
Abstract
Background and objective:
The purpose of our study was to evaluate whether routine follow-up radiographs after distal radius fracture (DRF) treated with volar locking plate (VLP) influenced clinical decision-making and treatment in working-aged patients (18–65 years). We evaluated the possible correlation between clinical status and problems with follow-up radiographs and analyzed the overall reoperation rate.
Methods:
The study population of this retrospective cohort study consisted of working-aged (18–65 years) patients with DRF who were treated with VLP between January 2010 and December 2020. Baseline data, follow-up visits, and radiographs were collected. Radiographs were classified as either routinely assigned or according to clinical findings. Patients were divided into four groups based on abnormal radiographic findings or major symptoms leading to reoperation. Patients also received patient-rated wrist evaluation (PRWE) questionnaire, which were analyzed.
Results:
A total of 861 patients were included in this study. Routine follow-up radiographs were available for 844 (98%) patients. In 7.0% of patients, 6-week radiographs led to a change of standard treatment protocol, most commonly additional imaging and/or clinical follow-up. Nine (1.1%) patients underwent an urgent reoperation, and 15 (1.8%) patients underwent reoperation later in the follow-up period. All these patients were exceptionally painful/symptomatic. In addition, 33 (3.9%) patients who underwent additional imaging and follow-up after abnormal radiograph, but did not undergo reoperation, were asymptomatic or suffered only mild pain. A total of 89 (10.5%) patients had reoperation for any reason during the follow-up period.
Conclusions:
Routine follow-up radiographs after the treatment of DRF with VLP in the working-aged population rarely leads to changes in treatment strategy or reoperation in asymptomatic patients suggesting that it would be safe and cost-effective to reduce routine follow-up radiographs and focus instead on those patients with moderate-to-severe symptoms.
Context and Relevance
Routine radiographs in the follow-up of patients with distal radius fractures (DRFs) treated with a volar locking plate are common and are used to verify implant positioning and bone healing, and to rule out any possible developing complications. However, the value of these radiographs is unclear. Although evidence is limited, it suggests there is no difference in outcomes based on the frequency of the radiographic evaluation of patients treated for DRFs. As routine radiographs seldom affect clinical decision-making, they have low value in screening for possible complications. According to this study, it seems to be safe and cost-effective to reduce the number of routine follow-up radiographs and to focus instead on those patients with moderate-to-severe symptoms.
Introduction
Distal radius fractures (DRFs) are among the most common fractures in adults. Incidence varies from 100 to 300 per 100,000 person-years.1–3 A Swedish population-based study reported the incidence of DRFs to have increased due to an increasing proportion of working-aged (17–64 years) adults. 2 Still, overall, fracture incidence has stabilized in recent decades.1–3 Several studies have reported a steep increase in the number of DRFs treated with surgery. In the Nordic countries, for example, 15% to 26% of DRFs are treated operatively.3–5 The most used operative method is volar locking plate (VLP), representing 80% to 82% of all used methods.1,3
The overall complication rate after surgery with VLP ranges from 3% to 36%. The most common complications are nerve-, tendon-, and implant-related problems. Furthermore, the most frequent reoperations after DRF treated with VLP are plate removal and release of the median nerve. The total number of plate removals varies from 2% to 14%, as postoperative pain, malaligned screws, and irritation or rupture of the tendon have all been reported as the main causes of removal.6–14
Routine radiographs in the follow-up of patients with DRF treated with a VLP are common and are used to verify implant positioning and bone healing, and to rule out any possible developing complications. However, the value of these radiographs is unclear, and their use has been mainly dictated by old dogma. Although evidence is limited, it suggests there is no difference in outcomes based on the frequency of the radiographic evaluation of patients treated for DRFs. 15 According to previous studies, routinely taken radiographs rarely influence clinical decision-making. Indeed, only 2% to 6% of the postoperative radiographs acquired during DRF follow-up in these studies had abnormal radiographs that impacted clinical decision-making and resulted in changes in treatment strategy.16–18 Unfortunately, previous studies have had limitations such as small sample sizes, short follow-up times, the exclusion of intra-articular and multi-fragmented fractures from the analyses, or they have been unable to combine data with clinical findings.16–20 As clinical symptoms can often be used to evaluate patients who require additional examination, it is essential to also consider the possible burden of routine imaging on the health care system and the individual, and to minimize unnecessary radiation exposure.19,21
The main aim of the study was to evaluate whether the standard follow-up of radiographs taken 6 weeks after the VLP of DRF in working-aged patients (18–65 years) influenced clinical decision-making and patient treatment. Furthermore, we also aimed to evaluate whether there is any correlation between clinical status and problems with follow-up radiographs and to analyze the overall reoperation rate.
The article was made according to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Patients and methods
Study design
This was a retrospective cohort study of working-aged (18–65 years) patients with DRF treated with VLP at Tampere University Hospital, Finland, between January 2010 and December 2020. The sample was collected using the International Classification of Diseases, 10th edition (ICD-10) diagnostic codes S52.5 and S52.6 for DRFs and the Nomesco procedural codes NDJ62 and NCJ62 for distal radius surgery with a plate. In cases where another wrist was operated in a different year, the patient exists in the data twice. The exclusion criteria were an operative method other than VLP, such as external fixation or dorsal plating.
