
Abstract
Background and objective:
The reported incidence of persistent hypoparathyroidism varies widely, and consensus on a definition is lacking. The objective was to evaluate the real-life incidence of persistent hypoparathyroidism by investigating a new pragmatic definition.
Methods:
This retrospective multicenter cohort study evaluated the effect of different definitions for persistent hypoparathyroidism on the incidence of hypoparathyroidism. In addition, risk factors for hypoparathyroidism were analyzed.
Results:
In total, 749 patients were included. Using the new pragmatic definition, we report an incidence of 7.9% of persistent hypoparathyroidism. When applying other commonly used definitions, incidence varied between 11.8% and 22.1%. Risk factors were parathyroid autotransplantation, presence of another surgical complication, and low postoperative serum calcium.
Conclusions:
Our data show that the incidence of persistent hypoparathyroidism in the literature may vary through the use of different definitions. This study indicates that a new pragmatic definition of persistent hypoparathyroidism has the potential to enable unbiased comparison between studies.
Introduction
Hypoparathyroidism is the most common iatrogenic complication after total or completion thyroidectomy and is caused by inadvertent resection or devascularization of the parathyroid glands, leading to the absence or insufficient production of parathyroid hormone (PTH). 1 Postoperative hypoparathyroidism results in hypocalcemia and may cause direct clinical symptoms such as paraesthesia and muscle cramps. On the long term, patients with hypoparathyroidism are at risk for various comorbidities and complications, such as chronic kidney disease, basal ganglia calcifications, and hospitalization due to seizures resulting in an impaired quality of life.2 –4 A recent study even described higher mortality rates in this population. 5
In most cases, parathyroid function will recover within the first year after surgery, and calcium levels will normalize.6,7 Although the majority of single-center studies have shown an incidence of persistent hypoparathyroidism of less than 5%, more recent national registries and multicenter studies have published much higher incidence rates up to 16.7%.8 –13 Incidence rates are affected by the populations case-mix, as patients with Graves’ disease and patients undergoing lymph node dissection have an increased risk of hypoparathyroidism.14,15 Besides case-mix, incidence rates are greatly influenced by the definition being used, as demonstrated by the study of Mehanna et al. 16 Definitions vary from the need for calcium supplements after 6 months to the need for calcium and/or active vitamin D analogues, and low PTH levels after 12 months. 17 Multiple studies have shown that parathyroid function may recover within the first year after surgery and by diagnosing patients with persistent hypoparathyroidism before 12 months may lead to inappropriate incidence rates.6 –8 The same principle applies when persistent hypoparathyroidism is defined as the need for calcium supplements only, without the use of active vitamin D since active vitamin D with or without calcium is the conventional therapeutic approach for hypoparathyroidism.18 –20 Furthermore, active weaning off supplementation must be attempted to prevent overtreatment and an incorrectly diagnosed hypoparathyroidism. 20 Currently, there is no international consensus on the definition of persistent hypoparathyroidism, which impedes an unbiased comparison of studies. To overcome these limitations, we evaluated a new pragmatic definition of persistent hypoparathyroidism (the need for active vitamin D analogues with or without calcium supplements 12 months after surgery with an attempt to actively wean off supplementation) in a retrospective multicenter cohort study and compared it with commonly used other definitions. In addition, we tried to identify risk factors for persistent hypoparathyroidism.
Materials and methods
Study design and setting
This is a retrospective multicenter cohort study performed in 10 hospitals in the Southwestern region of the Netherlands, who participate in the Thyroid Network. This collaboration entails one university hospital and nine non-university hospitals, and was formed to implement uniform and structured regional care pathways. Approval was obtained from the Medical Ethical committee of Erasmus MC (MEC-2018-1195). The requirement for written informed consent was waived, given the retrospective character of this study. The STROBE guidelines for reporting observational studies were used.
