
Abstract
Background and Aims:
The clinical significance of early ostomy complications has been emphasized worldwide, and the current evidence concerning the impact of emergency or elective surgery on ostomy complications is limited. This study aimed to investigate the effect of elective and emergency colorectal surgery on early ostomy complications and the risk factors associated with specific complications.
Methods:
A mandatory colorectal recording system for consecutive ostomy patients between 2012 and 2020 was reviewed retrospectively. Patient socio-demographics, ostomy-related variables, and early period ostomy complications were retrieved from the patient records. The chi-square test, t-test, analysis of variance (ANOVA), and logistic regression were used to analyze the data.
Results:
The study cohort included 872 patients. At least one or more complications developed in 573 (65.7%) patients, 356 (63.6%) in the emergency group, and 217 (69.6%) in the elective group. When comparing emergency surgery to elective surgery, necrosis (7.4% versus 3.4%, p = 0.009), mucocutaneous separation (37.2% versus 27.1%, p = 0.002), and bleeding (6.1% versus 2.1%, p = 0.003) were more prevalent. Peristomal irritant contact dermatitis (PICD) (37.3% versus 26%, p < 0.001) was more common in elective surgery. Risk factors for PICD were comorbidity (p = 0.003), malignant disease (p = 0.047), and loop ostomy (p < 0.001) in elective surgery; female sex (p = 0.025), neo-adjuvant therapy (p = 0.024), and ileostomy (p = 0.006) in emergency surgery. The height of the ostomy (less than 10 mm) was a modifiable risk factor for mucocutaneous separation in both elective surgery (p < 0.001) and emergency surgery (p = 0.045).
Conclusion:
Early ostomy complications were more likely to occur after emergency colorectal surgery than in an elective setting. Patient- and ostomy-related risk factors for complications differed between elective and emergency surgeries.
Context and relevance
Ostomy complications are currently a debated issue in both the medical and nursing aspects. However, the literature on the effects of emergency or elective surgery on the development of early ostomy complications is limited, and the risk factors for specific complications are rarely discussed. This study investigated the effect of elective and emergency colorectal surgery on early ostomy complications and the risk factors associated with specific complications. The results presented here highlight the high rate of ostomy-related complications, which is higher in cases requiring emergency surgery. Ostomy type, comorbidity, malignancy, female sex, and preoperative neo-adjuvant therapy increased the likelihood of PICD. Ostomy height of less than 10 mm was a significant modifiable variable in the development of mucocutaneous separation in the early postoperative period.
Introduction
The creation of an ostomy is a common procedure in both elective and emergency colorectal surgeries. In a subset of patients, ostomy creation is associated with a high survival rate. However, it is also associated with a decline in quality of life and early and/or late ostomy-related complications.1,2 Particular attention has been given to early ostomy complications due to their high incidence and negative effects on patients’ results. Ostomy complications have developed in nearly 80% of ostomy patients in the early postoperative period. Patient and/or surgery-related risk factors, including age, female sex, body mass index (BMI) greater than 25, and emergency surgery, have been associated with complications. 3
Most complications are usually related to inappropriate placement or construction of the ostomy, surgical technique, or misuse of ostomy care products.4,5 If surgery is performed as an emergency, the patient may have limited or no time to get mentally or physically prepared for the presence and management of the ostomy. In contrast to emergency procedures, a potential stoma site is marked, and preoperative education may be given to patients in elective surgery. Selection of the appropriate stoma site, considering the patient’s physique and body structure, may be an effective factor in the prevention of many ostomy complications. This may positively affect patient outcomes in the short and long term.5,6 Nevertheless, despite the fact that marking stoma sites provides better results, an ostomy site may not be marked in both emergency and elective conditions. 6 In addition, it is possible to develop many complications depending on the technical complexity of emergency surgical conditions. 4 Due to time constraints, it is not possible to provide preoperative counseling and planning, especially outside of working hours. In an emergency situation, ostomy construction is generally considered the least important part of the operation and can be handed off to the youngest member of the surgical team. 7
Ostomy complications are currently debated in both medical and nursing aspects. However, there is still a gap between the published studies in terms of the effect of emergency and elective ostomy surgery on complication rates and the specifically mentioned risk factors for complications.4,8,9 Previous studies have discussed the risk factors, complications, and consequences of an ostomy in both emergency and elective clinical settings. Findings from some studies showed that emergency surgery was a risk factor in the development of ostomy complications,7,10–12 while others reported that the type of surgery was not a predictive factor.8,13 In addition, few ostomy complications were examined according to the type of surgery, 6 and the risk factors for specific complications are rarely discussed. This study aimed to (1) investigate the effect of elective and emergency colorectal surgery on early ostomy complications (within 30 days after ostomy creation) and (2) explore the risk factors for specific complications in emergency and elective colorectal surgery. We hypothesized that there was a higher rate of early ostomy-related complications in those undergoing emergency surgery and that socio-demographic and ostomy-related factors had an influence on the occurrence of complications during the early period.
