
Abstract
Background and aims:
In retrospective studies, wound healing and leg salvage have been better if revascularization is targeted to the crural artery supplying arterial flow to the wound angiosome. No data exist on how revascularization changes the blood flow in foot angiosomes. The aim of this study was to evaluate the change in perfusion after infrapopliteal artery revascularization in all foot angiosomes and to compare directly revascularized (DR) angiosomes to the indirectly revascularized (IR) angiosomes.
Methods:
In this prospective study, foot perfusion was measured with indocyanine green fluorescence imaging (ICG-FI) before and after either surgical or endovascular below-knee revascularization. According to angiograms, we divided the foot angiosomes into DR and IR angiosomes. Furthermore, in a subanalysis, the IR angiosomes were graded as IR_Coll+ angiosomes if there were strong collaterals arising from the artery which was revascularized, and as IR_Coll– angiosomes if strong collaterals were not seen.
Results:
A total of 72 feet (28 bypass, 44 endovascular revascularizations) and 282 angiosomes were analyzed. Surgical and endovascular revascularization increased perfusion significantly in both DR and IR angiosomes. After bypass surgery, the increase in DR angiosomes was 55 U and 53 U in IR angiosomes; there were no significant difference in the perfusion increase between IR and DR angiosomes. After endovascular revascularization, perfusion increased significantly more, 40 U, in DR angiosomes compared to 26 U in IR angiosomes (p < 0.05). In the subanalysis of IR angiosomes, perfusion increased significantly after surgical bypass regardless of whether strong collaterals were present or not. After endovascular revascularization, however, a significant perfusion increase was noted in the IR_Coll+ but not in the IR_Coll− subgroup.
Conclusion:
Open revascularization increased perfusion equally in DR and IR angiosomes, whereas endovascular revascularization increased perfusion significantly more in DR than in IR angiosomes. Strong collateral network may help increase perfusion in IR angiosomes.
Keywords
Context and Relevance
The evidence on angiosome concept in patients with chronic limb-threatening ischemia comes from clinical case series. There are no prospective data on the change in perfusion in foot angiosomes after revascularization. Indocyanine green fluorescence imaging has been shown to measure the change in foot perfusion reliably. In this study, foot perfusion was measured before and after bypass surgery and/or endovascular revascularization in all foot angiosomes. The highest increase in perfusion was seen in those angiosomes that were revascularized directly with bypass surgery, and the lowest was seen in angiosomes revascularized indirectly with endovascular revascularization. This is the first study that shows how revascularization changes perfusion in angiosomes.
Introduction
Without revascularization, approximately one in three patients with chronic limb-threatening ischemia (CLTI) and a tissue lesion undergo amputation within 1 year.1–3 Thus, revascularization is recommended to all CLTI patients who are mobile and living independently. 4 The aim of revascularization is to increase arterial perfusion and oxygen in the foot and to achieve wound healing. One key element in the examination of a patient with a suspicion of leg ischemia is the assessment of foot perfusion. 4 Ankle-brachial index (ABI), which is the ratio of systolic pressure in an artery at ankle level to blood pressure at brachial artery, is the most used and easy to perform measurement with handheld Doppler and blood pressure cuff. Toe pressure (TP) measurement and toe-brachial index (TBI) are the basic measurements in vascular laboratory and usually routinely used in patients with suspicion of CLTI in referral centers. 5 Assessment of foot perfusion is also important after revascularization for quality control and evaluation of the effect of the procedure. Traditionally, the hemodynamic change after revascularization has been analyzed using ABI, TBI, or TP values.4,5 Indocyanine green fluorescence imaging (ICG-FI) is a highly repeatable method and potentially beneficial in analyzing the changes in perfusion after revascularization.6,7 ICG-FI allows the analysis of different regions of interest in the foot using the recorded ICG-FI after the examination has been performed.6–8
The discussion on angiosomes in patients with CLTI and tissue lesions has been active during the past 10 years.9–11 The concept was originally presented by Taylor and Palmer. 12 An angiosome represents a three-dimensional block of tissue supplied and drained by a specific “angiosomal vessel.” Later on, Attinger et al. 13 presented that the foot consists of six angiosome regions, each supplied by one of the crural arteries and its terminal branches (Fig. 1). Revascularization is called “angiosome-targeted” if the specific artery feeding the angiosome that is affected by a tissue lesion is treated and direct flow is thereafter achieved from the abdominal aorta to the angiosomal vessel and, thus, directly to the wound area.9–11 According to the angiosome theory, better wound healing is achieved if revascularization is angiosome-targeted than if it is not. Indirect revascularization means that the artery that is revascularized is not the one supplying primarily blood flow to the angiosome where the wound exists.10,11 Recent meta-analyses have reported that wound healing and limb salvage are better after angiosome-targeted, that is, direct revascularization compared to indirect revascularization.14–16 However, the included studies on the angiosome concept in CLTI were mainly retrospective and based on patient records.
