
Abstract
Background and Aims:
This study investigated patients with type B aortic dissection (TBAD) who were treated with thoracic endovascular aortic repair (TEVAR). The aim was to study whether patients who needed secondary aortic intervention (SAI) had worse survival than patients who did not require SAI after the initial TEVAR.
Methods:
Data were collected from the National Care Register for Health Care (CRHC) at the Finnish National Institute for Health and Welfare. All Patients over 15 years of age with TBAD (ICD-10; I71.01) treated with TEVAR during the years 2000–2019 were included in the study. Data were collected retrospectively. A data search of the Official Statistics of Finland Cause of Death registry was carried out to identify the date and cause of death in patients with TBAD.
Results:
236 patients with TBAD received TEVAR as primary operative treatment from year 2000 to 2019. SAI after initial TEVAR was performed in 45 (17%) patients during median follow-up time of 5.1 years. There was no significant difference in survival between the patients who underwent primary TEVAR alone and those who required additional SAI (p = 0.063). Age-adjusted survival did not differ between the groups either. Median follow-up time was significantly longer in the SAI group compared to patients with no SAI (5.9 vs 4.9 years, p = 0.047). The most common cause of death in both groups was an aortic-related event (47%).
Conclusions:
Based on this study, SAIs may not impair the overall survival of patients previously treated with TEVAR for TBAD. Systematic follow-up after the initial TEVAR may be beneficial in identifying patients with TBAD who may require secondary operation.
Context and Relevance
Thoracic endovascular aortic repair (TEVAR) has been widely adopted as the primary treatment for complicated type B aortic dissection (TBAD) based on survival benefits reported in several studies and in recent guidelines. This study aimed to identify patients with TBAD who were treated with TEVAR and needed secondary aortic intervention (SAI), and to evaluate the effect of SAIs in survival. There was no statistically significant difference in survival between the patients with or without SAIs after TEVAR. This suggests that later SAI may not worsen survival in patients who were initially treated with TEVAR for TBAD.
Introduction
TBAD is a life-threatening disease with a reported incidence of 1.6 to 6 per 100 000 inhabitants per year.1–6 TBAD represents 22% to 38% of all aortic dissections2,4 and up to 46% of all aortic dissections leading to hospital admission. 1 Risk factors for TBAD are the same as those for type A aortic dissection (TAAD), including high blood pressure, hereditary connective tissue disorders, aortic-arch elongation, and enlarged diameter of the aorta.7,8
Treatment for TBAD has evolved in the last 20 years. Conservative treatment with optimized medication for high blood pressure has traditionally been the primary treatment in patients with uncomplicated TBAD, whereas operative treatment (open surgery and repair of descending aorta and arch) was considered as the primary treatment for patients with complicated or unstable TBAD.9–11
Thoracic endovascular aortic endovascular repair (TEVAR) was introduced in the early 2000s as another treatment option for patients with complicated TBAD. Currently, TEVAR has been widely adopted as the primary treatment for complicated TBAD based on survival benefits reported in several studies.9,12–16 Recent AHA/ACC guidelines also proposed that TEVAR may be considered for patients with uncomplicated TBAD with high-risk features. 17
TEVAR seems to provide varying benefits for patients with TBAD. Some studies have reported shorter hospital stays, lower morbidity and lower mortality for TEVAR compared to patients with complicated TBAD receiving open surgery as the primary treatment. 14 Our study group reported better overall survival in patients treated with TEVAR than those treated with medical treatment. 1 In addition, age-adjusted survival was remarkably better in patients treated with TEVAR than in those treated with open surgery or medical treatment. 1 Other authors have recently studied aortic disease-related readmissions and SAIs after primary TEVAR for TBAD.18–21 However, SAIs’ impact on survival in patients treated with TEVAR for TBAD remains unclear.
This study identified patients with TBAD treated with TEVAR who needed SAI and evaluated the role of SAI in survival.
