
Abstract
Background and aims:
Tuberous breast is a rare anomaly affecting the development of mainly the female breast. It presents with varying degrees of hypoplasia in the breast base and skin. In some cases, herniation and widening of the areola is observed. The condition constitutes a great challenge for the reconstructive surgeon. In this study, the surgical cascades of implant and lipofilling corrections were compared with a focus on the need for re-interventions.
Methods:
In total, 129 patients whose treatment regimen started between January 2010 and October 2020 were included in this study. Patients were categorized into two groups based on the volume correction method used (lipofilling versus implant).
Results:
In 35 (27%) patients (41 breasts), breast volume increasement was executed with an implant, while 94 (73%) patients (169 breasts) underwent volume increasement with lipofilling. The mean number of operations during the primary correction process was 1.2 (range 1–5) for the implant group and 2.4 (range 1–5) for the lipofilling group. When assessing the need for re-operations within 5 years after completing the primary correction, 46% of patients in the implant group needed further surgeries, while the corresponding proportion for the lipofilling group was 21% (p = 0.04). There were six major complications, all of them in the implant group.
Conclusion:
Implant-based reconstruction is associated with more revision surgeries and major complications compared to autologous lipofilling corrections. Lipofilling offers a more durable result with less re-operations over time despite initial sequential primary surgeries.
Context and Relevance
The material presented is based on the original research of the authors. It has not been published and is not being offered for publication elsewhere. Previous studies have been done referring this topic, but they have been limited in size due to the rarity of this condition.
This study, based on a substantial patient material, reveals that implant reconstruction for the volume correction of the tuberous breast deformity leads to more re-operations compared to lipofilling corrections. Lipofilling for the correction of tuberous breasts has a low complication rate and few secondary corrections over time. This study contributes to the knowledge on correction of tuberous breast allowing for better informed patients with realistic expectations on their individual corrective journey.
Introduction
Tuberous breast deformity (TBD) is a rare condition affecting mainly adolescent women. It was first described in the work by Rees and Aston 1 in 1976. The deformity presents as abnormal development of the breast. The thickening of the superficial fascia leads to the impairment of lower pole breast development. 2 Clinical findings include hypoplasia of breast parenchyma and skin, superior positioning of the inframammary fold, herniation of the areola, and sometimes increased areolar diameter. TBD may be bilateral or unilateral.2–7 Asymmetry is almost always present in the tuberous breast.4,8 To date, the pathology and prevalence behind the tuberous breast remains obscure.
In 1996, Von Heimburg et al. 9 graded the TBD into four types and this classification was later modified in the work by Grolleau et al. 10 into three types. The grading addresses the distribution of hypoplasia of the breast parenchyma (Fig. 1). Areolar herniation is not included in the classification, but it is noted that areolar herniation is more frequent in grade III breasts.9–11
