
Abstract
Endovascular treatment for revascularization in patients with chronic limb-threatening ischemia (CLTI), which is commonly found in patients with diabetes mellitus demonstrates a variable result of vessel patency, wound healing rate, and limb salvage rate. The angiosome concept has been adopted to determine the best target arterial path (TAP) for revascularization for wound healing in CLTI patients. Recent publications demonstrated the benefit of angiosome-targeted revascularization to guide the endovascular treatment in patients CLTI. The best TAP under angiosome concept by direct revascularization with at least 2 of 3 below-the-knee arteries runoff to restore in-line pulsatile blood flow to the ischemic tissue shows the best patency and high rate of wound healing. However, the clinical evidence and application of the angiosome concept in daily practice are difficult and not well established. The vascular territories, collateral vessel, wound area, and locations which associated with angiosome are varied. This article review aims to summarize the concept of angiosome-targeted revascularization and multivessel revascularization for application to the real-world practice under the evidence-based data.
Keywords
Chronic limb-threatening ischemia (CLTI) arises from peripheral arterial disease (PAD) of the lower extremities. This is caused by the accumulation of atherosclerotic plaque, which eventually leads to lower limb tissue ischemia.1–4 This results in symptoms such as foot pain at rest, ischemic ulcers, and tissue necrosis (gangrene). Although the CLTI is found in only 1% to 3% of all PAD cases, it has a high amputation rate of up to 30% per year and a high mortality rate. 5 The amputation reduces the functional capacity and quality of life for CLTI patients, especially in patients with comorbidities of cardiovascular disease.5–7 Therefore, CLTI patients need to undergo appropriate revascularization surgery to save limb and save life.8–10
Tissue loss from ischemic ulcers and gangrenous tissue in CLTI patients is very hard to heal, leading to infections and loss of lower limbs. Based on the TIMERS concept, the factors in wound closure, which are described in many guidelines for treatment and promotes wound healing through standard care and adjuvant therapies, especially for chronic and complicated wounds, are very