Methods
Data collection
This was a retrospective study approved by the institutional review board of Kuopio University Hospital in 2019. Data were searched from the National Care Register for Health Care (CRHC) at the Finnish National Institute for Health and Welfare. This register automatically collects discharge data of all hospital admissions in Finland. All patients aged over 15 years with TBAD (International Classification of Disease, ICD-10 code I71.01) were included from 2000 to 2019. All data were collected retrospectively. The CRHC registry has been previously used in similar studies.1,22 Ahtela et al. 22 validated the reliability of this registry for infective endocarditis, which demonstrated the specificity of 96.8% of CRHC ICD-10 diagnostic codes. The CRHC-registry includes patients’ sex, age, length of the hospital stay, ICD-10 diagnosis codes, operational codes (Nordic Classification of Surgical Procedures) and the dates of procedures. Data search from the Official Statistics of Finland Cause of Death registry identified patients who died during the study period. The date and the cause of death of patients with TBAD were collected from the registry. All procedures (surgical or endovascular) after the initial TEVAR regarding descending thoracic aorta were considered as SAIs. Other aortic interventions such as repair of the ascending aorta or procedures to the abdominal aorta or iliac arteries were not defined as SAIs.
Statistics
Statistical analyses were done with SPSS software (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). Continuous variables were presented as means or medians with standard deviation or range. All categorical variables were presented as percentages and number of cases. Statistical differences between the two study groups (patients requiring SAI after TEVAR versus those without) were demonstrated by cross tabulation with Chi-square or Fisher’s exact tests and analysis of variance or the Kruskal–Wallis test. Survival analyses were made using the Kaplan–Meier and Cox regression models. p-value < 0.05 was considered statistically significant.
Results
Patient characteristics
Between 2000 and 2019, 1682 patients were treated for TBAD in Finland. 233 (14%) patients treated with open surgery and 1213 (72%) patients treated with medical treatment were excluded from the study. 236 (14%) patients received TEVAR as the treatment for TBAD and were included in the study. 195 (83%) patients treated with TEVAR had no SAI whereas 41 (17%) patients who received TEVAR as primary treatment needed SAI during the follow-up. 174 (74%) patients were male, and the mean age of patients was 65 years. The mean age of patients without SAI was 65 years compared to 62 years in patients with SAI. The groups did not differ significantly regarding sex or age. In the SAI group, 31 patients received TEVAR as SAI and 10 patients received open surgery as SAI. Patient characteristics are presented in Table 1. 