Methods
Design
The study was a retrospective cohort study that enrolled paper-based, standardized patient records of ostomy patients who were recruited at the stoma therapy unit of a tertiary hospital in Western Turkey. The research was reported according to the strengthening the reporting of observational studies in epidemiology (STROBE) criteria. 14
All patient records needed to be followed up on within 30 days after ostomy creation to be included in the cohort for analysis. Patients aged more than 18 years who underwent an ostomy creation between 1 January 2012 and 31 December 2020 were eligible if their records were followed up in the outpatient clinic at least once during the first month after discharge or in inpatient care for a month. Patients with a lack of follow-up at the outpatient clinic within 30 days postoperatively and missing information were excluded from the study.
Sample size
The sample size of the study was specified using the power analysis software G-Power 3.1.9.7. A priori power analysis, based on the study of Braumann et al. 6 of total complications rates, was conducted on the software with a Type 1 error of 0.05 and a power of 80%, resulting in a sample size of 192 patient records or greater in total. Logistic regression for the identification of complication predictors requires a larger sample with a minimum of 10 to 20 cases per predictor.15,16 It was, therefore, planned to include all suitable patient records in the sample to determine the results of the regression analysis precisely and to determine the incidence more accurately.
Routine hospital procedures and follow-up
After surgery, a wound and stoma care nurse evaluated the ostomy and provided training to the patients during hospitalization. The wound and stoma care nurse typically schedules an ostomy control 7–10 days after discharge. If the initial control revealed a complication that necessitated treatment, more controls were conducted, and the patient was monitored until recovery. The assessment of patients was registered in a paper-based patient registry during hospitalization and after discharge with standardized forms. Paper-based, standardized patient records included socio-demographic and ostomy-related features, inpatient ostomy care, outpatient follow-up, and early complications notes.
Inclusion, variables, and data collection
Eligible patients were identified retrospectively from the paper-based patient registry, which includes patients with an ostomy in our hospital. Data were collected in two standardized forms that were prepared specifically for this study in line with the literature3,4,7,17,18 between August and November 2021 (Supplementary Table 1). The first form, Demographic and Ostomy-Related Features, included baseline demographic variables (age, sex, smoking, BMI, preoperative neo-adjuvant therapy, comorbidity) and ostomy-related features such as height, marking of the stoma site in the preoperative period, ostomy type, the reason for ostomy creation, and the etiology of disease. At the time of postoperative hospitalization, the height of the ostomy was measured; height was defined as the distance between the top of the ostomy lumen and the skin.
The second form for the Diagnosis of Complications consisted of items that assessed early ostomy complications and the patient’s follow-up status. The main outcome variables were the presence or absence of early ostomy complications, which were defined as stomal necrosis, mucocutaneous separation, peristomal irritant contact dermatitis (PICD), peristomal suture granuloma, stomal retraction, bleeding, parastomal abscesses, and parastomal fistula.
Our exposure variables were patients’ demographic and ostomy-related features. A total of 13 predictor variables (Tables 3 and 4) and 9 complications were recorded.
Outcomes and definitions of complications
The primary outcome measure was the rate of complications within 30 days after ostomy creation. Valid and reliable definitions from Beitz and Colwell (2007) were used to identify complications as follows: necrosis (death of stomal tissue caused by compromised or inadequate stomal blood supply), PICD (skin irritation caused by contact with feces, or chemical preparations), mucocutaneous separation (the separation of stomal tissue from the peristomal skin around it), peristomal suture granuloma (localized extravagant tissue in which the retained or reactive suture material takes place at the skin or stoma base in sites), stomal retraction (the absence of pattern stomal protrusion at or below skin level), parastomal fistula (pathological passage between the stoma and/or the intestine and surrounding tissue), and parastomal abscess (purulent particles surrounded by inflammation caused by an infectious source). Intraluminal bleeding was defined as enough to fill the pouching system.
Ethical considerations
The approval of the Ethics Committee for Non-Interventional Investigations (Decision No. 2021/32-20) and hospital consent were obtained. The ethics committee waived the patient’s consent. The Helsinki Declaration was complied within the conduct of the research.