important. TIMERS consist of “T” tissue viability, which refers to tissue management. “I” infection/inflammation refers to controlling the substrates related to the body's inflammation process. “M” moisture balance refers to the balancing of wound moisture. “E” wound edge refers to wound edge management. “R” repair/regeneration refers to repairing and reinforcing wound tissue from various processes. “S” refers to social factors and patient factors that related to the patient's family, society, and the environment, respectively.11–13
The blood transported through the vessels into tissue loss or wound areas plays a vital role in delivering oxygen and nutrients, as well as mediators or various cells that are crucial in every process of wound healing. This is associated with the principle of the TIMERS concept. “T” controls the presence of devitalized tissue resulting from a lack of blood and oxygen, which is vital for the appropriate wound bed preparation for healing. “I” blood controls and transports substances related to the body's inflammatory process and creates immunity to reduce the risk or treat wound infections, including reducing the accumulation of bacterial biofilms. “M” blood regulates the moisture content of the wound. Wounds lacking blood supply tend to be dry and lack sufficient moisture. “E” blood plays a role in controlling and preventing the curling of wound edges (edge rolled or epibole) from inappropriate wound healing due to lack of wound blood supply. Proper wound edge contraction reduces wound size more quickly and stimulates epithelial tissue growth (epithelialization). “R” blood aids in transporting growth-promoting substances and accelerates tissue wound healing, such as various growth factors and cytokines. 14 “S” Surgical procedures to increase blood flow to areas with foot tissue loss can accelerate wound healing, reducing the time and costs associated with chronic wound care in the long run, leading to a decrease in the patients’ societal issues.11–13
Wound care in CLTI patients is essential to increase blood supply to the tissue loss area, along with the standard treatment through revascularization, which can be divided into 2 types: (1) open arterial bypass surgery and (2) endovascular therapy.15,16 The most appropriate method of revascularization for each patient depends on several factors, including