56 (24%) patients had TAAD during the study period. There were significantly more TAADs in the SAI group than in patients without SAI (41% vs 20% p = 0.003). 71% of all TAAD occurred after TBAD.
Demographics and operative details in 236 patients undergoing thoracic endovascular aortic repair for type B aortic dissection (TBAD).
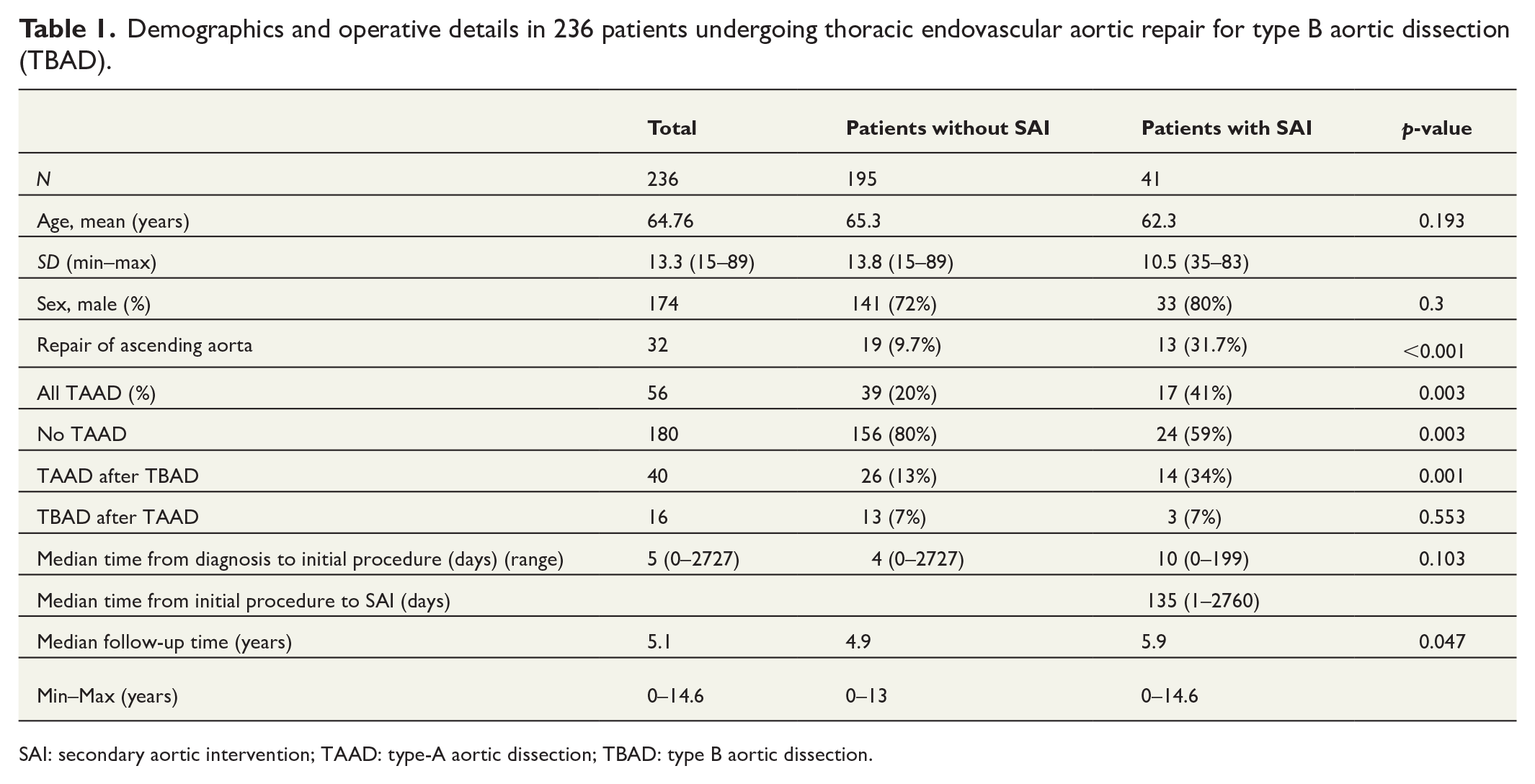
SAI: secondary aortic intervention; TAAD: type-A aortic dissection; TBAD: type B aortic dissection.
Survival
The median survival was 12.2 years (95% confidence interval 6.1–18.4) for patients without SAI and 14.6 years (95% confidence interval 6.4–22.8) for patients with SAI (Figure 1). There was no statistically significant difference in overall survival between the groups (p = 0.063). Age-adjusted survival was slightly, but not statistically significantly, better in patients who had SAI (hazard ratio 0.58, 95% confidence interval 0.27–1.22, p = 0.149) compared to patients without SAI (Figure 2). The 10-year survival was 59% for patients with SAI and 52% for patients without SAI.
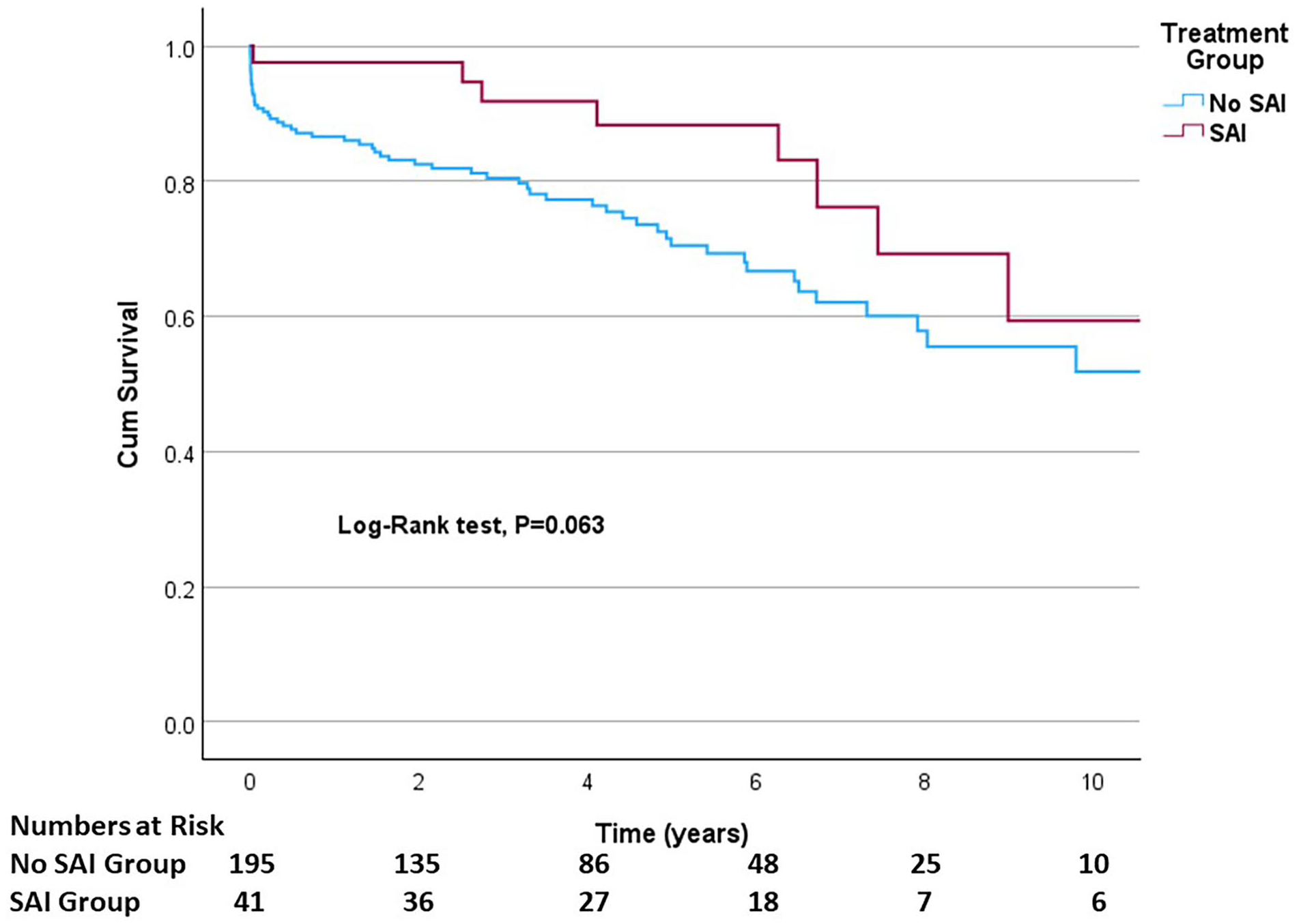
Ten-year survival of TEVAR-treated patients with type B aortic dissection.
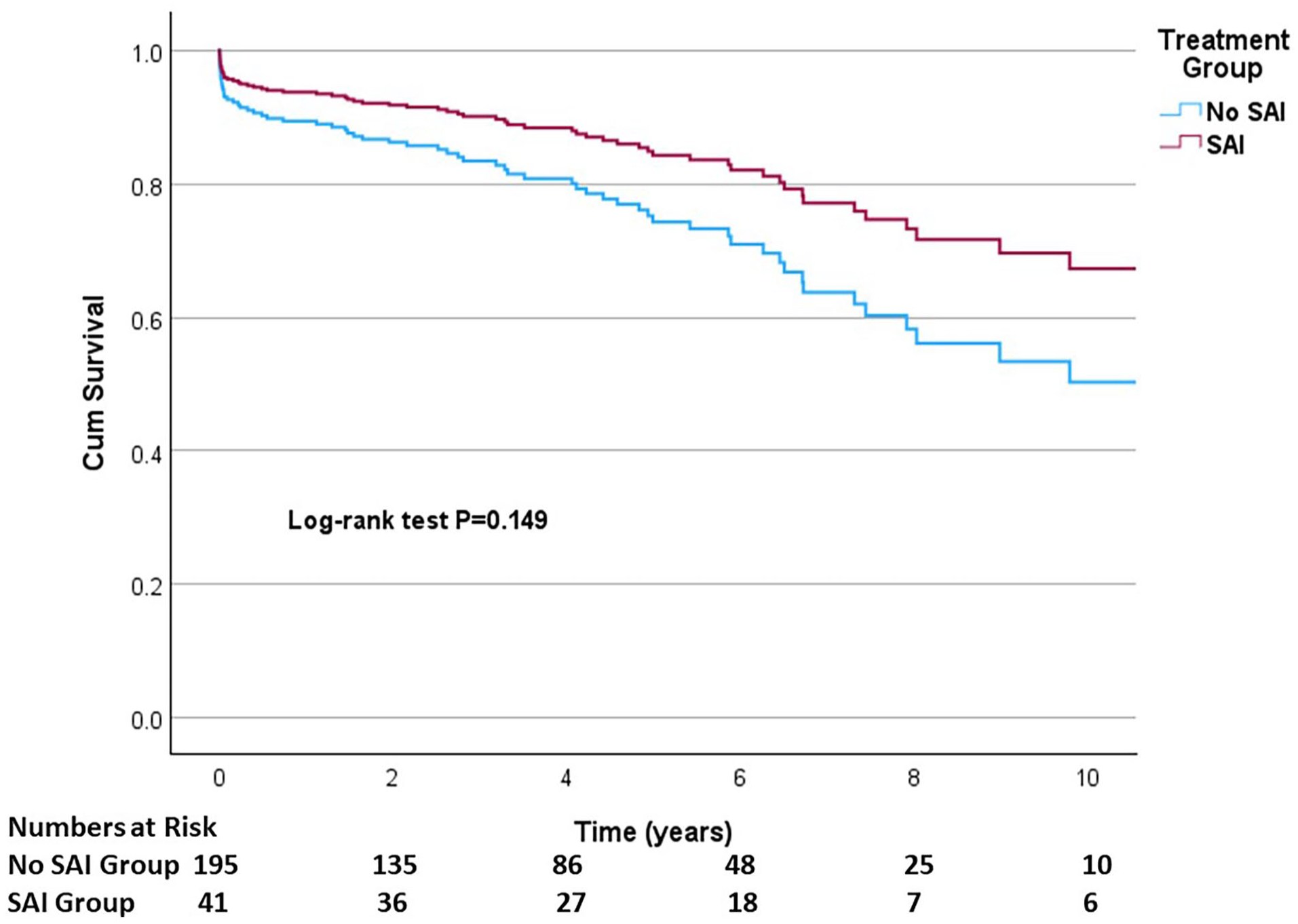