Data analysis
The data were analyzed using the SPSS 29.0 program. The socio-demographic and ostomy-related characteristics of patients were determined using percentages and descriptive statistics or median and interquartile range (IQR). The chi-square test, t-test, and analysis of variance (ANOVA) were conducted for univariate analysis. Binary logistic regression was conducted to evaluate the odds ratio (OR) and 95% confidence interval (CI) of predictive variables for the development of ostomy complications. Statistically significant variables from the univariate analysis and clinically significant variables according to the literature3,8,13,17,19 were included in the logistic regression. The p values less than 0.05 were regarded as statistically significant.
Validity, reliability, and rigor
The researchers double-checked all the data to ensure that there were no errors in this study. To assure data accuracy, Beitz and Colwell’s study definitions were applied to evaluate complications. Two researchers independently retracted the data at the same time, in accordance with the definition of complications. Missing data were excluded from the actual analysis. Before performing logistic regression, the assumptions of observations in terms of dependent and independent variables being linearly related to logic were checked and met.
Results
Patients with missing data (n = 84), who have never been followed up (n = 471), and who did not come for follow-up within the first month (n = 152) were excluded from further analyses. A total of 1579 potential patients were identified; of these, 872 (55.2%) were included (Figure 1). Of those, 477 (54.7%) were male, and 521 (59.7%) were younger than 65 years. Colorectal cancer (499; 57.2%) was the predominant diagnosis. The median number of follow-up visits for patients was 4.00 (IQR = 6.00). Table 1 shows baseline variables according to surgery type.
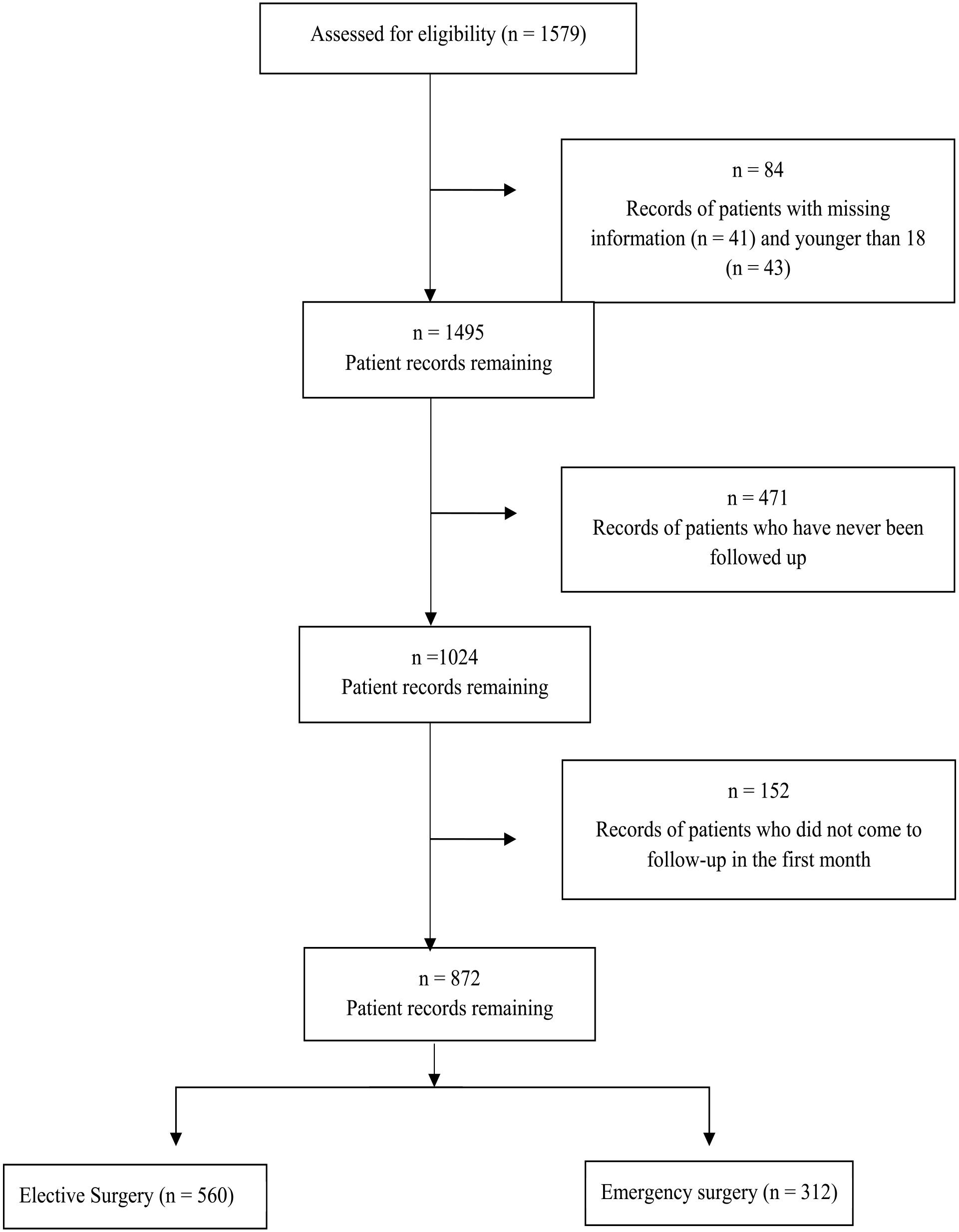
Flow Diagram.
