
Abstract
Backgrounds and aims:
We aimed to determine the incidence and severity of spine injuries among severely injured trauma patients (Injury Severity Score (ISS)/New Injury Severity Score (NISS) > 15) treated in a single tertiary trauma center over 15 years. We also wanted to compare the demographics between patients with and without spine injuries and to determine the mortality of spine-injury patients.
Methods:
Data from the years 2006–2020 from the Helsinki Trauma Registry (HTR), a local trauma registry of the trauma unit of the Helsinki University Hospital (HUH), were reviewed. We divided patients into two groups, namely those with traumatic spine injury (TSI) and those without traumatic spine injury (N-TSI). TSI patients were further subdivided into groups according to the level of injury (cervical, thoracolumbar, or multilevel) and the presence of neurological symptoms.
Results:
We included 2529 patients: 1336 (53%) had a TSI and 1193 (47%) had N-TSI. TSI patients were injured more frequently by a high-fall mechanism (37% vs 21%, p < 0.001). Among TSI patients, 38% of high-fall injuries were self-inflicted. High falls, young age, and female gender were overrepresented in spine-injury patients with a self-inflicted injury mechanism. Cervical spine-injury patients were mostly elderly persons injured by a low-energy mechanism.
Conclusions:
Unlike other severely injured trauma patients, severely injured trauma patients with spine injuries are more frequently injured by a high-fall mechanism and self-injury.
Context and relevance
Although there is considerable available research on spine injuries, there are few studies focusing on spine injuries in severely injured patients (Injury Severity Score/New Injury Severity Score > 15). Severe spine injuries have an additive effect on mortality and can have a major impact on quality of life. These injuries are costly to society in terms of healthcare expenses, social security expenses, and loss of working ability. Our study revealed that young women with a self-inflicted or suicidal injury mechanism (especially high-fall mechanism) are overrepresented among thoracolumbar spine-injury patients and elderly people injured by a low fall among cervical spine injuries. Targeted preventive methods, namely mental health programs and prevention of falls, should be considered for these cohorts.
Introduction
Spine injuries include a wide range of injuries that affect the bony, ligamentous, or neural structures of the spine. They can be severe injuries of severely injured patients due to high-energy trauma or osteoporotic fractures of an elderly patient with no detectable traumatic event. Despite the rising number of osteoporotic fractures of elderly, mostly female patients, spine injuries still often occur in working-age men.1–16 Motor-vehicle accidents and falls are the most common injury mechanisms.1,2,4–18 Spine injuries account for 6%–18% of all injuries.2,5,12 When considering major trauma patients (Injury Severity Score (ISS)/New Injury Severity Score (NISS) > 15), spine injuries occur in 20%–46% of these patients, and the mortality of these patients is 4.0%–7.8%.3,19–21
Spine injuries have an additive effect on mortality and can have a major impact on patient recovery and quality of life, especially if surgery is needed or neurological deficits are present due to injury of the spinal cord.2,6,22,23 There are limited data on the incidence of spine injuries with neurological symptoms among severely injured trauma patients (ISS > 15). In one previous study, neurological deficits were reported among 32% of spine-injury patients with major trauma. 21 Among severely injured trauma patients, spinal injury increases hospital length of stay even without initial neurological symptoms. 24 Spine trauma is often accompanied with injuries of the head, thorax, and extremities, which is predictive of poor outcome in previous studies.2,14 Spine injuries are costly to society in terms of healthcare expenses, social security expenses, and loss of working ability.18,25
Although there is an extensive body of research on spine injuries, there are few studies focusing on spine injuries in severely injured trauma patients (ISS/NISS > 15).3,20,21 Hence, further research on severely injured trauma patients with spine injuries is warranted to increase knowledge and to improve treatment, injury prevention, and cost savings related to these injuries.
The aim of this study was to determine the incidence and severity of spine injuries among severely injured trauma patients treated in a tertiary trauma center over 15 years. We also wanted to compare the demographics between patients with and without spine injuries and to determine the mortality of spine injury patients.
Methods
Data were collected from the Helsinki Trauma Registry (HTR). The HTR is a local trauma registry of the trauma unit of the Helsinki University Hospital (HUH).26–28 The HUH trauma unit is responsible for treatment of severe injuries of adults (age > 15 years) in Southern Finland. It is one of the largest tertiary trauma centers in Northern Europe, with a catchment area of 1.8 million people at the time of this study. Penetrating injuries were treated in another unit during the study period. The HTR was founded in 2005 and registry data are available since the beginning of 2006. The inclusion criterion of the HTR was ISS > 15 until the end of year 2011 and NISS > 15 since 2012. The exclusion criteria are > 24 h since the injury, asphyxia, and drowning. Every patient treated in the HUH trauma unit is included in the registry if the criteria are fulfilled.
We reviewed the HTR data from 2006 to 2020. We excluded patients dead on arrival (with no signs of life), patients < 16 years, patients with isolated burn injuries, and patients with isolated head injuries (defined as head Abbreviated Injury Scale (AIS) ⩾ 3, no other AIS ⩾ 2 injury). 29 Due to the change of the inclusion criterion of the HTR since the beginning of 2012 (the previous inclusion criterion was ISS > 15 and subsequently NISS > 15), we also excluded patients with ISS score < 16, thus all included patients had ISS score > 15 (and NISS score > 15 as well). Hence, all groups were comparable throughout the entire study period. All included patients were treated at the HUH trauma unit.
