
Abstract
Keywords
Summary
This study is a national population-based retrospective cohort study, comparing patients aged <35 years with early-onset rectal cancer versus those aged 35–49 years.
Introduction
We read with great interest the recent article titled “Early-onset rectal cancer: Experience of a single-center, high-volume unit” by Lehtonen et al. 1 This study investigated the characteristics and outcomes of early-onset rectal cancer (EO-RC). Notably, the authors found no significant differences in survival outcomes between very young patients (<35 years) with EO-RC and those aged 35–49 years.
These findings have significant clinical value for EO-RC; however, the study has some limitations. First, the authors acknowledged that the sample size was relatively small, which constrained further subgroup analysis. Second, the study did not compare the characteristics of very young patients with those aged 35–49 years. Potential baseline differences may have influenced the outcomes. 2 Third, the study did not perform Cox regression analysis, leaving it unclear which variables were prognostic factors for EO-RC. Finally, the study only included surgically treated patients, limiting the generalizability of its conclusions to the entire EO-RC population. To address these limitations, we utilized the Surveillance, Epidemiology, and End Results (SEER) database to retrieve a large cohort and conducted a comparative analysis between very young patients with EO-RC and those aged 35–49 years.
Methods
Patients aged 18–49 years, diagnosed with RC as the only primary tumor between 2004 and 2015, were retrieved from the SEER database (Supplementary File1). SEER is the national cancer database of the United States, covering approximately 48% of the national population. 3 Cases with unknown variable information were excluded. Since SEER data are publicly available and all records are de-identified, no ethics committee approval or informed consent was required for this study.
Group comparisons were conducted using the chi-square test or Fisher’s exact test. A 1:1 propensity score matching (PSM) with a caliper of 0.10 was applied to balance baseline characteristics. Survival analysis was performed using the Kaplan–Meier and Cox regression methods. Variables with a p-value < 0.10 in the univariable COX analysis were included in the multivariable model. A p-value < 0.05 was considered statistically significant. Analyses were conducted using R version 4.3.2 (Supplementary File2).
Results
A total of 9032 patients with EO-RC were included. Significant differences in characteristics were observed between the very young and 35–49 years groups (Table 1). The very young group had a greater proportion of high histological grade tumors and a smaller proportion of stage N0 and M0 (p < 0.05). More very young patients underwent surgery, while fewer received radiotherapy and chemotherapy compared to the 35–49 years group (p < 0.05). Univariable and multivariable Cox regression analyses revealed that sex, race, histological grade, T stage, N stage, M stage, surgery, radiotherapy, and chemotherapy were independently prognostic factors for overall survival (OS) (Fig. 1A). After PSM, the baseline characteristics were well balanced. The Kaplan–Meier analysis showed that, both before and after PSM, no differences in OS were observed between these two groups (p > 0.05, Fig. 1B, C). Furthermore, subgroup analysis revealed that patients aged <35 years had comparable OS to those aged 35–49 years across all subgroups (Fig. 1D).
Characteristics of patients with early-onset rectal cancer before and after PSM, n (%).