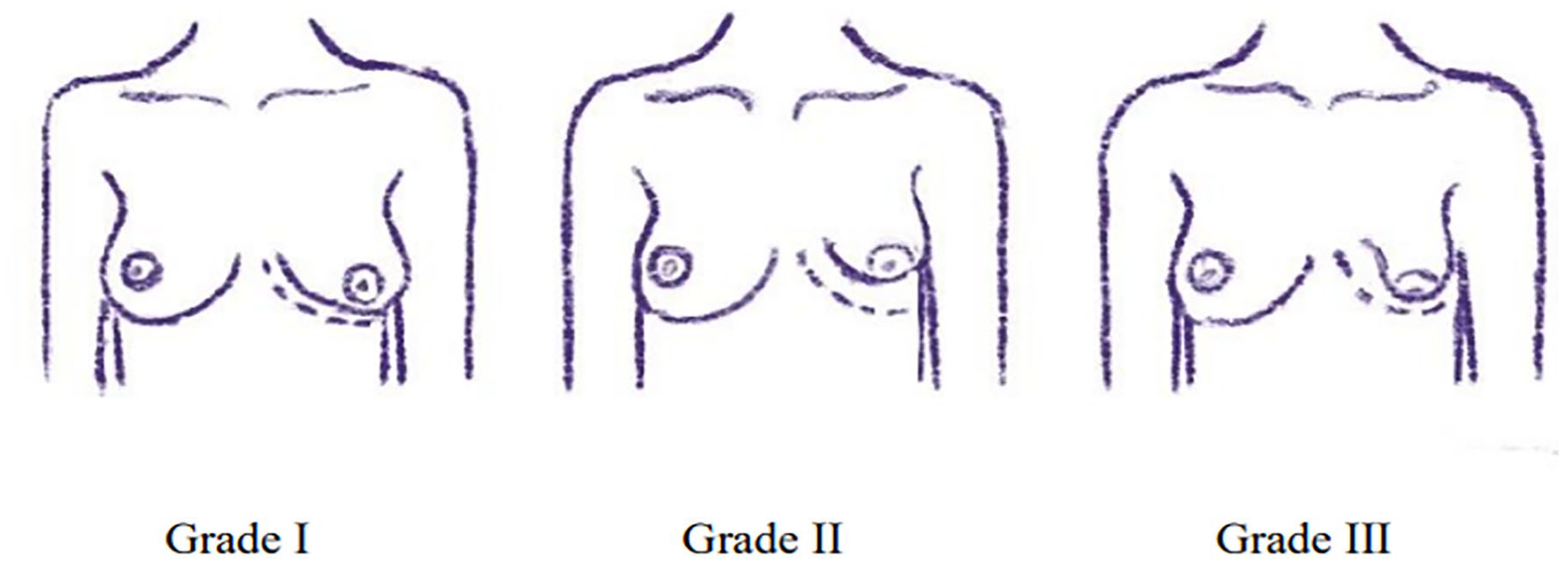
Illustration of the classification of tuberous breast anomalies. Based on the Grolleau classification.
Patient education plays a big role when planning the surgical correction of the tuberous breast. The deformity can cause poorer quality of life and profound psychological distress to the adolescent. Due to this strong emotional aspect, correct planning and thorough patient information is vital to achieve satisfactory results.7,12,13
Surgical management of the tuberous breast is ultimately determined by the severity of the presentation with several anatomic abnormalities to overcome. The correction method must address the need for expanding the breast base and establishing a new inframammary fold, augmenting the skin envelope, addressing areolar herniation, and requiring volume correction. To correct the different anatomical alterations, different types of flaps combined with glandular remodeling and surgical restoration of the areolar diameter can be used. Depending on the severity of the deformity and the chosen technique, the correction can be done in a single-stage or a multi-stage approach.5,6,11
Hypertrophic breasts can be reduced in size while in hypoplastic breasts, the breast volume is often enhanced. Generally tuberous breasts are hypoplastic. 4 Breast implants and more recently autologous fat grafting have become the most used techniques to obtain adequate breast volume. The augmentation technique frequently addresses both the constriction of the breast base and the establishment of the inframammary fold concurrently with volume correction.
The use of implants carries a potential risk of surgical complications leading to implant replacement or removal. 14 Autologous fat grafting significantly reduces the risk for re-operations, even though it often initially requires sequential procedures. 15 The gold standard technique in the surgical correction of the tuberous breast has not yet been determined.
The aim of this study was to compare the volume correction technique used and the severity of the anomaly in terms of duration of the primary correction process, complications, and number of later re-operations.
Methods
Patients whose treatment regimen had started at the Helsinki University Hospital in 2010–2020 were included in the study and they were followed-up through electronic health records until the end of year 2022. A total of 156 patients with TBD operated were reviewed in this retrospective cohort. All patients with grade I to III (Grolleau scale) deformity, with no associated breast disease were studied. The grade of deformity was retrieved from the digital database and verified from preoperative photographs by the authors. Patients with previous breast surgeries and patients with no need for volume increasement were excluded. The group with no need for volume increasement contained tuberous breasts deformities corrected with mastopexy or breast reduction techniques.
The patients included in this study were divided into two groups based on the surgical technique used: (1) breast reconstruction with implant with or without glandular remodeling and (2) breast reconstruction with autologous fat grafting with or without glandular remodeling (Fig. 2). The selection of the surgical correction technique was based on the preferences of the surgeon in conjunction with the preferences expressed by the patient.