Data collection and variables
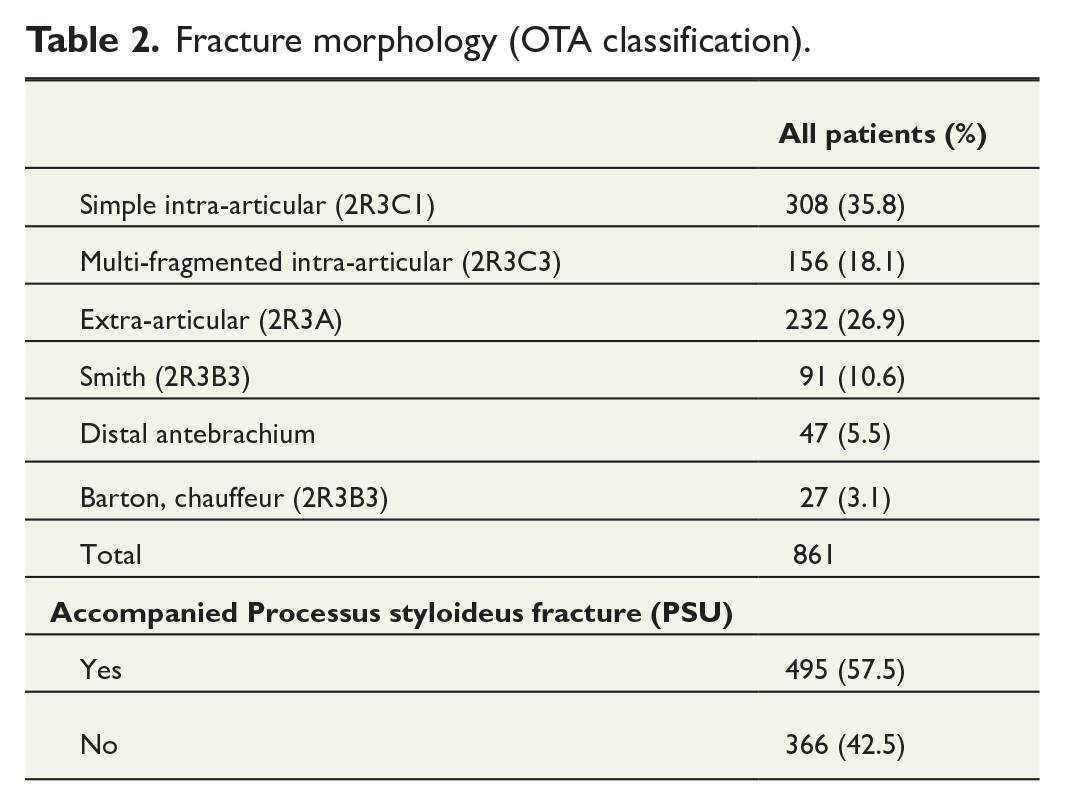
Baseline and follow-up data were collected from electronic medical records. The data included sex, age, fracture morphology, co-morbidities, smoking, and the date of injury and surgery. Co-morbidities that were considered meaningful were diabetes, rheumatic diseases, mental illness, memory disorders, and substance abuse. Fracture morphology, based on the Orthopaedic Trauma Association (OTA) classification, 22 was divided into 2R3A (extra-articular), 2R3C1 (simple intra-articular), 2R3C3 (intra-articular/multi-fragmented), 2R3B3 (Smith), 2R3B3 (Barton), and distal antebrachium fractures. Distal antebrachium fractures were included if the ulna did not require any osteosynthesis or fixation. All radiographs were analyzed, and any complications or subsequent follow-ups were recorded.
The patients in this study were treated in the emergency room at Tampere University Hospital after the trauma. Primary radiographs were taken, and closed reduction in the injured wrist performed. Criteria for nonoperative treatment were dorsal tilt of less than 10°, radial shortening, or an intra-articular step of more than 2 mm after closed reduction. 23 If the criteria for nonoperative treatment were not met, a decision to operate was made. If reduction was lost during follow-up, operative treatment was scheduled at the outpatient clinic. Operative treatment with VLP was performed within 0–21 days after the injury. Operating surgeons were orthopedic and hand surgery residents, who operated alone or under the supervision of a senior surgeon, and consultant orthopedic/hand surgeons.
During the study period, it was common practice to have routine follow-up, which also included radiographs, at the 6-week time point. In the first years of the study period, it was also common to have another routine follow-up at the 3-month time point. After follow-up, radiographs were assigned if patient symptoms required further evaluation, or the surgeon considered it otherwise necessary. At 6-week routine follow-up, patient symptoms were recorded from the database and classified as asymptomatic, mild, or severe symptoms. Patients who reported symptoms such as slightly reduced range of motion (ROM) and pain at heavier activities but not in activities of daily living (ADL) were classified as mild pain. Moderate-to-severe pain causing problems at ADL but showing some recovery since the operation, patients were considered as severely symptomatic if he or she was not able to perform ADL and disrupted sleep.
