Context and Relevance
Botulinum toxin (BTX) has been studied for a variety of uses. The published literature demonstrates that BTX is beneficial in a wide range of non-cosmetic conditions. Currently, BTX is approved for treating blepharospasm, strabismus, hemifacial spasm, cervical dystonia, spasticity, chronic sialorrhea, overactive bladder, and axial hyperhidrosis. BTX is however used to treat many other non-cosmetic conditions even without European Medicine Agency (EMA) approval. This narrative review provides an overview of both off- and on-label non-cosmetic treatment of BTX in surgical conditions.
Introduction
The therapeutic use of botulinum toxin (BTX) was recognized when Alan B. Scott published his data on the BTX effect on strabismus in the 1980s.
1
Since then, it has been widely used and especially become very popular in cosmetic treatments. In recent years, the use of BTX has however increased to also include treatment of several medical and surgical conditions, often without approval of the European Medicine Agency (EMA).
BTX is a neurotoxin inducing a fully reversible blockade of the cholinergic synapses and thereby it inhibits the release of acetylcholine. When injected intramuscularly, BTX causes muscle relaxation/paresis.
2
Moreover, BTX affects the cholinergic autoimmune nervous system impairing production of sweat, tears, saliva, and causes paralysis of smooth muscle.
2
BTX inhibits norepinephrine, substance P and glutamate, which reduces pain sensitization, thus making BTX an effective agent for treatment of pain.
2
BTX also inhibits fibroblast-to-myofibroblast differentiation in vitro, and this indicates a potential use in treating wounds that are expected to develop into hypertrophic scars after trauma, burns, or surgery.
3
There are seven serotypes of BTX named A-G.
2
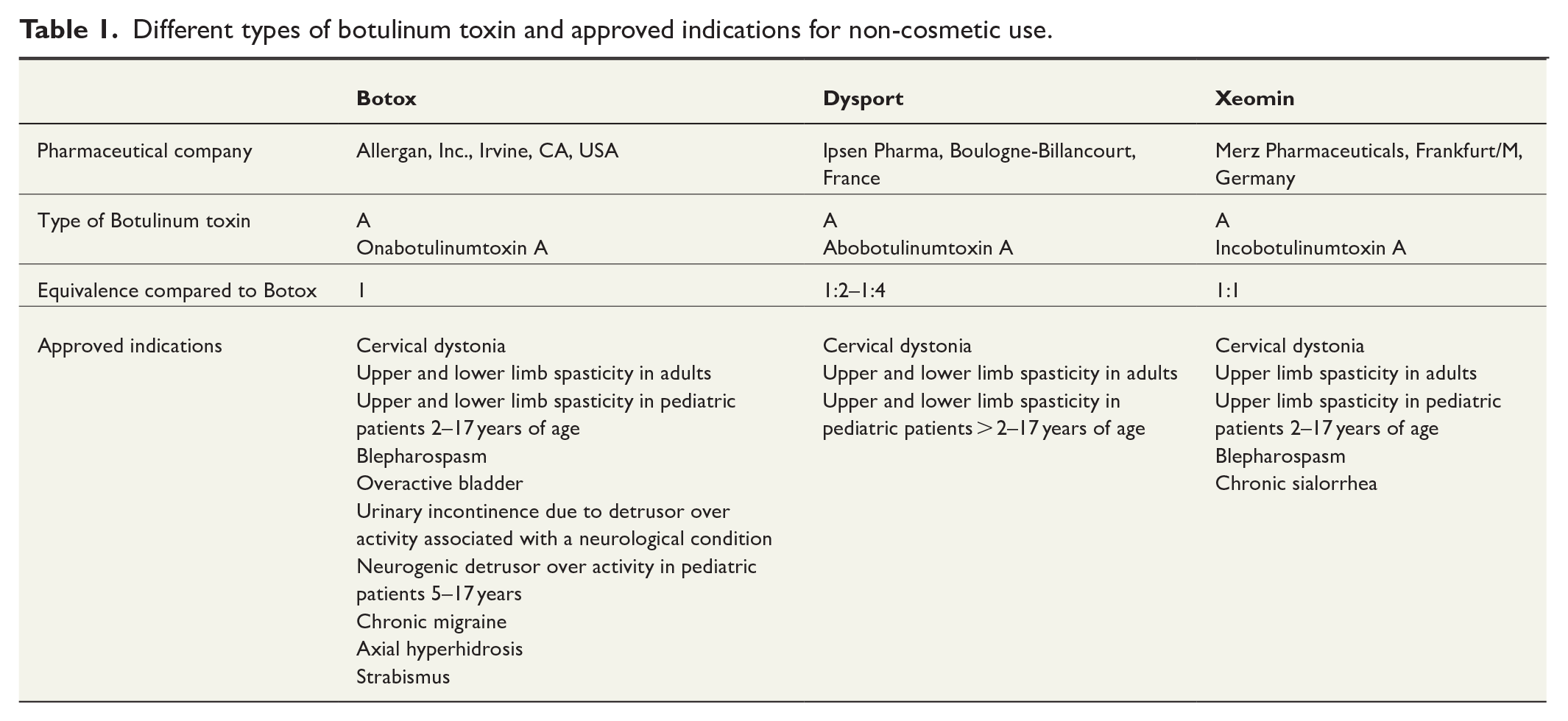
In medical treatment, BTX type A is preferred, of which there are three different types (Botox®, Xeomin®, and Dysport®) available in the European Union for treatment of non-cosmetic disorders (Table 1).
4
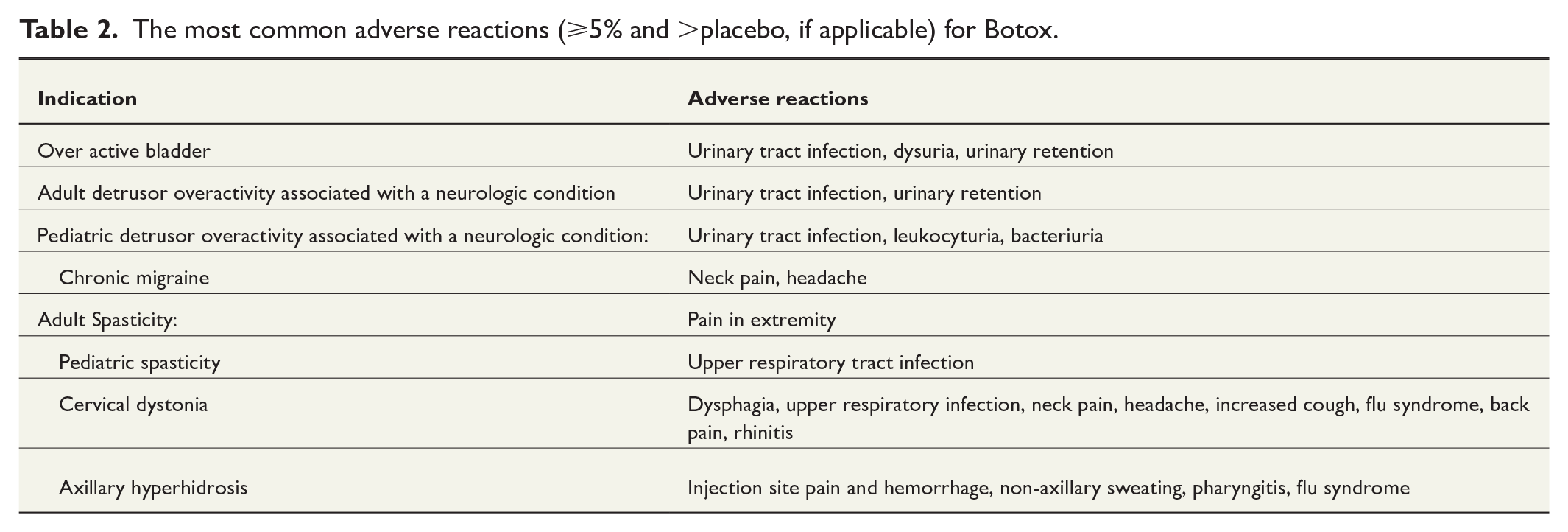
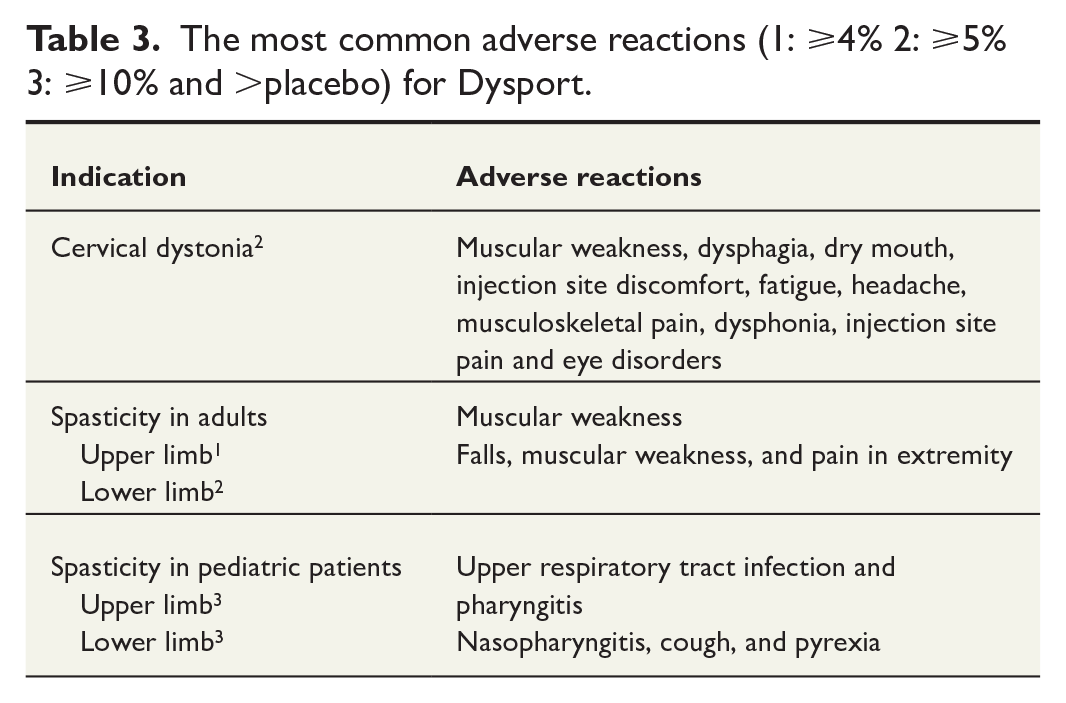
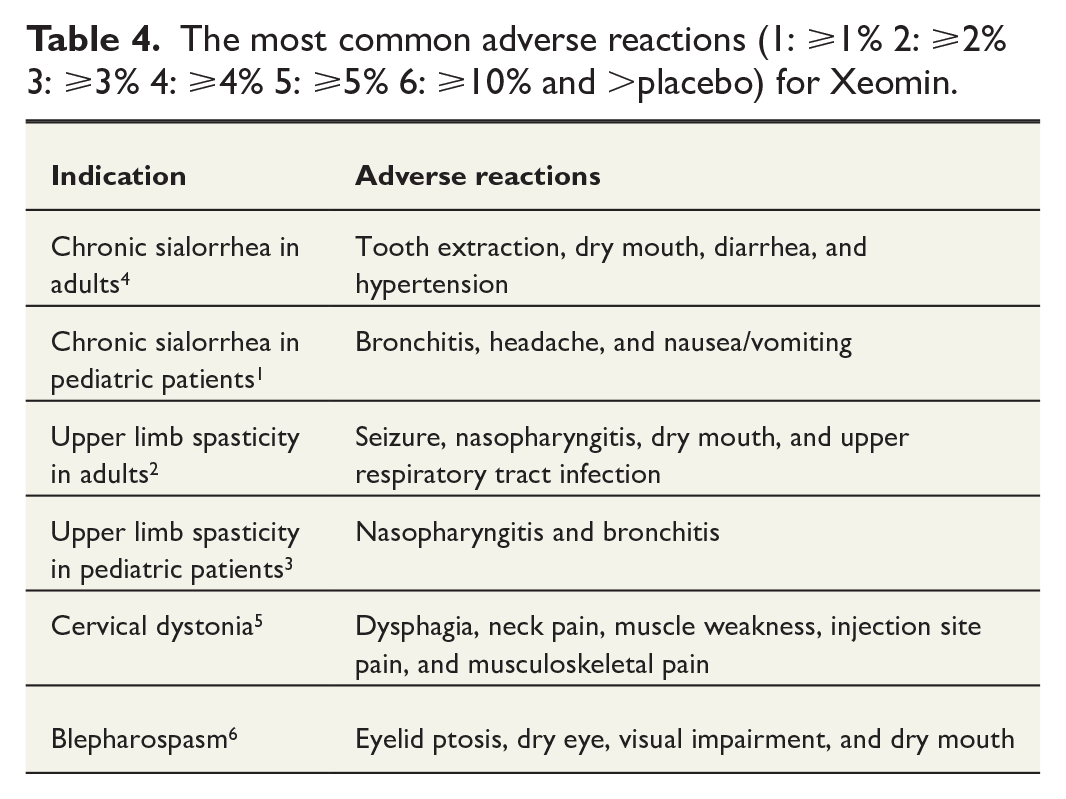
BTX is approved for a few non-cosmetic conditions (Tables 2–4).5–7 Most of these are neurological conditions. Because of BTX’s ability to cause muscle relaxation/paresis, it is used to treat spasticity in patients with multiple sclerosis (MS), infantile cerebral palsy (CP) and in patients with cerebral injuries (i.e., after stroke and trauma).
2
These abilities for BTX are also used to treat dystonia, here among blepharospasm and cervical dystonia.8,9 Moreover, it is used to treat chronic migraine due to its ability reduce pain sensitization.
10