the anatomical characteristics of the artery’s occlusion according to Trans-Atlantic Inter-Society Consensus II or Global Limb Anatomic Staging System (anatomic suitability and stage),8,9,17,18 the nature of ischemia (limb severity) as per Wound, Ischemia, and foot Infection (WifI; stage which includes the size of the ischemic wound (major and minor tissue loss), 18 life expectancy, availability of vein graft for open bypass surgery, comorbidities and operative risk, clinical severity of CLTI symptoms (rest pain, minor tissue loss, and major tissue loss), physician and staff expertise, availability of equipment for revascularization, and patient preference.2,18–22 Revascularization aims to increase blood flow to the limb to treat rest pain, ischemic ulcers, and tissue necrosis for limb amputation prevention. Among the group with ischemic ulcers and tissue death, it is the most severe form of PAD, which has a high rate of limb loss. Chronicity of the ischemic ulcers or gangrenous tissue can lead to multiple episodes or long-standing infections, eventually resulting in the need for amputation to lifesaving before septicemia or septic shock occurs.2,3,15
Endovascular therapy is increasingly being used for revascularization due to the comorbidities of patients and the advancements in medical technology and equipment. This focuses on delivering blood to areas with tissue loss from ischemic ulcers and gangrenous tissue for wound healing. However, the results of endovascular treatment in CLTI patients, where arterial occlusive disease is commonly located below the knee and the ankle, commonly found in diabetes mellitus (DM) patients, show low patency and limb salvage rate. Therefore, endovascular revascularization must consider the vascular territories to address the arterial occlusive lesion to match the area with ulcers or gangrenous tissue, which is defined as the “angiosome concept.”3,23–26 The Angiosome concept, which describes the territorial zones of foot and lower leg supplied by specific blood vessels, was first introduced in 1987. In particular, the angiosome of the foot is divided into 6 parts, derived from the branches of the posterior tibial artery (3 areas), the peroneal artery (2 areas), and the anterior tibial artery (1 area), as shown in Figure 1. These blood vessels are perfused to various tissues, including the skin, subcutaneous tissue, fascia, muscle, and bone. 24