Radiographs were classified into two categories: (1) routinely assigned and (2) according to clinical findings. If control radiographs resulted in any change of treatment in terms of further operations, prolonged immobilization, additional clinical follow-up, or additional diagnostic imaging, it was recorded. Abnormal radiograph findings were recorded if mentioned in the electronic medical records at 6-week follow-up. Abnormal radiographs were further divided into malpositioning or failure with implant or screws, malalignment of the fracture, and distal radioulnar joint (DRUJ) incongruence. All follow-up visits were recorded, and any complications (nerve and tendon related problems, superficial and deep infections, DRUJ problems, co-injuries) were noted. The total number of implant removals was also recorded.
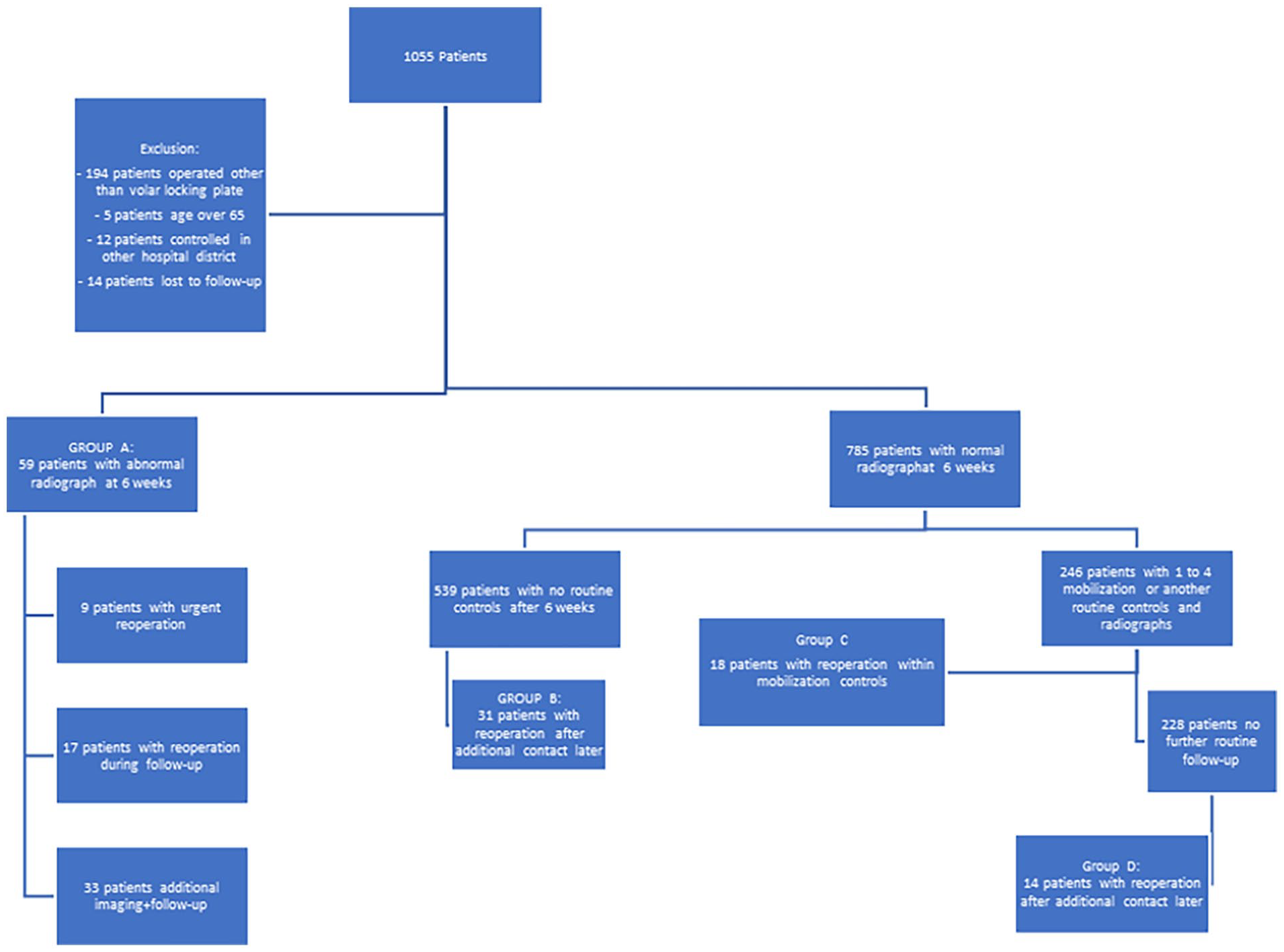
Patients with abnormal radiographic findings or major symptoms leading to reoperation were divided into four groups: (A) patients with abnormal radiographs at 6-week routine control, (B) patients who recovered as planned and had only one routine follow-up at the 6-week time point but subsequently contacted the hospital during the study period and underwent reoperation for any reason, (C) patients with normal 6-week routine radiograph assigned to another routine follow-up control or who had symptoms resulting in additional examinations or follow-ups leading to reoperation during these appointments, and (D) patients whose planned controls had ceased but developed major symptoms and were referred to the outpatient clinic where they later underwent reoperation during the follow-up period.
