
Abstract
Background:
Indeterminate biliary strictures, that is, a stricture with benign brush cytology but without clear etiology in clinical or radiological assessment, pose a challenge for clinicians. This study aimed to assess the incidence and risk factors for malignant disease in patients with indeterminate biliary strictures.
Methods:
This is a single-center retrospective study of patients with indeterminate biliary stricture undergoing first endoscopic retrograde cholangiopancreatography (ERCP) and biliary brushing between March 2011 and March 2020. The study included patients with atypical cytology in the first ERCP biliary brushing samples. Main exclusion criteria were primary sclerosing cholangitis, apparent malignancy or tumor in imaging studies, postoperative strictures, chronic pancreatitis, biliary tract stone, and no ≥12-month follow-up or a final pathological diagnosis.
Results:
A total of 2279 patients underwent first ERCP procedure because of a biliary tract stricture during the study period, of which 51 patients (2.2%) had an indeterminate biliary stricture and were included. A total of 30 patients (58.8%) had final diagnosis of malignant disease. The patients with final diagnosis of malignant disease were mostly men (n = 19, 63.3%), had jaundice (n = 25, 86.2%), and had significantly higher bilirubin and CA19-9 values than those with benign disease. A total of 25 patients were operated on, of which 21 patients (84%) had malignant disease. Twenty-six patients were followed up only, of whom nine patients (34.6%) had a malignant disease.
Conclusion:
Indeterminate biliary strictures are uncommon, but two-thirds of the initially indeterminate biliary strictures are malignant. The presence of clinical jaundice and elevated bilirubin and CA19-9 values are associated with increased risk of malignancy.
Keywords
Context and Relevance
Indeterminate biliary strictures, that is, a stricture with benign brush cytology but without clear etiology in clinical or radiological assessment, are challenging. Two-thirds of the initially indeterminate biliary strictures are malignant. This study aimed to assess the incidence and risk factors for malignant disease in patients with indeterminate biliary strictures. In this study, 51 patients had an indeterminate biliary stricture. A total of 30 patients had final diagnosis of malignant disease. The patients with final diagnosis of malignant disease had mostly jaundice and significantly higher bilirubin and CA19-9 values than those with benign disease.
Introduction
Despite several recent improvements in biliary tract endoscopic methods, the accurate diagnosis of biliary tract stricture remains challenging. The most common diagnostic approach is endoscopic retrograde cholangiopancreatography (ERCP) and the biliary brushing obtained for cytology. ERCP cytology has a specificity of 100%, but the sensitivity is just around 5%–40% for diagnosing a malignancy. 1 The brush cytology samples are classified with Papanicolaou (pap) class 1–5. Pap classes 1–3 represent atypical cytology and are defined as indeterminate biliary tract strictures.
The difficulty is to know which of these patients with indeterminate strictures have a malignant disease that should be operated on, and which patients can safely be followed up or even left unfollowed. It is also still unclear which is the adequate method in diagnosing an indeterminate biliary tract stricture. In earlier studies, 37%–65% of the indeterminate biliary tract strictures have proven to be malignant.1 –7
The aim of this study was to examine the risk of cancer in patients with indeterminate biliary tract stricture and whether the risk of cancer can be predicted to know which patients should be operated on even with negative cytology samples.
Methods
Patients
The data of patients with indeterminate biliary tract strictures between 29 March 2011 and 18 March 2020 were retrospectively analyzed at the Helsinki University Hospital (HUH). The hospital serves a population of roughly 1.6 million both as a secondary and a tertiary referral center. All patients with biliary tract strictures who had undergone ERCP and biliary brushing during the study period were identified from a prospectively maintained registry of ERCP procedures. The study included patients with atypical cytology in the first ERCP biliary brushing samples (EBBS). The brush sample cellular changes are determined using pap class which is divided into five classes: Pap 1 (normal cells), pap 2 (benign atypia), pap 3 (mildly suspicious for malignancy), pap 4 (highly suspicious for malignancy), and pap 5 (malign cells). Pap classes 1–3 represent atypical cytology. The location of the stricture was divided into three groups: intrahepatic stricture (proximal to liver hilus), perihilar stricture, and distal stricture (distal to liver hilus). Bile duct dilatation was measured from computed tomography (CT) or magnetic resonance imaging (MRI) images proximal to stricture.
Exclusion criteria were as follows: (1) known diagnosis of primary sclerosing cholangitis (PSC); (2) apparent malignancy or tumor in contrast-enhanced CT or MRI (malignant thickening and/or enhancement of the biliary tract wall or obvious metastasis in liver); (3) postoperative strictures; (4) chronic pancreatitis; (5) biliary tract stone; (6) no ⩾12-month follow-up or a final pathological diagnosis; (7) acute pancreatitis or other obvious reason for stricture in imaging; or (8) first ERCP done before 29 March 2011.
The final diagnosis of malignancy was confirmed by EBBS pap classification 4–5, follow-up radiological imaging, or histology from biopsy or surgery. The final diagnosis of benign disease was confirmed by benign histology from surgery or after at least 2.5 years of follow-up without any signs of malignancy. Patients were followed up from electronic patient records up to 26 October 2023 or death.