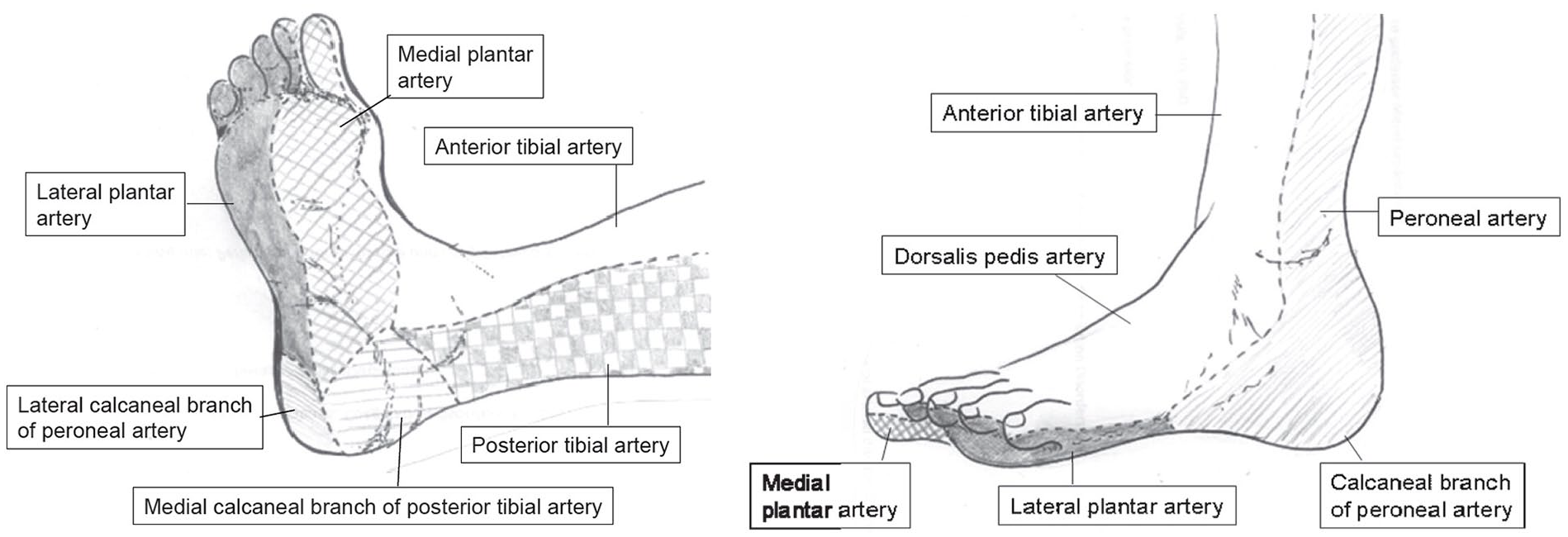
Distribution of the main foot and lower ankle angiosomes (published in the work of Alexandrescu et al. 10 ).
In the current prospective study, the objective was to study the change in perfusion in all foot angiosomes before and after revascularization and compare angiosomes that were revascularized directly and indirectly.
Methods
This is a prospective single-center study performed in Helsinki University Hospital, a tertiary referral center in Southern-Finland providing vascular surgical service to a population of 1.3 million inhabitants. Annually, we perform approximately 1000 revascularizations for CLTI, and half of the patients are treated on emergency basis. We have an active revascularization policy for CLTI patients who are mobile and living at home requiring that the patient does not have severe dementia or very short life expectancy. Our policy is endovascular first in short lesions and stenotic lesions, whereas in long lesions, it is bypass first. In moderate-length lesions, patient’s comorbidities and the availability and quality of autologous vein graft have a major role in decision-making. Our revascularization techniques have been published previously.11,17 In bypass surgery, we prefer autologous vein and actively use alternative veins, such as arm veins, if great saphenous vein is not available. During a bypass surgery, adjunctive endovascular intervention is performed, if required, to achieve unrestricted inflow. The best-possible crural artery leading to foot is selected as the outflow artery. In case of more than one possibility, we respect the angiosome concept. Endovascular procedures are performed by interventional radiologists or vascular surgeons under local anesthesia. Our goal is to achieve at least one open arterial line to the foot. If several crural arteries have an occlusive disease, our goal is to intervene all lesions; thus, very often, intervention is done to more than one crural artery.