We approached all study patients by letter in August 2023 and asked them to complete the patient-rated wrist evaluation (PRWE). Patients received a personal QR code that led to electronic questionnaire in RedCap (Research Electronic Data Capture, https://www.project-redcap.org/).
Statistical analysis
Continuous variables were compared using a Welch t-test. For categorical variables, p values were calculated using the chi-square test in Statistical Package for the Social Sciences (SPSS) and were considered significant if the two-tailed value was less than 0.05.
Ethics
As this was a registry study, no ethical approval was required.
Results
During the study period, 866 patients were operated with VLP. Of these, 861 patients were included in the final analysis. Six-week radiographs were available for 844 (97.5%) patients. Baseline characteristics are presented in Tables 1 and 2. Mean follow-up time in our study was 6.7 years (range: 0.8–12.4 years, standard deviation (SD): 5.1).
Baseline characteristics of the patients.
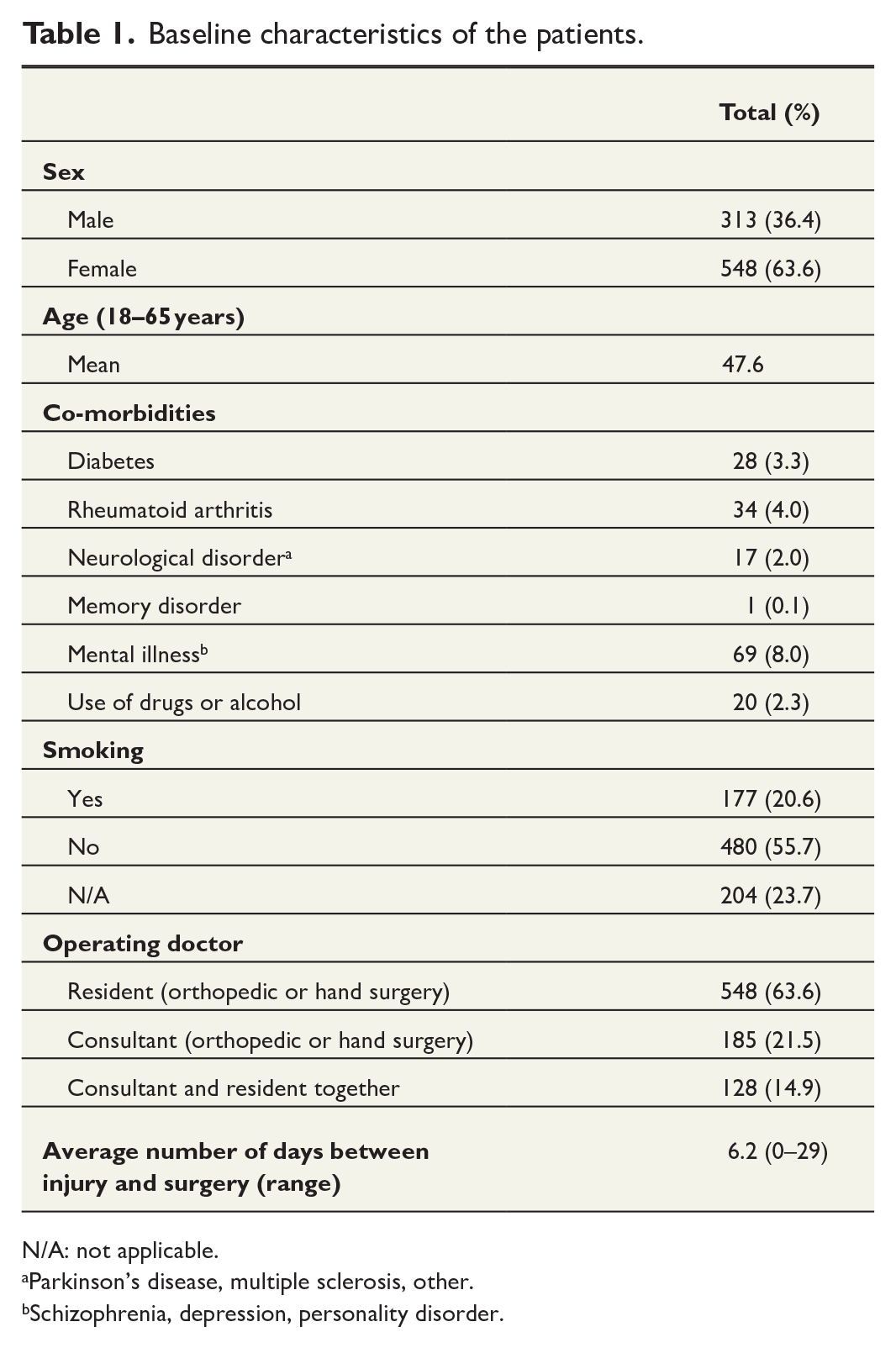
N/A: not applicable.