BTX can impair the production of sweat and saliva and is therefore used with great success to help patients with sialorrhea/excessive drooling. This is a condition associated with several neurological diseases such as Parkinson disease, amyotrophic lateral sclerosis (ALS), and CP.
11
BTX is also used in the dermatological condition of primary axillary hyperhidrosis.
12
BTX is generally considered to be safe and tolerable across a spectrum of therapeutic applications. The most common adverse reactions per indication are listed in Tables 2–4.5–7 Adverse events can however occur and are more likely to occur during therapeutic use compared to cosmetic use.
13
Injecting toxin to non-planned sites has been reported to cause a variety of side effects such as double vision, ptosis, dysphagia, limb weakness among others.
14
Antibody-induced treatment failure has also been described.
15
Although rare, pharmacovigilance data and case reports imply that BTX may be associated with serious adverse events such as botulism, generalized paralysis, respiratory depression and death.
14
The BTX effect is reversible and it is common that the treatment must be repeated.
4
Re-injections with BTX should not occur at intervals of less than 12 weeks.5
–7
The indication for the use of BTX is rapidly expanding. The purpose of this narrative review article is to provide a brief overview of the most frequent non-cosmetic treatments with BTX in surgical conditions.
Oto-Rhino-Laryngology
Frey’s syndrome, also called gustatory sweating, is characterized by redness and sweat secretion on the cheeks and temples while eating. The condition can occur after surgery on the major salivary glands causing salivary gland nerves to infiltrate the sweat glands of the skin. BTX injection to the affected skin area is the first line of treatment that has a long-lasting and sometimes curative effect.
16
Beerns and Snow investigated the BTX effect on 13 patients with Frey’s syndrome. After 3 months, 11 of 13 patients showed decreased gustatory sweating of more than 90%.
17
Ophthalmology
Strabismus is an impairment of the ocular alignment causing the axes of the eyes to deviate. This can lead to double vision and reduced vision of the affected eye because suppression of visual impression. Strabismus can be divided into esotropia (in-turning deviation), exotropia (out-turning deviation) or less commonly, hypertropia (up-turning deviation).
18
The treatment is glasses and in some cases surgery.
BTX is an approved treatment and can be used as an alternative.
18
BTX is injected into the shortened extra ocular muscle causing the deviation. Initially, there will be an overcorrection with contraction of the antagonist and weakening of the paralyzed muscle, which may persist after the effect of BTX disappears, thus creating a more permanent effect on ocular alignment.