Patients and data
All adult patients (⩾18 years) undergoing a total or completion thyroidectomy between January 2010 and December 2016 in the Thyroid Network were included. Exclusion criteria included preoperative parathyroid dysfunction, the use of active vitamin D for any cause, reoperation in the central neck compartment within 1 year after total or completion thyroidectomy or missing 1-year follow-up data. For clarity, the use of preoperative calcium supplementation is not an exclusion criteria as de novo calcium supplementation after surgery was assessed. Data on calcium and/or active vitamin D treatment at discharge and 12 months after surgery were retrieved directly from the medical charts. Other data that were retrospectively collected from electronic medical charts were as follows: baseline characteristics (age, gender, body mass index (BMI), indication for surgery), perioperative data (type of surgery, extent of surgery, parathyroid gland identification), postoperative data (length of hospital stay, hospital readmission and emergency department (ED) visits for hypocalcemic symptoms, serum calcium at first postoperative day), histopathological data (histopathological diagnosis, presence of parathyroid tissue), and data on adjuvant treatment. Hospital readmission is defined as a hypocalcemia event in which the patient could have been admitted from both the ED or outpatient clinic. ED visits are defined as a hypocalcemia related visit to the ED, without the need for hospital readmission. ED visits prior to hospital readmission are counted as a hospital readmission and not as an ED visit separately. Data on other complications were collected. Temporary laryngeal nerve paralysis was defined as laryngeal nerve paralysis confirmed by fibroscopy that resolved within the first year after surgery. Permanent laryngeal nerve paralysis was defined as laryngeal nerve paralysis 1 year or more after surgery confirmed by fibroscopy.
Surgical procedure
Total or completion thyroidectomy was performed by endocrine surgeons via a Kocher incision. Thyroidectomy procedures were performed in the same standardized manner by ligating the superior vessels, mobilizing the upper pole, followed by the capsular dissection technique with respect to the parathyroid glands. Inferior vessel ligation was performed after identification of the recurrent laryngeal nerve. Inadvertently resected parathyroid glands were autotransplanted into the sternocleidomastoid muscle. A central lymph node dissection (CLND) or lateral lymph node dissection (LLND) was performed when indicated (preoperative suspicion of lymph node metastasis or proven lymph node metastasis). Prophylactic cervical lymph node dissections were not performed.
Definitions and management
To assess the impact of definition on the rate of hypoparathyroidism, we applied the following three definitions. For the first definition, patients were considered to have persistent hypoparathyroidism (1) if they used de novo prescribed active vitamin D analogues with or without calcium supplements 12 months after surgery, irrespective of the dosage and (2) if they had an unsuccessful attempt of active weaning off in supplementation. Patient medical records were searched for attempts of weaning. Both treating physician notes and pharmacy prescriptions were checked. If no information was available, data were assumed as missing. The second definition included all patients who at least used a de novo active vitamin D analogue, whether or not in combination with de novo calcium supplements, 12 months postsurgery. This definition did not take into account active weaning off. The third definition included all patients who used de novo calcium and/or active vitamin D analogues, 12 months postsurgery without any confirmed attempt to decrease and stop this medication. Every hospital had their own calcium supplementation protocol, and weaning off medication was according to the discretion of the treating physician. Direct postoperative hypocalcemia was treated with calcium carbonate and active vitamin D analogues. Serum calcium levels were adjusted for albumin levels according to the following formula: adjusted total calcium (mmol/L) = measured calcium (mmol/L) + (0.025 × 40 − (albumin (g/L)).
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) or median with interquartile ranges (IQRs) as appropriate. Categorical variables were described as counts (n) and percentages (%). Normality was assessed using the Shapiro–Wilk normality test. Mean values and medians were compared with a Mann–Whitney U test and chi-square or Fisher’s exact test, where appropriate. Missing data are presented in parentheses behind variables. Univariate and multivariable logistic regression analysis was performed to evaluate risk factors for persistent hypoparathyroidism, using the first definition. Statistically significant variables in univariate analysis and those judged to be clinically relevant were included in the multivariable logistic regression analysis, considering the restricted number of variables of 1 variable per 10 cases. p-values of <0.05 were considered significant. IBM SPSS Statistics 25 (IBM Corp., Armonk, NY, USA) was used to perform all statistical analyses.
Results
Total study cohort
In total, 780 adult patients underwent a total or completion thyroidectomy between January 2010 and December 2016, of which 749 were included in this study (Fig. 1). Baseline characteristics of the total study cohort are summarized in Table 1. In total, 470 (62.8%) patients underwent a one-stage total thyroidectomy, and 279 (37.2%) patients underwent a completion thyroidectomy. CLND ± LLND was performed in 153 (20.4%) patients, of which 61 (8.1%) CLND only and 92 (12.3%) had both CLND + LLND surgery. A parathyroid autotransplantation was performed in 52 (6.9%) patients, and in 183 (24.4%) patients’ parathyroid tissue was found at histology. Other complications than hypoparathyroidism were wound infection in 9 (1.2%) patients, chyle leakage in 11 (1.5%) patients, reoperation for bleeding in 27 (3.6%) patients, temporary laryngeal nerve paralysis in 21 (2.8%) patients, and permanent laryngeal nerve paralysis in 43 (5.7%) patients.