Ten-year age-adjusted survival of TEVAR-treated patients with type B aortic dissection.
Timing of operative treatment
The median time from TBAD diagnosis to primary operative treatment was four days for patients with no SAI and 10 days for patients with SAI. The groups had no statistically significant difference in median time from diagnosis to primary procedure. The median time between the initial TEVAR and SAI was 135 days. Median follow-up was significantly longer in the SAI group than in patients with no SAI (5.9 vs 4.9 years, p = 0.047). More than 50% of TEVAR procedures were performed between years 2010 and 2019 (Figure 3).
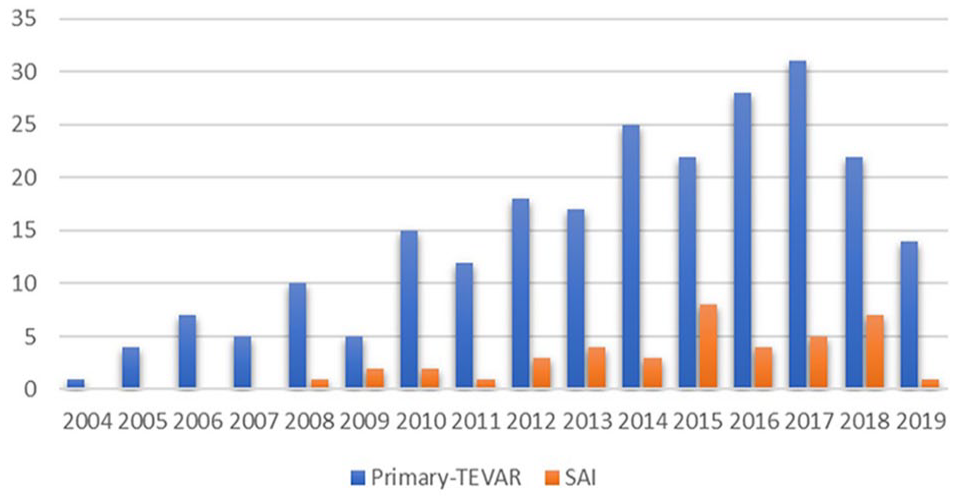
Initial TEVAR and secondary aortic interventions per year.
Cause of death
Sixty-eight (29%) patients died during the study period. The causes of death are shown in Table 2. There was no statistically significant difference in causes of death between the groups (p = 0.833). The most common cause of death in 47% of the patients was an aortic-related event (aortic dissection, rupture of aortic aneurysm). Twenty-five (37%) patients had aortic dissection as the cause of death. Cardiovascular death (aortic-related death excluded) was the second most common cause of death in both groups (32%).
Causes of death in 236 patients undergoing thoracic endovascular aortic repair for type B aortic dissection.
