detailed pathology results available for review; the records of the other 10 patients did not specify their type of head and neck cancer. The most common malignancies encountered were squamous cell carcinoma (SCC) of the tonsil (n = 5), SCC of the floor of the mouth (n = 4), SCC of the mandible (n = 2), SCC of the tongue (n = 2), and tonsillar lymphoma (n = 1). Most patients received concurrent chemoradiation treatment, with platinum-based chemotherapy being the most commonly used. Two patients received only radiation therapy and no chemotherapy. Unfortunately, we do not have access to the specific radiation doses or treatment protocols as they were performed at outside facilities. Of the 25 patients included in the series, 13 patients had an accurate medication list at the time of ORN diagnosis and intervention. Of these 13, no patients were prescribed osteoclast inhibitors prior to or at the time of diagnosis. 10 patients underwent hyperbaric oxygen therapy for treatment of ORN with the dives performed both prior to and after mandibular resection and reconstruction.
Six patients (24%) had orocutaneous fistulas and 4 (16%) had exposed hardware on initial presentation (Table 1). Twenty-two patients (88%) were classified as having Stage III ORN, defined by radiologic evidence of pathologic fracture. The remaining 3 patients (12%) were classified as having Stage II ORN, defined by lesions with a maximal diameter of less than 2.0 cm on radiography. Eight (32%) patients had left-sided ORN, 6 (24%) right-sided ORN, and 11 (44%) bilateral ORN, although only 1 patient required staged reconstruction with individual free fibula flaps per side.
Cohort Demographics and Classification of Disease (n = 25).
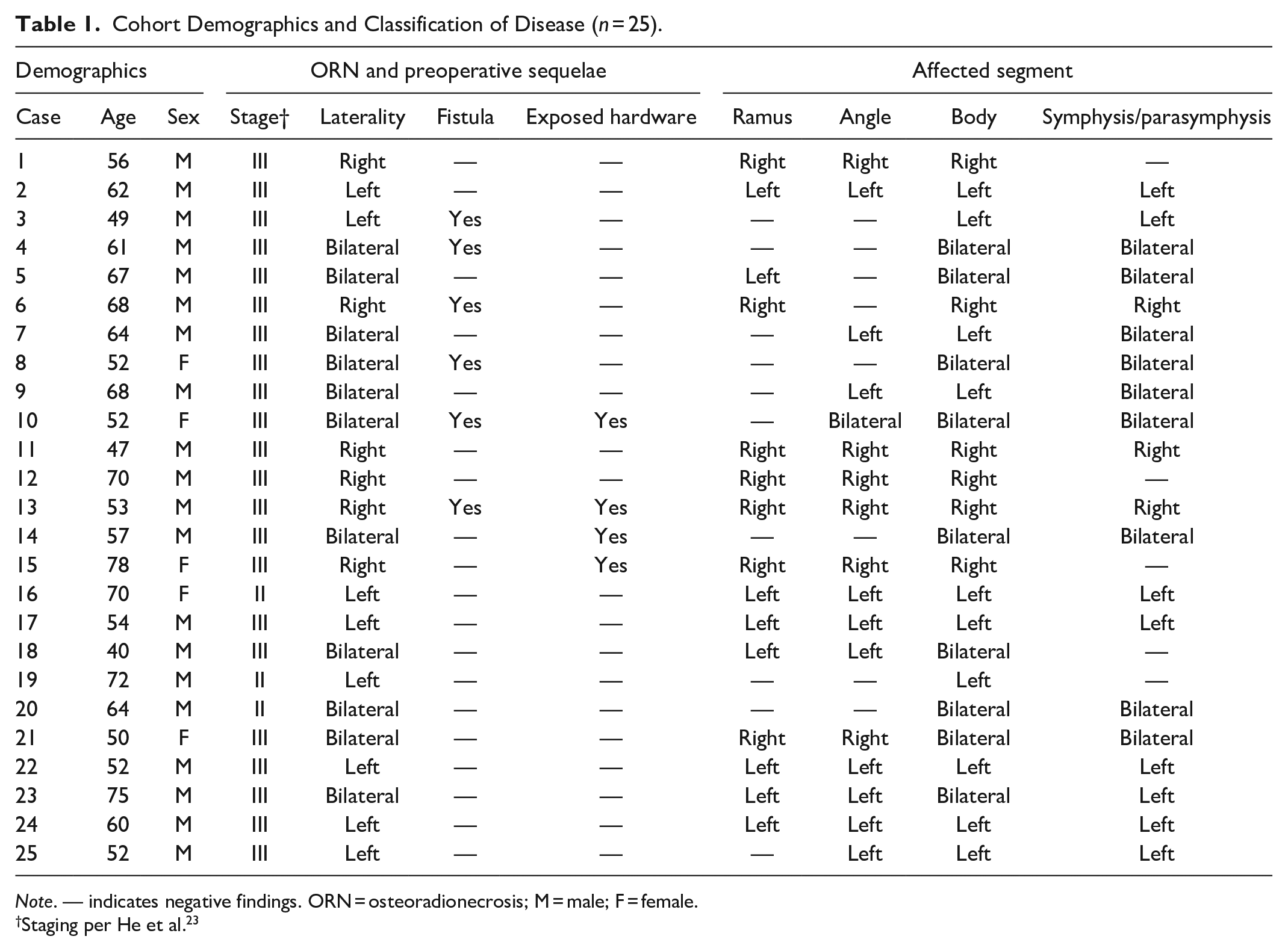
Note. — indicates negative findings. ORN = osteoradionecrosis; M = male; F = female.