Clinicopathological, procedural, and postoperative outcomes for the total study cohort.
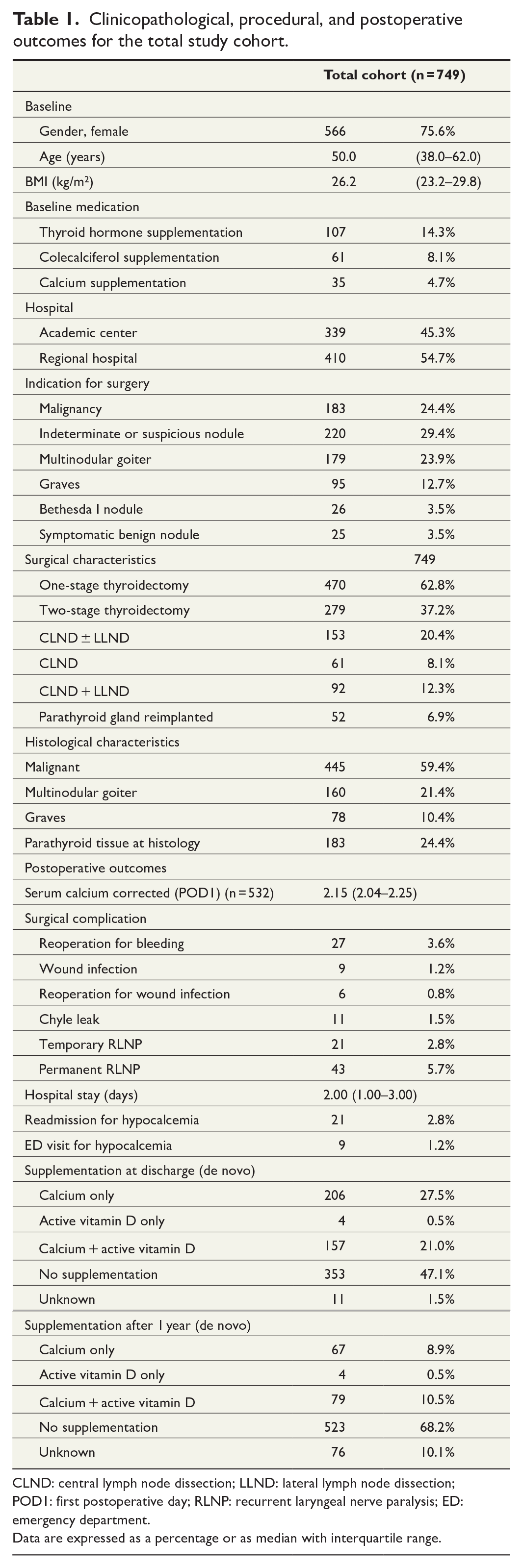
CLND: central lymph node dissection; LLND: lateral lymph node dissection; POD1: first postoperative day; RLNP: recurrent laryngeal nerve paralysis; ED: emergency department.
Data are expressed as a percentage or as median with interquartile range.