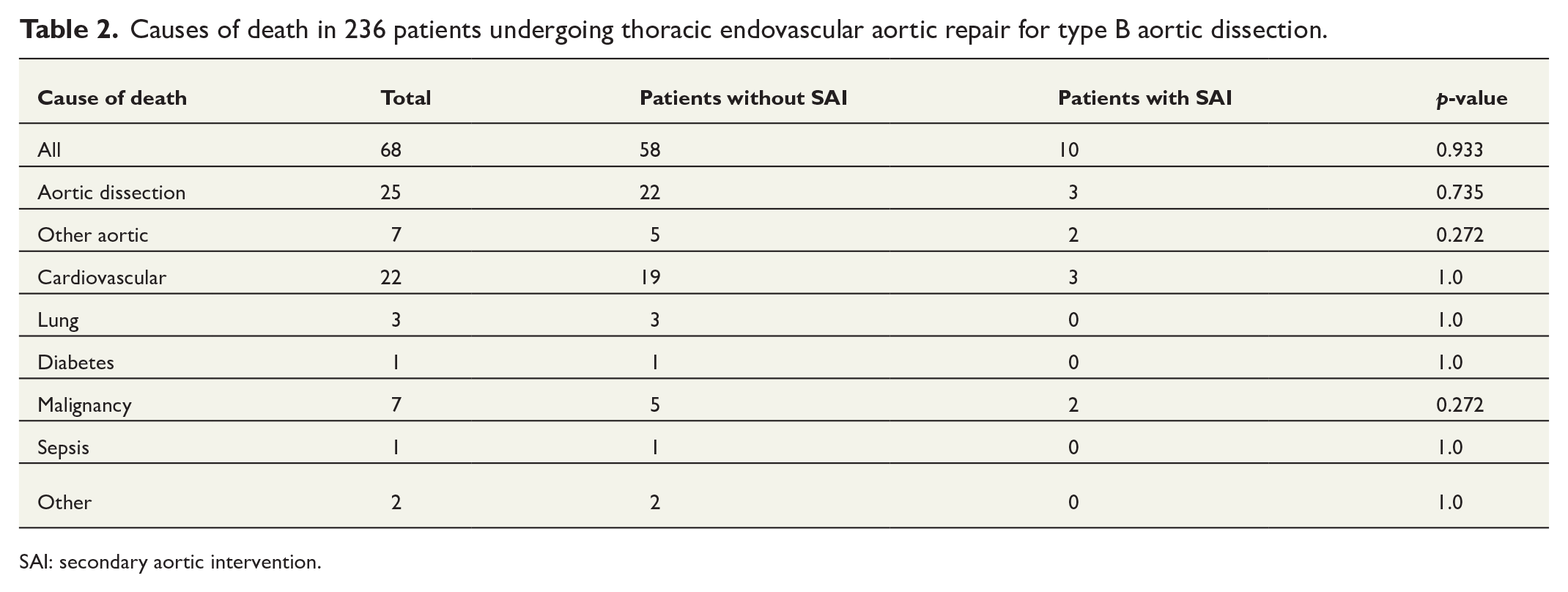
SAI: secondary aortic intervention.
Discussion
The survival benefit of TEVAR treatment compared to other treatment methods of TBAD has been shown in several studies.14,16 However, studies of the impact of SAIs’ in survival for TEVAR-treated patients with TBAD remains still unclear, and there are no recommendations for follow-up after TEVAR that could help identify patients who require SAIs. In this study, we explored patients treated with TEVAR and compared the results to those of TEVAR patients with TBAD who needed a SAI.
Demographics
The overrepresentation of the male sex in patients with TBAD has been reported in other studies.1,19,20,23 Some authors have also reported the same age and sex profile for TEVAR-treated patients with or without SAI in their studies.19,20,24 Based on these findings, with no difference in sex or age between the patients who underwent TEVAR with or without SAI, it can be concluded that neither sex nor age seems to be a risk factor for SAI after TEVAR for TBAD.
Need for SAI
In this study, the amount of SAIs performed was at the same level as other authors have reported.18–21,24,25 It is notable that in our study, patients with SAI were slightly but not statistically significantly younger than patients without SAI. This may indicate that young patients may have a genetic predisposition or more complex morphology of aortic disease than older patients and, therefore, require SAI more often. In our study, the mean time from initial TEVAR to SAI was 135 days. Other authors have presented the same length of time between the initial TEVAR to SAI in their studies.19–21,26,27
Survival
Other authors have reported survival rates similar to this study in patients with SAI compared to patients without SAI.20,21,27 This has been reported in patients with acute as well as chronic TBAD. 20 In this study, there was no statistically significant difference in survival between the groups. This may indicate that SAI does not impair survival in patients treated with TEVAR for TBAD. A possible explanation for this is that patients who received SAI were identified as high risk patients during the follow-up, and therefore, the need for SAI may have been identified more frequently compared to patients who had no SAI. The 10-year survival in both groups was less than 60%. A close follow-up would be beneficial in identifying those patients who require additional SAIs due their aortic disease progression.
