
Abstract
Background and aims:
Appendectomy has historically been the standard treatment of acute appendicitis, but lately, conservative treatment of uncomplicated acute appendicitis with antibiotics has successfully been used in selected patients. Complicated acute appendicitis is often treated conservatively initially, but may benefit from interval appendectomy due to the higher risk of appendiceal malignancy and recurrence. Recommendations for follow-up after conservatively treated appendicitis vary. Furthermore, the risk of underlying malignancy and the necessity of routine interval appendectomy are unclear. This study aims to evaluate follow-up status, recurrence, and underlying appendiceal malignancy in conservatively treated uncomplicated and complicated acute appendicitis.
Methods:
This study included patients with conservatively treated acute appendicitis at Skåne University Hospital, Sweden during 2012–2019. Information on patient demographics at index admission and data on follow-up, recurrence, number of appendectomies after initial conservative treatment, and underlying malignancy were retrieved from medical charts.
Results:
The study cohort included 391 patients, 152 with uncomplicated and 239 with complicated acute appendicitis. Median time of study follow-up was 52 months. The recurrence risk was 23 (15.1%) after uncomplicated and 58 (24.3%) after complicated acute appendicitis (p = 0.030). During follow-up, 55 (23%) patients with complicated acute appendicitis underwent appendectomy. Appendiceal malignancies were found in 12 (5%) patients with previous complicated acute appendicitis versus no appendiceal malignancies after uncomplicated acute appendicitis (p = 0.002).
Conclusion:
The risk of appendiceal malignancy and recurrent appendicitis was significantly higher in patients with complicated acute appendicitis compared with uncomplicated acute appendicitis.
Context and Relevance
Standard treatment of uncomplicated acute appendicitis has been appendectomy, but conservative treatment is gaining popularity. For patients with complicated acute appendicitis, the treatment is often conservative initially. Previous studies have reported underlying malignancy in up to 20% after conservatively treated complicated acute appendicitis. There are no established guidelines for follow-up after conservative treatment, and the necessity of interval appendectomy is unclear. In this study, the risk of appendiceal malignancy and recurrent appendicitis was significantly higher in patients with complicated acute appendicitis compared with uncomplicated acute appendicitis.
Introduction
Appendectomy is the most frequently performed general surgical procedure worldwide and in Sweden, with approximately 12,500 appendectomies performed annually.1–3 In uncomplicated acute appendicitis, appendectomy has historically been the gold standard. However, conservative treatment with antibiotics, in this article also referred to as non-operative management (NOM), is considered an option for selected patients.4,5 For patients with complicated acute appendicitis, defined as perforation of the appendix with phlegmon or abscess, the initial treatment of choice is often NOM, including antibiotics with or without drainage.4 The rationale for a conservative approach regarding complicated acute appendicitis is the risk of extended surgical resection with consequent postoperative complications and, in some cases, uncertainty of the underlying diagnosis.4,6 Following conservative treatment in patients with complicated acute appendicitis, the need of interval appendectomy, elective appendectomy after initial successful NOM, is still a matter of discussion. Withholding interval appendectomy avoids unnecessary surgical procedures, resulting in decreased postoperative complications and cost savings. Without appendectomy, the exact diagnosis will be uncertain, which is of concern for patients with underlying malignancy, that is, specifically patients ⩾ 40 years of age. 7 An appendectomy also eliminates recurrence, with a reported risk of 39% for uncomplicated and 12%–24% for complicated acute appendicitis. 4 Laparoscopic appendectomy performed by surgeons with advanced laparoscopic expertise, instead of NOM, has recently been suggested for patients with complicated acute appendicitis, an approach eliminating recurrence, need of standardized follow-up, and misdiagnosed appendiceal malignancy. 8
Although appendicitis is an old and familiar diagnosis, the optimal choice between appendectomy and NOM for both uncomplicated and complicated acute appendicitis is unclear.