Staging per He et al. 23
Without regard to laterality, the mandibular body (100%) was the most frequently affected by ORN, followed by the symphysis/parasymphysis (84%), then the angle (76%). The ramus and condyle (56%) were the least frequently affected segments. When examining these segments unilaterally, the single most affected segment was the left body (76%); the body was affected bilaterally in 9 (36%) patients. Nine patients had bilateral symphysis/parasymphysis involvement as well. Only a single patient had bilateral angle involvement, while no patients had ORN of both rami. Assessment of dentition was limited by incomplete medical records, though 4 patients were edentulous on the side of the affected mandible, 1 patient had prior extraction of 4 teeth on the affected side, and 1 patient had loose anterior incisors.
All procedures were performed by the senior authors (HSH and MWS). The mean number of resected anatomic segments per patient was 3.8 (SD = 1.0) (Table 2). The VSP-derived margins, operationalized by the osteotomy guides, resulted in healthy bleeding at the bony edges in 100% of cases. Mean clinical follow-up time was 27.4 months (SD = 24.9) (Table 2). Five partial flap failures (20%) were observed, primarily threatening overlaying ALT flaps. No instances of total flap loss were observed. No cases of persistent or recurrent ORN were observed during follow-up. No patients received dental implants concurrently with reconstruction as that was not common practice at our institution during the period studied. All patients were referred to oral maxillofacial surgery for dental implants at a later time.
Summarized Operative Characteristics and Postoperative Outcomes (n = 25).
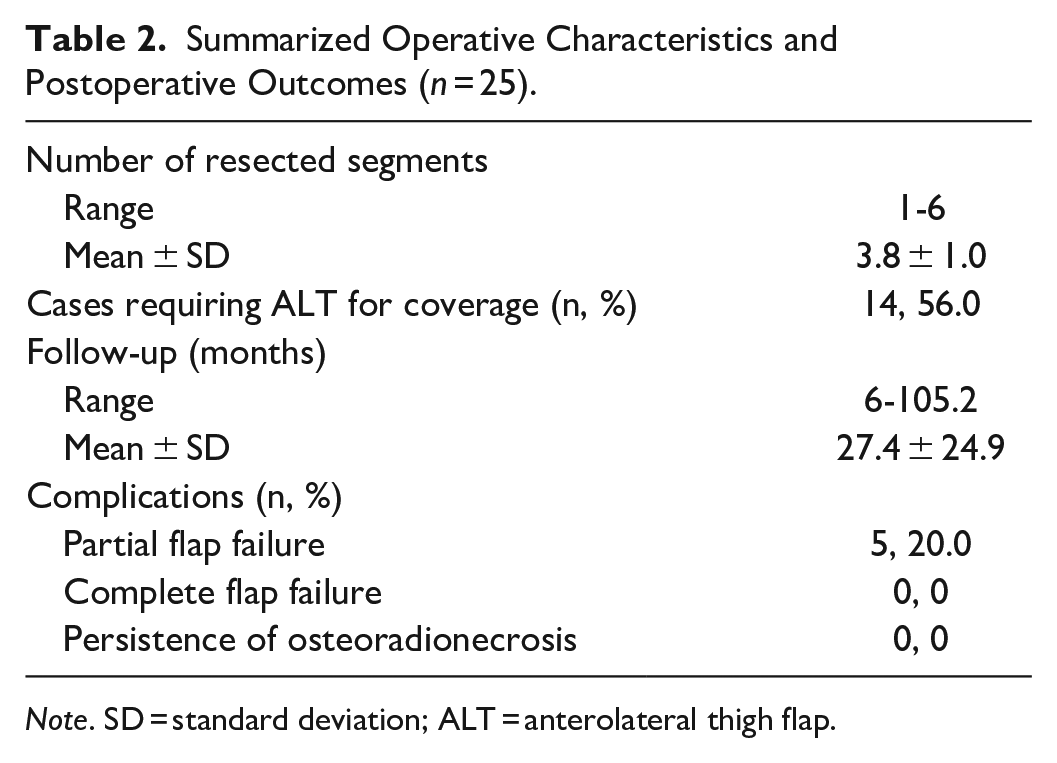
Note. SD = standard deviation; ALT = anterolateral thigh flap.