Descriptive characteristic of ostomy patients according to type of surgery (n = 872).
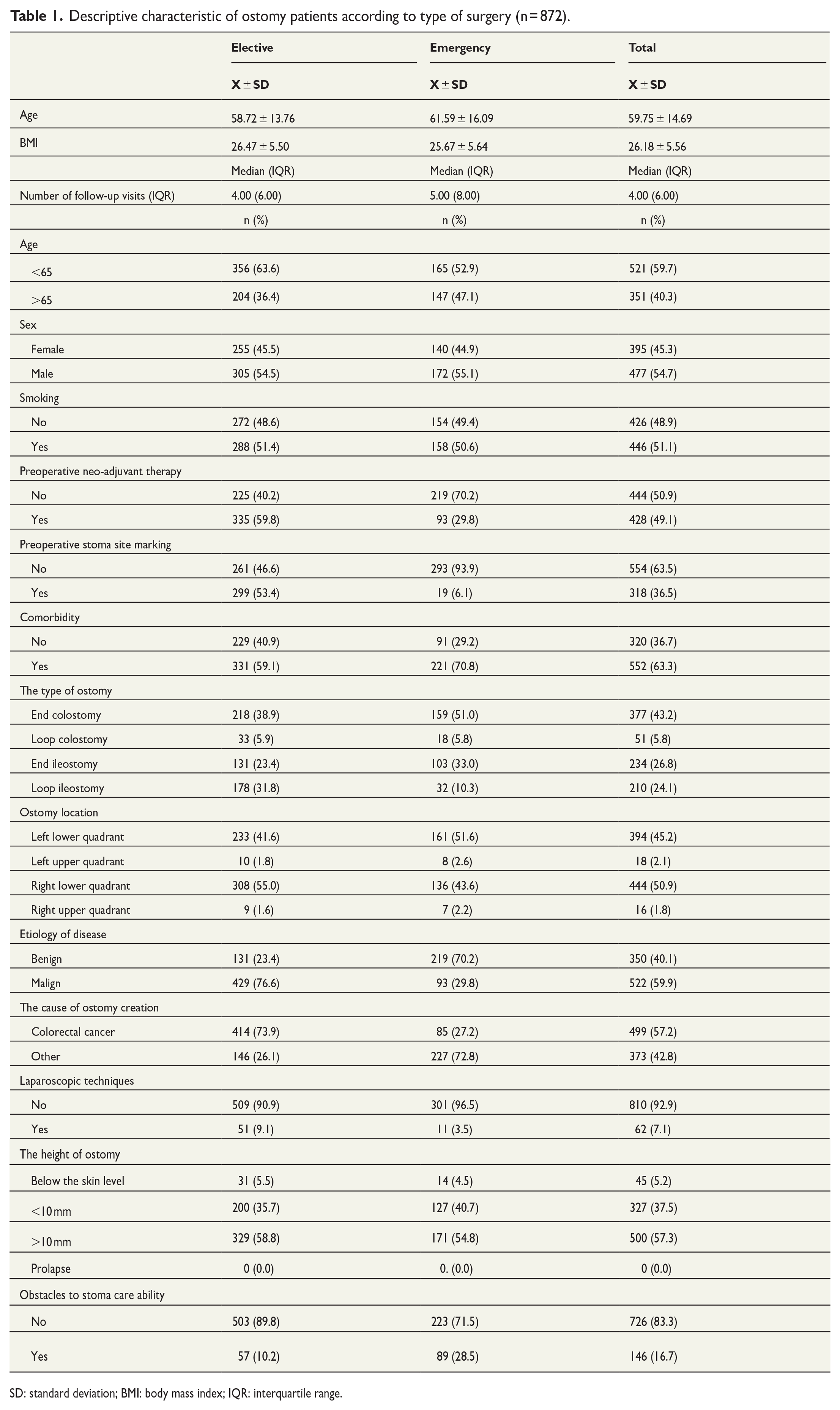
SD: standard deviation; BMI: body mass index; IQR: interquartile range.