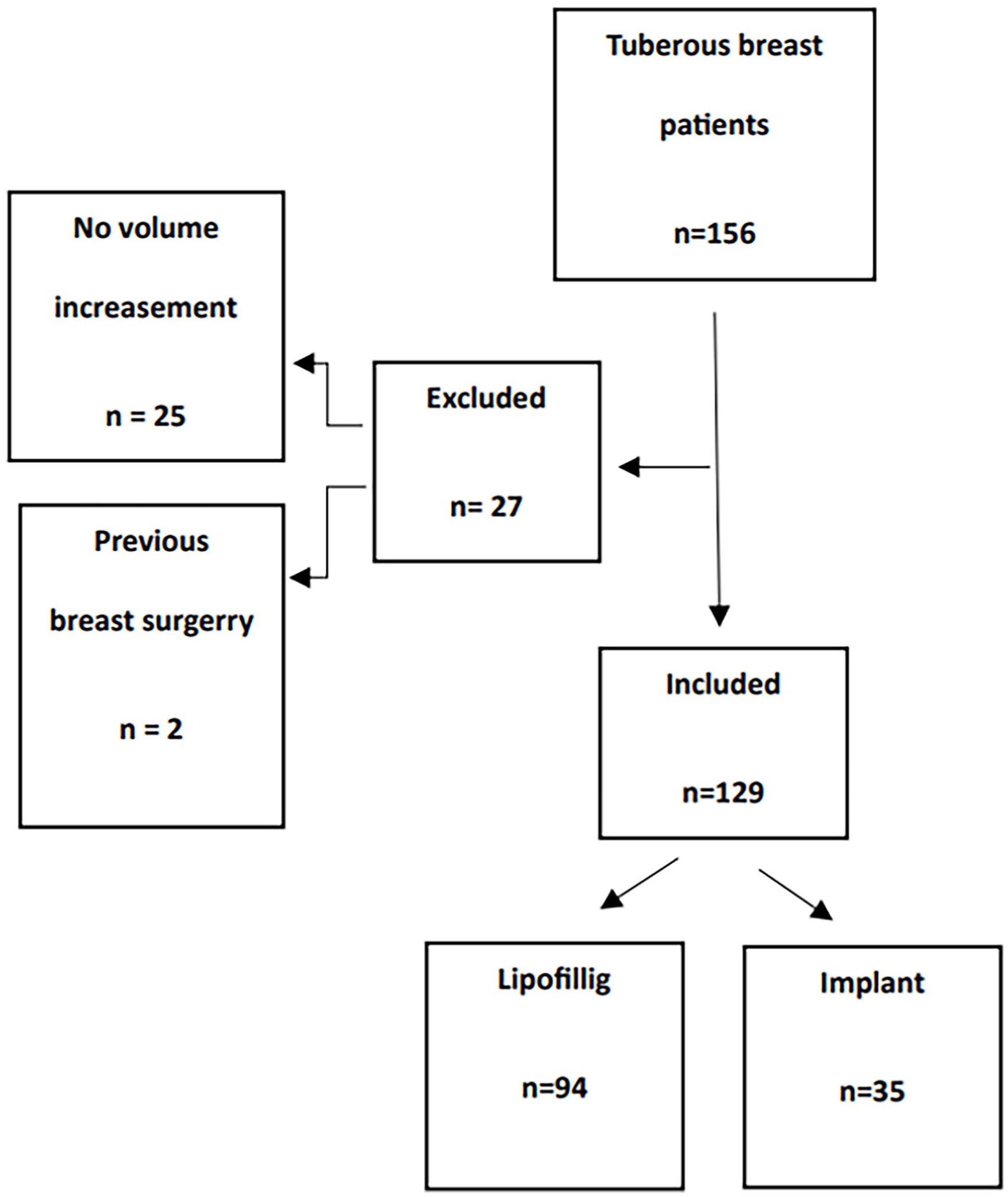
Patient inclusion criteria and study groups.
Glandular remodeling included various methods involving the reshaping of the areola and releasing of the constriction bands in the parenchyma. The different approaches demonstrate diversity and often comply to a “cut as you go” methodology, making it impossible to reliably specify them. For the volume correction, fat grafting was mainly performed with water-assisted liposuction (WAL) and the use of a multilayer approach from several different entrance points. Implant placement was made using various techniques according to the surgeon’s preference. Up to 2017, the most implants used were anatomic textured implants, and after the risen awareness of breast implant-associated anplastic large cell lymphoma (BIA-ALCL), related mainly to textured implants, the majority of implants used in the study were smooth and round implants.
The following demographic and clinical data were retrieved from the Helsinki University Hospital digital database: age, body mass index (BMI), surgical technique, the presence of asymmetry, degree of deformity, operation dates, and complications. The size of the implant used, and the volume of grafted fat were also recorded. In addition, major complications leading to in-hospital stay or further surgeries, specifying the number and reasons of re-operations were noted. Minor complications were not documented, as the reliable identification of such occurrences is challenging given the retrospective design of the study.