In 5 of 6 anatomic dimensions compared, the planned reconstructions and the postoperative results were not significantly different (Table 3). Only intergonial distance was statistically different (P = .03). Fourteen (56%) patients required an additional anterolateral thigh free flap for soft tissue coverage; use of ALT flap had been anticipated preoperatively in 86% of these cases. Regression analyses did not reveal any significant predictor of the number of resected segments or use of an additional flap for coverage. However, relative to the other examined factors, tobacco use trended toward statistical significance as predictor of partial flap failure (P = .06) and the need for an additional soft tissue free flap for coverage (P = .09). Upon logistic regression, partial flap failure was predicted by initial presentation of ORN with orocutaneous fistula (β = 1.41, P = .013).
Comparison of Mean Anatomic Measures of Planned Versus Postoperative Reconstructions (n = 25).
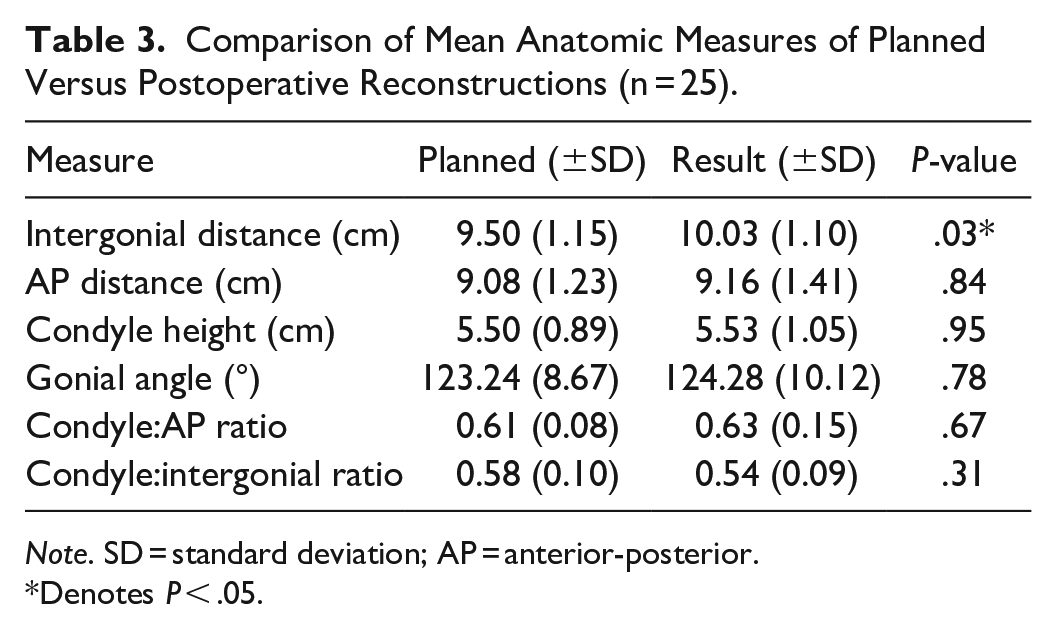
Note. SD = standard deviation; AP = anterior-posterior.
Denotes P < .05.