AIS is an injury score that classifies every injury on a scale from 1 to 6 according to injured body region. 30 AIS score 1 refers to a minor injury (such as spinous ligament injury) and 6 is a lethal injury. AIS scores ⩾3 are considered severe injuries. In spinal trauma, AIS score 3 could refer to, for example, spinal cord contusion or major compression fracture of vertebral body with >20% loss of anterior height. NISS and ISS scores are calculated based on the patient’s AIS scores and range from 0 to 75. ISS score is calculated by the sum of squares of patient’s three highest AIS injury scores of three different body regions. NISS is calculated the same way, except that the three AIS scores do not have to be from different body regions. NISS and ISS scores > 15 are considered as severe trauma.
We divided included patients into two main groups based on AIS codes from the HTR, namely those with traumatic spine injury (TSI) and those without traumatic spine injury (N-TSI). Diagnosis of TSI was based on whole body computed tomography (CT) scans. Magnetic resonance imaging (MRI) was also performed as relevant regarding neurological symptoms. TSI patients were further subdivided into groups according to level of injury (thoracolumbar, cervical, or multilevel) and the presence of neurological symptoms based on each patient’s AIS codes. If a patient had any AIS spine code that includes neurological symptoms of any degree, the patient was considered as having neurological symptoms due to the spine injury. To investigate changes in injury patterns over time, we also divided TSI patients into three time groups based on year of the injury (2006–2010, 2011–2015, 2016–2020).
The STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) Guidelines for reporting observational studies were followed. 31
Statistical analyses
We performed statistical analyses to compare differences between groups. The tested variables included patient age and sex, time period of injury (2006–2010, 2011–2015, or 2016–2020), presence of spine injury (yes or no) and level of possible spine injury (cervical, thoracolumbar, or multilevel), AIS score of spine injury (1–2, ⩾3, or ⩾5), NISS score, American Society of Anesthesiologists (ASA) score (1–2 or 3–4), occurrence of in-hospital death during the first 30 days (after discharge no deaths were recorded), occurrence of neurologic symptoms due to the spine injury, possible purposefulness of the trauma (self-inflicted or other), and injury mechanism. A high fall was defined as falling above one’s own height. NISS scores were used instead of ISS scores because NISS is a better predictor of mortality for blunt trauma patients than ISS. 32