We separated the surgical process into two timeframes: (1) the primary surgical correction process leading to a stable good result, determined as a satisfactory outcome by the surgeon and the patient, (2) the re-operations arising at a later timepoint, with a new referral separate from the primary process. By this division, we were able to obtain a realistic overview of the operation cascade of the different surgical methods and thus truly compare the need for revisional surgical interventions.
The study was approved by the Ethics Committee of Helsinki University Hospital.
Summary statistics are presented as the mean and range. Between-group comparisons for continuous variables were performed using two-sample t-test and categorical data were analyzed using the chi-square test. Analyses were performed using SPSS for Windows (version 27, IBM Corp., Armonk, NY, USA) and R Statistical Software. 16
Results
Altogether 156 patients were identified for the study. After exclusions, 129 patients were included in the analyses (Fig. 2). The mean age of the patients at the time of the first surgery was 25.0 (16.1–54.1) years and the mean BMI was 24.5 (18.1–39.1) kg/m2 (Table 1). Data of BMI were missing for 14 patients (10.9%).
Patient characteristics.
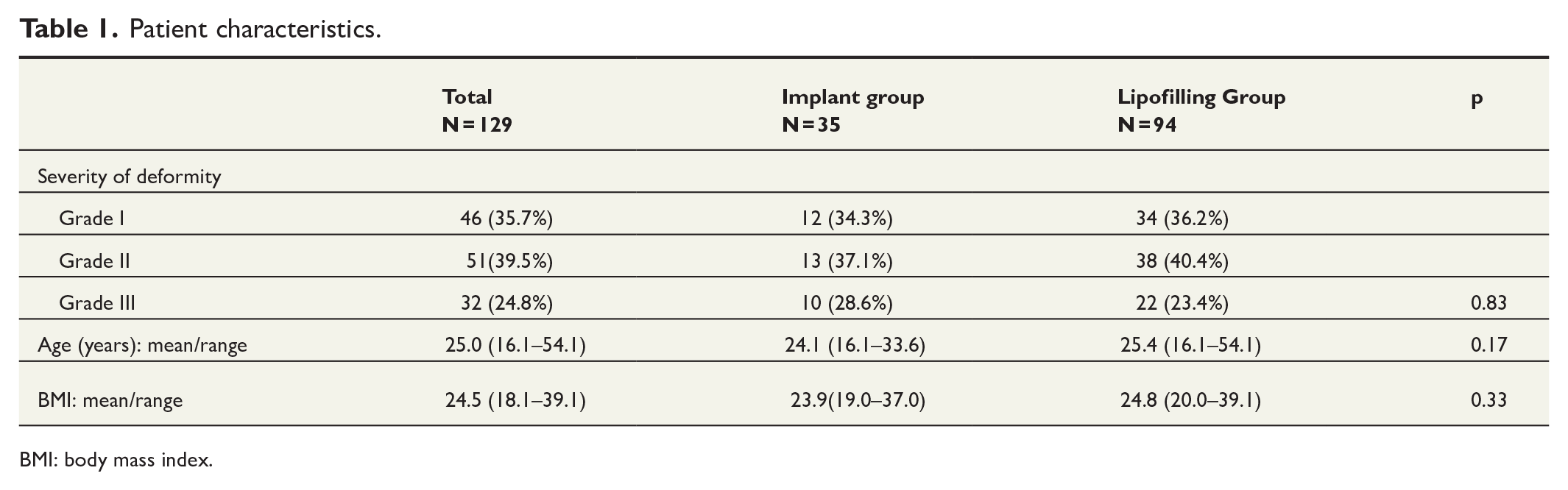
BMI: body mass index.
The study population consisted of 46 patients with grade I deformity, 51 patients with grade II, and 32 patients with grade III deformities. Asymmetry was present in the majority (77%) of patients. A unilateral deformity was found in 15%, and bilateral deformity in 84% of the patients (Table 1).
As shown in Fig. 2, 35 (27%) patients underwent breast volume increasement with an implant (46 breasts) and 94 (73%) patients underwent volume increasement with lipofilling (169 breasts). In terms of the demographic data (age, BMI, grading of deformity), the two groups were comparable (Table 1).
The severity of the deformity had no major impact on the chosen surgical correction technique (Table 1). The mean volume of implants used was 218 (range 80–385) mL and the mean volume of total fat grafted per operated breast during the correction period was 277 (range 20–880) mL. Comparing the association between the degree of deformity and the total volume increasement needed, we observed that the amount of volume required for satisfactory results was greater in the patients with grade III compared to the patients with grade I or II, but the difference did not reach statistical significance (Fig. 3).