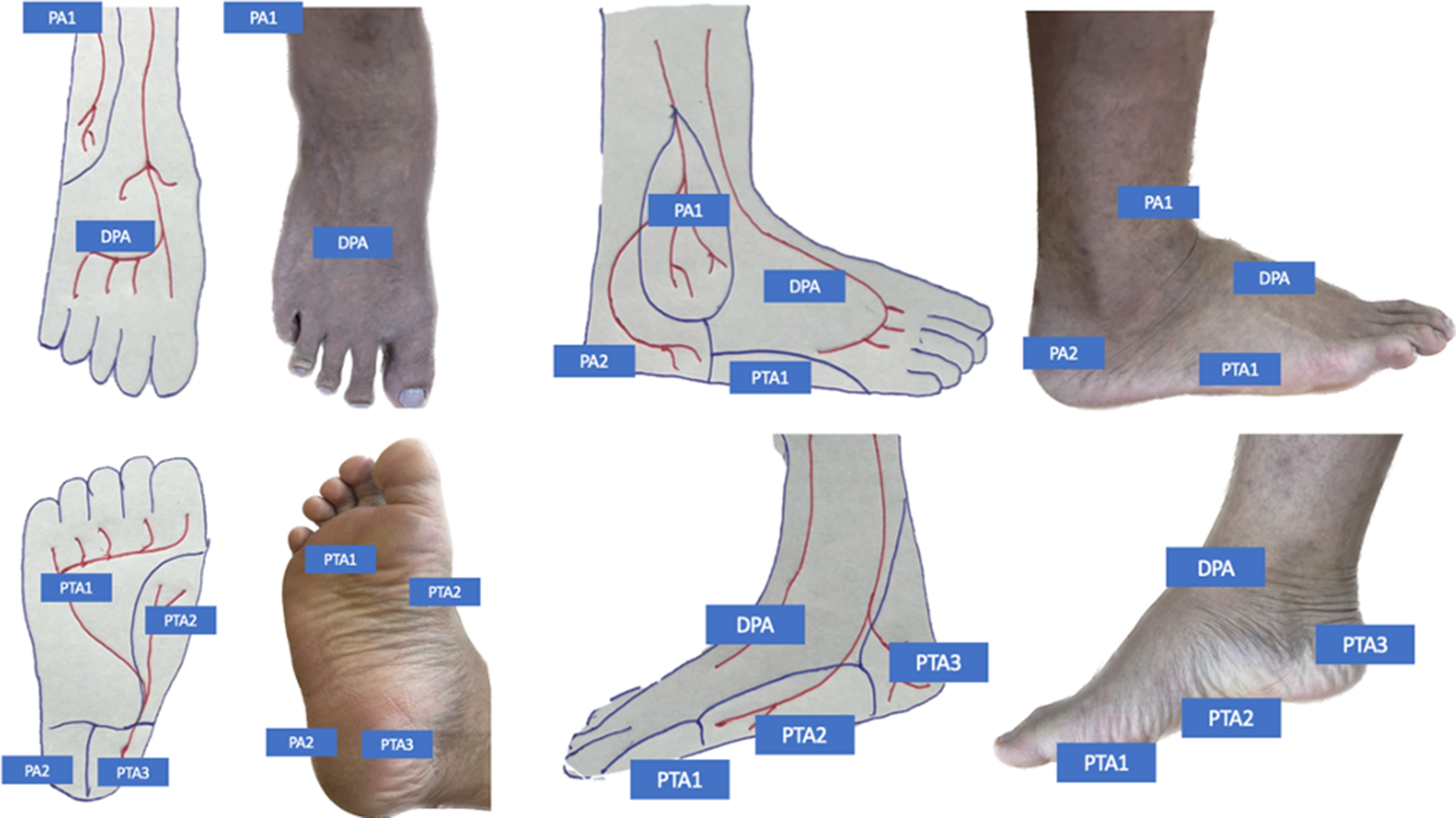
The vascular territories that supply blood to areas of the leg and foot (Angiosome concept). PA1, Anterior perforating branch of peroneal artery; PA2, Calcaneal branch of peroneal artery; PTA1, Lateral plantar branch of posterior tibial artery; PTA2, Medial plantar branch of posterior tibial artery; PTA3: Calcaneal branch of posterior tibial artery; DPA, Dorsalis pedis artery of anterior tibial artery.
The Angiosome Concept and Multivessel Revascularization Related to Wound Healing in the Foot of CLTI Patients
The anatomy of the 3 main arteries of the leg that provide branches of the small arteries of the foot, which direct blood according to the territories of the angiosome in 6 areas of the foot, informs the best choice of target artery pathway for revascularization surgery. The specific artery route that can provide blood to areas with tissue loss is defined as the target arterial path (TAP). 2 Vascular surgeon, angiologist, and interventionist are choosing the best vessel for endovascular revascularization based on the appropriate angiographic image as the optimal arterial pathway to restore in-line pulsatile blood flow to the ankle and foot associated with angiosome concept for the best healing rate of the wound. Therefore, the outcomes of the endovascular revascularization based on the angiosome concept can be categorized into 3 types including (1) Direct perfusion of blood flow to the angiosome of the tissue loss area (direct revascularization [DR]), (2) Indirectly perfusion blood flow to the angiosome of the tissue loss area via collateral arteries (indirect revascularization through collaterals [IR-tc]), and (3) Indirectly perfusion blood flow to the other area of the angiosome which not associated with the tissue loss area (indirect revascularization without collaterals [IR-wc]) as shown in Figure 2.3,27
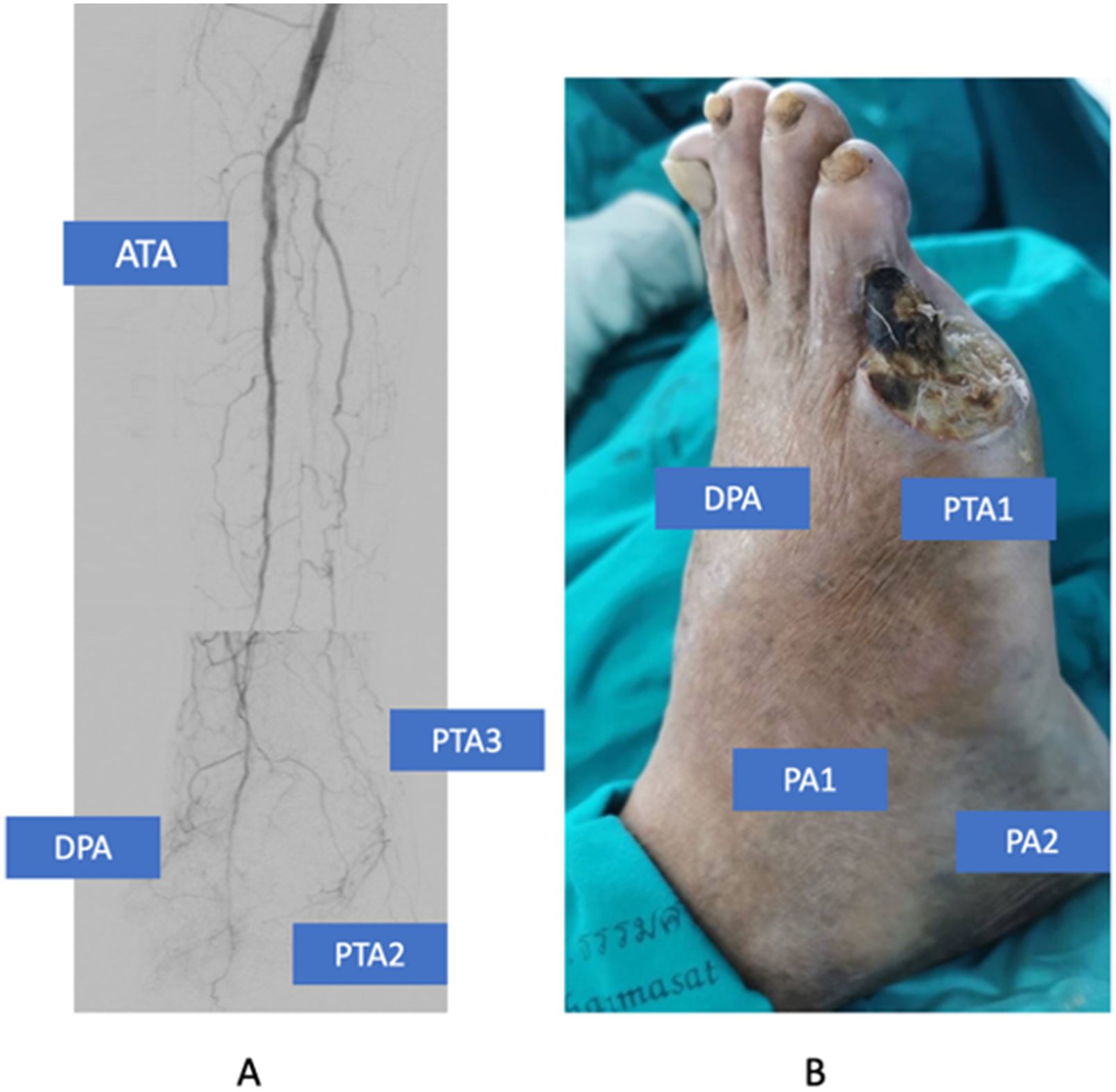
The angiogram of right below the knee arteries demonstrated the suboptimal target arterial path to restore in-line pulsatile blood flow to the DPA to the foot through ATA without the collateral vessel to tissue loss area (indirect revascularization without collaterals [IR-wc]) and absent of lateral plantar artery and pedal arch (A), left fifth toe which need the blood supply