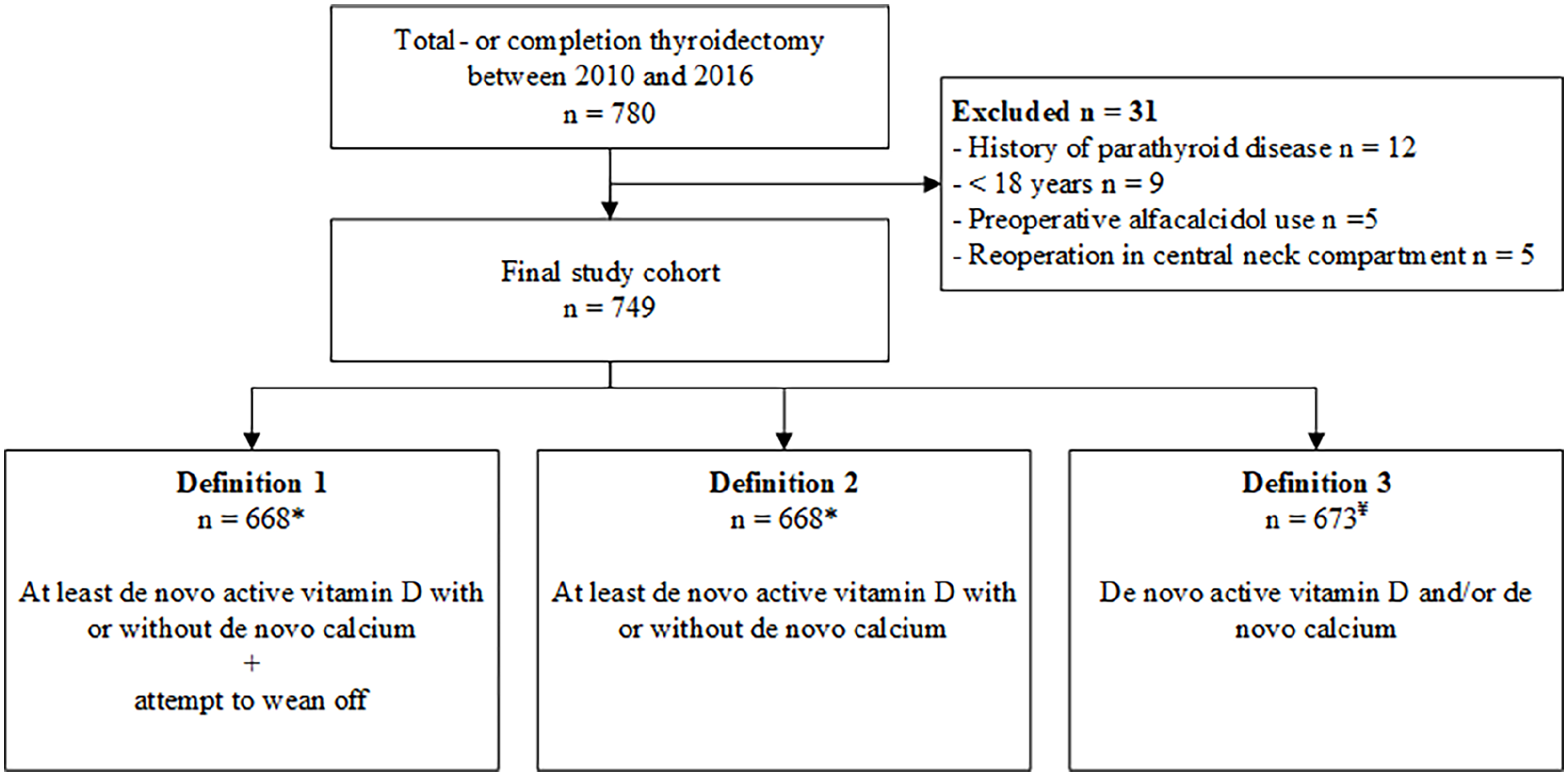
Flowchart of patient enrollment.
Incidence of hypoparathyroidism using different definitions
Three different definitions were used to assess the incidence of persistent hypoparathyroidism. Due to the use of different definitions, three different cohorts were created (Fig. 1). For the first and second definitions, 81 patients were excluded due to missing data on active vitamin D 1 year after surgery. For the third definition, 76 patients were excluded due to missing data on calcium and/or active vitamin D 1 year after surgery. When applying the first definition, 53 out of 668 (7.9%) patients were considered to have persistent hypoparathyroidism (Table 2). The incidence of persistent hypoparathyroidism was 11.8% (79/668) when using the second definition and 22.1% (149/673) when using the third definition. Subgroup analysis of patients with benign versus malignant disease and whether a CLND ± LLND was performed showed a similar trend for the three definitions (Table 2).
Subgroup analysis on the incidence of hypoparathyroidism using the three different definitions.