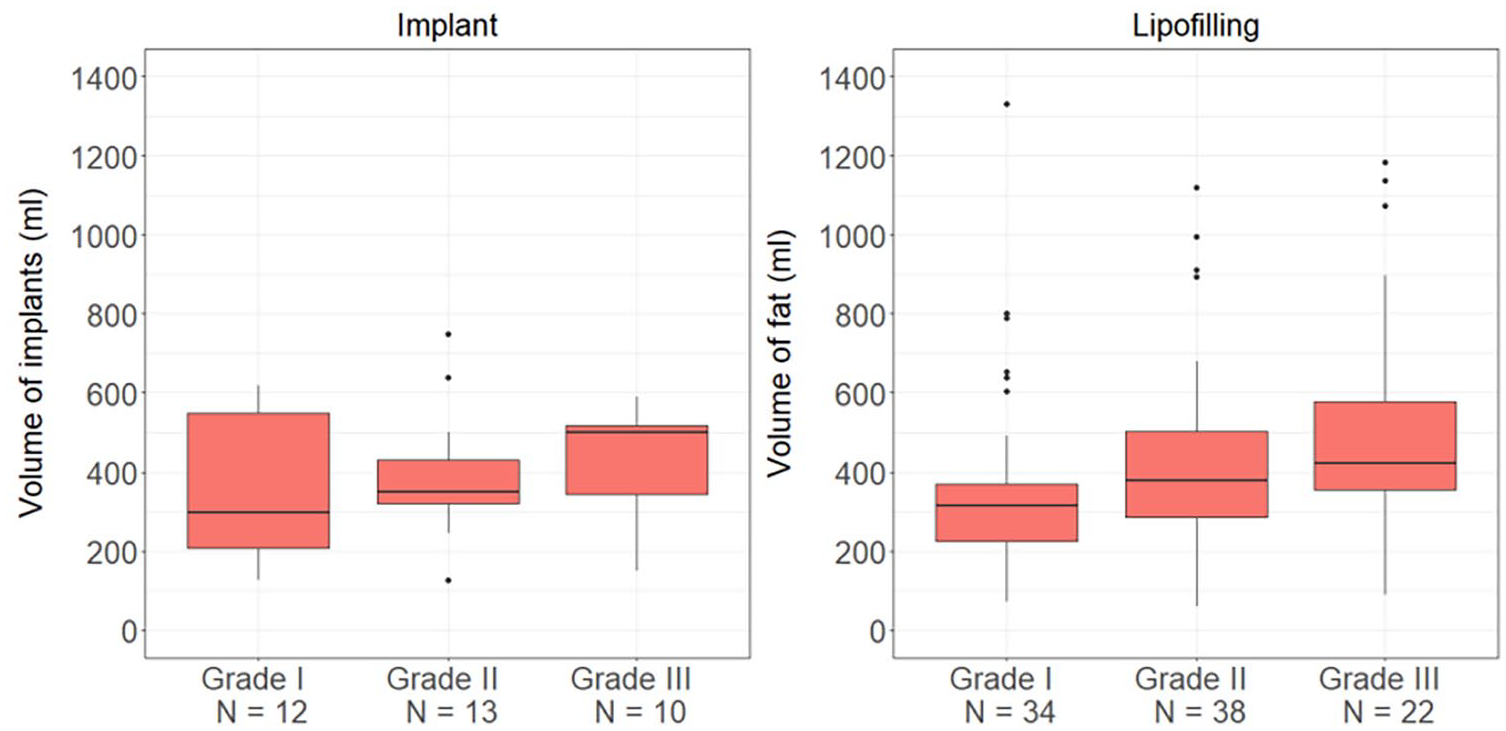
Total volume increasement in different grades.
The mean number of surgical interventions within the primary correction process was significantly lower in the implant group (1.2; range 1–5) compared to the lipofilling group (2.4; range 1–5); p < 0.001. In the lipofilling group, the BMI of the patient was not associated with the number of interventions or with the volume grafted. The degree of the deformity had a major impact on the number of primary operations in the lipofilling group. The patients with grade I deformity had lower mean number of primary operations (mean 2.0) compared to patients with grade II deformity (mean 2.6, p = 0.012) or patients with grade III deformity (mean 2.7, p = 0.016). The mean number of primary operations increased by the degree of deformity also in the implant group although the differences between the groups were small. The mean number of primary surgeries was 1.0 in grade I group versus 1.2 in grade II group (p = 0.08) and 1.5 in grade III group (p = 0.24) (Fig. 4).