from lateral plantar branch of posterior tibial artery or collateral vessel from pedal arch to healing of the wound (B). PA1, Anterior perforating branch of peroneal artery; PA2, Calcaneal branch of peroneal artery; PTA1: Lateral plantar branch of posterior tibial artery; PTA2: Medial plantar branch of posterior tibial artery; PTA3, Calcaneal branch of posterior tibial artery; DPA: Dorsalis pedis artery of anterior tibial artery.
One ischemic wound may need perfusion from one or more areas of angiosome which supply from 3-vessel of below the knee. Especially in CLTI patients with major tissue loss, the revascularization of more than one vessel may need to salvage the limb because of a lack of collateral vessel or foot arch vessel to perfuse the large area of ischemic tissue (Figures 3 and 4). In addition, small arterial disease (SAD) or below-the-ankle arterial occlusive disease (inframalleolar disease), which usually occurs in end-stage renal disease and DM patients, is essential in determining endovascular therapy outcomes for revascularization. Related to SAD patients, one below-the-knee artery may not achieve wound healing for CLTI because of a lack of collateral network from the main revascularized vessel to the ischemic tissue area.28,29 Troisi and colleagues report the positive impact on time to healing, limb salvage, and survival in diabetic patients with foot wounds undergoing infrainguinal endovascular revascularization by pedal arch status. The absent pedal arch is associated with high amputation, low limb salvage rate, and survival. 28 Nakama and colleagues reported the outcome of inframalleolar revascularization. The result shows the trend of increasing limb salvage and decreasing intervention rate by adjunctive pedal artery angioplasty. The time to wound healing was significantly shorter (211 days vs 365 days, P = .008), and the wound healing rate was significantly higher (57.5% vs 37.3%, P = .003) and in the adjunctive inframalleolar revascularization patients. 30
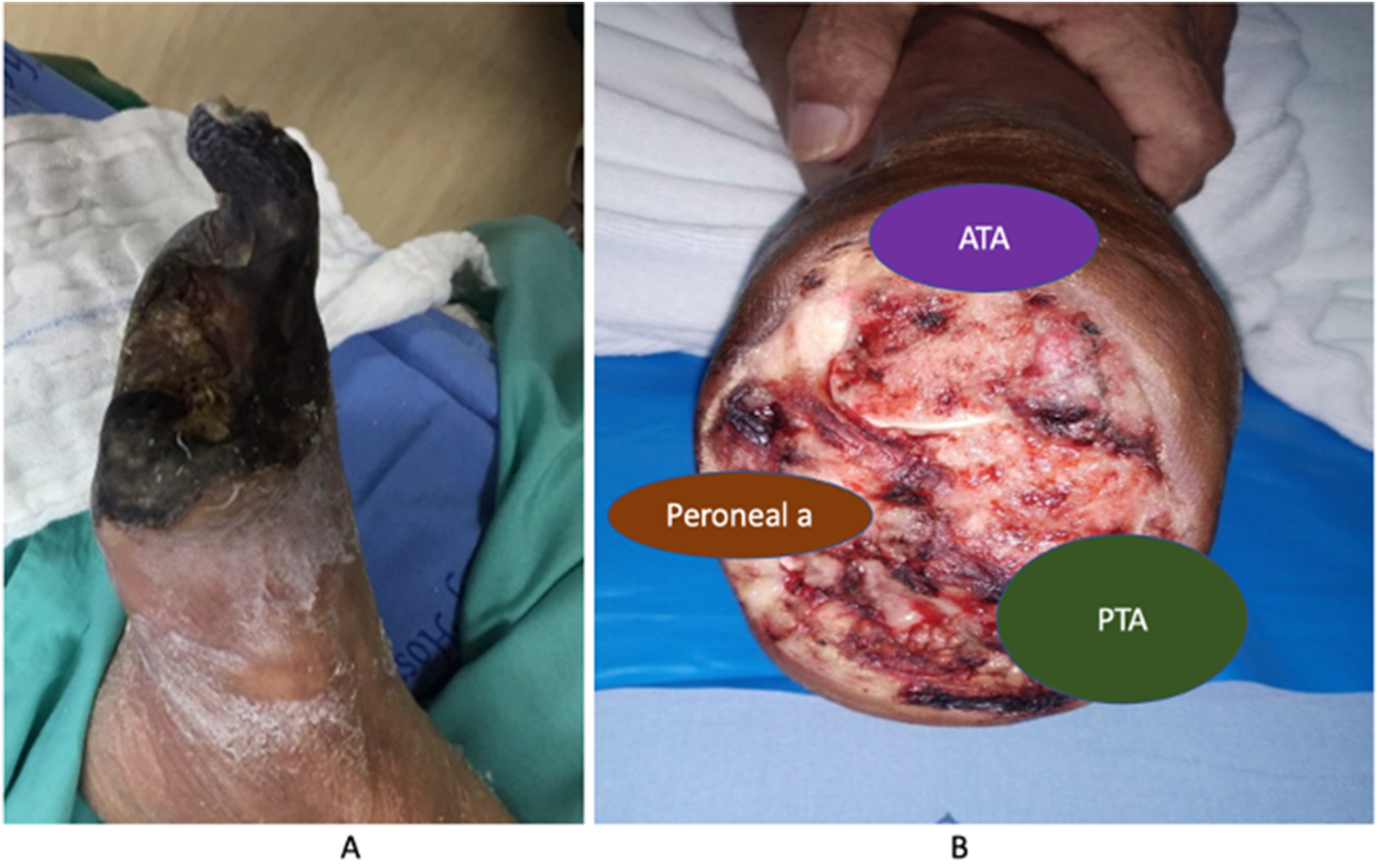
Right forefoot gangrene due to infrapopliteal occlusive disease associated with the absence of pedal arch in patients with CLTI (A), right lisfranc amputation shows the areas of angiosome which perfused the blood to the healing of foot stump after forefoot amputation (B). CLTI, chronic limb-threatening ischemia.