Endoscopic retrograde cholangiopancreatography
During ERCP, the primary tools for primary biliary cannulation were a sphincterotome (Ultratome, Boston Scientific, Miami, FL) and a 0.035-inch 260-cm-long guide wire (Hydrosteer, St. Jude Medical, Minnetonka, MN). If primary cannulation failed, further techniques (pancreatic sphincterotomy, needle knife precut) to gain access were used. After gaining access to the biliary duct, the brush inside its sheath was passed above the stricture over the guidewire under fluoroscopic guidance. Leaving the bare brush above the stricture, the sheath was pulled back below the stricture. The brush was then withdrawn back into its sheath. This maneuver was repeated five times. The brush within its sheath was then pulled out as a single unit. The brush segment was cut from its wire and placed in 50% ethanol. Before that, 2 mL of cytology solution was aspirated into a syringe. The sheath of the brush was then flushed with the cytology solution into the same sample. The whole sample, brush and flushing sample, was transported to the cytology laboratory for routine processing. Cytospin slides were stained with Papanicolaou stain. A cell block was also prepared if there was enough material, and cell block sections were stained with hematoxylin and eosin. 8
Boston Scientific single-operator per-oral cholangioscopy, SpyGlass, endoscopic ultrasound (EUS), and papillabiopsies were performed for the patients with benign brush cytology and a strong suspicion for malignancy. The use of SpyGlass increased during the study period. In HUH, SpyGlass cholangioscopy consists of spybiopsies, flush fluid sample, and normal biliary brushing samples. Papillabiopsies are taken if there is a suspicion of autoimmune disease or if the papilla seems abnormal.
Statistics