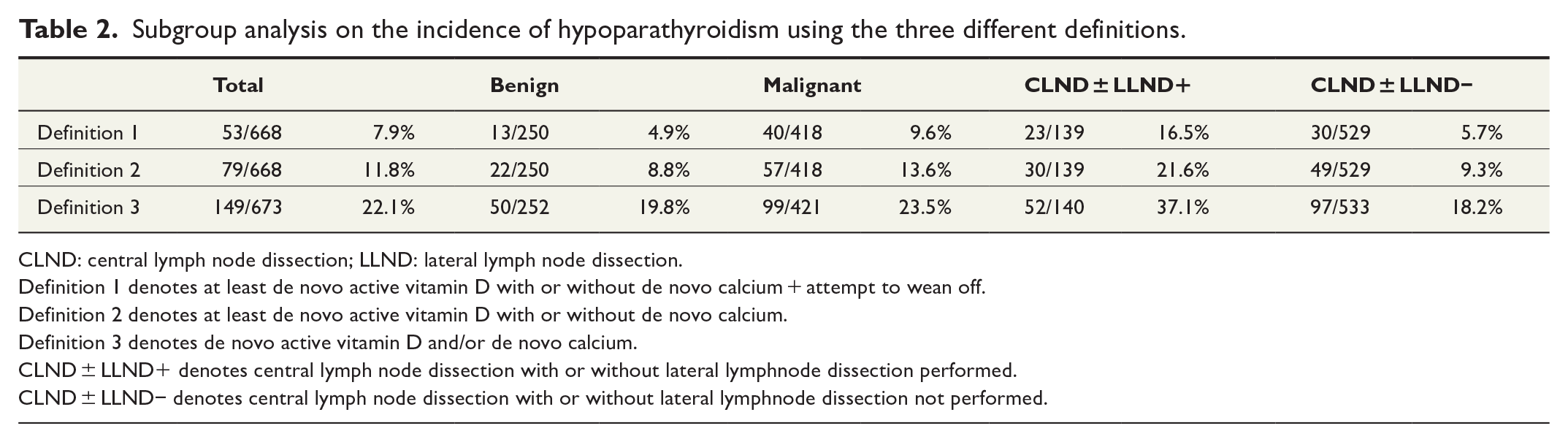
CLND: central lymph node dissection; LLND: lateral lymph node dissection.
Definition 1 denotes at least de novo active vitamin D with or without de novo calcium + attempt to wean off.
Definition 2 denotes at least de novo active vitamin D with or without de novo calcium.
Definition 3 denotes de novo active vitamin D and/or de novo calcium.
CLND ± LLND+ denotes central lymph node dissection with or without lateral lymphnode dissection performed.
CLND ± LLND− denotes central lymph node dissection with or without lateral lymphnode dissection not performed.
Postoperative outcomes and risk factors for persistent hypoparathyroidism
The postoperative outcomes of patients with or without persistent hypoparathyroidism are depicted in Table 3. Patients with persistent hypoparathyroidism had a longer hospital stay than patients without persistent hypoparathyroidism (4.00 (IQR = 2.24–6.75) days vs 2.0 (IQR = 1.0–3.00) days; p < 0.001). Patients with persistent hypoparathyroidism were readmitted to the hospital more often and visited the emergency department more often for hypocalcemia (15.1% vs 2.1%; p < 0.001% and 9.4% vs 0.7%; p < 0.001, respectively). Univariate analysis showed that a