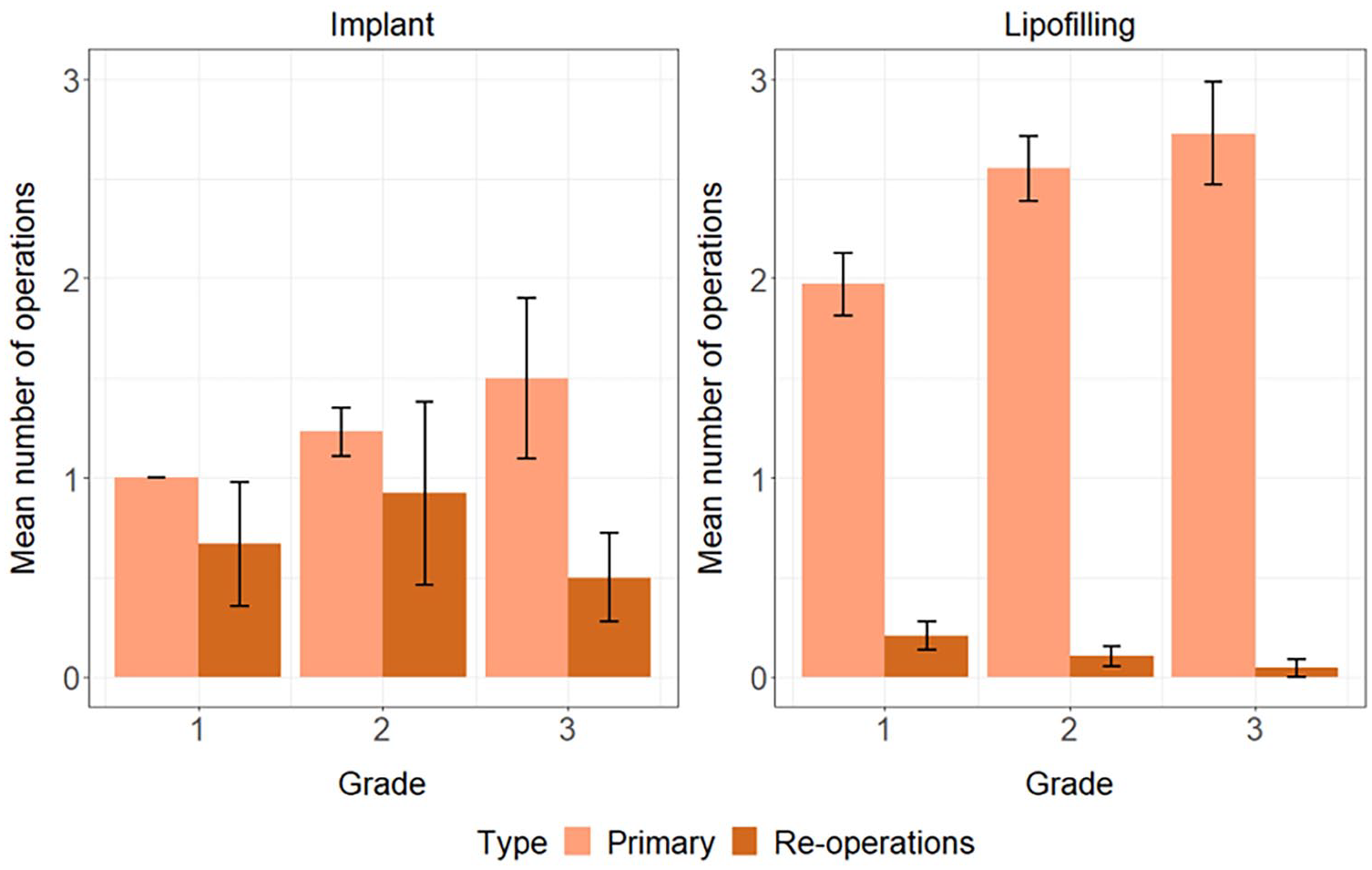
Number of operations within different grades.
The primary correction process of all patients was complete before the follow-up time ended. The mean duration of the primary process was 0.2 years (range 0–5.0) in the implant group and 1.1 years (range 0–4.0) in the lipofilling group (p < 0.001). The average length from the first surgery to the end of follow-up time in the study population was 6.8 (2.5–13.0) years. In the implant group, the average follow-up was 8.2 (2.6–13.0) years and in the lipofilling group, 6.3 (2.5–12.6) years (p = 0.001). The paradigm shift toward autologous reconstruction over time was evident in the study population. Because of this trend, the follow-up in the lipofilling group was shorter.