The categorical variables were compared with Fisher’s exact test. The continuous variables were analyzed with Mann–Whitney U test. Patients with missing values were excluded from analyses of that variable. Statistical analyses were conducted using IBM SPSS software, version 25 (IBM Corp, Armonk, NY). Two-tailed p < 0.05 was considered statistically significant.
Results
A total of 2279 patients underwent first ERCP procedure because of a biliary tract stricture during the study period. After exclusion of PSC (29), patients with apparent malignancy or tumor in imaging studies (1511), postoperative strictures (250), chronic pancreatitis (139), biliary tract stone (69), no biliary brush samples (161), no ≥12-month follow-up or a final pathological diagnosis (38), or other reason (31), a total of 51 patients were included in this study.
Baseline characteristics of the study population are shown in Tables 1 and 2. The median age at referral was 67 (36–92), of whom 51% were male. Most of the patients presented with symptoms (n = 46, 90.2%) and had clinical jaundice (n = 33, 64.7%). Only 20 (39.2%) patients had abdominal pain. The majority (n = 33, 64.7%) had a distal stricture. All of the nine patients who had wirsungianus dilatation also had bile duct dilatation, meaning that nine patients had double-duct sign. Only four (44.4%) of them had final diagnosis of malignant disease. The patients who had final diagnosis of malignant disease (n = 30) were mostly men (n = 19, 63.3%), had jaundice (n = 25, 86.2%), and had significantly higher bilirubin and CA19-9 values than those with benign disease.
Baseline characteristics of the patient cohort.
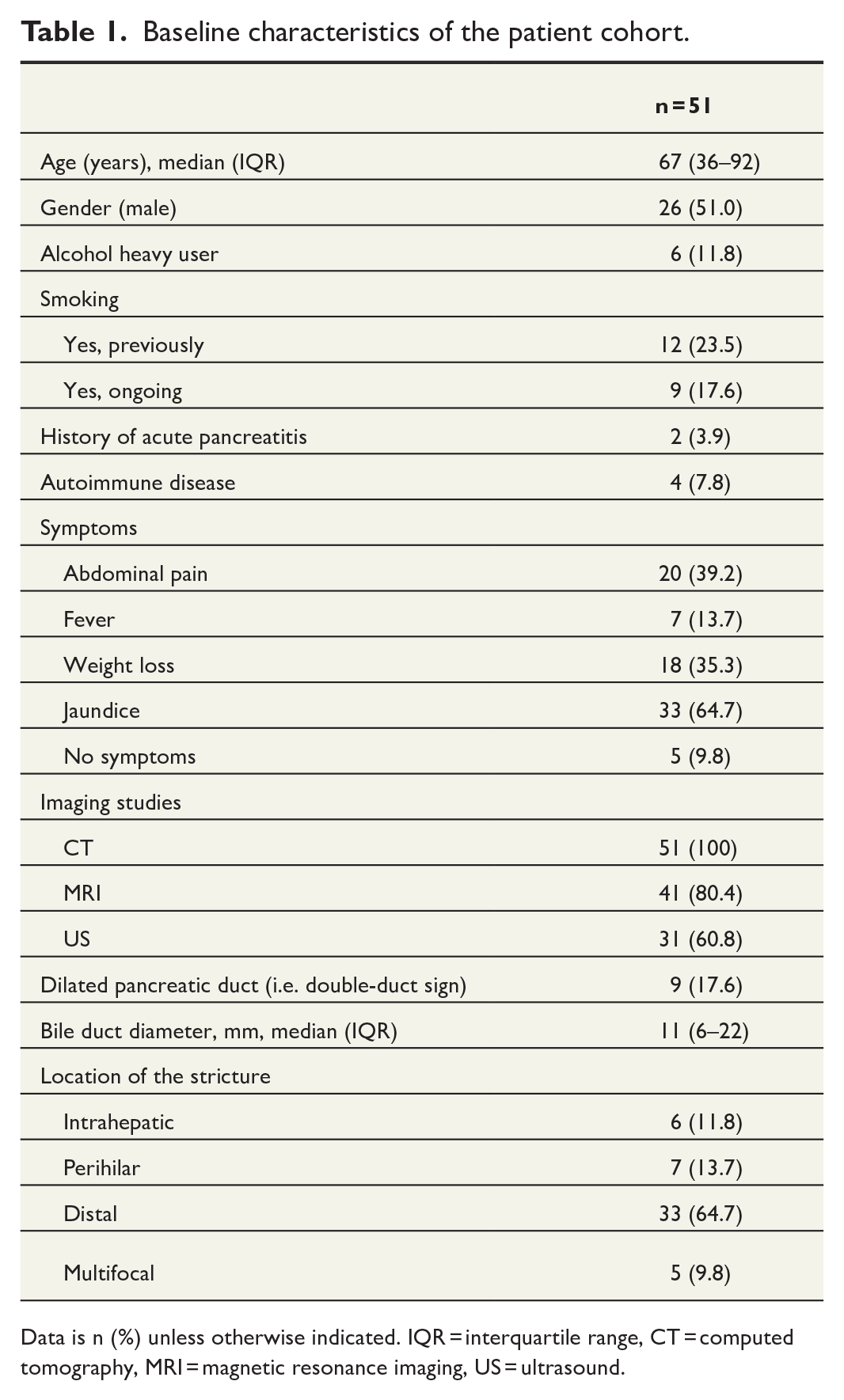
Data is n (%) unless otherwise indicated. IQR = interquartile range, CT = computed tomography, MRI = magnetic resonance imaging, US = ultrasound.
Baseline characteristics of the patient cohort.
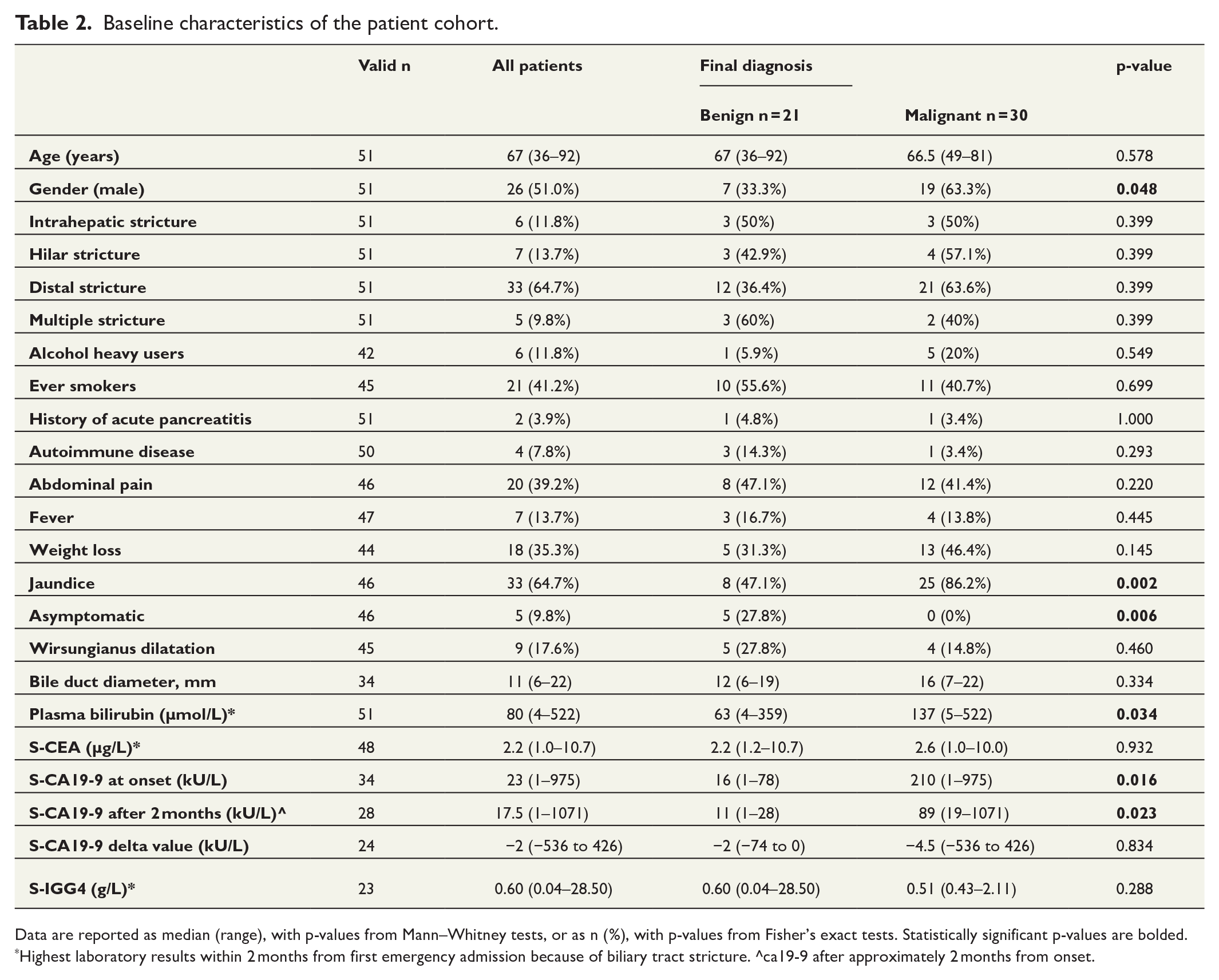
Data are reported as median (range), with p-values from Mann–Whitney tests, or as n (%), with p-values from Fisher’s exact tests. Statistically significant p-values are bolded.