We analyzed the distributions of continuous variables (age, NISS score) with Kolmogorov–Smirnov and Shapiro–Wilk tests. As the distributions were non-normal, we used the nonparametric Mann–Whitney U test for comparisons of two groups. When more than two groups were compared, we used the Kruskal–Wallis test with Bonferroni correction. We performed cross-tabulation analyses to compare proportions of categorical variables. If the observed or predicted value of any cell in a 2×2 table was ⩽5, we used Fisher’s exact test. In all other situations, we used Pearson’s chi-square test. When more than two groups were compared and differences with statistical significance were noted, we further analyzed all between-group comparisons with Bonferroni corrections. Statistical significance was set at p-value < 0.01. Missing data were not imputed. IBM SPSS version 29 (IBM Corp., Armonk, New York) was used for all analyses.
Ethical considerations
The study protocol was approved by the Helsinki University Hospital administrative board. According to Finnish law, ethics committee approval and patient informed consent were not required for this registry study.
Results
During 2006–2020, 5401 patients were included in the HTR. A total of 2529 patients were included in the study, of which 1336 (53%) had a TSI and 1193 had N-TSI (Fig. 1). Patient demographics are shown in Table 1. The two groups were comparable regarding age, sex, ASA classification, NISS scores, and 30-day in-hospital mortality.
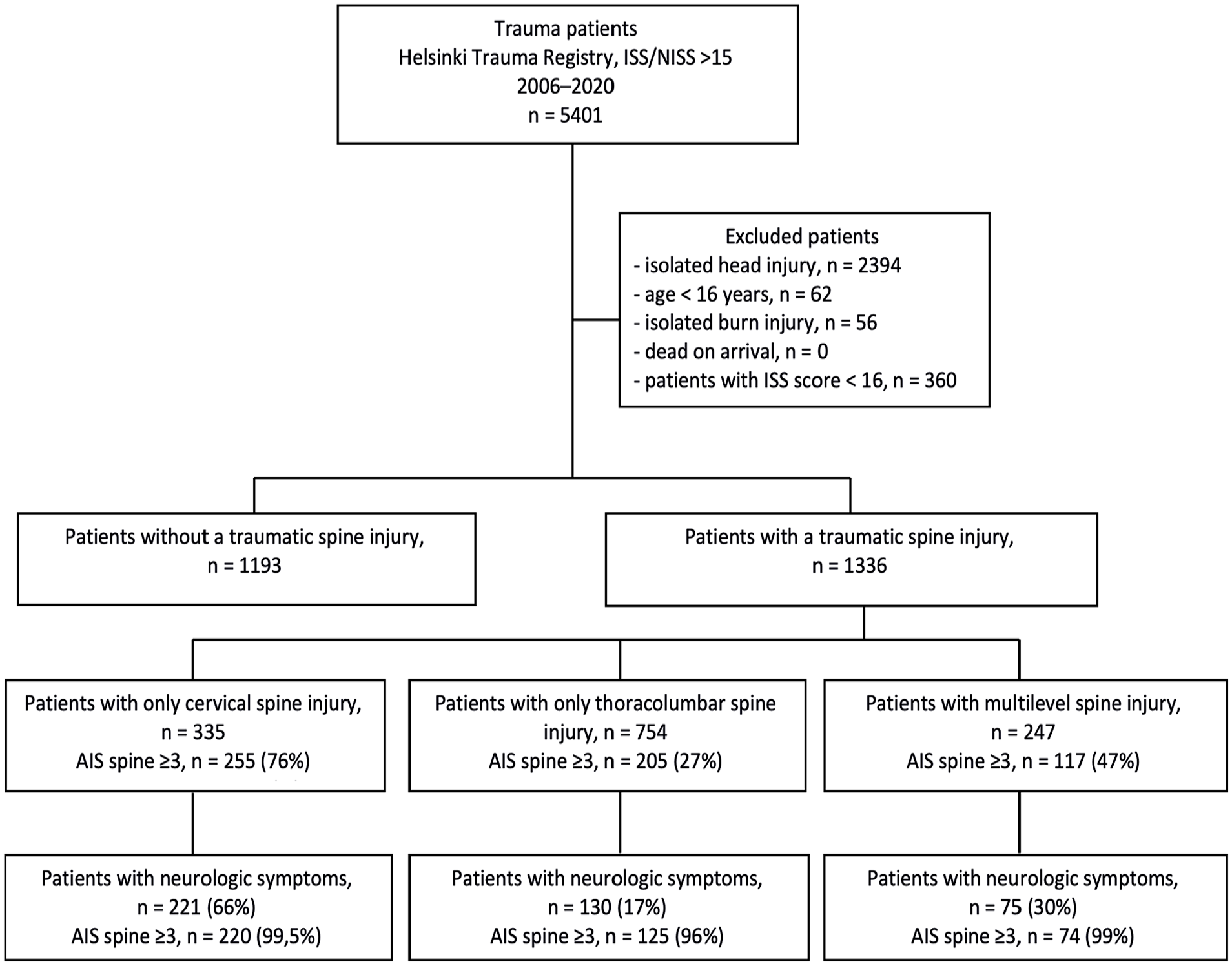
Flowchart of included and excluded patients.
Patient demographics.
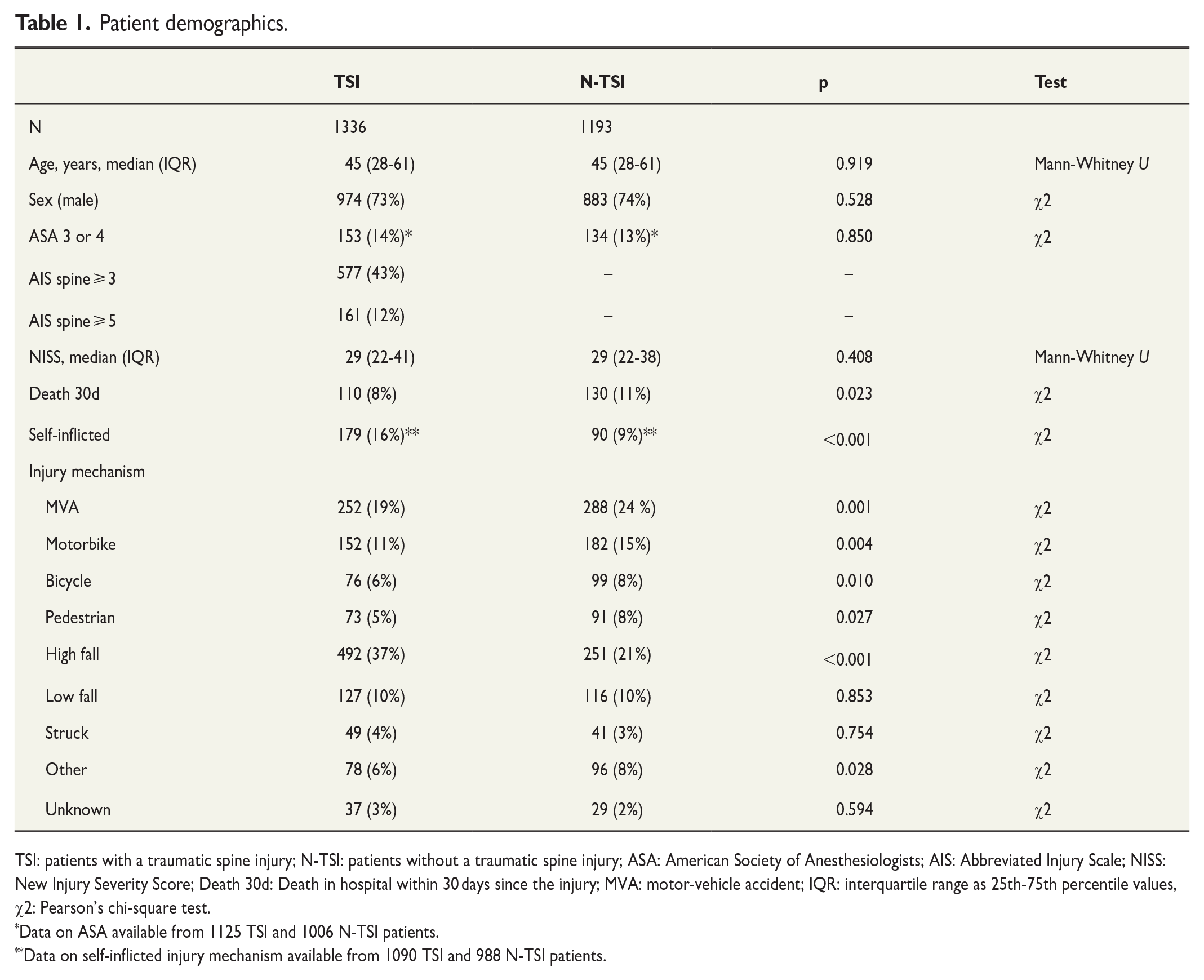
TSI: patients with a traumatic spine injury; N-TSI: patients without a traumatic spine injury; ASA: American Society of Anesthesiologists; AIS: Abbreviated Injury Scale; NISS: New Injury Severity Score; Death 30d: Death in hospital within 30 days since the injury; MVA: motor-vehicle accident; IQR: interquartile range as 25th-75th percentile values, χ2: Pearson’s chi-square test.