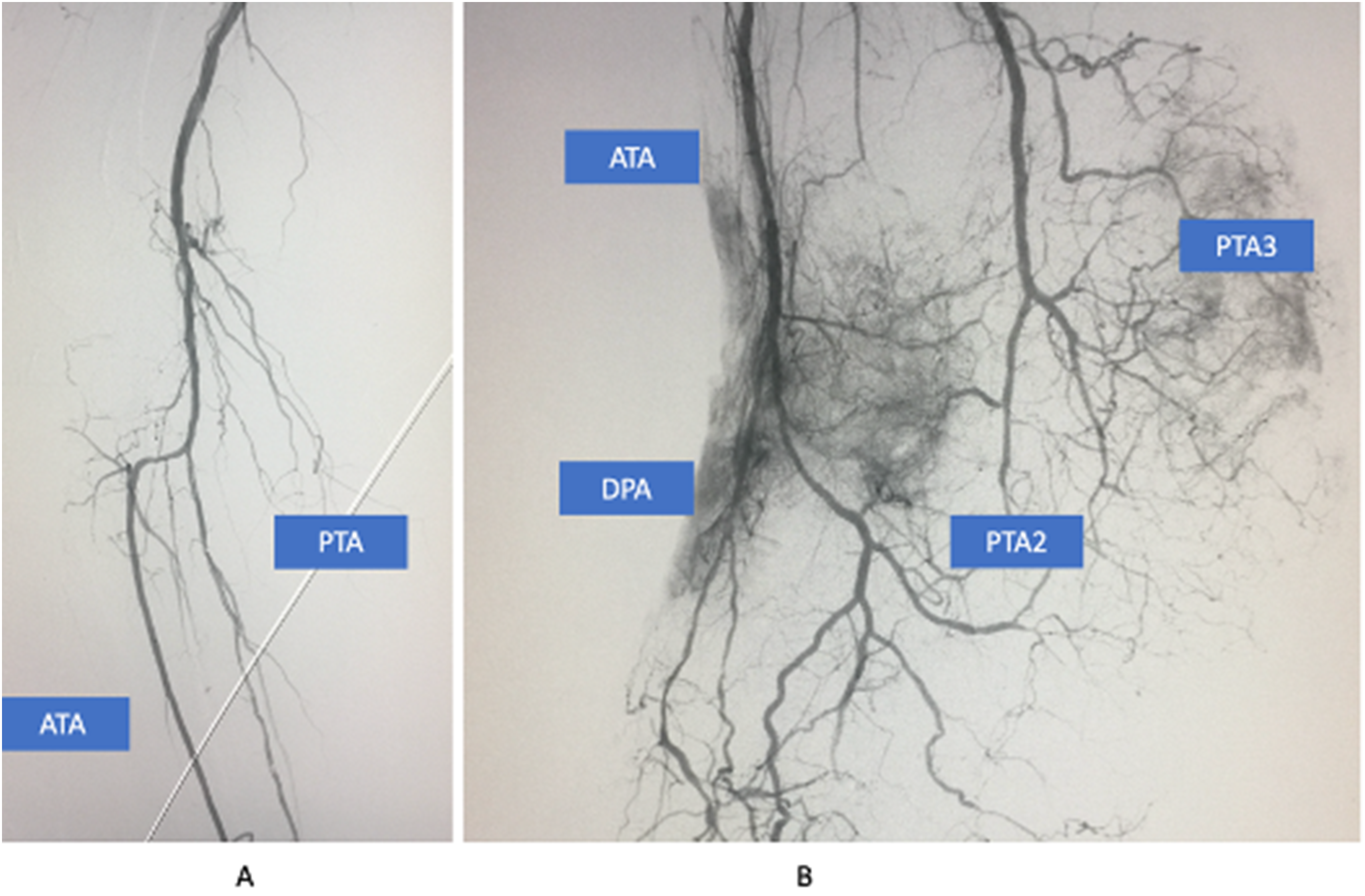
The angiogram of right below the knee arteries demonstrated the optimal outcome of 2 vessel revascularization for 2 target arterial paths from the medial plantar and calcaneal branch of PTA and ATA (dorsalis pedis artery), which directed perfused to a large area wound of lisfranc amputation stump. PTA2: Medial plantar branch of posterior tibial artery; PTA3, Calcaneal branch of posterior tibial artery; DPA, Dorsalis pedis artery of anterior tibial artery.