Highest laboratory results within 2 months from first emergency admission because of biliary tract stricture. ^ca19-9 after approximately 2 months from onset.
Twenty-five (49.0%) patients developed either clinical/radiological or biopsy-proven suspicion for resectable malignancy and were surgically operated on, of which four patients proved to be non-operatable intraoperatively (Table 3, Fig. 1). For 23 patients (45.1%), surgery was the method that confirmed the diagnosis. The method of surgery was pancreatoduodenectomy for majority of the patients who were operated on (n = 17, 68%). Only four (16%) patients who underwent surgery had a final diagnosis of benign disease. A total of 26 patients were not operated on and were followed up only (consisting of repeated EBBS (approximately after every 3 months during stent replacements), imaging (every 3–12 months), and laboratory controls (usually simultaneously with EBBS) and possible EUS), of which nine patients had a final diagnosis of malignant disease (four of them were cholangiocarcinomas, three pancreatic adenocarcinomas, one ampulla carcinoma, and one lymphoma). Two of those were intrahepatic, two perihilar, and five were distal strictures. For these nine patients, the malignant disease was diagnosed between 1 month and 3 years after the first indeterminate biliary tract stricture episode and none of them underwent surgery. There were no significant differences between the patients who were and were not operated on in terms of comorbidity and age.
Results, procedures, and diagnosis of the patient cohort.
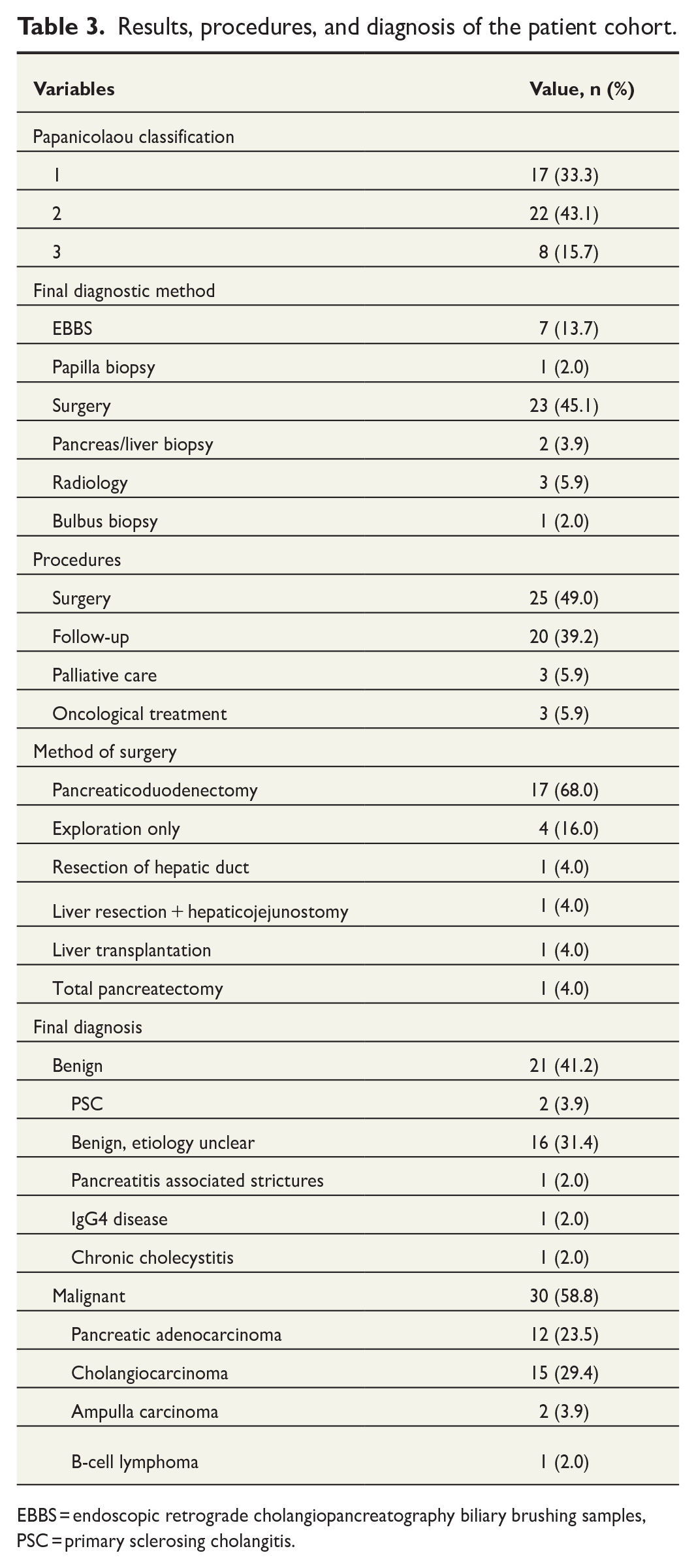
EBBS = endoscopic retrograde cholangiopancreatography biliary brushing samples, PSC = primary sclerosing cholangitis.