Data on ASA available from 1125 TSI and 1006 N-TSI patients.
Data on self-inflicted injury mechanism available from 1090 TSI and 988 N-TSI patients.
When compared with N-TSI patients, TSI patients were injured more frequently by a high-fall mechanism (37% vs 21%, p < 0.001) (Table 1). TSI patients were also injured more often by a self-inflicted mechanism than N-TSI patients (16% vs 9%, p < 0.001). Motor-vehicle accidents (MVA) and motorbike accidents were less frequent in the TSI group (19% vs 24%, p = 0.001 and 11% vs 15%, p = 0.004, respectively).
Of TSI patients, 754 (56%) had only thoracolumbar spine injuries, 335 (25%) had only cervical spine injuries, and 247 (18%) had multilevel spine injuries (Table 2). Patients in the cervical group were older (p < 0.001), had lower NISS scores (p < 0.001), and self-inflicted injury mechanism was less frequent compared with thoracolumbar and multilevel groups (p < 0.001). Cervical spine injuries were more often caused by a low-fall mechanism than other spine injuries (p < 0.001). All groups differed from each other regarding neurological symptoms (p < 0.001); cervical patients had the most neurological symptoms and thoracolumbar patients the least. Thoracolumbar patients were injured more often by a high-fall mechanism than the other groups, followed by multilevel group (p < 0.001). The 30-day in-hospital mortality in the cervical group was higher than in the thoracolumbar group (p = 0.005). There was no statistical difference in 30-day in-hospital mortality between cervical and multilevel or thoracolumbar and multilevel groups. A significantly higher proportion of cervical patients had AIS spine ⩾ 3 compared with other groups, followed by the multilevel group (p < 0.001).