Study patients and perfusion assessment
Consecutive patients who were scheduled for a revascularization of crural arteries due to CLTI during a 6-month period between September 2015 and March 2016 were asked to participate in the study. Patients were informed on the details of the study, and they signed a written consent. Participation did not affect the patient’s revascularization procedure and postoperative care. The preoperative evaluation included a clinical assessment, as well as ABI and TP measurements. One or two days before the revascularization, ICG-FI was performed twice: once on the plantar and once on the dorsal side of the foot with a 30-min interval between the two studies. After ICG-FI to the plantar and dorsal side of the foot, ABI and TP measurements were repeated within 2 days after the revascularization. In addition, we registered patient’s age, sex, and risk factors (diabetes, hypertension, coronary artery disease, smoking, and dyslipidemia).
Indocyanine green fluorescence imaging
In our vascular laboratory, ICG-FI has been used for measuring foot perfusion since 2010, and we have described the details of the ICG-FI protocol previously. 7 ICG-FI assessments were performed by one study nurse. The measurements were taken in a room with no daylight and a temperature of 20 °C–25 °C. At the beginning of the examination, the patient was lying in a supine position, and after a 15-min rest, the ICG-FI camera was positioned 20 cm above the plantar region of the foot (Fig. 2A). ICG (0.1 mg/kg) was injected intravenously into the brachial vein, after which the foot was recorded with an infrared camera for 4 min. The second examination on the dorsum of the foot took place after a 20-min break to let the ICG from the first study to disappear from the body before the new examination.
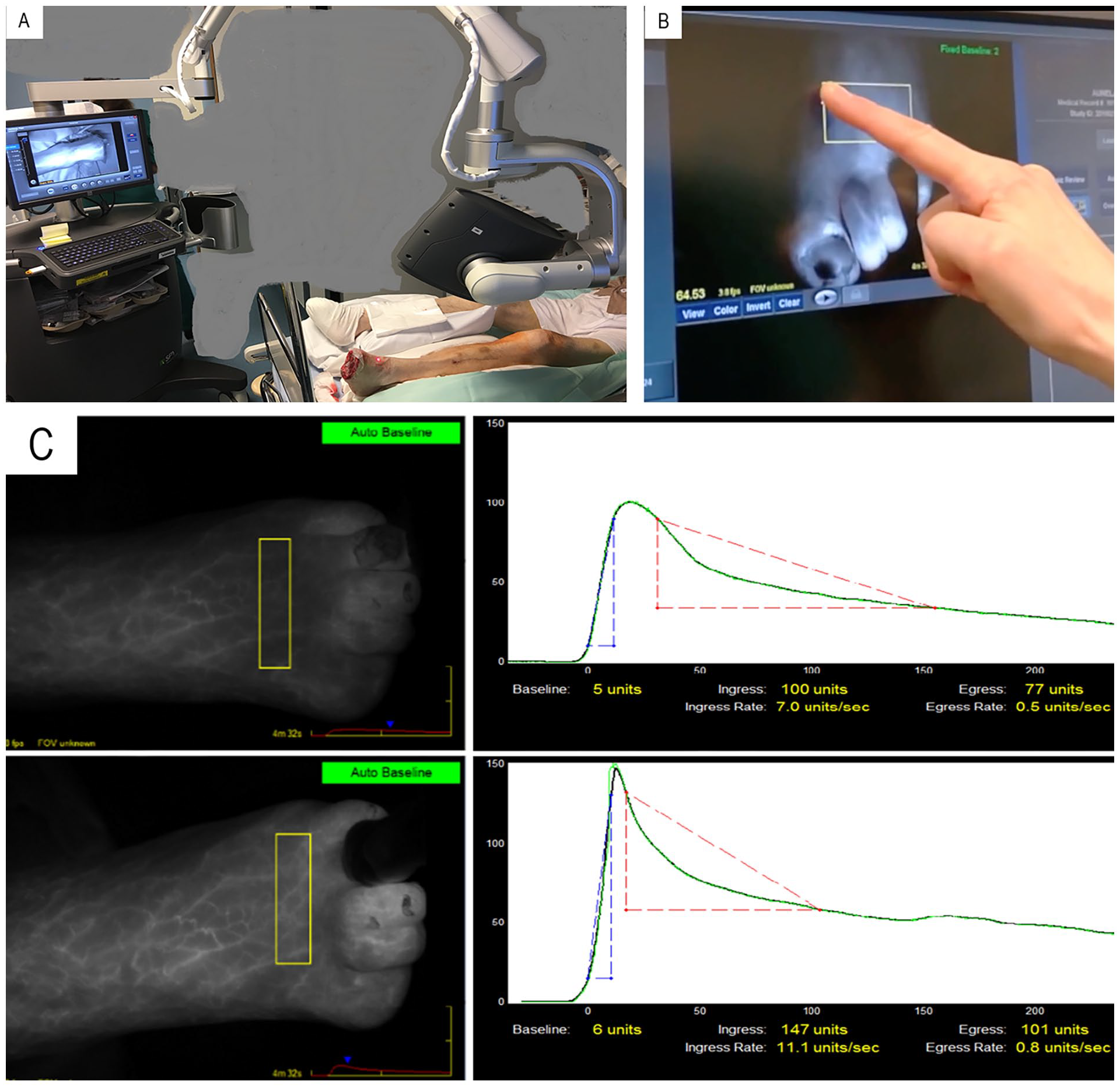
Indocyanine green fluorescence imaging. (A) Set up during the procedure. (B) Selecting region of interest from the recorded image. (C) Time intensity curve before and after revascularization.