Parkinson’s disease, multiple sclerosis, other.
Schizophrenia, depression, personality disorder.
Fracture morphology (OTA classification).
In total, 59 (7.0%) of 844 patients had an abnormal radiograph at 6-week routine follow-up (Group A in Fig. 1). Of these 59 patients with abnormal radiograph, 9 (15.2%) patients were reoperated urgently within 1–2 weeks after the follow-up visit (Additional Supplemental Material 1), as the symptoms prevented patients from mobilizing the operated wrist and delayed return to work. A further 17 (28.8%) of 59 patients who were first assigned to follow-up were reoperated later during the follow-up period (3 months to 5 years after index operation). Implant removal was the most common cause (22%) of reoperation among all patients who had an abnormal radiograph (Table 3). Of the 26 patients who underwent reoperation, 11 did not undergo computed tomography (CT) imaging, and the decision to operate was based solely on plain radiographs. The remaining 15 patients had an additional CT scan before the reoperation. Examples of abnormal radiographs are presented in additional supplemental material 2.
Results.
Outcomes of patients with abnormal radiograph at 6-week follow-up after distal radius plating.
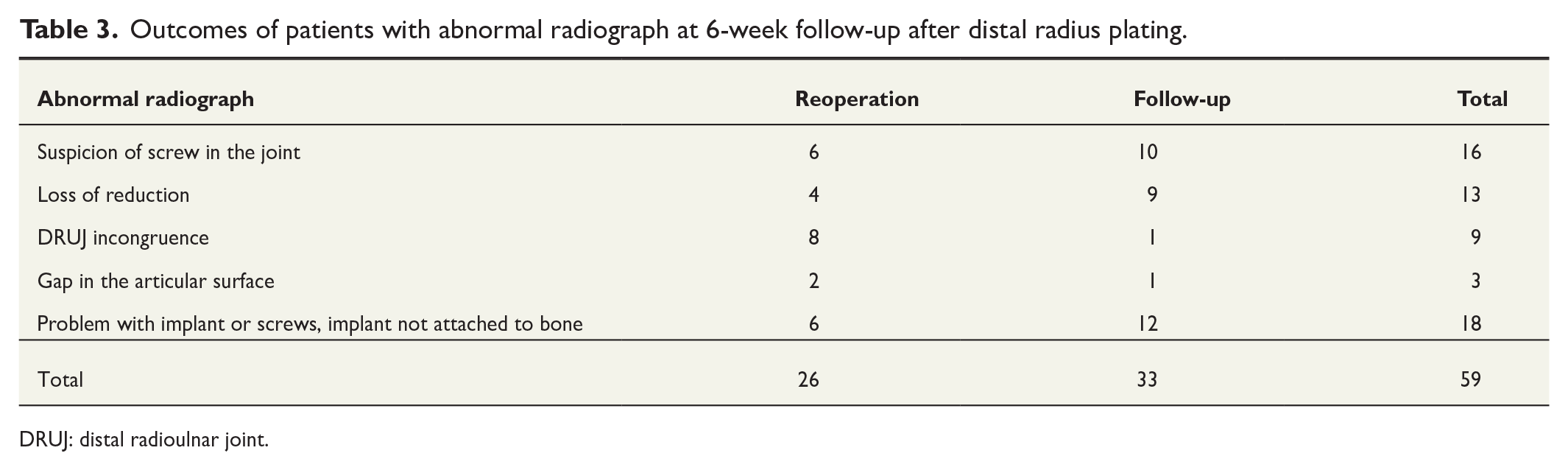
DRUJ: distal radioulnar joint.
All 26 patients who underwent reoperation after abnormal radiograph reported major pain or stiffness in the operated wrist either at the 6-week time point or developed symptoms later during the follow-up period. Of the 33 patients with abnormal radiographs who did not undergo reoperation, 23 were completely asymptomatic and considered fully healed at the 6-week time point. A further 10 patients had mild pain, which was considered a normal postoperative status.
The 6-week radiographs of 785 (93%) patients were considered normal. Of these, 539 (64.7%) had only one routine follow-up visit. However, 31 of 539 patients (Group B in Fig. 1) who had no additional routine follow-up visit scheduled after the first 6-week control were later referred to the outpatient clinic for complaints and symptoms related to the wrist. These patients underwent reoperation, and the most common reason for reoperation was plate removal (19 out of 31 patients). (Table 4).
Reoperations in patients with normal radiograph in 6-week follow-up.