Appendiceal malignancies are incidentally found during appendectomy in 0.9%–1.4% of all surgical specimens.3,9 As conservative treatment of acute appendicitis gains popularity, early detection of appendiceal malignancies becomes increasingly important. 10 A recent randomized controlled trial (RCT) revealed 20% of underlying appendiceal malignancies in patients with complicated acute appendicitis, initially treated conservatively, who underwent interval appendectomy. The incidence for patients > 40 years of age was even higher (29%). 11 Other non-randomized studies have shown a risk of underlying appendiceal malignancies of 10%–29%. 12 Updated guidelines by World Society of Emergency Surgery (WSES) recommend follow-up with computed tomography (CT) and colonoscopy for patients ⩾40 years of age after conservatively treated acute appendicitis, including both uncomplicated and complicated cases. However, evidence regarding follow-up after NOM of acute appendicitis in adults is scarce. Whether interval appendectomy is indicated after NOM for patients ⩾ 40 years of age is unclear since the risk of appendiceal malignancy is uncertain. 4
To evaluate the need of a standardized follow-up protocol and interval appendectomy after NOM for patients with acute appendicitis, this study intends to assess the risk of underlying appendiceal malignancy and recurrence after conservative treatment.
Aim
This study aims to examine the follow-up status, recurrences, number of appendectomies after initial NOM, and underlying appendiceal malignancies in patients with conservatively treated uncomplicated and complicated acute appendicitis. We expected patients with complicated acute appendicitis to have a higher risk of recurrence and underlying appendiceal malignancy than patients with uncomplicated acute appendicitis.
Methods
Study population
Patients ⩾ 18 years of age admitted at Skåne University Hospital (SUS), Sweden with acute appendicitis (International Classification of Disease (ICD)-10 diagnosis codes: K35.2, K35.3, K35.8, K36.9, or K37.9) and without operation code for appendectomy (JEA00, JEA01, JEA10, JFB20, JFB21, JFB30, and JFB31) from 1 January 2012 to 31 December 2019 were identified via the in-patient registry. SUS serves a population of approximately 750,000 inhabitants. All patients conservatively treated for acute appendicitis at the index admission with verified diagnosis by ultrasound (US), CT, or exploratory abdominal surgery without appendectomy were included in the study. Exclusion criteria were admission outside the study period, clinical diagnosis (no radiologic or surgical verification of diagnosis), other diagnosis, and appendectomy at the index admission.
Definition of acute appendicitis
In this study, uncomplicated acute appendicitis was defined as inflammation confined to the appendix and complicated acute appendicitis as perforation of the appendix with phlegmon or abscess, which corresponds to grade IV in the American Association for the Surgery of Trauma (AAST) scale for acute appendicitis.
Data collection and follow-up of conservatively treated acute appendicitis
Patient data from index admission and follow-up were retrospectively collected by medical chart review according to a predetermined case report form. Information on demographics, diagnostics, treatment, planned follow-up after index admission (clinical, laboratory, endoscopy, radiology, or no planned follow-up), readmissions, and appendectomies with consequent histopathological analyses during follow-up were gathered for comparison of patients with uncomplicated acute appendicitis versus complicated acute appendicitis. All patients diagnosed with appendiceal malignancy during follow-up were analyzed separately regarding baseline data, type of surgery, time to malignant diagnosis from index admission, and alive or not at follow-up.
In this study, patients were followed-up from date of index admission until date of death, date of histopathological verification from appendectomy after initial NOM, or if neither occurred, until the end of study follow-up in the interval during July 2020–October 2022. All patients were followed for a minimum of 33 months after diagnosis of acute appendicitis.
Estimations of surgically treated acute appendicitis
At SUS, the number of routine acute appendectomies performed at index admission during 2015–2019 was estimated using Orbit, theater planning program. These estimations were based on data from patients ⩾ 18 years of age. The number of diagnosed appendiceal malignancies, following both elective and acute appendectomy, in the county of Skåne during 2015–2019 was extracted from the statistical database at Swedish National Board of Health and Welfare.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics software version 26 for Windows (IBM Corp, Armonk, NY, USA). Continuous numerical variables were presented as median and first to third quartile (Q1–Q3), or mean and standard deviation (SD). Differences between two groups were calculated by independent t-test or Mann–Whitney U test. Dichotomous and categorical variables were presented as frequency and percentage. Differences were determined by Pearson’s chi-square test, or if results were less than 5, by Fisher’s exact test. A p-value of less than 0.05 was considered significant. Power calculations were not applied because of the retrospective study design.
Ethical considerations
This study was approved by the Regional Ethics Committee at Lund University (Dnr 2019-03583).