Alhussaini et al. 19 reported better survival for patients who did not have SAI than patients who had SAI after primary TEVAR. However, the better survival was demonstrated in patients with acute TBAD but not in patients with chronic TBAD. Patients with <30 days mortality were excluded from the study. Therefore, the study of Alhussaini et al. is different from our study. Based on our observations and the other studies, SAI after primary TEVAR may not impair the survival of patients with TBAD.18,20,21
Timing of operative treatment
The optimal timing of TEVAR after TBAD is still unclear. Some authors have proposed that patients with non-complicated TBAD the treatment should be performed after two weeks of the onset. 28 This delay may not affect mortality but potentially decreases the need for later SAIs. 28 During 2000–2019 in Finland, decisions regarding the TEVAR treatment were based on the current clinical guidelines. Therefore, it is very likely that patients who received TEVAR had complicated TBAD. However, because of the lack of information regarding the type of dissection (complicated versus uncomplicated), it is impossible to say if the delay in TEVAR treatment for TBAD is a risk factor for SAI. Nevertheless, the difference between the groups in median time from diagnosis to invasive treatment was not statistically significant. This should be studied further.
Cause of death
Prior cardiac events have been recognized as a remarkable risk factor causing significant morbidity and mortality after TEVAR. 29 Similarly, cardiovascular events were one of the leading causes of death in our study population (32%). Aortic-related causes of death were remarkably high in both groups, 47% combined. This indicates that patients with TBAD in both groups have a high risk for aortic-related death, and patients should be carefully followed in order to recognize the patients with progressive aortic disease and in need of additional SAI.
Limitations
This study had several limitations because it was a retrospective study based on a national registry, and therefore, there may be some deficiencies in the collected data. The study group did not have a permission from the registry authorities to validate the accuracy of the collected diagnoses. However, other authors have previously validated the CRHC registry’s reliability. 22 Another limitation of the CRHC registry is that the amount of gathered data is very limited, and information considering the dissection type (acute, subacute, chronic) was not available. However, majority of the procedures were made within 10 days from the diagnosis, and therefore, it is very likely that the majority of the dissections were acute. We recognize that specific information regarding the type of SAI of each patient would have been valuable. Unfortunately, CRHC registry does not gather specific information on surgical details. We could only report the type of SAI (TEVAR vs open surgery of descending aorta). Information regarding patient’s genetic predispositions would also have been valuable. We recognize that patient groups may differ from each other regarding comorbidities and genetic predispositions, and are not directly comparable in this regard. Unfortunately, adding diagnoses other than the primary diagnosis to the CRHC registry is not mandatory, and it entirely depends on clinicians how accurately other diagnoses have been recorded in the patient’s medical records. We performed a sub-analysis of patients’ comorbidities regarding the treatment group; a notable share of the patients lacked necessary information on diagnoses other than main diagnosis of TBAD. Therefore, the results were too unreliable to be presented in this study. We are also aware that the share of patients primarily treated in TEVAR centers were followed by the hospitals that are not TEVAR centers. Therefore, it is possible that some patients that could have benefited from SAI were not in fact referred to the TEVAR centers.
Conclusions
There seems to be no difference in survival between the TBAD patients who required additional SAI after TEVAR and patients who did not require later SAI. This should be understood in a way that SAI may not worsen survival in patients who have had TEVAR as a primary operative treatment for TBAD. There is a need for high-quality randomized trial for patients with TBAD treated with TEVAR to investigate possible differences in long-term survival between patients who undergo SAI versus conservative treatment.
Footnotes
Acknowledgements
We thank Antti Valtola, MD, PhD, for his help and general support during the writing process of the manuscript.
Author contributions
Juhana Toimela collected data, performed analysis, and wrote the paper. Marja Hedman conceived and designed the analysis and wrote the paper. Tuomas Selander performed the statistical analysis and wrote the paper, Annastiina Husso conceived and designed the analysis and wrote the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J. Toimela received funding from Kuopio University Hospital Research Foundation