The ICG-FI recordings were analyzed using regions of interest according to each foot angiosome (Fig. 2B), and the following variables were extracted from the time–intensity curve: (1) maximum intensity, which is the absolute value of the maximum intensity in units (U) in the time–intensity curve; (2) SPY10 (U), which is the intensity in units achieved during the first 10 s after the foot starts to gain intensity; and (3) intensity rate (U/s), which is the value from the time–intensity curve describing the increase in maximum intensity per second (Fig. 2C). During the ICG-FI recording, an automatic baseline setting allowed adjustment for possible confounding factors, such as possible daylight.
Angiogram review
After the ICG-FI studies before and after revascularization had been analyzed, all angiograms were reviewed. According to the achieved revascularization, foot angiosomes were divided into (1) angiosomes that received their blood supply from the artery that underwent revascularization (directly revascularized (DR) angiosomes) and (2) angiosomes that were revascularized indirectly (indirectly revascularized (IR) angiosomes). A subanalysis based on angiograms was performed for the IR angiosomes, and they were divided into two groups: (2a) indirect revascularization with presence of strong collaterals arising from the artery that underwent revascularization (IR_Coll+ angiosomes) and (2b) indirect revascularization with no good collaterals to the angiosome from the artery that was revascularized (IR_Coll− angiosomes). The angiograms were evaluated by two researchers (MV, NS) who were blinded to the ICG-FI measurements.
Statistical analysis
SPSS 25.0 was used in the statistical analysis. The continuous variables are expressed as mean ± standard deviation (SD) and as median with interquartile range (IQR). Dichotomous variables are expressed as percentages. A comparison of the perfusion variables before and after revascularization was made using the paired samples t test. We analyzed the change in foot perfusion in the DR and IR angiosomes using the maximum intensity, SPY10, and intensity rate.
The study plan was approved by the Ethical Committee of Helsinki University Central Hospital.