Traumatic spine injury patient demographics according to level of injury.
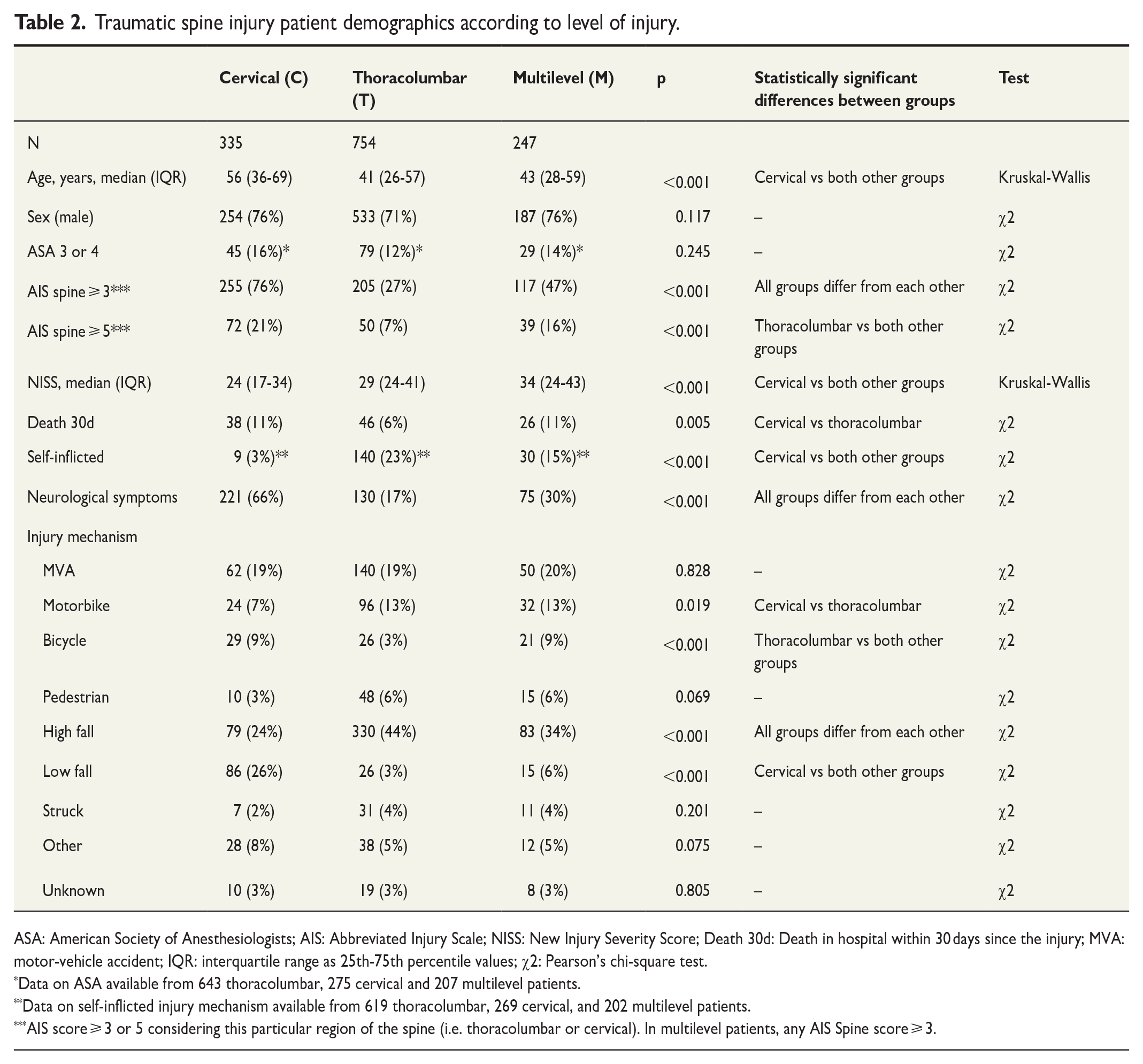
ASA: American Society of Anesthesiologists; AIS: Abbreviated Injury Scale; NISS: New Injury Severity Score; Death 30d: Death in hospital within 30 days since the injury; MVA: motor-vehicle accident; IQR: interquartile range as 25th-75th percentile values; χ2: Pearson’s chi-square test.
Data on ASA available from 643 thoracolumbar, 275 cervical and 207 multilevel patients.
Data on self-inflicted injury mechanism available from 619 thoracolumbar, 269 cervical, and 202 multilevel patients.
AIS score ⩾ 3 or 5 considering this particular region of the spine (i.e. thoracolumbar or cervical). In multilevel patients, any AIS Spine score ⩾ 3.
Among the cervical group, patients with neurological symptoms were older (p < 0.001), AIS spine was ⩾ 3 more often (p < 0.001), patients had lower NISS scores (p < 0.001), and self-inflicted injury mechanism was less frequent (p < 0.001) compared with cervical patients without neurological symptoms (Table 3). Cervical patients without neurological symptoms were more frequently injured by MVA (p < 0.001) or as pedestrians (p < 0.001), whereas low falls were more frequent (p < 0.001) in cervical patients with neurological symptoms.
Traumatic spine injury patient demographics according to level of injury and presence of neurological symptoms.
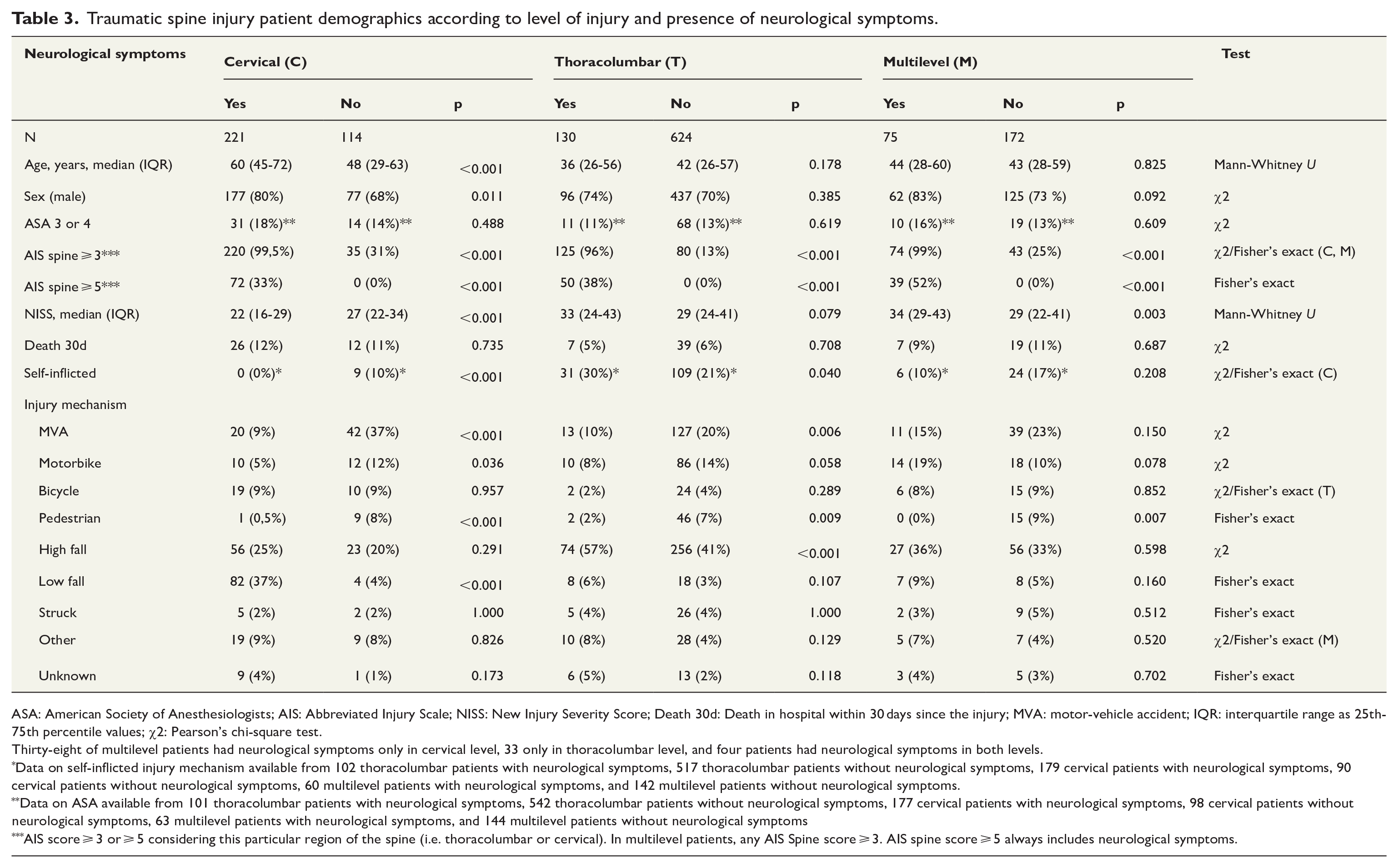
ASA: American Society of Anesthesiologists; AIS: Abbreviated Injury Scale; NISS: New Injury Severity Score; Death 30d: Death in hospital within 30 days since the injury; MVA: motor-vehicle accident; IQR: interquartile range as 25th-75th percentile values; χ2: Pearson’s chi-square test.