Results
In all, 615 patients admitted at SUS with acute appendicitis diagnosis and without operation code were identified in the in-patient registry. After reviewing the medical charts and exclusions, 391 patients fulfilled the inclusion criteria and constituted the final study cohort, whereof 152 with uncomplicated and 239 with complicated acute appendicitis (Fig. 1). Patients with complicated acute appendicitis had significantly higher levels of C-reactive protein (CRP) and longer duration of symptoms before admission in comparison to patients with uncomplicated acute appendicitis (p < 0.001). No significant differences were found regarding age, gender, body mass index (BMI), medical history, and previous abdominal surgery (Table 1). A total of 55.5% of the patients were followed-up with colonoscopy and radiology after conservatively treated acute appendicitis. Radiologic modalities used for follow-up were CT, US, or magnetic resonance imaging (MRI). Among the patients with complicated acute appendicitis, 209 (87.4%) had a radiologically verified abscess. Mean follow-up time, including both patients with uncomplicated and complicated acute appendicitis, was 52 (28) months. All patients, unless appendectomy was performed during follow-up, were followed for a minimum of 33 months, and 71.4% were followed for over 5 years after diagnosis of acute appendicitis. The risk of recurrence in patients with uncomplicated acute appendicitis was 15.1% versus 24.3% in complicated acute appendicitis (p = 0.030; Table 2). Overall, 29 (12.1%) patients with complicated acute appendicitis were conservatively treated during their first recurrence (data not shown).
Patient characteristics in conservatively treated uncomplicated and complicated acute appendicitis.
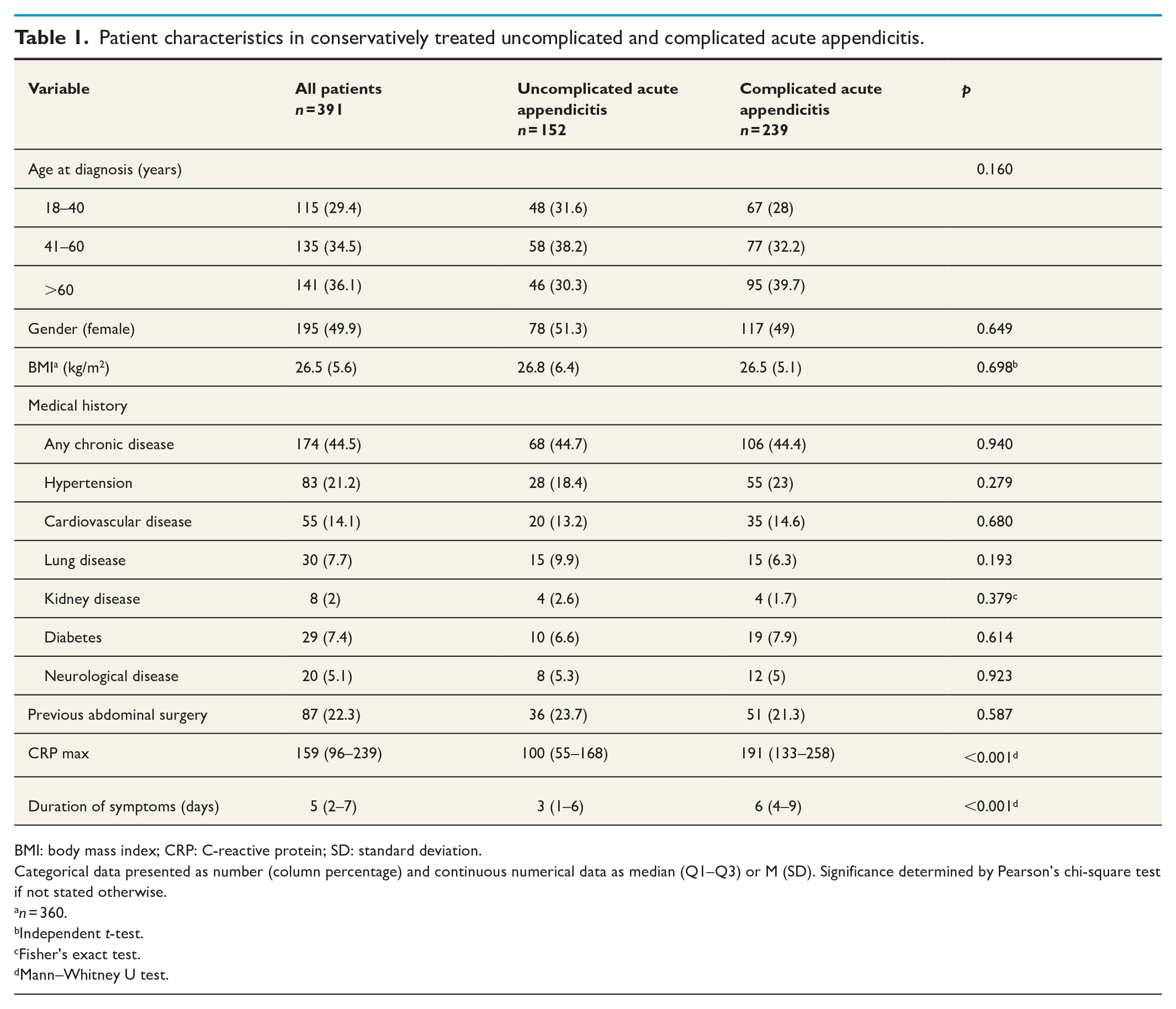
BMI: body mass index; CRP: C-reactive protein; SD: standard deviation.