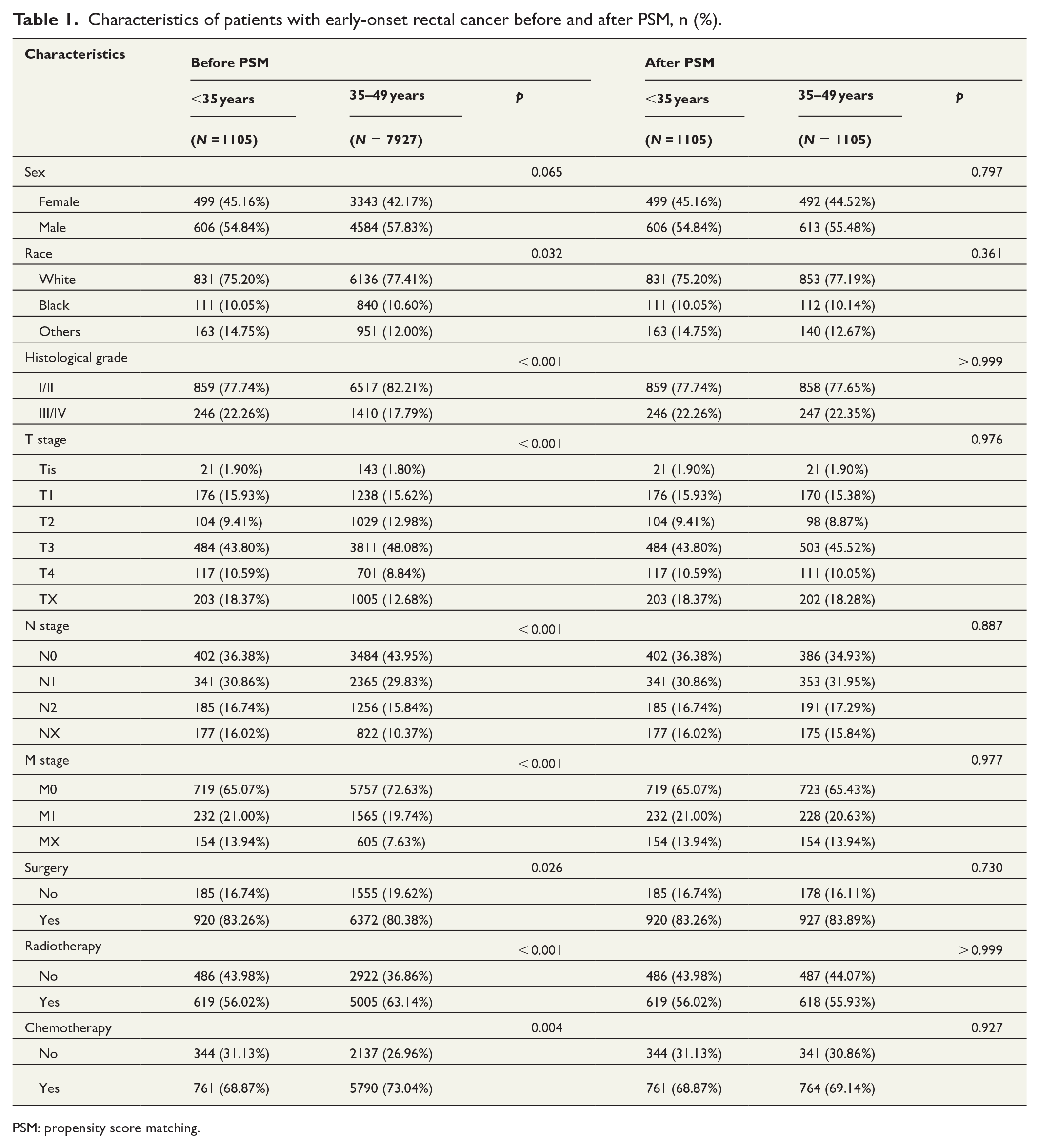
PSM: propensity score matching.
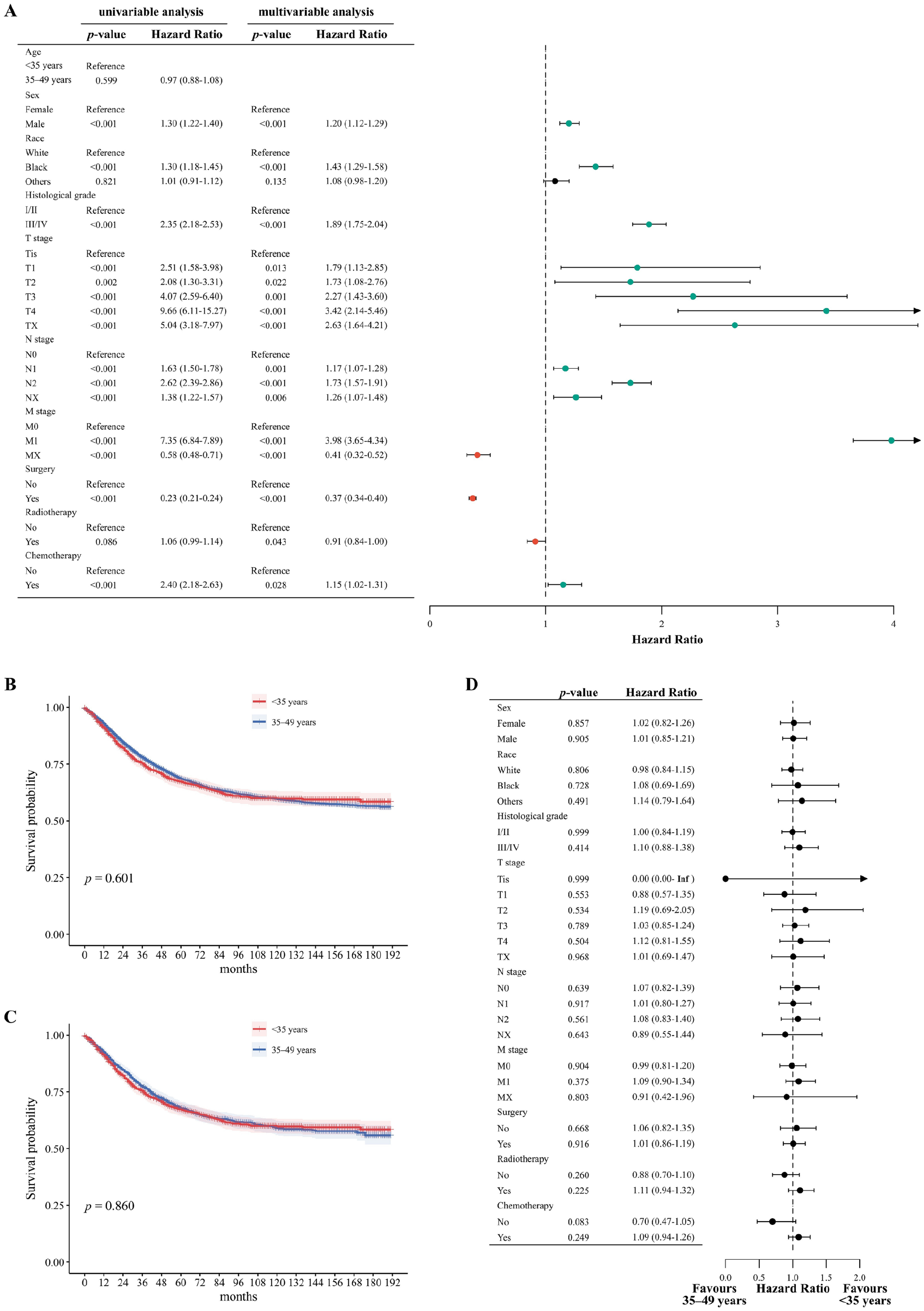
(A) Univariable and multivariable Cox regression analyses for OS in patients with EO-RC; the Kaplan–Meier curves for OS in patients with EO-RC before (B) and after (C) PSM; (D) Forest plots depicting subgroup analysis of OS between patients aged <35 years and 35–49 years.
Discussion
Before PSM, our findings revealed significant differences in clinical characteristics and treatment options between the very young and 35–49 years groups. To minimize potential confounding, we employed PSM, ensuring more reliable results. 4 Both before and after PSM, no difference in OS was observed between the two groups. Subgroup analysis further supported these results. Moreover, we explored the prognostic factors for EO-RC. The main limitation of our study was the lack of some information that was unavailable from the SEER database. 5
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251337847 – Supplemental material for Comparative analysis of early-onset rectal cancer in patients aged <35 years and 35–49 years A national population-based retrospective cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969251337847 for Comparative analysis of early-onset rectal cancer in patients aged <35 years and 35–49 years A national population-based retrospective cohort study by Qiuhan Yao and Wei-Yu Yang in Scandinavian Journal of Surgery
Supplemental Material
sj-xlsx-2-sjs-10.1177_14574969251337847 – Supplemental material for Comparative analysis of early-onset rectal cancer in patients aged <35 years and 35–49 years A national population-based retrospective cohort study
Supplemental material, sj-xlsx-2-sjs-10.1177_14574969251337847 for Comparative analysis of early-onset rectal cancer in patients aged <35 years and 35–49 years A national population-based retrospective cohort study by Qiuhan Yao and Wei-Yu Yang in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We thank the SEER database for providing valuable and public data sets.
Author contributions
Q.Y. contributed to writing the original draft. W.-Y.Y. contributed to conceptualization and edited the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent
As the SEER database is a publicly available database and all data are anonymized, patient informed consent and ethical approval were not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.