19
Mayet et al. compared BTX injections to surgery in children with infantile esotropia. They found that the proportion of children who achieved a complete response was significantly higher in the surgery group compared to the BTX group. They concluded that surgery remains the gold standard for treatment. BTX injection, however, is a safe alternative.
20
Maxillofacial surgery
Temporomandibular joint disorders (TMDs) are a group of conditions that cause pain and dysfunction in the temporomandibular joint and the muscles of mastication. TMDs have a multifactorial etiology such as genetics, arthritis, or jaw injury. Initial treatment is conservative with soft diet, home exercises, non-steroidal anti-inflammatory medications and occlusal splints for bruxism. Surgery is indicated if conservative treatment fails, and the patients have severe pathology in the temporomandibular joint.
21
Owing to its reduction of muscle activity and pain-relief effects, BTX is increasingly being used to treat muscle-related diseases associated with TMD, but it is still controversial. In a double-blinded randomized control trial, 21 patients with TMD associated with masticatory muscle pain (MMP) and headache received either BTX or saline injections. The trial showed a significant decrease in pain and trigger points after 4, 8, and 12 weeks.
22
Thoracic surgery
Thoracic outlet syndrome (TOS) is defined by a group of symptoms caused by neurovascular compression in the thoracic outlet. Depending on the compressed structure, TOS can be divided in three subtypes: arterial TOS, venous TOS, or neurogenic TOS (NTOS). Diagnosis and treatment of TOS remains challenging. Surgical decompression of the thoracic outlet, commonly achieved by first rib resection and scalenectomy, is thought to be the ultimate therapeutic option.
In the recent years injections with BTX in the anterior scalene muscle, middle scalene muscle or pectoralis minor muscle has been suggested as a minimally invasive technique and as a diagnostic tool for NTOS as symptom relief confirm the etiology.
23
There is limited quality evidence on BTX efficacy on TOS. In a randomized control trial, it was shown that 11 (55%) patients reported symptom reduction after primary BTX injection compared to 7 (39%) in the placebo group. This was however not statistically significant
24
and should be verified in larger trials.
Orthopedic surgery
Chronic lateral epicondylitis (chronic tennis elbow) is characterized by functional impairment and chronic pain around the lateral epicondyle persisting for more than 1 year. It is one of the most common musculoskeletal disorders and occurs in 1%–3% of the population.
25
The condition might get better without treatment and have a self-limiting nature. Analgesics, relief and physiotherapy are primary treatment. In patients with persistent pain for more than 1 year, BTX can be effective when injected into the extensor tendon attachment.
25
In a randomized control trial including 57 patients, it was shown that BTX injections into the extensor carpi radialis brevis led to a significant decrease in pain and gave positive effect on quality of life compared to the placebo group.
26
Plantar fasciitis is degeneration and inflammation of the plantar fascia at its insertion of the calcaneus bone. Plantar fasciitis can be caused by a number of factors, including type of shoes, foot structure, overuse, and types of walking surfaces. A typical symptom of plantar fasciitis is heel pain.
27
Conservative treatment is often the primary approach. In some patients, surgery is considered, but might be challenging with risk of complications.
27
BTX has shown to be efficient to treat patients with plantar fasciitis. A meta-analysis indicated that pain relief was sustained at 12 months after BTX injections.
28
Late diagnosed ruptures or re-ruptures of muscle tendons are often disabling injuries and have a complex character. The cases often require specialized surgery and rehabilitation.
29
The focus during surgery is to ensure a strong fixation of the tendon, to avoid tendon gap or a new rupture during rehabilitation. BTX can be injected into the muscle connected to the tendon perioperatively. This means that the muscle can only function with reduced force thus avoiding the peak of muscle contraction. This helps protect the tendon sutures for a few months during the healing and rehabilitation period.
30
Perioperative BTX treatment may also be beneficial in the late-detected shortened tendon rupture.
30
A systematic review of flexor tendon rupture repair in the hand, shows there were no cases of re-rupture, or adhesions reported. The conclusion was that BTX therapy is a safe and efficacious augmentation to flexor tendon repair.
31
Chronic compartment syndrome in the lower leg is characterized by activity-induced massive pain and swelling in one or more muscle compartments with simultaneous increased intramuscular pressure above normal physiological range.