Discussion
VSP has become a useful tool in the reconstruction of traumatic and ablative defects of the mandible, but few reports discuss its specific utility in the treatment of mandibular ORN.39,42,44-46 Many studies of VSP-assisted mandibular reconstruction report ORN as a common surgical indication but do not exclusively investigate this population.37,45,47-57 Indeed, a recent meta-analysis found that patients with ORN tend to receive conventional reconstruction without VSP. 58 In 11 comparative studies of VSP outcomes, only 36 patients with ORN were reported.12,36,44,46,52-54,56,59-61 Nevertheless, our study corroborates the results of these limited series, findings that VSP can accurately facilitate reconstruction in ORN and predict reconstructive outcomes. Additionally, we notably observed no persistent or recurrent disease in our patients after more than 684.2 person-months of clinical follow-up. To our knowledge, our series is the largest to-date of mandibular ORN patients who underwent VSP-optimized free fibular reconstruction and the first to describe a defined margin of resection.
With a reported survival rate of 52%, incidence of oropharyngeal cancer has steadily increased over recent decades; over 47 000 new cases were reported in 2019 compared to only 29 000 in 2000. 62 Bone exposed to a radiation dosage exceeding 66 grays (Gy) is considered to be at increased risk of ORN.63,64 Although more people are being exposed to radiation for treatment of oropharyngeal cancer, the incidence of mandibular ORN has been on the decline since the 1990s. 13 This has been attributed to the advent of targeted techniques such as megavoltage, intensity-modulated, and three-dimensional conformational radiotherapies, as well as improved preventative dental care.8,19,24,63,64 It’s unfortunate, and a limitation of our study, that we do not have access to the specific radiation treatments used in our series. Other factors investigated as possible mediators in the development of ORN include poor oral hygiene, dental extractions, tumor size, tumor location, staging, and chemotherapy.8,24,64 Although the management of ORN has also evolved over this time, standard methodology remains unclear in critical areas such as the appropriate extents of conservative therapy and surgical resection.8,11,65
Although staging systems for clinical ORN are variable, there is some consensus that early stage ORN can be managed conservatively before surgery is considered.8,11,21,65 Non-surgical treatments of mandibular ORN include ensuring adequate wound care and oral hygiene, hyperbaric oxygen treatments, empiric antibiotics, vasodilatory agents such as pentoxifylline, and antioxidants such as tocopherol. 66 Although some cases may stabilize or even regress spontaneously, evidence suggests that these treatments can indeed halt disease progression.10,11 None of the patients included in this series received vasodilatory or antioxidant medications to slow the progression of ORN, though 10 patients did undergo hyperbaric oxygen treatments. Nevertheless, progression of ORN often occurs regardless of treatment, necessitating surgical debridement, sequestrectomy, or segmental mandibulectomy and reconstruction with an osseous free flap.21,65,67,68
Very few studies examine the incidence of ORN between distinct segments of the mandible.12,69 In contrast to the maxilla, the mandible is significantly more susceptible to ORN due to its restricted and localized blood supply that is often completely within the radiation field. Additionally, differences in the mandibular bone density by segment result in variable absorption of radiation during radiotherapy.8,70 Notably, the mandibular body was involved, at least unilaterally, in all patients in our cohort. As the body is positioned centrally in each mandibular hemi-segment, perhaps it is more likely to receive radiation regardless of tumor location. In a large cohort of 213 patients with ORN, Liu et al 12 similarly found the body affected in 89% patients; it was also the most likely site for ORN persistence following resection. It has previously been suggested that the symphysis might be less vulnerable than the ramus because radiation generally advances from a lateral direction.34,51 However, the ramus was the least affected in our sample, while the symphysis/parasymphysis demonstrated the second highest rate of anatomic involvement. Only 9% of Liu et al’s sample had bilateral involvement, in contrast to 44% in ours.
However, as nearly all bilateral ORN involved the bodies and/or symphysis/parasymphysis with minimal angle and ramus involvement, it was possible to reconstruct these contiguous areas with a single free fibula. Only a single patient required 2 flaps. The ability to consistently create a single construct spanning both halves of the face with a single fibula underscores the exceptional utility of VSP for these patients.
It is not surprising that VSP has found such a strong foothold in head and neck reconstruction, as there is consistent evidence that the planning technique can decrease operative times, provide for accurate reconstructions of complex three-dimensional bony defects, and take the guesswork out of osteotomies. In our study, we demonstrated the technical accuracy of VSP in the setting of reconstruction quantitatively. The postoperative results we observed were found to be highly consistent with our plans and consistent with results seen in other reported studies.38,44,71 Only the intergonial distance was found to be significantly different between the virtual plans and the postoperative anatomy. However, the average difference was found to be less than 1 mm, which is of questionable clinical significance given limited evidence of its aesthetic importance in contemporary literature. 72
While the primary goal of VSP in many cases is to design the fibula flap construct, the importance of this technique for planning the mandibulectomy should not be overlooked.27-29 By identifying the radiologic extent of the ORN during the VSP session, we can design osteotomy guides that incorporate pre-defined surgical margins. Apart from debridement to bleeding bone, few other methods have been proposed to achieve adequate margins of resection for ORN. 26 One reported alternative is the use of tetracycline bone fluorescence to intraoperatively visualize ORN and guide resection. Pre-labeling of bone with doxycycline induces fluorescence in healthy bone that has incorporated the antibiotic, while necrotic bone does not. The successful resection of ORN can then be confirmed on histopathologic analysis. 27 However, few studies have adopted this approach in larger scale trials.