Results
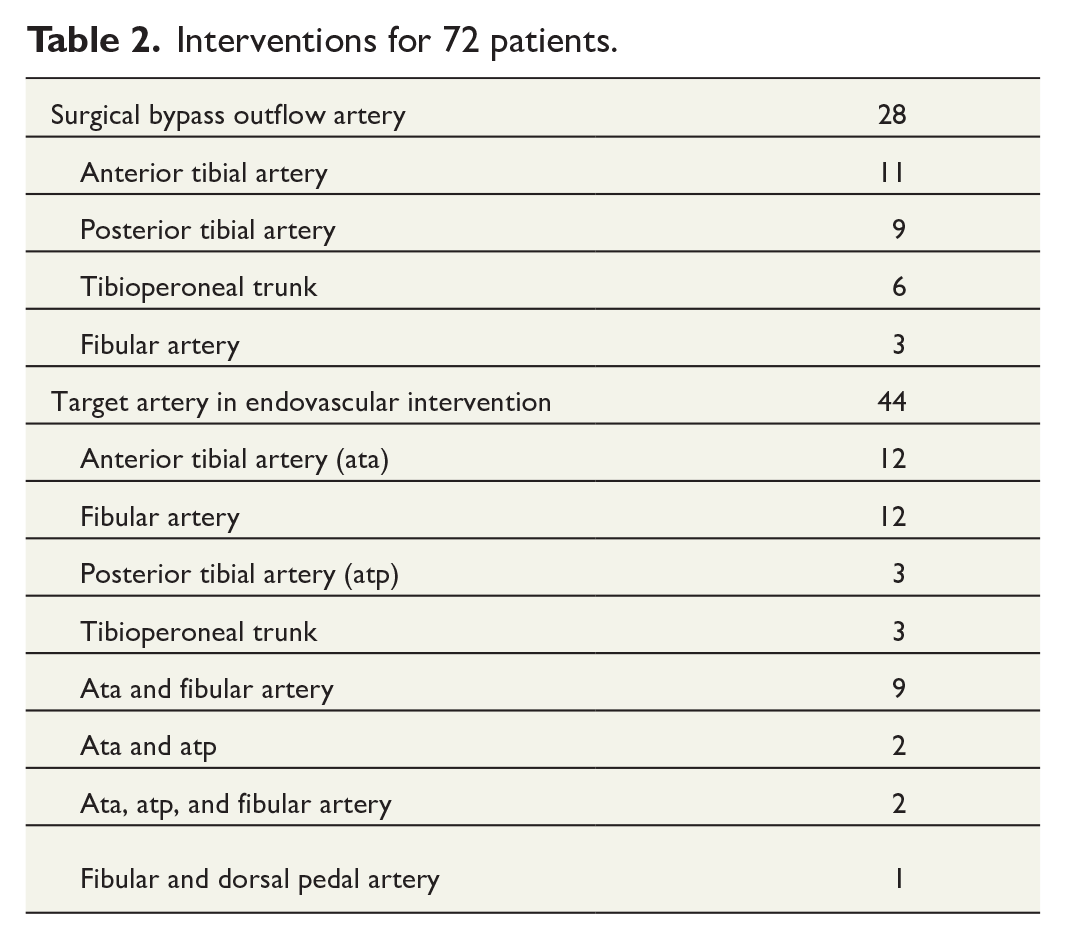
A total of 72 patients were included in the study. Basic characteristics of the study patients are presented in the Table 1. Twenty-eight patients underwent surgical bypass, and 44 patients underwent endovascular revascularization (Table 2).
Basic demographics of the study patients.
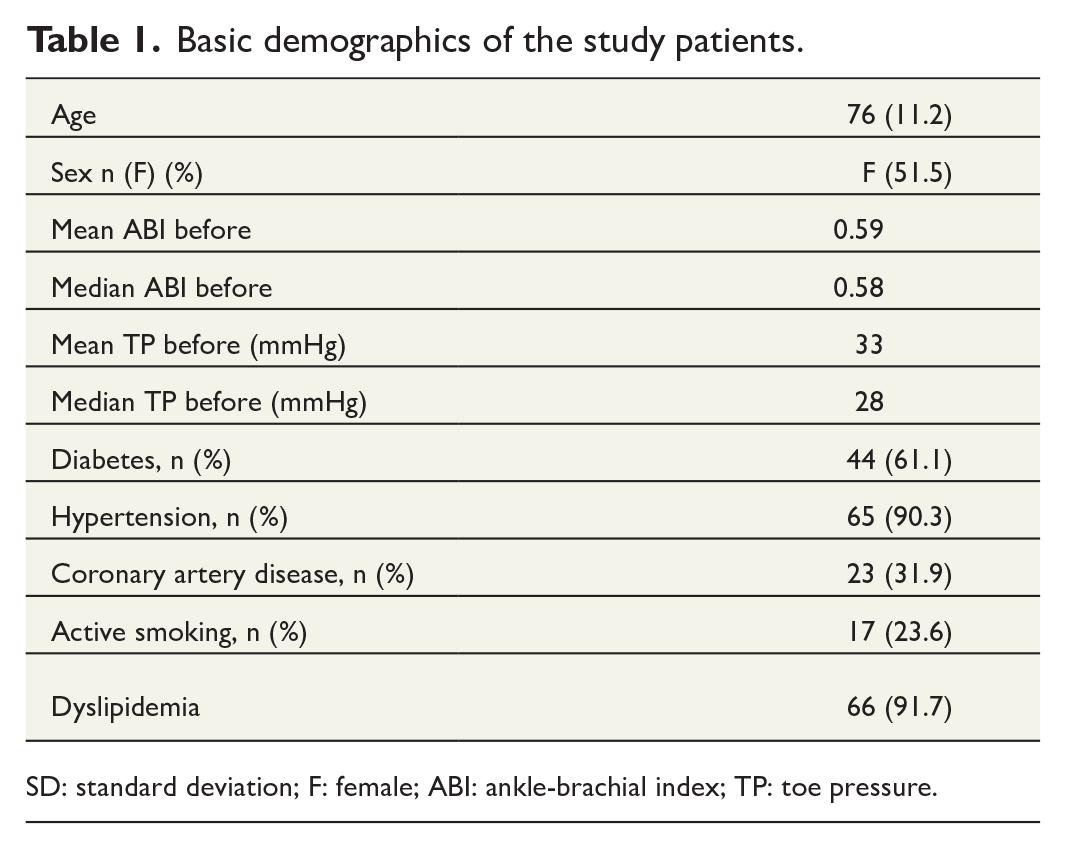
SD: standard deviation; F: female; ABI: ankle-brachial index; TP: toe pressure.