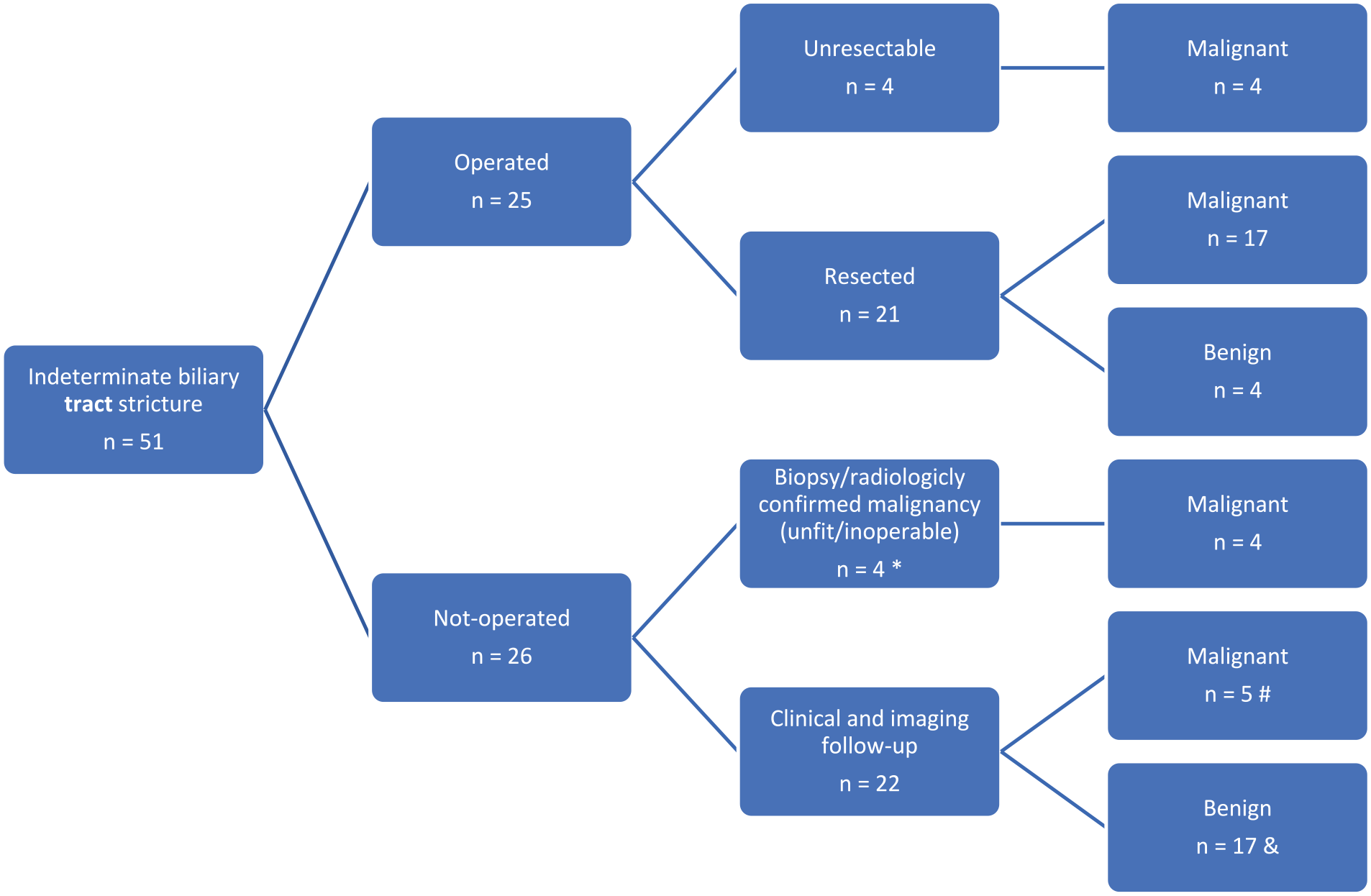
Flow chart demonstrating the outcome of the patients with an indeterminate biliary tract stricture.
Twenty-one patients had the final diagnosis of benign disease of which 13 (62%) had the diagnosis remained indeterminate during at least 54 months of follow-up. Thirty patients (58.8%) had the final diagnosis of malignant disease and the majority of them had either pancreatic adenocarcinoma (n = 12, 40%) or cholangiocarcinoma (n = 15, 50%).