Although some literature report the failure to demonstrate the benefit of multiple vessel of below-the-knee revascularization when compared with a single vessel for limb salvage and unnecessary to treat the largest number of arteries possible in CLTI patients.31,32 The 2-vessel below-the-knee revascularization are increasing of wound healing rate (87% vs 79%, P = .003), shorter time to wound healing (83 vs 142 days; P = .01), and lower reintervention rate (15% vs 35%; P = .03) when compared with single vessel below the knee revascularization. 33 Athayde Soares and colleagues report the main factors associated with worse outcomes in the endovascular treatment of femoropopliteal occlusive. The single tibial vessel or isolated popliteal artery runoff is associated with loss of primary patency (hazard ratio [HR] = 7.9, 95% confidence interval [CI] = 1.41-14.3, P = .005) and limb loss (HR = 4.69, 95% CI = 1.22-10.5, P = .039). 34 In addition, early failure of endovascular therapy for isolated tibial disease significantly increases 30-day major amputation and adverse limb events. 35
Zheng and colleagues report the prospective study of using the angiosome concept for treating infrapopliteal occlusive disease in patients with critical limb ischemia through endovascular therapy and determining the clinical significance of collateral vessels with a follow-up duration of 1 year. The endovascular therapy to revascularization in patients who have tissue loss from CLTI using the IR-wc method has a significantly higher rate of nonhealing wounds than DR and IR-tc (83.4%, 31.7% [P < .001] and 34.8% [P < .001], respectively). The limb salvage rate of the IR-wc method is significantly lower than DR and IR-tc (70.4%, 89.2% [P < .001], and 85.4% [P = .0013], respectively). Furthermore, there is no significant difference in the rate of unhealed ulcer and limb salvage rate between the IR-tc and IR-wc groups. 27 There is a meta-analysis that included 29 studies found that the DR method of revascularization has a significantly higher wound healing and limb salvage rate than IR, with an odd ratio of 0.51 (95% CI: 0.39-0.68, P < .001) and 0.37 (95% CI 0.24-0.58, P < .0001). The time to complete wound healing in the DR group was also shorter than in the IR group, and there were no effects in the group for mortality rates or rerevascularization.3,23 However, a recent meta-analysis, which included 36 studies to compare the effectiveness between DR and IR, open and endovascular treatment for limb outcomes inpatients with DM and PAD is still inconclusive with the very low level of certainty of evidence. However, the wound healing and major amputation outcomes were favored for DR than IR in the majority of studies in the meta-analysis. The amputation-free survival and limb salvage outcomes were inconsistent. 3 In addition, only 1 RCT were included in meta-analysis with 35 cohort study. 