At least one or more complications developed in 573 (65.7%) patients, 356 (63.6%) in the elective group, and 217 (69.6%) in the emergency group. PICD (290; 33.3%) was the most common complication, mostly developing in the second or third week postoperatively. The other prevalent complication was mucocutaneous separation (268; 30.7%), which developed in the second postoperative week in 142 (53%) cases. Other less frequent complications were retraction (67; 7.7%), granuloma (49; 5.6%), necrosis (42; 4.8%), bleeding (31; 3.6%), fistula (10; 1.1%), and abscess (9; 1%), respectively (Table 2).
Ostomy complications in the early period (n = 872).
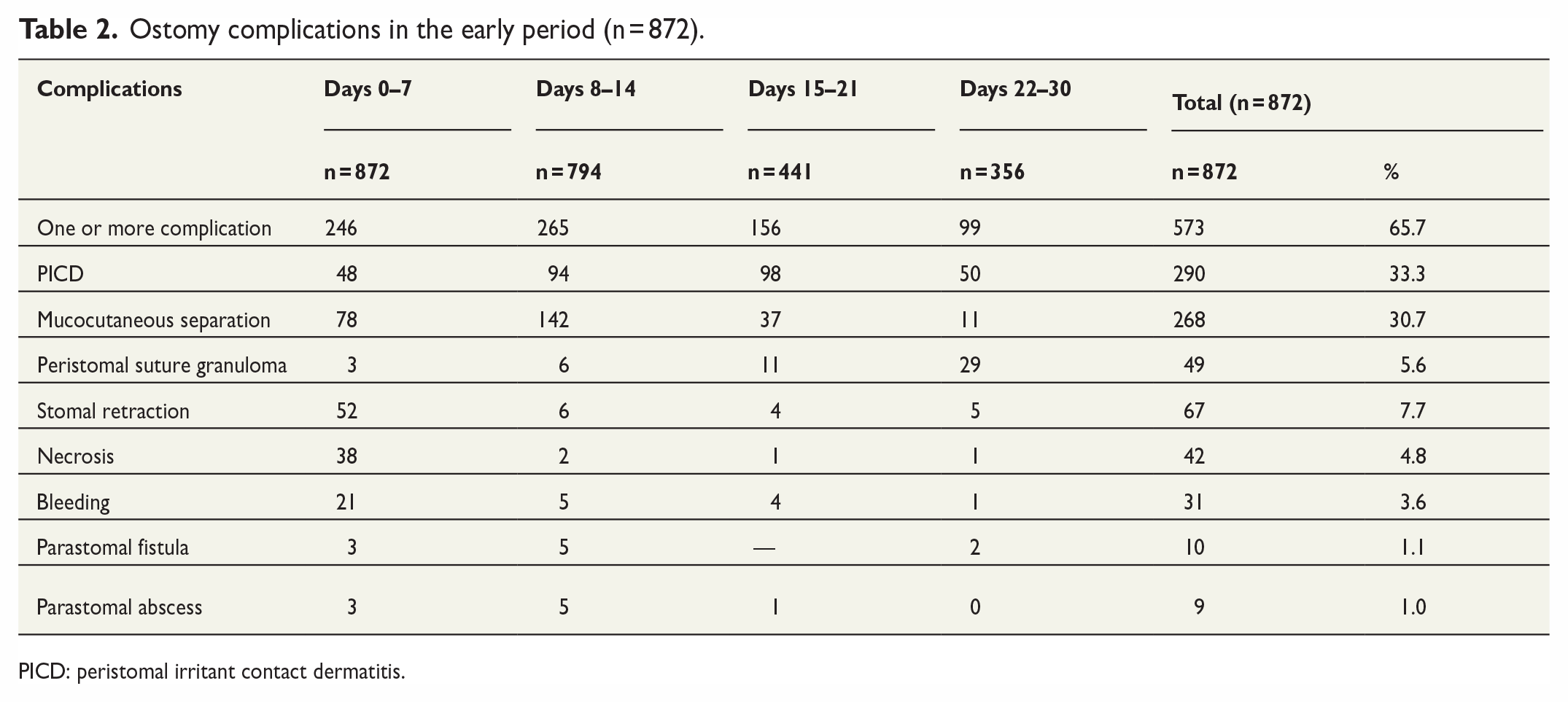
PICD: peristomal irritant contact dermatitis.