malignancy, one-stage thyroidectomy, CLND ± LLND and CLND + LLND, parathyroid autotransplantation, parathyroid tissue at histology, lower postoperative serum calcium, and the occurrence of a surgical complication were significantly associated with persistent hypoparathyroidism (Table 3). Multivariable analysis showed that a lower postoperative serum calcium, parathyroid gland autotransplantation, and presence of another surgical complication were significantly associated with persistent hypoparathyroidism (Table 4).
Clinicopathological, procedural, and postoperative outcomes stratified by hypoparathyroidism for the first definition (n = 670).
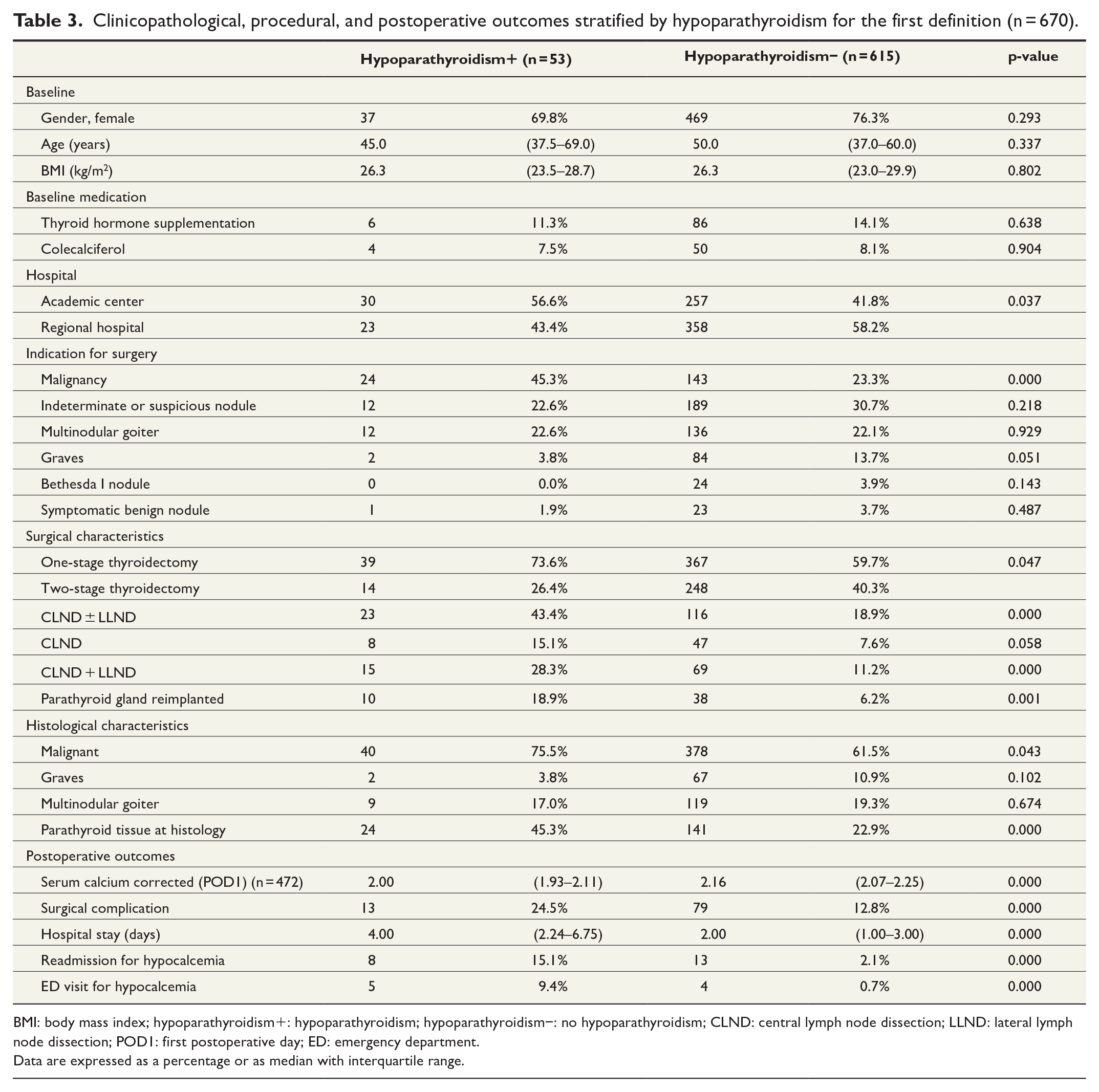
BMI: body mass index; hypoparathyroidism+: hypoparathyroidism; hypoparathyroidism−: no hypoparathyroidism; CLND: central lymph node dissection; LLND: lateral lymph node dissection; POD1: first postoperative day; ED: emergency department.
Data are expressed as a percentage or as median with interquartile range.
Multivariable analysis of variables affecting the development of hypoparathyroidism using the first definition.
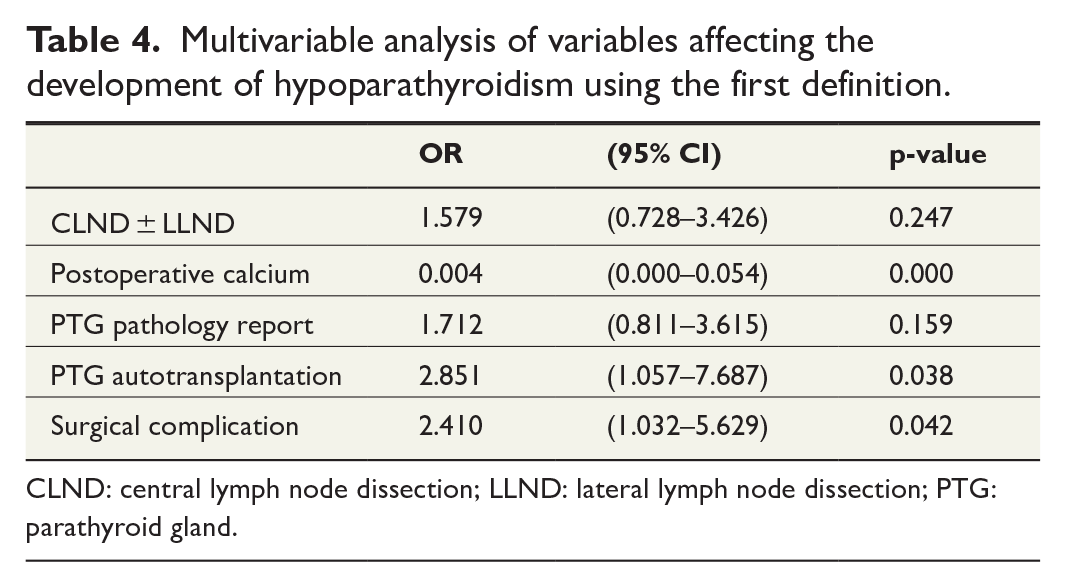
CLND: central lymph node dissection; LLND: lateral lymph node dissection; PTG: parathyroid gland.