32
It is often diagnosed and treated with both patient and doctors delay because of difficult differential diagnosis. Conservative treatment might be attempted but the primary treatment is mainly surgical fasciotomy of the affected muscle compartment.
32
Patients who do not tolerate surgery or who do not have an effect from fasciotomy might have a beneficial effect from BTX intramuscular injections. In a case series, 16 patients were treated with BTX injections in the anterior or lateral compartment of the leg. BTX reduced the pressure and pain, and the effect lasted for up to 9 months.
33
Piriformis syndrome is a condition with buttocks and posterior hip pain with limited articular range of motion caused by prolonged or excessive contraction of the piriformis muscle. The sciatic nerve can be compressed or injured by the scar tissue of the piriformis muscle, which gives a sciatic-like pain. Conservative strategies include stretching exercises, massage, physical therapy, non-steroidal anti-inflammatory drug (NSAID), and muscle relaxant. If this fails local injection of piriformis muscle, surgery and trigger-point injections with local anesthetic with or without corticosteroids is the next line of treatment.
34
In recent years, BTX has emerged as a new therapeutic option. In a retrospective cohort study including 97 patients, injections with bupivacaine and lidocaine with or without BTX was compared. The BTX group had a longer duration of response with a median of 30 days compared to the non-BTX group with a median of 1 day.
35
Cerebral palsy (CP) is a result of damage to the developing brain, which results in disorder of movement and posture that is permanent and progressive. CP is the most common cause of physical disability affecting children in developed countries.
36
New management strategies are described, in which spasticity management by intramuscular injections of BTX and deformity correction, by orthopedic surgery are combined.
36
Patients with CP with classic toe walking, due to spastic contraction in the Achilles tendon on both sides can be treated with BTX injections in the flexor muscles of the lower leg as an alternative or adjunct to surgery with tenotomies of the Achilles tendons.
37
Gastroenterology
Achalasia is a motility disease in the esophagus characterized by reduced peristalsis in the distal 2/3 of the esophagus and lack of relaxation in the lower oesophageal sphincter. Patients experience gradually increasing dysphagia. The treatment is balloon dilatation or myotomy, which can both be done laparoscopically ad modum Heller or as a per-oral endoscopic myotomi (POEM). In patients who do not meet the diagnostic criteria or where surgery is contraindicated, injection with BTX into the oesophageal sphincter can be offered.
38
Injections with BTX are suggested to be a safe and effective way to treat patients with achalasia and that the effect is sustained for several months.
39
A double-blinded randomized control trial including 21 patients showed a decrease in the pressure of the lower oesophageal sphincter of 33% in the treatment group, as compared with a mean increase of 12% in the placebo group after 1 week. Overall, 67% of the patients treated with BTX were still in in remission after 14 months.
40
Gastroparesis is a condition resulting from delayed gastric emptying in the absence of mechanical obstruction. It can interfere with normal digestion, cause nausea, vomiting, weight loss, and pain. These symptoms have a huge impact on patient quality of life. The most common aetiologies are idiopathic (64%), diabetes (31%), and post-surgical. Dietary modifications to restore fluid and electrolyte balance is the initial goal of treatment. To help relieve symptoms prokinetics like metoclopramide, erythromycin, and anti-emetics can be used. If the patient is refractory to medical therapy, intra-pyloric injection with BTX can improve symptoms for about 3–6 months.
41
Surgical treatments include venting gastrostomy, feeding jejunostomy, pyloroplasty, and partial gastrectomy that can be performed when medical therapy fails.
41
In a retrospective review of prospectively collected data including 204 patients who underwent either laparoscopic pyloroplasty or gastric peroral endoscopic myotomy (G-POEM), it was shown that patients who received BTX prior to surgery were 3.2 times more likely to improve postoperatively.