To compare the lipofilling and implant groups with the same follow-up period, the patients with at least 5 years of follow-up after the primary process were selected to further analysis and re-operations performed within this 5-year period were observed. Altogether, 71 patients reached at least 5 years of follow-up period after primary process, 28 in implant group and 43 in lipofilling group. The need for re-operation within 5 years after completing the primary process was more common among patients in the implant group (46%) compared to patients in the lipofilling group (21%) (p = 0.044). The mean time for the first re-operation was 2.0 years both in implant and lipofilling groups (p = 0.89).
When observing the entire follow-up period, 11 patients in the lipofilling group needed a re-operation, none of them more than one. In the implant group, 9 patients needed one revision and 5 patients needed two or more additional operations. The most common reasons for re-interventions in the implant group were the re-development of the tuberous contour in the breast and the changes occurring in the non-operated breast over time resulting in asymmetry. In the implant group, there were three capsular contracture cases, two implant ruptures and one case of double bubble formation leading to surgical intervention. In the lipofilling group, none of the re-operations involved volume correction. Most corrections in the lipofilling group were for areola widenings and other scar issues after glandular remodeling. Indications for all late re-interventions are shown in Fig. 5. The different grades of the deformity and the need for re-operations were compared, and the deformity degree had no major impact on the incidence of re-operations (Fig. 4).
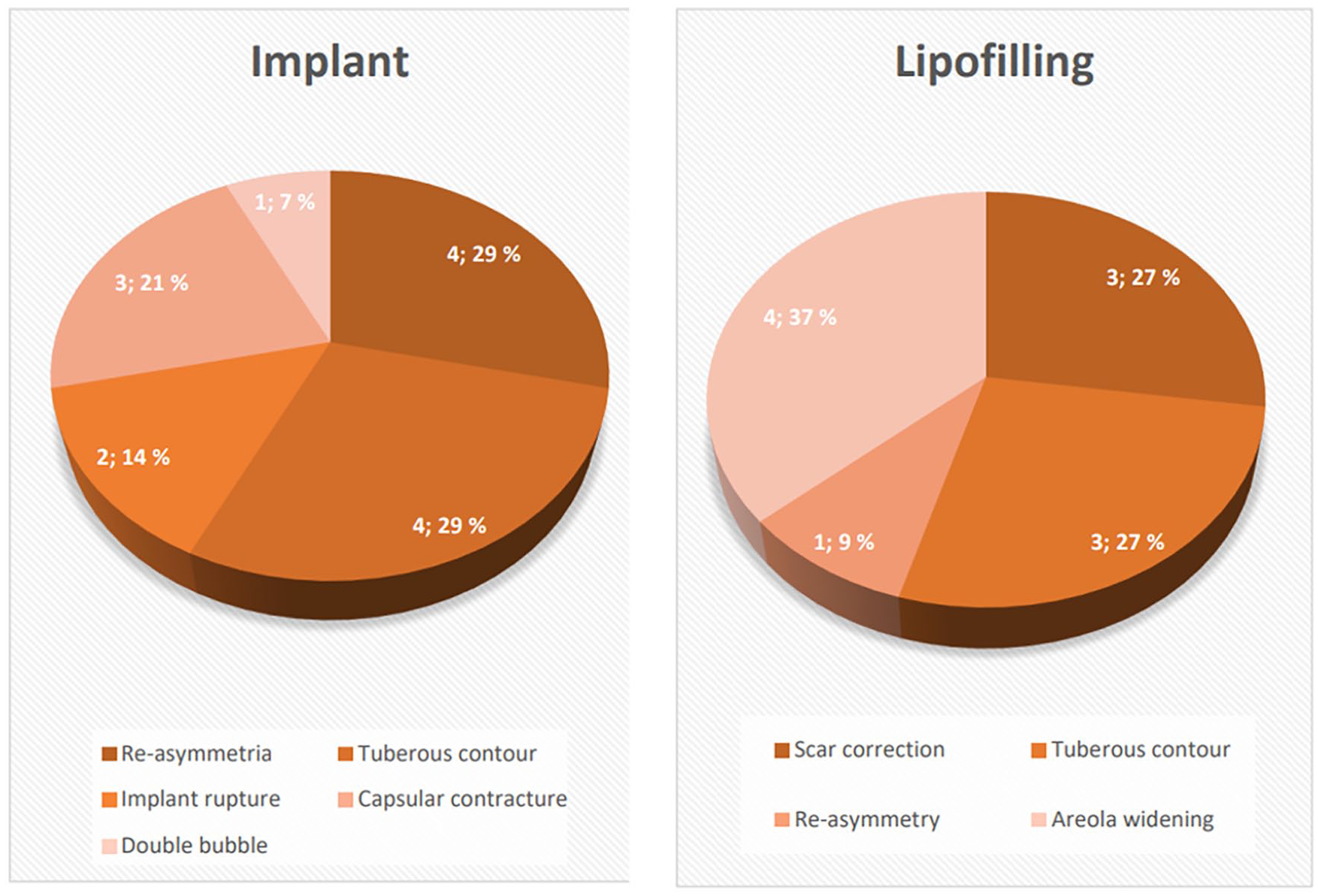
Reason for re-intervention.