Categorical data presented as number (column percentage) and continuous numerical data as median (Q1–Q3) or M (SD). Significance determined by Pearson’s chi-square test if not stated otherwise.
n = 360.
Independent t-test.
Fisher’s exact test.
Mann–Whitney U test.
Treatment at index admission and follow-up of conservatively treated uncomplicated and complicated acute appendicitis.
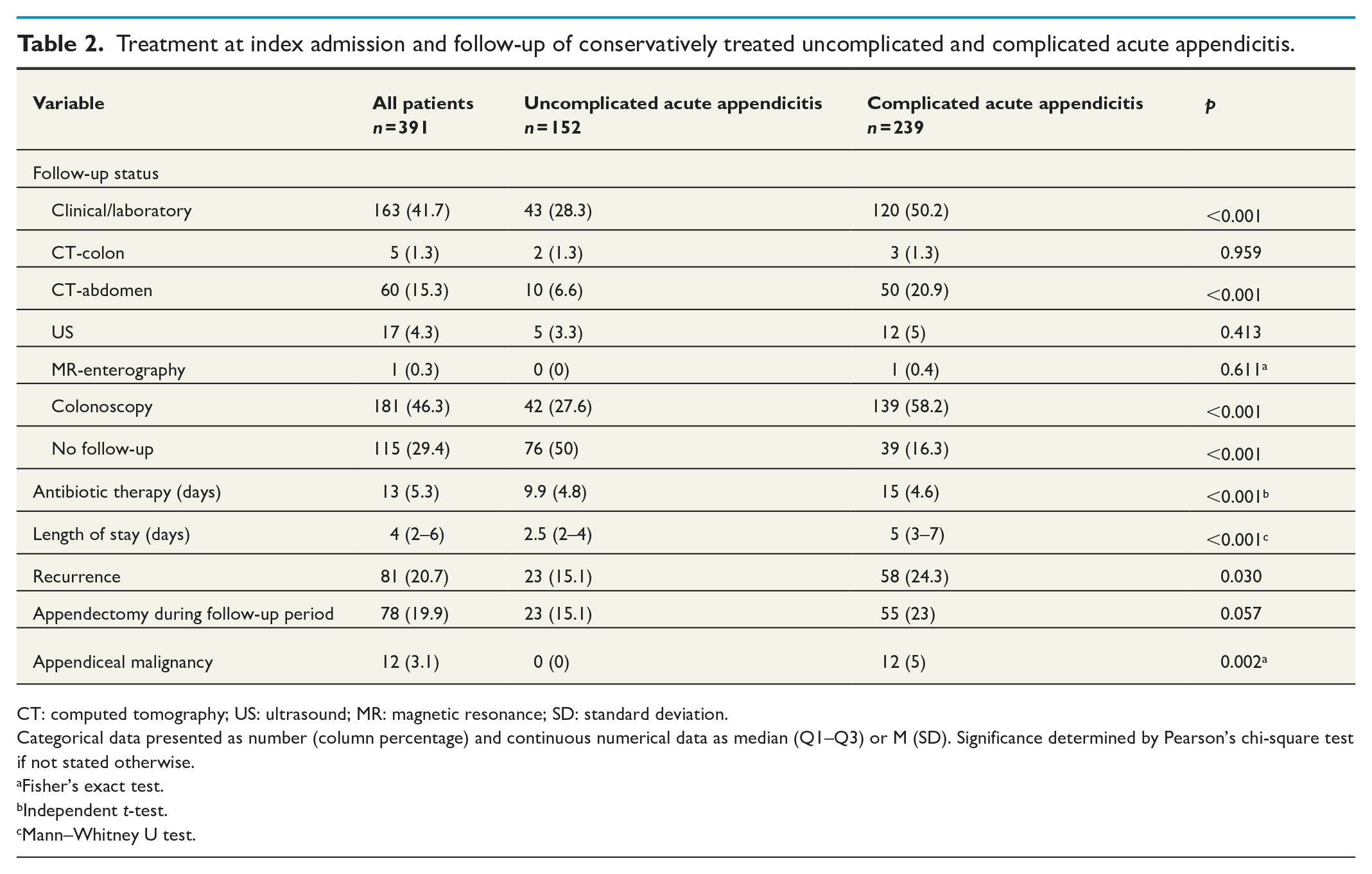
CT: computed tomography; US: ultrasound; MR: magnetic resonance; SD: standard deviation.