Thirty-eight of multilevel patients had neurological symptoms only in cervical level, 33 only in thoracolumbar level, and four patients had neurological symptoms in both levels.
Data on self-inflicted injury mechanism available from 102 thoracolumbar patients with neurological symptoms, 517 thoracolumbar patients without neurological symptoms, 179 cervical patients with neurological symptoms, 90 cervical patients without neurological symptoms, 60 multilevel patients with neurological symptoms, and 142 multilevel patients without neurological symptoms.
Data on ASA available from 101 thoracolumbar patients with neurological symptoms, 542 thoracolumbar patients without neurological symptoms, 177 cervical patients with neurological symptoms, 98 cervical patients without neurological symptoms, 63 multilevel patients with neurological symptoms, and 144 multilevel patients without neurological symptoms
AIS score ⩾ 3 or ⩾ 5 considering this particular region of the spine (i.e. thoracolumbar or cervical). In multilevel patients, any AIS Spine score ⩾ 3. AIS spine score ⩾ 5 always includes neurological symptoms.
Thoracolumbar patients with neurological symptoms were injured by a high fall more often (p < 0.001) than thoracolumbar patients without neurological symptoms (Table 3). MVAs and injuries as a pedestrian were more frequent among thoracolumbar patients without neurological symptoms (p = 0.006 and p = 0.009, respectively). AIS spine ⩾ 3 was more common (p < 0.001) among thoracolumbar patients with neurological symptoms.
Among the multilevel group, patients with neurological symptoms had AIS spine ⩾ 3 more frequently (p < 0.001) and higher NISS scores (p = 0.003) (Table 3). Patients without neurological symptoms were more frequently injured as pedestrians (p = 0.007).
One hundred and seventy-nine TSI patients were injured by a self-inflicted mechanism. When patients with self-inflicted TSI and other TSI were compared, patients with self-inflicted TSI were younger (p < 0.001), more often female (p < 0.001), had higher NISS scores (p < 0.001), and were injured more often by a high-fall mechanism (p < 0.001) (Table 4).
Traumatic spine injury patient demographics according to whether the injury was self-inflicted or not.
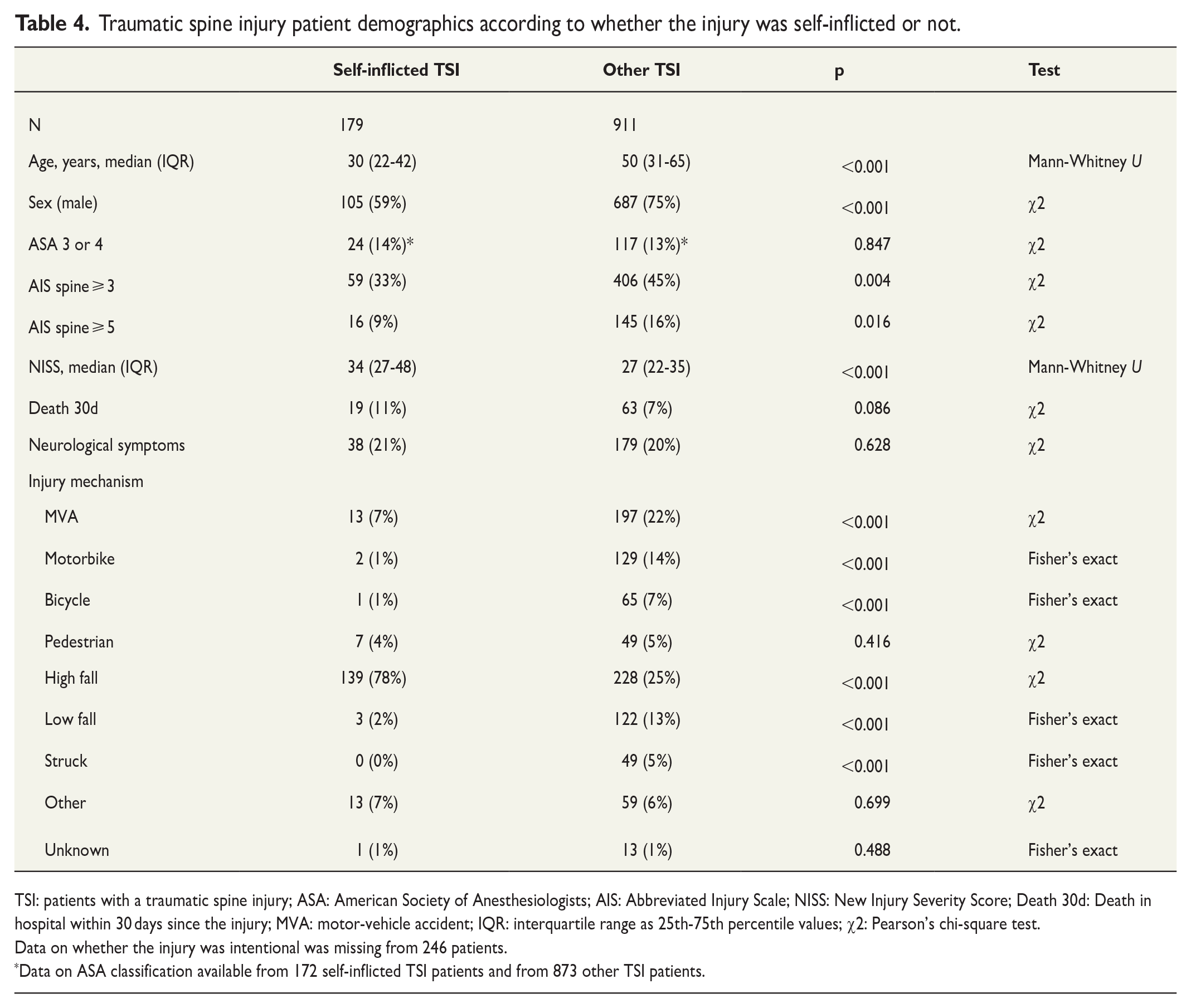
TSI: patients with a traumatic spine injury; ASA: American Society of Anesthesiologists; AIS: Abbreviated Injury Scale; NISS: New Injury Severity Score; Death 30d: Death in hospital within 30 days since the injury; MVA: motor-vehicle accident; IQR: interquartile range as 25th-75th percentile values; χ2: Pearson’s chi-square test.
Data on whether the injury was intentional was missing from 246 patients.
Data on ASA classification available from 172 self-inflicted TSI patients and from 873 other TSI patients.
When comparing TSI patients during the 5-year periods of 2006–2010, 2011–2015, and 2016–2020, ASA classification score 3 or 4 was more frequent during 2016–2020 than the other periods (p < 0.001) (Supplement 1). Patient NISS scores were higher during 2016–2020 compared with 2006–2010 (p < 0.001). AIS spine ⩾ 3 and neurological symptoms were less common during 2016–2020 compared with the other time periods (p < 0.001). There were no statistically significant differences regarding age, sex, 30-day in-hospital mortality, or injury mechanisms between these groups.
Discussion