Discussion
Utilizing a new pragmatic definition, we report in this multicenter study an incidence of 7.9% of persistent hypoparathyroidism. This new definition incorporates both the use of an active vitamin D analogue with or without calcium supplementation with an attempt to actively wean off supplementation. When applying other commonly used definitions, incidence of hypoparathyroidism in this study varied between 11.8% and 22.1%. 17 These differences further underline the need for international consensus on the definition of hypoparathyroidism. Active vitamin D has been the conventional therapeutic approach for many years18 –20 in patients with persistent hypoparathyroidism after surgery. However, active weaning off vitamin D and calcium supplementation in these patients is often overlooked and leads to often, lifelong overtreatment. 20 We therefore propose to use this new definition, which gives a fair picture of the true incidence of postoperative hypoparathyroidism. This definition is underlined by the recently published expert consensus statement regarding the management of parathyroid disorders in which they state that persistent hypoparathyroidism should be diagnosed if active vitamin D analogues are still necessary to maintain calcium concentrations low normal. They also recommend to confirm the chronicity by carefully tapering active treatment. 21 When utilizing our definition of hypoparathyroidism, lower postoperative serum calcium, parathyroid gland autotransplantation, and the occurrence of surgical complications were found to be independent risk factors for persistent hypoparathyroidism.
The herein reported rate of persistent hypoparathyroidism is high compared to single-center studies applying the definition of using active vitamin D analogue only. For example, a single-center study by Almquist et al. 22 reported an incidence rate of 1.9%, while we found an incidence of 11.8% when applying the same definition. Furthermore, nationwide and multicenter studies reported higher incidence rates up to 5.2%, using this definition, yet this is not as high as in this study.5,23 Studies that used the definition of calcium and/or active vitamin D analogues use, 12 months postsurgery without any confirmed attempt to stop this medication reported higher incidence rates. A nationwide population-based cohort study from Sweden reported an incidence rate of 12.5%; however, only patients with benign disease were included. 12 Differences in incidence rates might not only be explained by the definitions used for hypoparathyroidism but also by the included population. In this study, more than half of the patients underwent surgery for malignant disease of whom 20.4% underwent lymph node surgery. This might explain the relatively high incidence of hypoparathyroidism, which is about equal to the finding by Diez et al. 10 who reported an incidence of hypoparathyroidism of 16.7% in a population comparable to ours.
Influence of definition on incidence of hypoparathyroidism
Previous studies have investigated the influence of the use of different definitions on the incidence of hypoparathyroidism. Mehanna et al. 16 described that the incidence of persistent hypoparathyroidism varied from 0.9% to 4.4% when different definitions were applied. On the contrary, a study by Harsløf et al. 17 did not find an association between the incidence rate and the use of different definitions. However, they did express their concern regarding the wide variety of definitions that are used across studies which might be linked to confounding factors affecting the reported incidence of hypoparathyroidism. All definitions for hypoparathyroidism that were applied in this study were defined solely by a clinical parameter: the use of active vitamin D analogues with or without calcium supplements 1-year postsurgery. Serum calcium and PTH levels were not part of the definitions, which makes this definition pragmatic to use and enhance the comparability of hypoparathyroidism rates between different centers.