The overall complication rate for the study population was 6/129 (4.7%). In the implant group, there was a total of 6/35 (17%) complications and in the lipofilling group, the complication rate was 0/94. There were three cases of capsular contracture, two cases of implant rupture, and one case of double bubble formation leading to revision surgery. Four of the patients had grade II deformities and two had grade I deformity.
Discussion
The best correction method for the TBD has not been determined. In this study, we compared implant reconstruction and lipofilling for volume correction in terms of the number of operations in the primary correction process and the need for later re-interventions. The study population of 129 patients is comparably large5,6,11,15 and presents with a distribution of the different grades of tuberous deformity in parallel with previously published studies.11,15 Interestingly, more than two-thirds of the patients in this study were initially corrected with fully autologous means. This differs from the studies by Brault et al. 15 and Tenna et al., 6 where the distribution between use of implants or fat grafting was more even.
Depending on the laxity of the skin envelope of the breast, only a limited amount of fat can be transferred in one session for maximum retention. This results in more surgical interventions when using lipofilling for volume gain. Our results indicate that despite a generally longer primary correction process, the lipofilling group has few late re-interventions compared to the implant group. This demonstrates that even though autologous fat grafting is primarily a longer process, the result is durable. Patients should be informed that implant reconstruction will more likely lead to re-interventions in the future.7,12,17 Keeping in mind the young age of these patients, the need for an implant exchange is almost inevitable. Breast augmentation with implants carries a risk of complications leading to implant replacement or removal with time. The tuberous breast carries an extra challenge and the risk for revision surgeries after implant reconstruction is higher compared to simple implant augmentation. 18
The overall complication rate in our study is low, zero in the fat grafting group, and 17% in the implant group. Complications here defined as those leading to re-operation or in-hospital stay. Minor complications are challenging to catch let alone standardize in a reliable manner due to the retrospective nature of the study. The absence of complications within the lipofilling group may relate to the very short incisions needed for the technique and to the anti-inflammatory effect of adipose tissue itself as stated in the work by Monsarrat et al. 19
During the last decades, there has been a paradigm shift toward autologous breast reconstruction techniques.5,19 Di Summa et al. 20 compared a single surgeon experience over 13 years and stated that in the early years of the study period, implants were mainly used as the primary correction method, while lipofilling was used as a salvage tool. Over time, this attitude progressively changed to a lipofilling-based approach. This is also evident in this study. The evolution regarding equipment and operative strategy, such as multilayer technique of fat grafting, has allowed for better graft take per session. 21 Thus, the predictability of graft retention allows for better planning and staging of the operations. Even patients with a low BMI can be treated with fat graft by good surgical planning. Our results did not show association between BMI and number of interventions or with the volume grafted.
Time is crucial when estimating the longevity of the surgical results.12,15 We present a reasonably long follow-up, with 71 patients reaching the follow-up of 5 years. A longer follow-up might make the results even more evident as many implant-related complications arise years after the operation. 22
Limitation of this series is the retrospective nature of the study. We focused on operative techniques and the longevity of the results measured by the number of interventions. We lack standardized assessment of aesthetic outcome and quality of life (QOL). The non-randomized nature of the study method also states as a limitation.
This study contributes to the body of knowledge on correction of tuberous breast allowing for better informed patients with realistic expectations on their individual corrective journey. Lipofilling for the correction of tuberous breasts has a low complication rate and few secondary corrections over time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.