When comparing complications based on the urgency of the operation, the rates of necrosis (7.4% versus 3.4%, p = 0.009) and mucocutaneous separation (37.2% versus 27.1%, p = 0.002) were statistically more common after emergency surgery than after elective surgery. PICD was more common in elective surgery (26.0% versus 37.3%, p<0.001). There was no statistically significant difference in the incidence of granuloma, retraction, abscess, or fistula according to the type of surgery (p > 0.05; Table 3).
Distribution of developing ostomy complications by type of the surgery (n = 872).
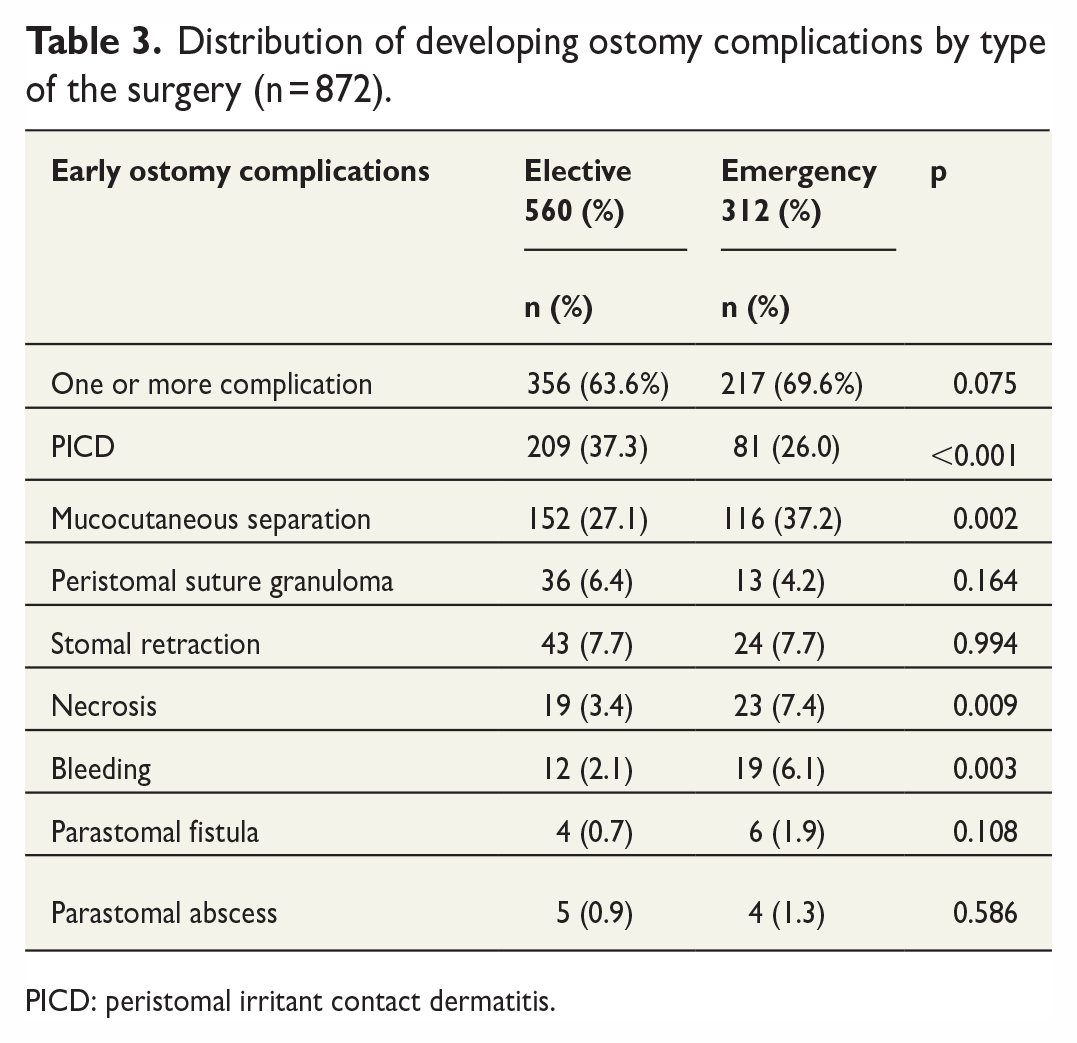
PICD: peristomal irritant contact dermatitis.