Categorical data presented as number (column percentage) and continuous numerical data as median (Q1–Q3) or M (SD). Significance determined by Pearson’s chi-square test if not stated otherwise.
Fisher’s exact test.
Independent t-test.
Mann–Whitney U test.
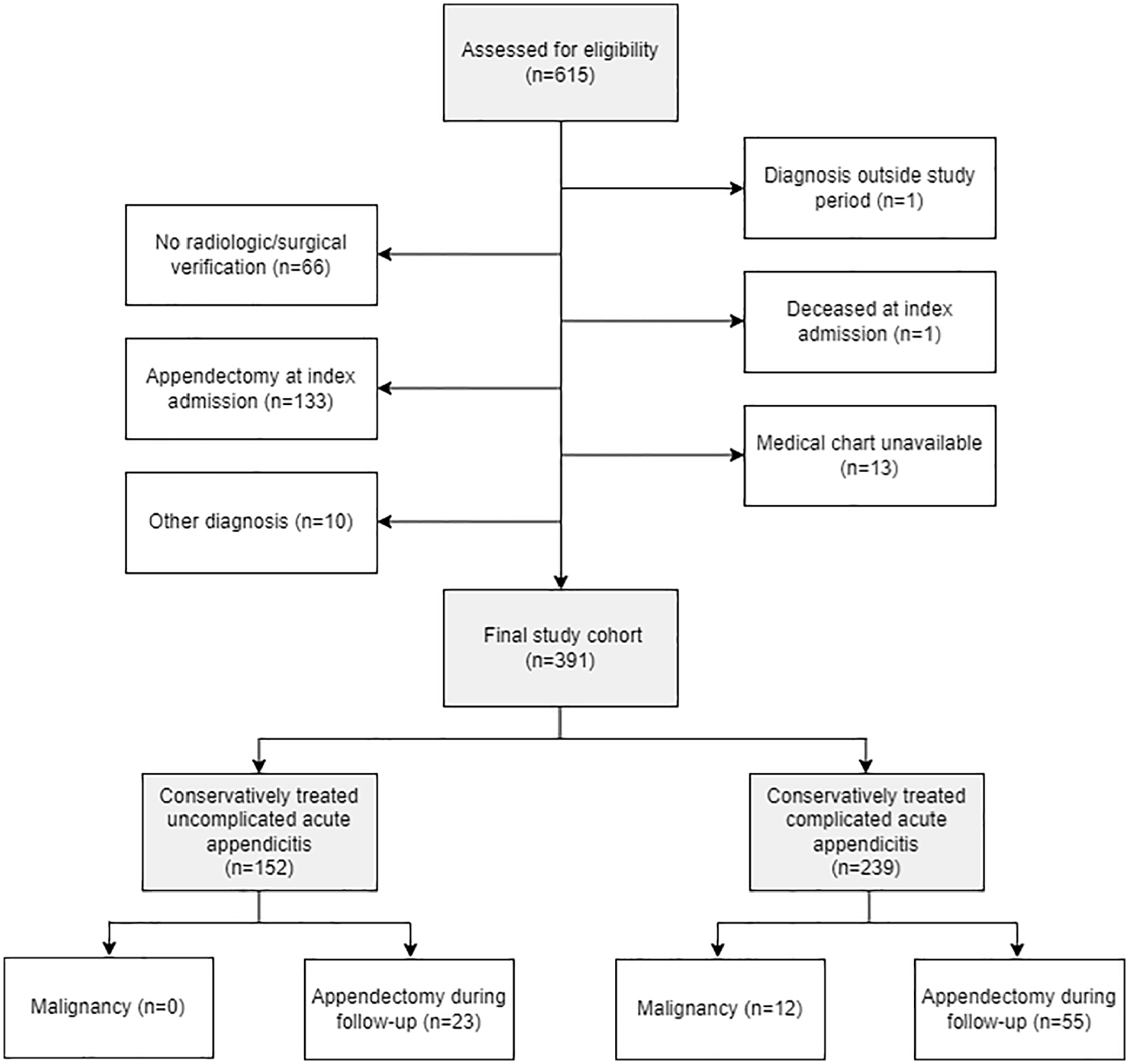
Study flowchart demonstrating defined cohort and outcomes regarding appendiceal malignancy and appendectomy during follow-up.