Our study presents data of severely injured trauma patients from a large tertiary trauma center over a 15-year period. As 53% of our included patients and 25% of all the HTR patients had at least one traumatic spine injury, it seems that these injuries are common among severely injured trauma patients. Our results are consistent with previous research. Bliemel et al. 3 analyzed 24,974 patients with ISS > 15, and 36% of patients had documented spinal injuries with AIS spine ⩾ 2. Lee et al. 20 retrospectively analyzed 2893 major trauma patients (ISS > 15) during 2016–2020, of which 781 (27%) had a spine injury. The 30-day in-hospital mortality of TSI patients in our population was 8%, which is consistent with previous literature on TSI patients with ISS > 15 reporting mortality rates of 4.0%–7.8%.20,21
Our results show that among all included patients, MVAs and high falls were the two most common injury mechanisms. When comparing injury mechanisms between TSI and N-TSI patients, the most evident feature was that TSI patients were injured more frequently by a high-fall mechanism than N-TSI patients. MVAs were the second most common injury mechanism among TSI patients. Similar results can be found in previous literature, as many previous studies suggested that the two most common injury mechanisms for spine injuries are MVAs and falls.1,2,4,5,7–13,15–18,20–22,24,33–36 Another difference between TSI and N-TSI patients was that self-inflicted injuries were more common among the TSI group. Among the most common methods of suicide attempts in Finland are hanging, poisoning by drugs or other means, firearms, drowning, jumping from height, and the use of moving objects. 37 Poisoning does not directly cause traumatic injuries and drowned patients are treated in another HUH unit. Furthermore, gunshot wounds were also treated in another unit at the time of the study period, thus the proportion of jumping and high falls in suicidal patients treated in the HUH trauma unit is higher. As falls > 2–3 m have previously been shown to be predictors for spinal fractures/dislocations and spinal cord injuries, this may explain the difference between the two groups.5,33
Patients with TSI in only the cervical region differed from other groups in several ways. Based on our results, older patients whose injury mechanism was low fall were overrepresented in the cervical-injury group compared with other groups. Self-inflicted injuries were less likely and NISS scores were also lower in these patients. Among the cervical-injury group, these same characteristics were observed especially in patients with neurological symptoms. In addition, all but one cervical-injury patient with neurological symptoms had AIS spine ⩾ 3, which was a significantly higher rate than among cervical-injury patients without neurological symptoms. This is intuitive, as spine injuries causing neurological symptoms result in higher AIS scores than injuries without neurological symptoms. However, NISS scores were lower in cervical-injury patents with neurological symptoms compared to those without. It appears that cervical-injury patients can be divided into a group of younger patients that are injured by a higher-energy mechanism and have more other associated injuries with higher NISS scores and older geriatric patients who are injured by a low fall and sustain a more serious local cervical injury with neurological symptoms but do not develop as many associated injuries due to the lower-energy injury mechanism. A similar observation was made by Leucht et al. 9 in a German population. As the number of elderly people is increasing, geriatric trauma in general is becoming more common and it is probable that the incidence of these more severe cervical spine injuries will increase in the future. 38 In Finland, the number of fall-induced cervical spine injuries among patients aged > 50 years has already been increasing rapidly over the past decades. 39 Therefore, attention to fall prevention among elderly persons may be an effective way of reducing these injuries.