42
Large ventral hernias are a challenging to operate on, as prolonged muscle retraction and contracture can make it difficult to close the fascia. Moreover, loss of domain is often observed in which a large part of the abdominal cavity content lies outside the hernia. Reducing the hernia content and closing the fascia can lead to an increase in intra-abdominal pressure a state also known as abdominal compartment syndrome, which can be a fatal condition if not treated. By using BTX injections to paralyze the oblique and transverse muscles, the abdominal wall cavity will increase. This will make suturing of the fascial defect easier and reduces the intra-abdominal pressure.43,44 Buenu-Liedó et al. used preoperative BTX injections combined with progressive pneumoperitoneum in patients with large ventral hernias with loss of domain. They found that the combination of BTX and progressive pneumoperitoneum increased the abdominal cavity and thereby showed this to be a useful tool for preoperative optimization.
45
Chronic anal fissure is a fissure in the distal part of the anal canal that extends below the linea dentata. The fissure causes pain during defecation. Spasms in the internal sphincter muscle makes it difficult for the fissure to heal. The initial treatment is constipation prophylaxis and local treatment with ointment containing glyceryl nitrate or calcium antagonists. BTX injections into the internal sphincter can be attempted if primary treatment fails or at relapse.
46
Other methods of treating chronic anal fissure are with lateral internal sphincterotomy (LIS). In general LIS is a more effective than BTX but with a higher risk of incontinence.
47
In a randomized controlled trial, 50 patients with chronic anal fissure were randomly treated with either LIS or BTX. The results showed that there was a higher recurrence rate after 12 months in the BTX group (50%) compared to the LIS group (8 %), but the LIS group had a significant higher rate of anal incontinence (4% vs 0%).
48
ACNES (Anterior cutaneous nerve entrapment syndrome) is distinct pain in the abdominal wall, where anterior cutaneous branches from an intercostal nerve are pinched between the muscles in the abdominal wall. This condition is very rare, and there is a lack of evidence, but BTX seem to have an effect both in the treatment and as part of the diagnostics before possible neurectomy.
49
Urology
Overactive bladder (OAB) is diagnosed in the absence of urinary infection and is characterized by urgency, a sudden urge to urinate and inability to postpone voiding, with or without incontinence. Moreover, OAB causes daytime frequency, as well as nocturia, frequent passing of urine during the night. It can occur based on a neurogenic detrusor overactivity or idiopathic detrusor overactivity. Initial management includes lifestyle modifications and physical therapy. Second-line treatment is oral anticholinergics or β3-adrenergic agonist.
50
If first- and second-line treatment fails, transurethral injections of BTX into the detrusor-muscle of the bladder may be indicated.
51
A randomized controlled trial investigating patients with neurogenic detrusor overactivity and idiopathic detrusor overactivity receiving BTX injections versus placebo showed significant reduction of urinary incontinence episodes and improvement in quality of life compared to placebo.
52
Interstitial cystitis also known as painful bladder is characterized by reduced bladder emptying, urethral pressure, and residual urine pressure. Symptoms are increasing pain with increased bladder filling as well as increased urinary frequency without infection and often pain-relief when voiding. The etiology is unclear.
53
Conventional therapies include lifestyle-changes, different oral treatments or intravesical installation with hyaluronic acid or heparin.
53
Current evidence supports that BTX injection can improve symptoms and reduce pain compared to placebo.
54
Benign prostatic hyperplasia (BPH) is a common condition and the main reason for obstructive lower urinary tract symptoms (LUTS) in older men. When changes in lifestyle, nutrition and weight loss fail to improve symptoms, oral 5-α-reductase inhibitors and α-adrenergic blockers are first-line medical treatments.
55
If medical treatment fails surgical methods are available. These include transurethral resection of the prostate, transurethral microwave treatment, prostate artery embolization, and are all well established for relief of LUTS.
55
BTX injections have been suggested as a minimally invasive procedure for patients with BPH and LUTS. In a study, 41 men received BTX injections into the prostate resulting in an improvement in LUTS and quality of life in 76% of the patients.
56
Other studies have shown no differences in the efficacy between BTX and a placebo.
57
The therapeutic role of BTX in patients with BPH remains to be established.
Plastic surgery
Scar formation is one of the physiological processes of wound healing in the deepest part of the damaged dermis. Hypertrophic scars and keloids are formed as the muscles pull the edges of the wound while the collagen fibers of the skin are still immature. Temporarily paralyzing the muscles around the wound with BTX is a newer method used in reconstructive surgery.