Appendectomy after initial NOM, either acute or elective, during the follow-up period was registered in 23 (15.1%) patients with uncomplicated and 55 (23%) patients with complicated acute appendicitis (p = 0.057). The indication for appendectomy was not failure of NOM at index admission, but rather recurrence of acute appendicitis or suspected underlying malignancy during follow-up. In total, 12 (5%) patients with complicated and no patients with uncomplicated acute appendicitis were diagnosed with histopathologically verified appendiceal malignancy (p = 0.002; Table 2). The appendiceal malignancies consisted of 11 adenocarcinomas, of which 7 were mucinous, and 1 neuroendocrine tumor. One patient with adenocarcinoma was diagnosed with pseudomyxoma (Supplement 1).
Overall, 9 (75%) out of 12 patients with underlying appendiceal malignancy had recurrent appendicitis during follow-up (Table 3). The appendectomies after index admission in patients with underlying appendiceal malignancy were performed as open right hemicolectomy in six (50%) patients, open ileocecal resection in one (8%) patient, and laparoscopic appendectomy in four (33%) patients. Two surgical procedures were converted from laparoscopic procedures. One patient had histopathologically verified appendiceal malignancy based on colonoscopy during follow-up, but did not undergo appendectomy due to high comorbidity and age > 80 years. Four (33%) patients with appendiceal malignancy were deceased during follow-up due to disseminated or recurrent malignancy (Table 3). The tumor staging of all patients with adenocarcinoma was T3–T4 at the time of diagnosis (Supplement 1).
Patient characteristics and treatment at index admission, initially chosen follow-up modality after index admission and treatment during follow-up of conservatively treated appendicitis in patients with underlying appendiceal malignancy.
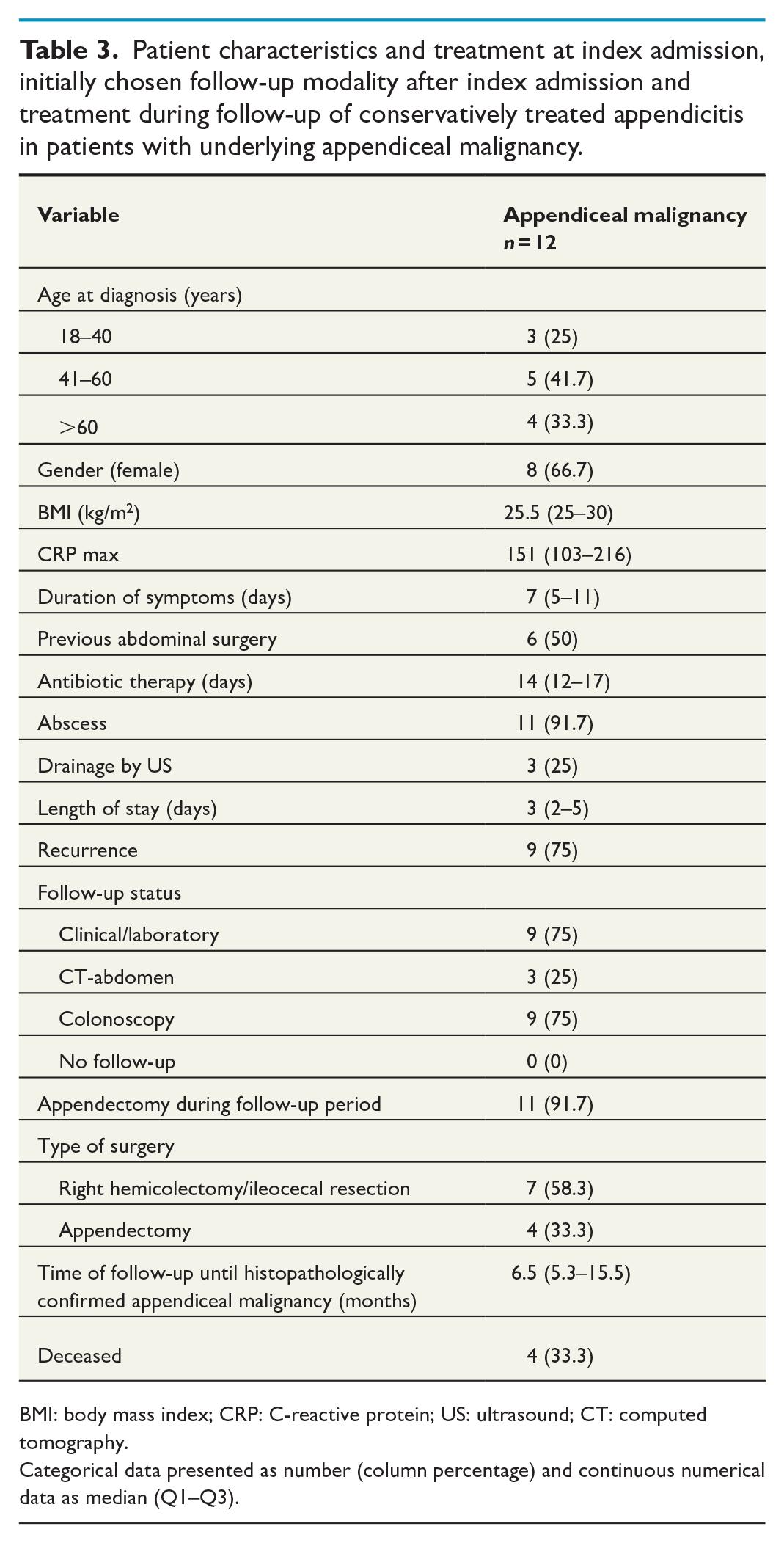
BMI: body mass index; CRP: C-reactive protein; US: ultrasound; CT: computed tomography.
Categorical data presented as number (column percentage) and continuous numerical data as median (Q1–Q3).
Clinical and treatment characteristics of patients with underlying appendiceal malignancy from index admission are shown in Table 3. Eight (66.7%) patients were females and the median age was 56 years. Most patients (75%) with appendiceal malignancy were > 40 years of age. However, 6 (50%) of the 12 patients had previously undergone abdominal surgery. Only one patient had radiologically suspected malignancy at the index episode.