Approximately two-thirds of the patients who had pap 2 or 3 in the first ERCP the final diagnosis was malignant (68.2% and 62.5% respectively), whereas only less than half (47.1%) of the patients with pap 1 had malignant final diagnosis (Fig. 2). In the majority of patients (n = 22, 73%) whose final diagnosis was malignant, the diagnosis was made within 6 months from the first ERCP, while one stricture turned out to be malignant 49 months after first ERCP (Table 4).
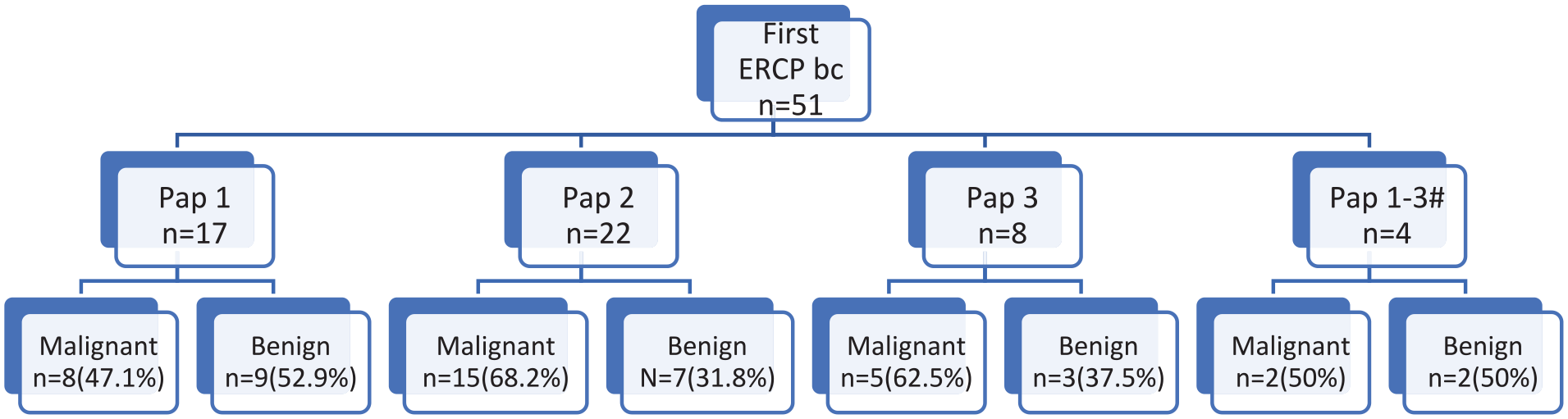
Flow chart showing the enrollment of study patients and distribution based on first endoscopic retrograde cholangiopancreatography (ERCP) brush cytology (bc) and the final diagnosis (four patients were missing the data of exact pap classification). #Not accurately specified.
Time interval from first ERCP with brush cytology pap 1-3 to cancer diagnosis in patients whose indeterminate biliary stricture turned out to be malignant.
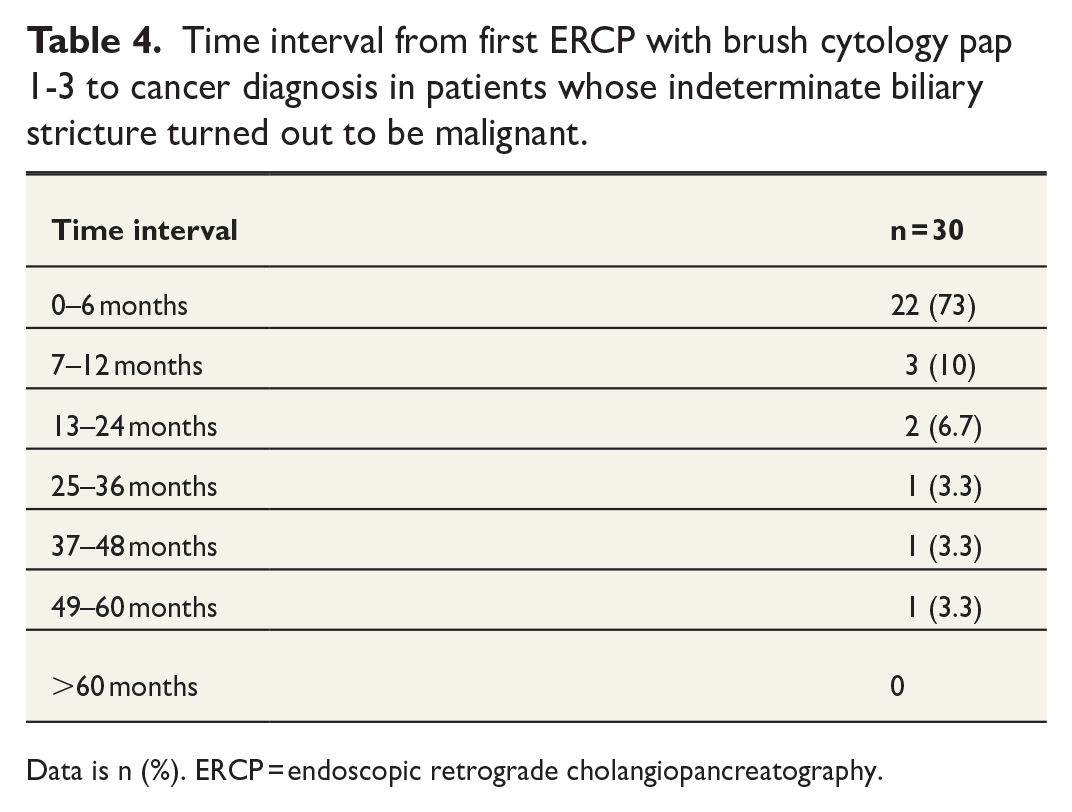
Data is n (%). ERCP = endoscopic retrograde cholangiopancreatography.