The risk factors related to PICD in elective and emergency surgery are summarized in Table 4. The odds of PICD in elective surgery increased with comorbidity (OR = 1.798, 95% CI = 1.220–2.650; p = 0.003), malignant disease (OR = 1.665, 95% CI = 1.008–2.753; p = 0.047), and loop ostomy (OR = 2.113, 95% CI = 1.395–3.201; p < 0.001). Female sex (OR = 1.884, 95% CI = 1.082–3.280; p = 0.025), receiving neo-adjuvant therapy (OR = 2.015, 95% CI = 1.094–3.709; p = 0.024), and having an ileostomy (OR = 2.220, 95% CI = 1.259–3.917; p = 0.006) were risk factors for PICD in emergency surgery (Table 4).
Risk factors for PICD by type of the surgery: Logistic regression.
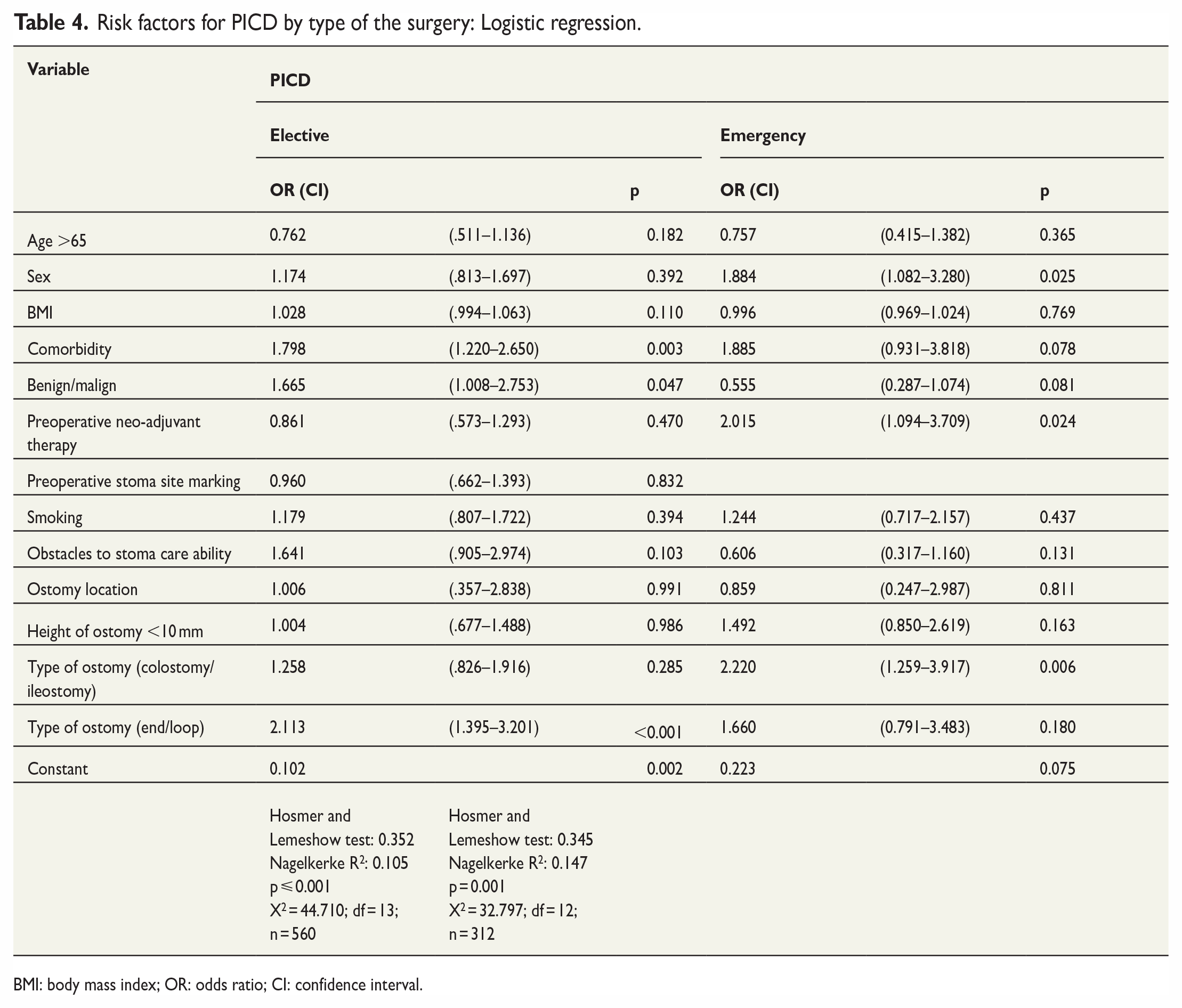
BMI: body mass index; OR: odds ratio; CI: confidence interval.