Interventions for 72 patients.
The number of angiosomes in the analysis was 282, of which 129 (45.7%) were revascularized directly (DR angiosomes) and 153 (54.3%) indirectly (IR angiosomes). ABI was available before and after revascularization for 32 patients, and TP for 40 patients. After revascularization, the mean ABI increased from 0.59 to 0.82 (p = 0.02), and the mean TP from 33 mmHg to 41 mmHg (p = 0.06).
ICG-FI was successful in all patients, and no adverse events related to the study were seen. Overall, the mean maximum intensity in DR angiosomes increased by 46 U (from 81 to 127 U, p < 0.001). The mean maximum intensity in IR angiosomes increased by 39 U (from 88 to 127 U, p < 0.001). There was no significant difference in the overall increase of mean maximum intensity between DR angiosomes and IR angiosomes (p = 0.11).
After bypass surgery, the mean maximum intensity increased by 55 U in DR angiosomes (from 72 to 127 U, p < 0.001) and by 53 U in IR angiosomes (from 81 to 134 U, p < 0.001). The increase was equally high in both DR and IR angiosomes after open surgery (p = 0.96). After endovascular revascularization, the increase in DR angiosomes was 40 U (from 85 to 125 U, p < 0.001) and 26 U in IR angiosomes (from 91 to 117 U, p < 0.001). After endovascular revascularization, the increase was significantly higher in DR angiosomes than that in IR angiosomes (p = 0.045; Fig. 3A).
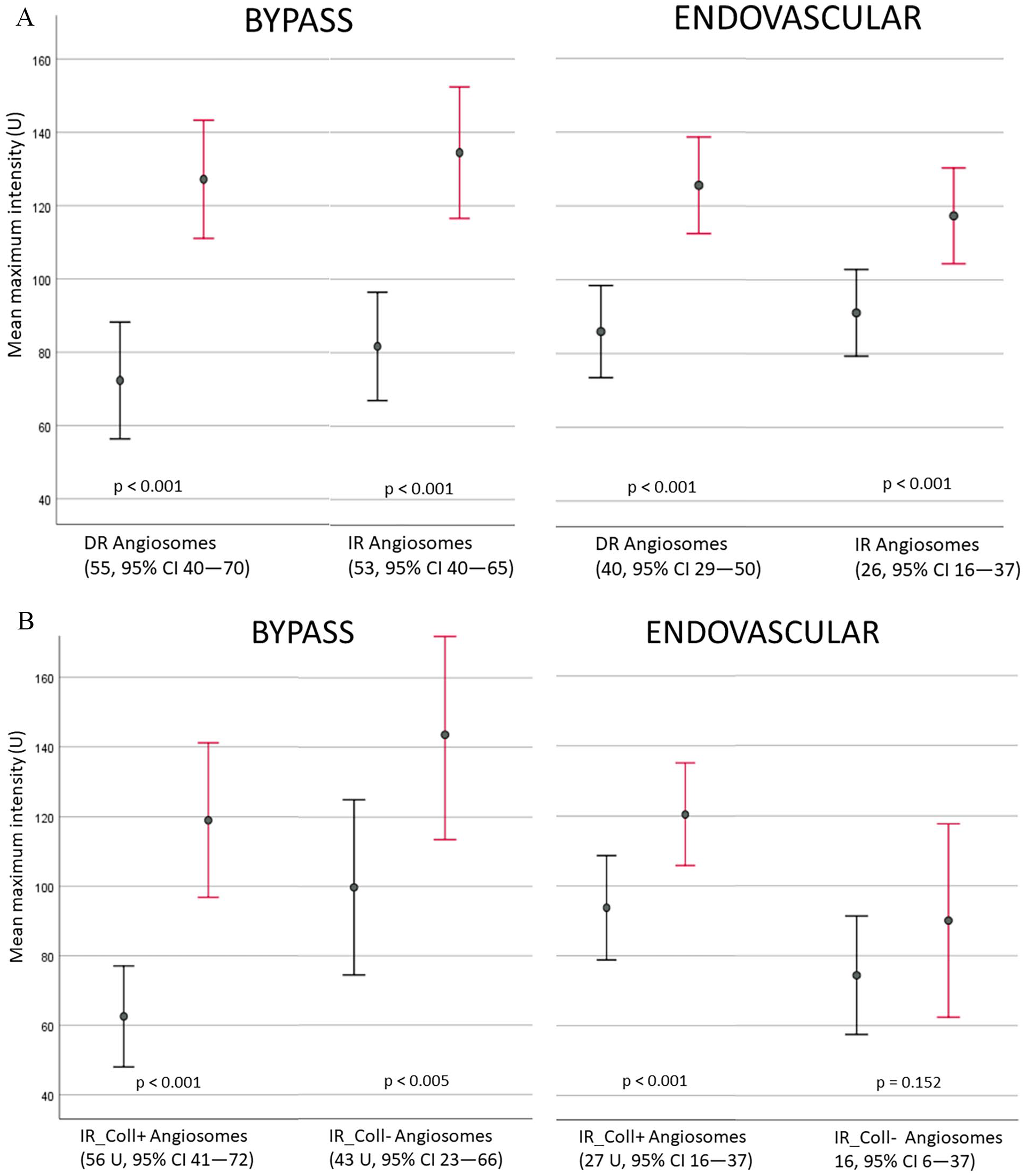
(A) Mean maximum intensity (with 95% confidence intervals) before (black) and after (red) bypass or endovascular revascularization in directly revascularized (DR) and indirectly revascularized (IR) angiosomes. (B) Mean maximum intensity (with 95% confidence intervals) before (black) and after (red) bypass or endovascular revascularization in angiosomes with strong collaterals arising from the revascularized artery (IR_Coll+) and angiosomes without strong collaterals (IR_Coll−).