SpyGlass cholangioscopy procedure was done for 22 (43.1%) patients and for 6 patients it was done twice. SpyGlass cholangioscopy result (spybiopsy or flush fluid sample) was malignant only in five patients. A total of 11 (50%) patients who underwent SpyGlass cholangioscopy procedure had final diagnosis of malignant disease. Sensitivity of SpyGlass cholangioscopy was 45.5% and specificity was 100%. However, the sensitivity was better (3/5 60%) for the latter 11 patients of the SpyGlass cholangioscopy patient population than for the first 11 patients (2/6 33.3%). EUS was done for 10 (19.6%) patients and for 5 (50%) of them result was suspicious for malignancy (tumor or biliary tract wall thickness in the EUS). Four of those five patients who had suspicions for malignancy in EUS had final diagnosis of malignant disease. In total, six (60%) patients who underwent EUS had final diagnosis of malignant disease. The sensitivity of EUS was 66.7% and specificity was 80%. Papillabiopsy was taken from 20 (39.2%) patients during an ERCP and only one of them was malignant (adenocarcinoma) (Table 5).
Number of ERCP brush cytology malignant results, SpyGlass procedures, endoscopic ultrasounds and papillabiopsies of the patient cohort.
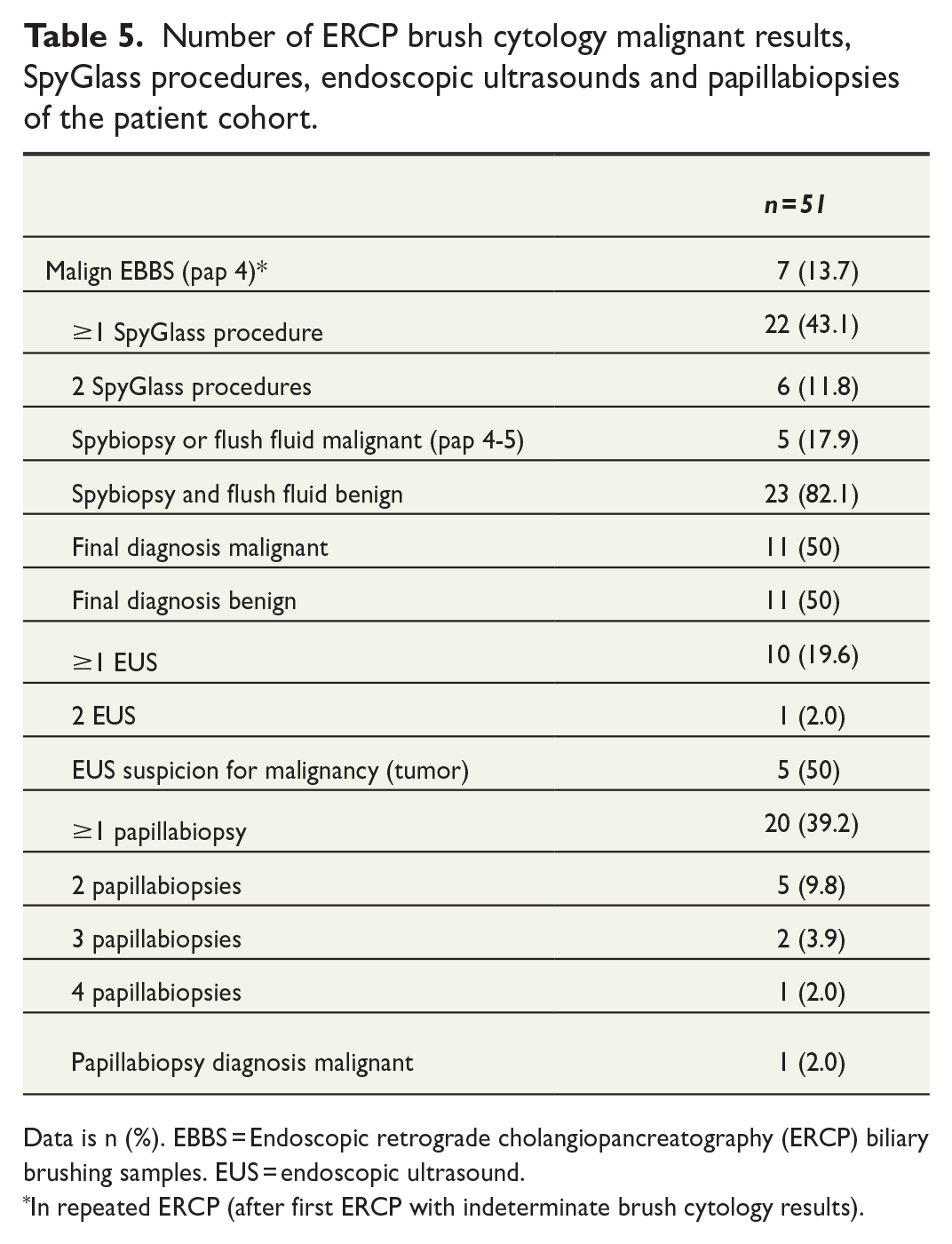
Data is n (%). EBBS = Endoscopic retrograde cholangiopancreatography (ERCP) biliary brushing samples. EUS = endoscopic ultrasound.