The discrepancy in incidence between the groups with and without any attempt to wean off supplementation (a difference of 16.0%) implies that a significant proportion of our patients might use unnecessary supplementation 1 year after surgery. This highlights the importance of the implementation of a standardized and uniform protocol for weaning off medication, especially if only calcium supplements are prescribed. Unfortunately, to date, there is no worldwide consensus on such a treatment algorithm, and it is to be expected that overtreatment is not solely a problem in the Netherlands. However, data on this topic are lacking. Furthermore, by including only the use of calcium in the definition, patients receiving supplementation for another indication are defined as having hypoparathyroidism which increases the incidence rate. To our knowledge, this is the first study including patients with an inability to wean off vitamin D and calcium supplementation which is different from most studies including patients based on serum PTH levels in their definition of hypoparathyroidism.24 –26 Nevertheless, a normal PTH level does not preclude the occurrence of hypocalcemic symptoms necessitating supplementation.25,27,28 As discussed previously by Lorente-Poch et al., 28 hypoparathyroidism could be subclassified into aparathyroidism (undetectable PTH levels), hypoparathyroidism (detectable but subnormal PTH levels), and relative parathyroid insufficiency (normal PTH levels but insufficient to maintain calcium levels). This is highly suggestive for heterogeneity of persistent hypoparathyroidism, which makes it all the more difficult to reach consensus regarding the definition. Also, this could partly explain why some patients will never be tapered off medication. Furthermore, PTH levels are not measured routinely in the participating centers of this study. Also, national investigation shows that PTH levels are not measured in standard protocols. 29 We therefore propose the use of our pragmatic and clinical definition without the use of serum PTH levels, to enable worldwide and unbiased comparison of incidence rates. Yet, it should include the effort of the clinician to wean off supplementation, which should also be standardized.
Risk factors of persistent hypoparathyroidism
In this study, we found that lower serum calcium level on the first postoperative day is an independent risk factor for persistent hypoparathyroidism, which confirmed a previous finding in a meta-analysis. 14 Moreover, parathyroid autotransplantation was found to be an independent risk factor for persistent hypoparathyroidism. However, the influence of autotransplantation on persistent hypoparathyroidism is still debated. Some studies have found that it may prevent hypoparathyroidism on the long term or found no association at all.6,22,30 However, others reported autotransplantation as a risk factor of persistent hypoparathyroidism, which is in line with our results.12,31 Parathyroid tissue on pathology report was not found to be an independent risk factor for persistent hypoparathyroidism. However, in nearly one quarter of the patients, parathyroid tissue was found on histology, which is comparable to the 22.7% found by Diez et al. 10 and the 29.0% incidence of inadvertent parathyroid gland resection found by Paek et al. 31 Although, comparable to the literature, the incidence of inadvertent parathyroid gland resection in our cohort is substantial and future research should focus on developing new techniques for the surgical preservation of parathyroid glands. It is hypothesized that lymph node surgery increases the risk of inadvertent parathyroid gland removal or damaging the parathyroid gland, and therefore increases the risk for persistent hypoparathyroidism.10,15 In this study, there was no statistically significant association between CLND and persistent hypoparathyroidism on univariate analysis, while there was an association for CLND ± LLND and CLND + LLND. This could be explained by insufficient power for CLND, but also by the higher risk for parathyroid gland damage when an LLND is performed. However, on multivariable analysis, no association was found for any type of lymph node dissection. The occurrence of surgical complications was an independent risk factor for persistent hypoparathyroidism which could partially be explained by reoperation for bleeding, as described previously. 30
Limitations
This study is a non-randomized, retrospective study, and despite the care of data collection and the use of clear inclusion criteria, observation bias cannot be ruled out. Second, the number of cases precluded an extensive multivariable analysis. Finally, serum PTH levels were not available, and therefore, the use of PTH in a definition could not be compared to our pragmatic definition.
Conclusion
Our data show that the incidence of persistent hypoparathyroidism in the literature may vary through the use of different definitions. This study indicates that a new pragmatic definition of persistent hypoparathyroidism, solely based on clinical parameters and in alignment with all current guidelines for hypoparathyroidism management, has the potential to enable unbiased and universal comparison between studies.
Footnotes
Acknowledgements
The authors thank all the medical representatives of all participating hospitals of the Thyroid Network.
Author contributions
I.L. and C.M.J.v.K. contributed to the study design, data collection, analysis and interpretation of data, and manuscript draft. S.P.J.v.D. contributed to the data collection, interpretation of data, and critical review. G.J.H.F., E.E.V., and C.J.H.v.E. contributed to the interpretation of data and critical review. R.P.P. and C.v.N. contributed to the study design, interpretation of data, and critical review. T.M.v.G. contributed to the study design, interpretation of data, manuscript draft, and critical review. All authors reviewed the results and approved the final version of the manuscript.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request, without undue reservation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Shire International GmbH, a Takeda company (Investigator Initiated Research Grant (no. IIR-NLD-001380) awarded to Dr T.M. van Ginhoven).