During follow-up, 1 patient with uncomplicated and additionally 12 patients with complicated acute appendicitis, all > 50 years of age, were diagnosed with a colon malignancy; namely, eight cecal cancer, one unspecified non-intestinal origin in the caecum, one transverse colon cancer, one sigmoid colon cancer, one at an unspecified location in the colon, and one patient with ileal carcinomatosis from previous rectal cancer.
At SUS, covering approximately 54% of the population of the county of Skåne, a total of 2744 routine acute appendectomies were performed during 2015–2019. Including both elective and acute appendectomies, 93 histopathologically verified appendiceal malignancies were identified, and thus estimated to comprise approximately 1.8% of all appendectomies.
Discussion
This retrospective study examined the follow-up status, recurrences, number of appendectomies after initial NOM, and underlying appendiceal malignancies in patients with conservatively treated uncomplicated and complicated acute appendicitis in an era in which guidelines for treatment and follow-up of appendicitis have been inconsistent. In total, 23% of patients with complicated acute appendicitis underwent appendectomy during the follow-up period and almost 85% were subjected to follow-up. The recurrence risk for complicated acute appendicitis found in this study was in alignment with previous studies, while the recurrence risk for uncomplicated acute appendicitis and the number of appendiceal malignancies were lower than previously reported. All cases of appendiceal malignancies were found within the group of complicated acute appendicitis.
At our institution, patients presenting with typical medical history and clinical signs of acute appendicitis are subjected to diagnostic laparoscopy. A CT scan for diagnostic work-up is only used in patients with long duration of symptoms (>3–4 days) before admission, in elderly patients, or if the diagnosis is uncertain. If the CT scan indicates complicated acute appendicitis, patients are individually evaluated and may be treated conservatively. Patients in which initial CT scan indicates underlying malignancy are, if the clinical situation permits, treated conservatively, investigated further (CT-thorax, colonoscopy, and tumor markers) and referred to colorectal surgeons for definitive treatment after multidisciplinary conference. With this exception, our general approach to patients with uncomplicated acute appendicitis is laparoscopic appendectomy. The most likely reason for the high number of patients with uncomplicated acute appendicitis treated conservatively is spontaneous recovery while awaiting surgery.