16 The majority of studies are retrospective reviews with a high risk of bias with the Newcastle-Ottawa bias analysis due to heterogeneity of patient populations, the potential effect of confounding factors on study outcomes. The timeframe for the search for large systematic review included studies reported between 2000 and 2022. The improvement of the endovascular device, bypass graft technique and the new classification system of the severity of disease by new global vascular guideline trend to improving the result of endovascular treatment. Thus, further high-quality large randomized controlled trials are required to gain evidence-based treatment protocols for revascularization in people with diabetes and PAD in relation to both DR and IR.
From the medical records of the tertiary vascular center of Thammasat University Hospital, Pathum Thani, Thailand, between January 2019 and June 2022, 116 patients underwent revascularization surgery with indications of ischemic ulcers or gangrene. The results of the revascularization surgery were categorized into the DR group with 58 patients, the IR-tc group with 39 patients, and the IR-wc group with 19 patients with the 2-year median time to follow-up, the limb salvage rate after the best endovascular treatment for the DR group was 87.93%, the IR-tc group was 84.61%, and the IR-wc group was 47.36%, respectively. Seven and 6 patients of the DR and IR-tc groups underwent amputation, respectively. The most common causes for these amputations were severe wound extension and infection grade of the WifI classification system (Figure 5). 36
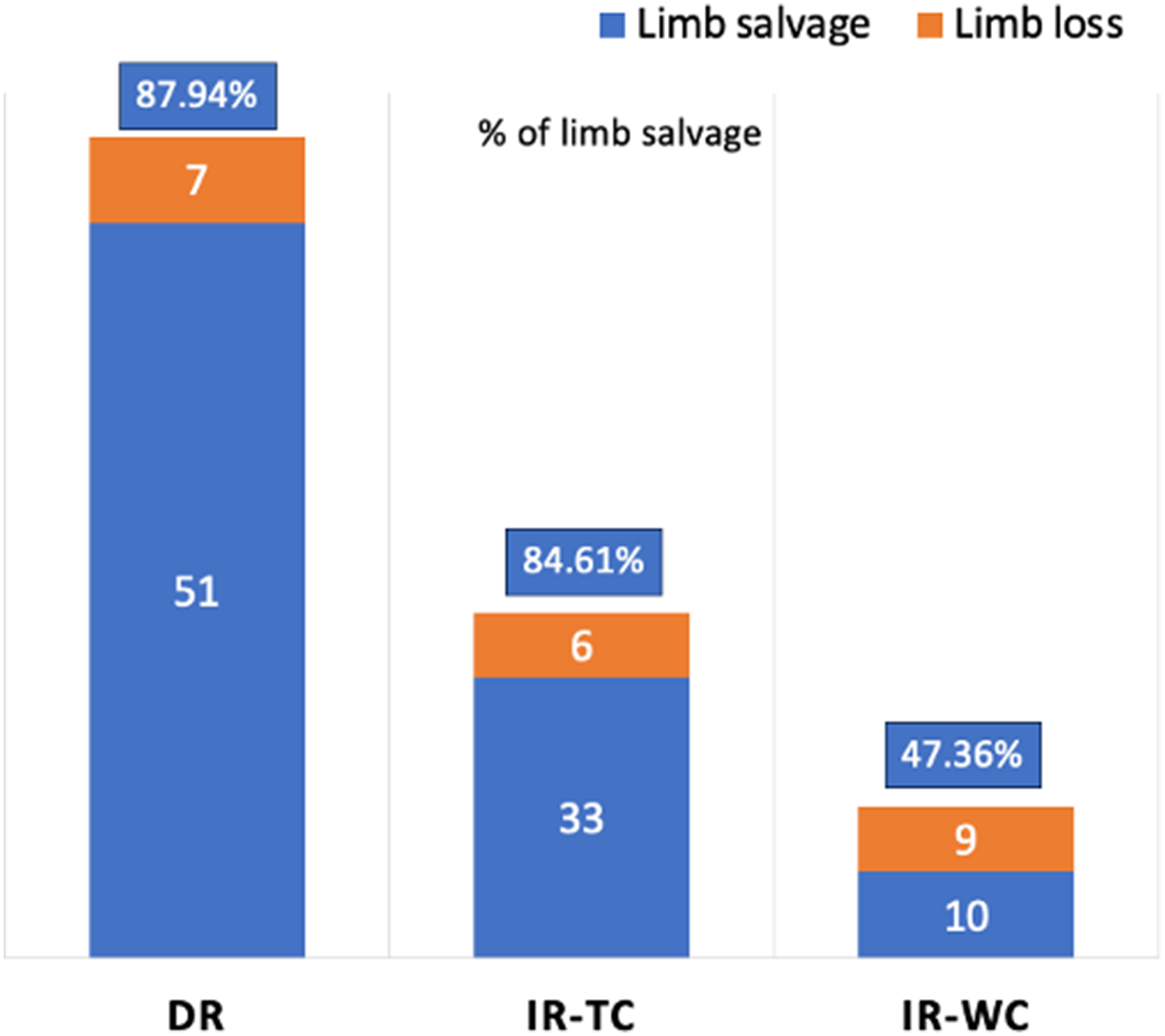
The bar chart demonstrates the 2-year limb salvage rate of CLTI patients after endovascular treatment at Thammasat University Hospital (TUH) during 2019 to 2022, categorized by types of revascularization under angiosome concept including direct revascularization (DR), indirect revascularization through collaterals (IR-tc) (3) indirect revascularization without collaterals (IR-wc).3,27 CLTI, chronic limb-threatening ischemia.
Conclusion
Indirect revascularization without a collateral vessel to ischemic tissue and single below-the-knee vessel revascularization with inframalleolar disease are poor outcomes and high risk of amputation. Therefore, the aim of revascularization, especially endovascular treatment to enhance wound healing based on the TIMERS and angiosome concepts, it is imperative to consider and select the best TAP under angiosome concept with at least 2 of 3 below the knee arteries to restore in-line pulsatile blood flow to the ischemic tissue in CLTI patients. The patients who reported in publications and authors’ data included the Asian population. So, this approach's outcome is associated with wound, vascular territories variation, and collateral network, which aims to increase the limb salvage rate and improve the quality of life of Asian country CLTI patients.
Footnotes
Acknowledgments
This work was supported by Research Group in Surgery, Faculty of Medicine, Thammasat University, Thailand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.