An additional subanalysis was performed for IR angiosomes according to the collateral network in the foot, as described in the Methods section (Fig. 3B). Among bypass patients, the maximum intensity increased by 56 U in IR_Coll+ angiosomes (from 62 to 119 U, p < 0.001) and by 44 U (from 104 to 144 U, p < 0.005) in IR_Coll− angiosomes. With endovascular treatment, the mean increase in the maximum intensity was 27 U in IR_Coll+ angiosomes (from 93 U to 120 U, p < 0.001) and 16 U (from 74 to 90 U, p = 0.152) in IR_Coll− angiosomes.
The variables analyzed from the ICG-FI images in each angiosome (maximum intensity, intensity 10 s, and intensity rate) are presented in Supplemental Table S1.
Discussion
To our knowledge, this is the first prospective study to compare the perfusion change in foot angiosomes before and after revascularization of crural arteries. There was a greater increase in perfusion in DR angiosomes than in IR angiosomes, especially after endovascular revascularization, supporting the angiosome concept in concurrence with published meta-analyses.14–16 The highest increase in perfusion was measured in the angiosomes that were DR, followed by angiosomes which were perfused through a good collateral from a revascularized artery. The lowest increase was observed in the angiosomes that were either not revascularized directly or with no good collateral network from the revascularized artery.
The difference in the increase in IR angiosomes between bypass and endovascular intervention is interesting, but not extremely surprising. After bypass with a good-quality vein, blood pressure is effectively transferred to the distal outflow artery, which has to be of reasonable quality to allow distal anastomosis. Bypass delivers blood flow directly to the target area in the foot with little resistance and provides blood flow in both directions from the distal anastomosis. In contrast, after endovascular revascularization, blood flow has to travel to the foot via a diseased artery, segments that have been ballooned with potentially more resistance and inferior flow compared with a good venous conduit.