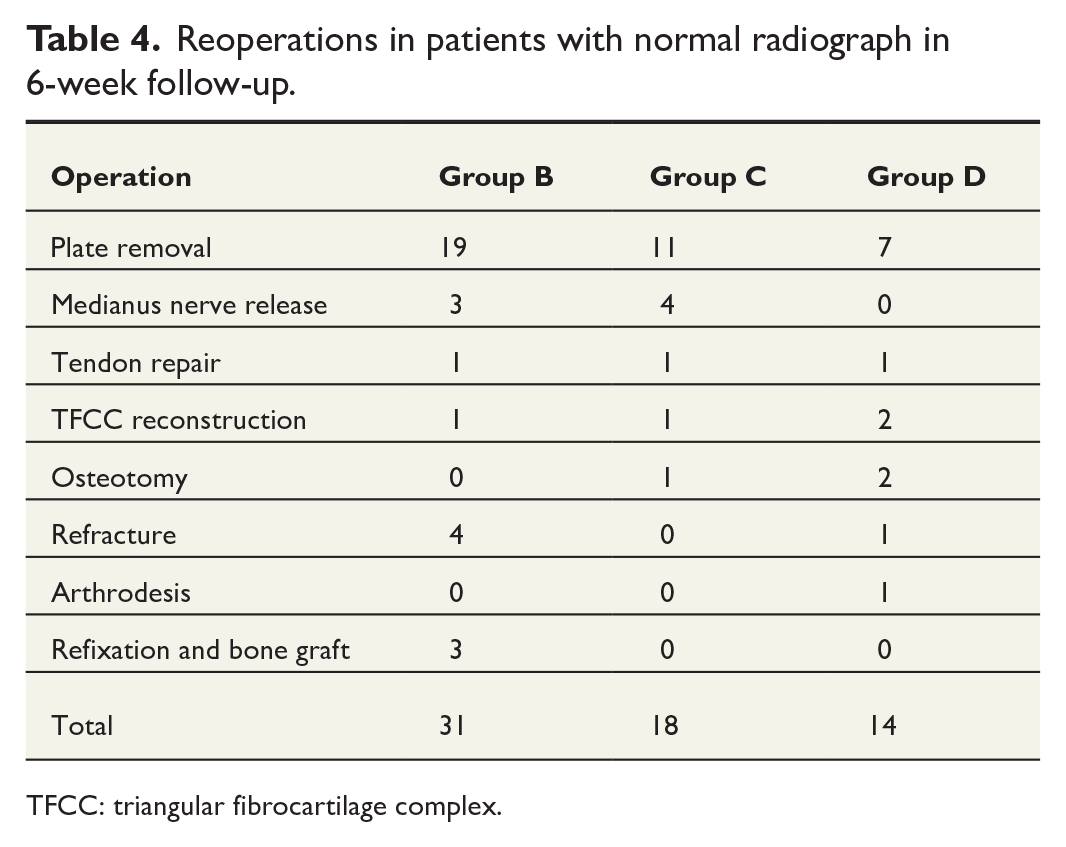
TFCC: triangular fibrocartilage complex.
A total of 246 patients with normal 6-week radiograph had an additional, routinely or due to symptoms, scheduled follow-up visit after 6 weeks. These visits were usually scheduled 12 weeks after index operation. Of the 246 patients, 18 had major symptoms in the operated wrist (Group C in Fig. 1), and follow-up visits led to further examination (nerve conduction studies, CT, or magnetic resonance imaging (MRI)) and eventually reoperation (Table 4). Furthermore, 228 (92.7%) out of 246 patients who were without complaints had normal radiographs, had uneventful visits to the outpatient clinic at 12 weeks, and had no further routine follow-up visits.
However, 14 of 228 patients who had no further routine follow-up visits and became asymptomatic during routine or additional follow-up visits later developed major complaints and symptoms in the operated wrist and were referred to the outpatient clinic and underwent reoperation (Group D in Fig. 1).
The most common reason for reoperation in all groups was tendon irritation. Total amount of plate removal was 50 cases (5.9%) (Table 4). During the follow-up period, the total number of reoperations in our study population was 89 (10.5%) out of 844.
Table 5 shows a comparison of baseline variables between patients with normal and abnormal 6-week radiographs. Interestingly, mental illness was overrepresented in the abnormal group. C-type fractures were also overrepresented in abnormal radiograph Group A, but this had borderline significance. No dissimilarity among other variables could be found (Table 5).
Comparison of patients with abnormal radiograph to those with normal radiograph.