Based on our findings, the need for follow-up of patients with conservatively treated uncomplicated acute appendicitis can be questioned since no underlying appendiceal malignancy was found in this group, but this matter needs to be studied further. In complicated acute appendicitis, several factors, such as age, and initial radiological and clinical findings, must be considered when determining the method of follow-up and need for interval appendectomy.
In this study, the overall incidence of appendiceal malignancies in patients with complicated acute appendicitis was less than previously reported by Mällinen et al. 11 (5% versus 20%). This RCT, however, suffered from a small study population, failure to recruit all potentially eligible patients, and premature termination due to alarming appendiceal malignancy rates, leaving the study underpowered to draw firm conclusions. Moreover, the study only included a subgroup of complicated acute appendicitis, specifically, patients presenting with an inflammatory mass. Comparing our results to previous retrospective studies, the incidence of appendiceal malignancies found in this study is consistent with some,13,14 while others have demonstrated higher risks of appendiceal malignancies.15,16 Authors solely investigating patients with acute appendicitis who underwent interval appendectomy, not considering the type of index appendicitis and heterogeneous definition of complicated acute appendicitis are potential explanations for ambiguous results.
The WSES guidelines suggest reservation of interval appendectomy for patients with recurrence after conservatively treated complicated acute appendicitis. 4 After individual evaluation, interval appendectomy may also be a treatment option for some patients ⩾ 40 years of age after the first episode of conservatively treated complicated acute appendicitis.
As expected, the risk of recurrence and appendiceal malignancies were higher in patients with complicated acute appendicitis, but the number of malignancies was still relatively low. Our results support the WSES recommendation to reserve interval appendectomy for patients with recurrence after conservatively treated complicated acute appendicitis.
We tried to estimate the risk of underlying appendiceal malignancy after routine acute appendectomy at SUS. This calculation revealed less likelihood than 1.8%, which further strengthens our statement. However, appendiceal malignancy was still three to five times more common after complicated acute appendicitis than what is reported in the general population after routine appendectomy (0.9%–1.4%). In addition to the incidental finding of colon cancer, these observations motivate follow-up after conservatively treated complicated acute appendicitis. Due to a higher incidence of cecal cancer among the elderly, 17 a combination of colonoscopy and CT scan after both uncomplicated and complicated acute appendicitis may be the modalities of choice for patients ⩾ 40 years of age, as suggested by the latest WSES guidelines. 4 Since a CT-colon offers a complete imaging of both the appendix and the intestinal wall, it might be an alternative modality for follow-up in this context. The mentioned suggestions of follow-up methods have recently been implemented at SUS as standardized guidelines for follow-up of patients with conservatively treated acute appendicitis (Supplement 2). This protocol will be further evaluated in a future prospective study.
The strengths of this study include data collection based on predefined variables and performed by one individual. The dataset was considered complete with only missing data regarding BMI (8%; Table 1). The study was carried out at a large surgical department, providing a large initial study cohort. Another strength is the objective verification of diagnosis.
The study was limited by its retrospective design and the lack of an equivalent control group. The main reason for the high number (36.4%) of excluded patients from the initially identified study cohort was a lack of registered operation codes for patients who underwent appendectomy at the index admission. These patients were incorrectly included in the initial study cohort since they were not conservatively treated. Therefore, the risk of selection bias is smaller than what may be perceived by the presented figures.
Conclusion
The risk of appendiceal malignancy and recurrent appendicitis was significantly higher in patients with complicated acute appendicitis compared with uncomplicated acute appendicitis.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231190293 – Supplemental material for Risk of appendiceal malignancy in conservatively treated acute appendicitis
Supplemental material, sj-docx-1-sjs-10.1177_14574969231190293 for Risk of appendiceal malignancy in conservatively treated acute appendicitis by Shaima Ramadan, Pamela Buchwald and Åsa Olsson in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969231190293 – Supplemental material for Risk of appendiceal malignancy in conservatively treated acute appendicitis
Supplemental material, sj-docx-2-sjs-10.1177_14574969231190293 for Risk of appendiceal malignancy in conservatively treated acute appendicitis by Shaima Ramadan, Pamela Buchwald and Åsa Olsson in Scandinavian Journal of Surgery
Supplemental Material
sj-png-3-sjs-10.1177_14574969231190293 – Supplemental material for Risk of appendiceal malignancy in conservatively treated acute appendicitis
Supplemental material, sj-png-3-sjs-10.1177_14574969231190293 for Risk of appendiceal malignancy in conservatively treated acute appendicitis by Shaima Ramadan, Pamela Buchwald and Åsa Olsson in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.