Data on whether the injury was intentional were available from 1090 (82%) out of 1336 TSI patients. Of these, 179 (16%) patients were injured by a self-inflicted injury mechanism. Compared with other TSI patients, self-inflicted TSI patients were more often younger women and the injury mechanism was mainly high fall. Similar results were observed previously in two Italian studies.35,40 Spota et al. 35 also compared patients who had fallen accidentally to intentional jumpers. They discovered that jumpers had a higher height of fall, which has been previously associated with higher ISS scores.41,42 In our population, self-inflicted TSI patients had also significantly higher NISS scores compared with other TSI patients, perhaps reflecting a higher energy of trauma, even though we did not analyze, for example, heights of fall from individual patients. Niemi-Nikkola et al. 11 investigated the incidence and epidemiological features of traumatic spinal injuries in Northern Finland during 2007–2011. They found that most spinal cord injuries (SCI) in the age group < 45 years were caused by road traffic accidents and discussed the need of focusing preventive measures on road traffic accidents in younger age groups, as SCIs in younger age groups cause major burden from a human and economic perspective, as longer life expectancy means more years with lowered quality of life and higher economic costs. In the same way, as self-inflicted TSI patients seem to be younger female patients compared with other TSI patients, preventive mental health programs targeted to this population may reduce self-inflicted TSIs.
Over the three 5-year periods, there were a few detectable changes in patient demographics among TSI patients. ASA classification 3–4 was more frequent during the last period (2016–2020). NISS scores were also higher during these years compared with 2006–2010. Based on these findings, TSI patients during the last 5 years had more pre-existing comorbidities and had more severe injuries, which would be expected to associate with higher mortality and a poor prognosis. However, we did not find a significant increase in 30-day mortality of patients. In a previous study based on the HTR data considering pelvic ring fractures (PRF), there was a significant decrease in PRFs over time, which was thought to be explained by improved safety features in new cars, traffic-injury prevention programs, and investments in better road safety. 26 This kind of reduction in MVAs causing TSIs was not observed in our study even though MVAs were the second most common injury mechanism of TSIs during every 5-year period. However, TSI patients during 2016–2020 were less likely to have neurological symptoms or AIS spine score ⩾ 3 compared with previous time periods. Hence, it seems that even though the injury mechanisms of TSIs did not change, these injuries were less severe during the last time period. As NISS scores during the last 5-year period did not decrease compared with the first two time periods and were in fact higher compared with 2006–2010, the associated injuries of these patients seem to have been more serious than during the previous 10 years; we are not able to provide an explanation for this.
The strength of this study is the large number of patients treated during a consecutive 15-year period in one of the largest tertiary trauma centers in Northern Europe. The data of the HTR have also been validated previously and its coverage and accuracy are considered excellent.28,43
There are a few limitations in our study. The patients treated in the HUH trauma unit are mainly injured by blunt mechanisms, as stab wounds and gunshot wounds of the torso were treated in another unit at the time of the study period. Hence, the results of this study cannot be used in evaluating penetrating injuries. However, over 95% of major trauma patients in Finland are injured by a blunt mechanism, as in most other countries in Europe.44–46 As patients included were mainly polytrauma patients, independent effects of particular injuries to patient outcomes cannot be determined based on our results.
Conclusion
Unlike other severely injured trauma patients, severely injured trauma patients with spine injuries are injured mostly by a high-fall mechanism and over a third of these high falls are suicide attempts. High falls, young age, and female gender are overrepresented in TSI patients with a self-inflicted injury mechanism. Cervical spine-injury patients are mostly elderly persons injured by a low-energy mechanism. Prevention programs focused on mental health of young persons and falls in the elderly may be beneficial for reducing these injuries.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241271781 – Supplemental material for Spine injuries among severely injured trauma patients: A retrospective single-center cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969241271781 for Spine injuries among severely injured trauma patients: A retrospective single-center cohort study by Henri Lassila, Mikko Heinänen, Joni Serlo and Tuomas Brinck in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We thank Satu Tirkkonen, Pirkko Tonder, Markku Kytönen, Iiu Laitinen, and Marja Bergman for excellent work in accurately recording the data for the Helsinki Trauma Registry. We also thank Kirsi Willa for managing the databank of the Helsinki Trauma Registry and Tim Söderlund for valuable advice during the writing process.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.