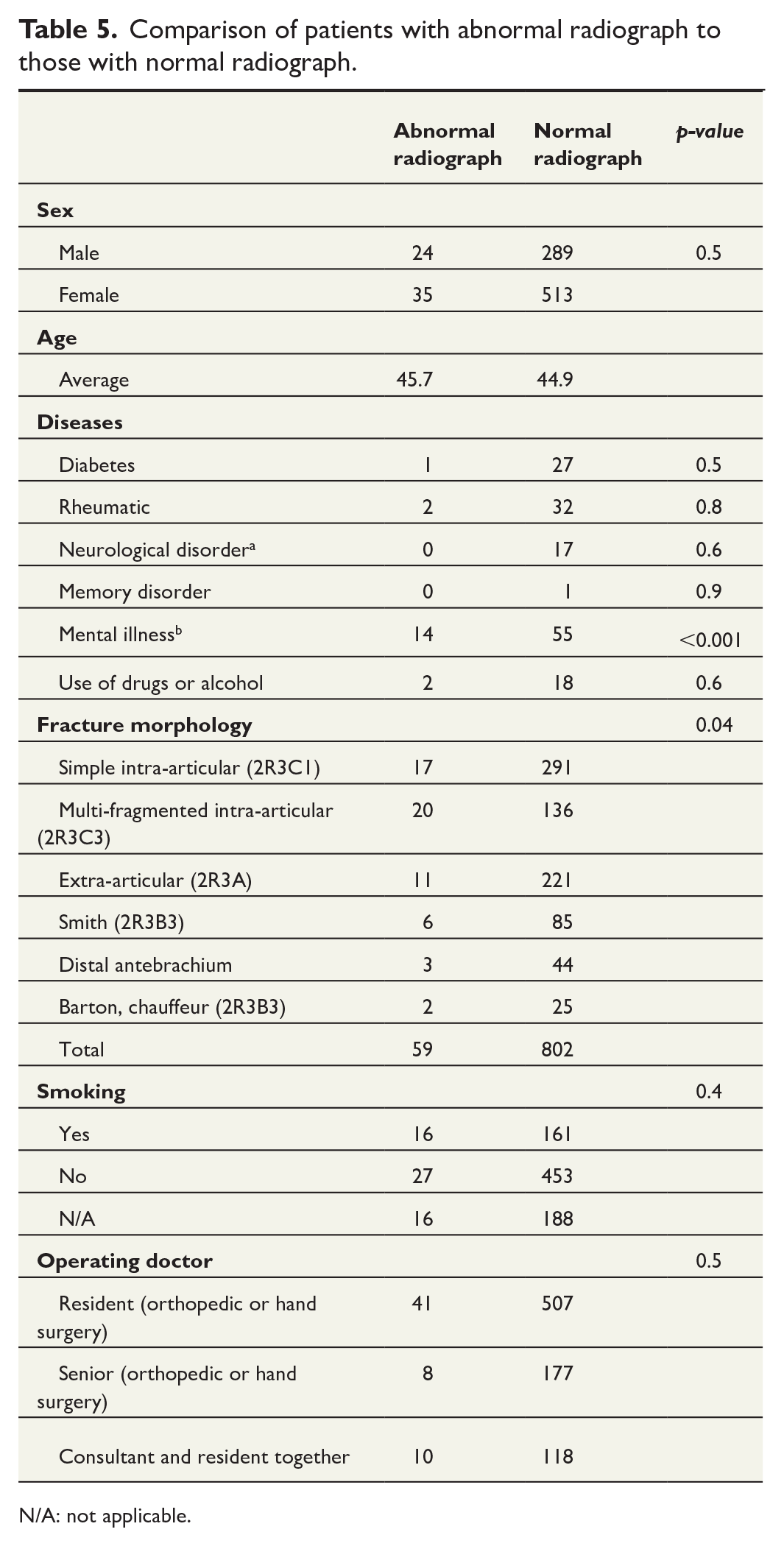
N/A: not applicable.
Patients with abnormal radiograph at 6 weeks not requiring a reoperation had an average PRWE of 10 (SD: 9.0) points. This was comparable with patients with uneventful postoperative recovery (mean difference: −1.9, 95% confidence interval [CI]: −11.4 to 7.5). Patients with abnormal radiograph at 6 weeks followed by a reoperation had poorer PRWE (mean: 32, SD: 29.7) but compared with patients with uneventful recovery the difference did not reach statistical significance (mean difference: 20.1, 95% CI: −74 to 47.6).
Discussion
Routine radiographs in the follow-up of DRFs treated with a VLP are a common practice, but the value of such routine imaging is unclear. Indeed, the majority of patients in our study cohort had a normal radiograph and did not have symptoms leading to reoperation. Furthermore, at the 6-week time point, no asymptomatic or mildly symptomatic patients required reoperation in our cohort, even when there was an abnormality in the radiograph. In contrast, all patients who underwent reoperation in abnormal radiograph group were moderately or severely symptomatic. However, 7.3% of patients who had a normal radiograph and were asymptomatic or suffered mild symptoms at initial follow-up visit only developed clinical symptoms warranting reoperation later during the follow-up period. Moreover, only a few of these patients had an abnormal radiograph later.
DRFs are one of the most common fractures in working-aged adults, and they are treated operatively if the criteria for nonoperative treatment are not met. During the past two decades, the amount of operative treatment has increased greatly. For example, in Finnish data, the incidence of plate fixation in women aged 50–70 years quadrupled during the years 2006 and 2016, while the use of all locking plates has also increased. 1 Due to this high volume, health care systems are using a marked amount of resources both in the treatment and the follow-up of this injury. The majority of the costs come from the time spent in the operating theater, which includes the cost of the implant, and from follow-up visits. The costs of the follow-up visits can be optimized, since routine appointments include radiographs and a visit to the outpatient clinic in many hospitals. The findings of this study suggest that routine radiographs seldom affect clinical decision-making and treatment strategy, and hence, they have a low value alone in screening for possible complications. It seems, therefore, that routine radiographs in operatively treated DRF are not justified due to the extra costs and unnecessary radiation exposure of the patients.