Our use of VSP to guide ORN resection has notably resulted in no incidence of ORN persistence or recurrence over a mean clinical follow-up period of 27.4 months. As previously mentioned, resection to punctate bleeding is presently the predominant method of resection described in the literature7,20,25,26,30,31,53,55,67,69,73-77 and has been employed when the reconstruction is planned using VSP.34,47-50 This assumes that bleeding represents healthy tissue and therefore has a low probability of progressing to ORN. 26 However, some of these studies have reported up to a 25% persistence of ORN when employing this technique.12,25 Interestingly, 1 group has reported using VSP to ensure adequate margins for resections of both tumors and ORN. 28,29 In the first report of VSP being used to plan resection margins in ORN, radiotherapy isodose curves were converted into a 3D model. This 3D visualization was then transposed onto the 3D model of the mandible, and the resection was then planned around high-dose areas. However, a cut-off value for radiation dose was not offered, nor margins of resection defined. In contrast, here we demonstrate that a strict one-centimeter margin of radiologically healthy-appearing bone performed with VSP assistance has, to-date, resulted in resections free from persistence or recurrence for all patients included in this series.
These findings support the notion that clinically healthy appearing tissue could be harboring cellular damage that could eventually manifest as persistent ORN. As previously mentioned, Zaghi et al 26 found that histopathologic assessment at the time of surgery did not adequately predict curative resection of ORN. Instead, persistence is likely explained by the persistence of radiation-induced osteoblast, osteoclast, and myofibroblast dysfunction, as detailed in the fibroatrophic theory first proposed by Delanian et al 2 Postoperative ORN relapse has previously been found to be associated with greater radiation exposure, more advanced staging, 23 affliction of the mandibular body, and isolated sequestrestomy. 12 Given the unavoidable nature of some of these risk factors, the implementation of defined surgical margins may offer a practical clinical strategy to prevent ORN persistence following resection and reconstruction.
Our study suffers from several notable limitations. Because all mandibular ORN patients were reconstructed using VSP at our institution throughout the study period, we have no control group for comparison and thus cannot definitively attribute our outcomes to VSP. Additionally, we are prone to standard retrospective biases and, despite being the largest study of mandibular ORN patients reconstructed using VSP, still have a relatively small series size which reduces our power. A larger cohort of patients with VSP-assisted reconstructions would also facilitate subgroup analysis of pathologic features, such as fistula, which may be more or less amenable to this technique. As previously mentioned, we were unable to evaluate cumulative radiation dose and radiotherapy protocols, which have been shown to influence persistence rates and may confound our results. Another limitation is our mean clinical follow-up time of 27.4 months. Although 5 patients in our series were followed for more than 3 years, prior studies have observed a modest but significant number of ORN relapses occur as far out from reconstruction as 10 years. To address these limitations, further studies should investigate the efficacy of VSP-assisted mandibular reconstruction in ORN by: comparing outcomes to those of a control group; capturing of pertinent risk factors such as cumulative radiation dosage; and monitoring for persistence for 5 to 10 years. Future prospective studies may also consider the relative efficacy of a smaller margin compared to the 1-cm standard used here as well as alternative radiographically techniques to determine extent of disease in VSP.
Conclusion
In this series of mandibular reconstruction using free fibula flaps following ORN, VSP effectively informed extent of resection, guided flap design, and accurately predicted anatomical outcomes. The virtual plans can be confidently assumed to be adequate and realistic depictions of postoperative anatomy. Furthermore, our findings suggest that the implementation of a 1-cm margin around radiographically evident ORN may reduce persistence and recurrence.
Footnotes
Authors’ Note
Presented at: American Society for Reconstructive Microsurgery (ARSM) 2020 in Fort Lauderdale, FL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This project was approved by the local Institutional Review Board (#2405) and all policies and procedures set forth were followed throughout the duration of the study.