In repeated ERCP (after first ERCP with indeterminate brush cytology results).
Discussion
In this study, only 2.2% of the patients with a biliary stricture undergoing an ERCP had an indeterminate stricture, which makes it a relatively uncommon finding. Furthermore, almost two-thirds of initially indeterminate biliary stricture turned out to be malignant in the follow-up, which indicates that such strictures need to undergo strict surveillance if not undergoing upfront surgery. Especially patients with jaundice and elevated CA19-9 seem to be at high risk for final diagnosis of malignancy, whereas patients without symptoms seemed to have the final diagnosis of benign stricture.
Our findings are similar to earlier studies. In previous studies, there has been an association between elevated bilirubin and CA19-9 values and a malignant stricture.3,9 In patients with malignant biliary tract strictures, the average bilirubin level was over two times higher than in the benign group and almost seven times higher than the upper limit of normal. The male gender as an independent predictor for malignancy has not been mentioned in previous studies and the result might be explained by the limited number of patients in our study population. On the other hand, some of the studies have reported much lower percentages for final diagnoses of malignant disease being closer to one-third of the patients compared to almost two-thirds of the patients in our series. 3 Double-duct sign has significantly increased the probability of malignancy in previous studies. 10 However, in our study, double-duct sign did not increase the probability of malignancy.
There is a need for new diagnostic methods for indeterminate biliary tract strictures. There are new improved diagnostic methods such as the cholangioscopy and mini-forceps biopsy and EUS. SpyGlass cholangioscopy has much higher sensitivity of 71%–77% compared to normal ERCP and biliary brushing cytology.2,11 However, in our study, the sensitivity of SpyGlass cholangioscopy was only 45.5%. That is probably because procedures in the early years of this study were performed using older SpyGlass equipment with lower image quality. Moreover, the SpyGlass cholangioscopy was a rather new procedure in HUH in 2011 and there was a learning curve for taking proper biopsies and for the pathologists to analyze them correctly, which is in line with the higher sensitivity (60%) for the latter half of the patients. In addition, in the beginning, there had usually been a biliary stent before the first SpyGlass cholangioscopy that hampers the visual impression. In recent years, the SpyGlass cholangioscopy has usually been performed before stenting. In a consensus guideline statement, it is suggested that SpyGlass cholangioscopy might be advisable to perform before biliary tract stenting for patients with indeterminate biliary tract stricture because it allows optimal visual inspection of the stricture morphology and targeted biopsies without the inflammation, trauma, and neovascularization, which may be associated with previous ERCP and stent placement. 12 Our findings suggest that SpyGlass cholangioscopy may have lower sensitivity in indeterminate biliary strictures than suggested by the previous studies. However, that is probably explained by the learning curve.
Imaging has a vital role in diagnosing biliary tract malignancies. In previous studies, only finding a mass lesion in imaging was strongly associated with underlying biliary tract malignancy. EUS has significantly better sensitivity and accuracy compared to CT and MRI especially for small tumors (<2 cm).13,14 In our study, the EUS was done only for 10 (19.6%) patients and the sensitivity was 66.7%. 64.7% of the strictures were in distal bile duct where EUS is most accurate. Performing routine EUS for selected indeterminate biliary tract stricture patients, especially for those with distal stricture, potentially improves the diagnostic yield. There is still a need for better diagnostic methods for indeterminate biliary tract strictures such as larger biopsy forceps and intraluminal ultrasound.
The limitation of this study was the small number of patients included in our study population. This is in line with previous studies. 3 That is probably because the current imaging methods are so precise and sensitive to find even the smallest of tumors that there are only a few biliary strictures which are truly indeterminate. Limitations include the retrospective design of the study with its potential flaws. For example, some of the clinical data were missing for the patients referred to HUH from other hospitals, which may have affected the results. The absolute strength of this study was the long-term follow-up (at least 2.5 years) of all the included patients. One of the strengths was the use of SpyGlass cholangioscopy in this study that has not been possible for many of the other studies on this subject.
Conclusion
Patients with indeterminate biliary tract stricture and elevated ca19-9 and bilirubin values are at a higher risk of underlying malignant disease. These patients should be thoroughly examined with all possible diagnostic methods. There is still a need for better diagnostic methods for indeterminate biliary tract strictures.
Footnotes
Acknowledgements
There were no other contributors to the research than the authors listed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from Helsinki University Hospital research grants.
Patient consent
Patient consent was not needed as this was a retrospective study.
Trial registration
Not registered as this study was not a trial.
Grant number
TYH2023419
Ethical statement
Ethical board approval was waived due to the retrospective nature of the study.
Data availability
Finnish laws do not permit sharing individual patient data.