The findings of this study also indicate that complications warranting a reoperation are almost uniformly symptomatic. Therefore, the clinical status should be used to evaluate those patients who require additional studies or follow-up visits. PRWE results in our study are in line with the main findings. Perhaps, contact via a remote clinic would be enough for all patients, and only those patients with moderate-to-severe symptoms (i.e. not able or having major restrictions in ADL) would attend a further face-to-face appointment with radiographs taken. Education to ensure that intra-operative radiographs are standardized is also important so that the radiographs can be re-evaluated by experts in standardized radiograph meetings. This would result in patients who are at higher risk for problems later on being followed more thoroughly.
Our results are consistent with the findings of prior studies. Weil et al. demonstrated that changes in the early treatment strategy are rarely based on routine radiographs, as only 2.4% of operatively treated patients had a change in treatment strategy after routine radiograph. However, the proportion increased when radiographs were taken based on clinically observed symptom. Indeed, 9% of these patients underwent a change in treatment strategy. 16 Huffaker et al. evaluated OTA type A fractures treated with VLP and found that 94% of routine follow-up radiographs did not influence clinical decision-making. All patients who required further interventions had symptoms affecting the operated wrist. 18 In addition, Sjølander et al. 20 reported a 3.1% change in standard treatment at routine 2-week follow-up radiographs. In our study, 1.5% of patients had loss of reduction seen in 6-week follow-up radiographs, but only four of these patients (0.005%) underwent reoperation. The remaining patients were asymptomatic.
Stone et al. 21 evaluated the value of very early routine radiographs and reported that in only 1% of cases with 2-week follow-up radiographs did the treatment strategy change. van Gerven et al. compared 1- and 2-week routine radiographs to multiple routine radiographs in a randomized controlled trial that included patients with DRF treated both nonoperatively and operatively. They found there was a significant difference in costs without compromising functional outcomes. Of these patients, only 10% were treated operatively. There was, however, no difference in complication rate and patient-reported outcomes between two control radiographs versus multiple control radiographs. Moreover, the overall complication rate was similar in both groups (11.3% versus 11.4%). 19
The strengths of this study include a large cohort and a low number of cases lost to follow-up at the early time points, since 98% of the data for the 6-week follow-up time point were available. Previous studies have had minor limitations such as small sample size, excluding intra-articular and multi-fragmented fractures, or not relating data to clinical findings. Many studies have also investigated multiple routine controls with patients treated nonoperatively. Furthermore, in most of the previous studies, the radiograph time point has been 1 or 2 weeks, with routinely taken radiographs later. In contrast, in our study, we included all fracture morphologies and evaluated the relation of the clinical status to the radiographs.
The limitation of this study is that it is retrospective. First, we sent PRWE to all study patients, but we received only 29% answer coverage. In addition, due to retrospective nature of the study, we did not have a pre-study definition for abnormal radiological finding, which at present is based on the treating surgeon’s evaluation and, as such, the results may be prone to selection bias. Furthermore, we were unable to acquire patient data if the patient had moved to another hospital district or had later outpatient visits or reoperation in private hospitals after the first routine follow-up visit at our hospital. This might have affected our analysis of long-term follow-up data and could be the reason our total implant removal amount (5.8%) was lower than in the national data. 17 Finally, as the assessment was based on electronic health record notes, we may have overestimated the positive findings. For example, a resident may have ordered a CT with a lower threshold than the experienced surgeon.
We conclude that routine follow-up radiographs after the treatment of DRF with VLP in an asymptomatic working-age population rarely lead to changes in treatment strategy or reoperation suggesting that it would be safe and cost-effective to reduce the number of routine follow-up radiographs and to focus on those patients with moderate-to-severe symptoms.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241234740 – Supplemental material for Routine follow-up imaging is not necessary in uneventful early recovery after distal radius fractures treated with volar locking plate in working-aged patients: A retrospective single-center cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969241234740 for Routine follow-up imaging is not necessary in uneventful early recovery after distal radius fractures treated with volar locking plate in working-aged patients: A retrospective single-center cohort study by Laura Kärnä, Antti P. Launonen, Toni Luokkala and Aleksi Reito in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969241234740 – Supplemental material for Routine follow-up imaging is not necessary in uneventful early recovery after distal radius fractures treated with volar locking plate in working-aged patients: A retrospective single-center cohort study
Supplemental material, sj-docx-2-sjs-10.1177_14574969241234740 for Routine follow-up imaging is not necessary in uneventful early recovery after distal radius fractures treated with volar locking plate in working-aged patients: A retrospective single-center cohort study by Laura Kärnä, Antti P. Launonen, Toni Luokkala and Aleksi Reito in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.K. and A.R. have received government funding related directly to this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has received Finnish state funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.