58
In a prospective randomized controlled trial including 15 patients undergoing mastectomy, BTX was shown to reduce the severity of postoperative scar formation and to enhance the overall appearance of scars.
59
In another prospective randomized controlled trial including 22 patients undergoing cleft lip surgery, BTX-treated patients had a statistically significantly better visual analog scale (VAS) score and lesser scar width compared to the control group.
60
Discussion
BTX has proven to be an effective treatment for a wide range of non-cosmetic disorders. The EMA and the US Food and Drug Administration (FDA) have however only approved the use of BTX for few conditions (Tables 1 and 2).5
–7
Few side effects and the fact that the treatment with BTX is typically reversible have led to testing BTX for the treatment of conditions that have traditionally been difficult to treat. The conditions are often relatively rare, and therefore, it is difficult to obtain relevant high-level evidence. To assess patient safety and expand or restrict treatment indications, it should however be mandatory to perform such testing within clinical trials and with protocolled data collection.
Treatments with BTX are often described in the literature to be safe. Most data about adverse events are generated from case reports, retrospective studies, and spontaneous reporting systems. There is a great need for larger studies on the adverse events and on the long-term safety of BTX. Thorough knowledge of the anatomy of the treated muscles and of the pharmacology of the drug is imperative to avoid serious adverse events.
There is ongoing research into various areas of the use of BTX in non-cosmetic treatment within many surgical specialties. New research suggests that BTX can be used to reduce the local pain experience in cancer patients after surgery or radiotherapy.
61
There is also an on-going study for BTX indication in treating open abdomen. The hypothesis is being that BTX relaxes the abdominal wall musculature to ensure better and faster closure, a study inspired from results using BTX in large ventral hernias.
62
A recent phase I/II prospective study has moreover shown promising results for prevention of post-surgical pancreatic fistula when BTX is injected intrapapillary after distal pancreatectomy. No clinically relevant fistulas were observed in BTX-treated patients compared to 33% postoperative pancreatic fistula in control patients.
63
Based on this observation an on-going study is investigating the efficacy for prevention of post-operative pancreatic fistula if BTX is injected intrapapillary during an endoscopic procedure before pancreatic surgery.
64
BTX has also been suggested to suppress atrial fibrillation (AF) after cardiac surgery. In a double-blinded randomized controlled trial, 60 patients received either BTX or saline injections into the epicardial fat pads during coronary artery bypass graft (CABG) surgery. The incidence of early postoperative AF within 30 days after CABG was 2 of 30 patients in the BTX group and 9 of 30 patients in the placebo group. Seven of the 30 patients in the placebo group, and none of the 30 patients in the BTX group had recurrent AF after 1 year.
65
A new study found a lower rate of AF in patients ⩾65 years undergoing CABG and receiving BTX injections into the epicardial fat pads during surgery.
66
BTX has been studied for treatment of osteoarthritis. A meta-analysis looking at the efficacy and safety of intra-articular BTX for knee osteoarthritis including six randomized controlled trials, the results suggested that intra-articular BTX has the same efficacy as corticosteroid, while BTX may be superior to hyaluronic acid.
67
Its analgesic properties and the reported safety make intra-articular BTX a candidate to also treat other forms of osteoarthritis. There is an on-going randomized controlled trial investigating the assessment of pain after intra-articular BTX injections in carpometacarpal osteoarthritis of the thumb.
68
In Scandinavia injection treatments of the joints is very controversial, because of the risk of septic arthritis. Physical therapy and weight loss would normally be the first step before considering knee alloplastic. BTX has also been shown to be effective in the treatment of burn itching. In a prospective study including 10 patients with deep partial thickness to full thickness burns, they all received injections with BTX. At baseline, 87.5% of patients rated their burns itch as being severe (> 7 on the pain scale). This fell to 0 out of 10 at 4 weeks after BTX treatment. The average duration of the symptom free period was 9 months.
69
There is an on-going randomized controlled trial investigating the use of BTX in the treatment of itching from hypertrophic scar.
70
As discussed in this review, BTX injections have an enormous therapeutic potential, and indications are likely to increase. This, however, requires effectively performed studies and preferable randomized controlled trials as well as long-term follow-up of patients.