This higher pressure after bypass may also better reach small collaterals in the foot. We used ICG-FI to evaluate the change in perfusion. ICG-FI is well tolerated, with a very low incidence of adverse events. In earlier studies, we have found that the time–intensity curve is very repeatable, which makes it an ideal method to investigate change in perfusion.6–8 However, ICG-FI is highly individual, meaning that the values of two persons cannot be compared with each other, and there is no available threshold for distinguishing CLTI. The wide SD of ICG-FI measures also reflects this phenomenon. Furthermore, a fulminant infection of the foot increases the maximum intensity and makes the perfusion appear better than it actually is. If the two measurements are timed very close to each other, this has a small effect on the pre–post comparison. However, if there is a longer time period between the measurements and the treatment of the infection has been effective in the meantime, it is probable that the impact of inflammation is lower in the second study, and the change in ICG-FI is not necessarily associated with perfusion changes alone. In the current study, we had two patients in whom it was obvious that an infection increased the ICG-FI maximum intensity in the first ICG-FI study. In both patients, the revascularization and second ICG-FI study took place within 2 days, and the control imaging showed an increase in perfusion. We recommend that the presence of an infection should be clearly stated in an ICG-FI report so that it can be considered as a confounding factor in later evaluation. In the majority of the CLTI patients with a chronic wound or gangrene, the infection is mild and does not impact the interpretation of ICG-FI results.
In a recent study, Unno et al. 18 employed a near-infrared spectroscopy oximeter (TOE-20) for real-time monitoring of regional tissue oxygen saturation (rSO2) in the foot angiosomes of 23 CLTI patients who underwent recanalization of the superficial femoral artery. In their study, rSO2 increased in all angiosomes after revascularization, and the increase was larger if the crural artery feeding the angiosome was patent when compared to the angiosomes with an occlusion in the feeding crural artery. In concurrence with our fndings, a higher increase was seen in rSO2 in the angiosomes that had a direct line from the end of the aorta to the angiosome, when compared to the angiosomes without a direct line. A recent study with 52 patients used ICG-FI before and after revacularization, and they did not find significant difference in perfusion increase between DR and IR angiosomes. 19 In their series, only two were crural revascularizations, and the rest (95%) were aortoiliac and femoropopliteal interventions.
The impact of collaterals has been evaluated in earlier clinical studies.20–22 In a meta-analysis on the angiosome concept and the importance of collaterals, with over 4000 endovascular revascularizations, the overall wound healing rates were significantly higher for direct revascularization than for indirect revascularization, but no difference was seen between direct revascularization and indirect revascularization with significant collaterals. 22 Leg salvage was superior in the DR group, but it was significantly better in IR patients with collaterals than in IR patients without collaterals. Again, the outcomes in these retrospective clinical trials are in line with our findings on perfusion increase after revascularization.
Our study has limitations. First, the number of patients is small. However, the number of angiosomes analyzed is large enough to achieve a relevant comparison between the groups. Second, the analysis of collaterals in the foot is difficult, as the angiograms may not always show all the collaterals, if the concentration of the contrast medium stays low. Especially in the case of patients undergoing bypass surgery with long occlusions in preoperative images, the quality of the angiogram was sometimes compromised. However, we also used angiograms that were taken after bypass surgery—if, for example, the bypass graft underwent balloon angioplasty—when the contrast medium concentration was better in the foot region. This limitation did not affect the comparison between DR and IR angiosomes, which was reliable in all patients, but it may have affected the subanalysis comparison between IR Coll+ and IR_Coll− angiosomes.
The current study shows the immediate increase in ICG-FI perfusion measures, and our results support the angiosome concept. However, the ultimate question is, “does this have an impact on wound healing?,” and this should be addressed in future studies with higher number of patients with CLTI and tissue lesions and a long-enough follow-up to assess the effect of increased perfusion in ICG-FI studies on wound healing. In our earlier study, we showed that ICG-FI can be used for immediate quality control after revascularization. 7
In conclusion, perfusion after endovascular revascularization increased more in angiosomes that were DR compared with IR angiosomes. Furthermore, it seems that the increase in IR angiosomes is related to collaterals; if there are good collaterals, the perfusion increases more than it does in angiosomes where poor or no good collaterals exist from the revascularized artery.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241242205 – Supplemental material for Perfusion increase in foot angiosomes: Comparison between direct and indirect revascularization of crural arteries
Supplemental material, sj-docx-1-sjs-10.1177_14574969241242205 for Perfusion increase in foot angiosomes: Comparison between direct and indirect revascularization of crural arteries by Maarit Venermo and Nicla Settembre in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.