Table 5 summarizes risk factors related to mucocutaneous separation in elective and emergency surgery. While malignant disease (OR = 1.805, 95% CI = 1.176–2.770; p = 0.007), the height of the ostomy less than 10 mm (OR = 2.104, 95% CI = 1.427–3.103; p < 0.001), and end ostomy (OR = 1.606, 95% CI = 1.053–2.451; p = 0.028) were risk factors for mucocutaneous separation in elective surgery, only the height of the ostomy less than 10 mm (OR = 1.613, 95% CI = 1.010–2.576; p = 0.045) was a risk factor in emergency surgery (Table 5).
Risk factors for mucocutaneous separation by type of the surgery: Logistic regression.
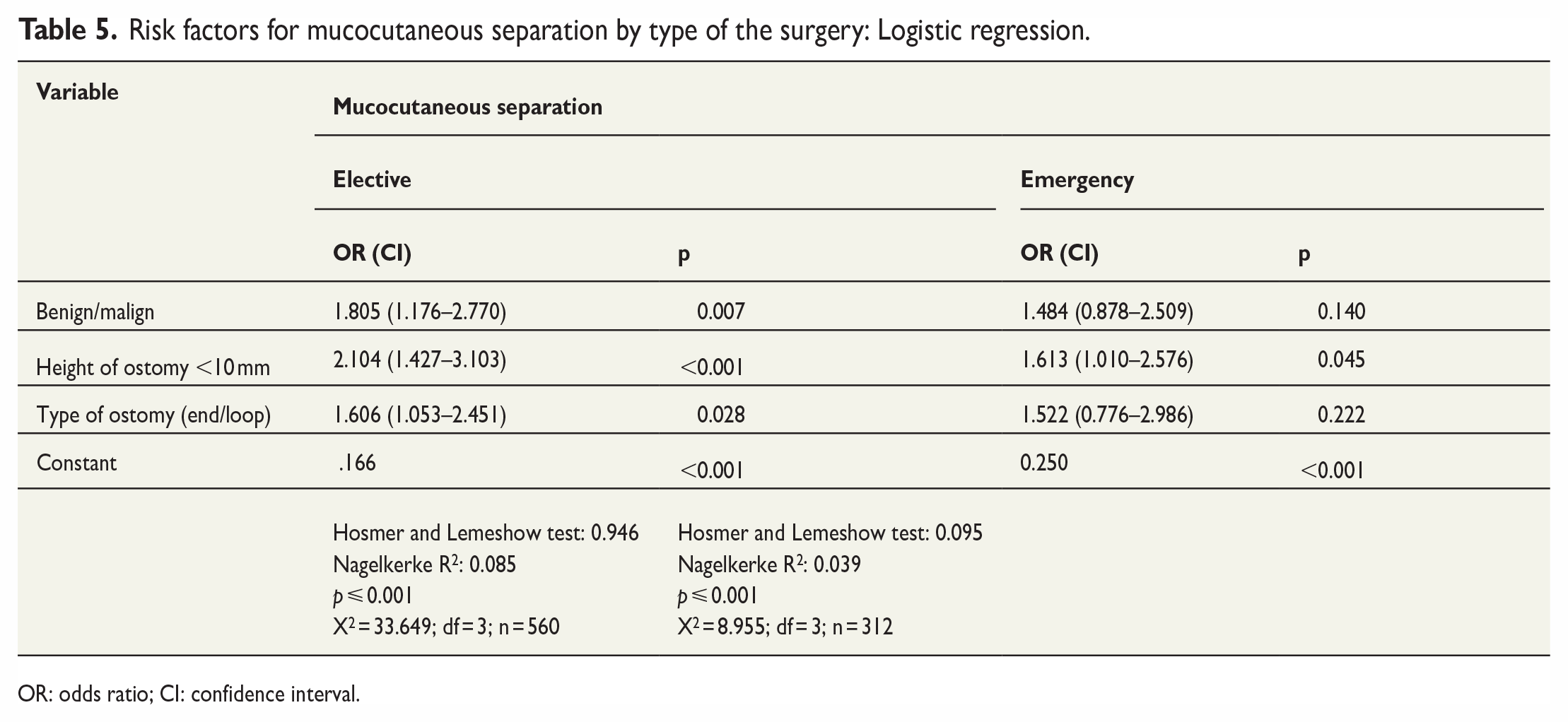
OR: odds ratio; CI: confidence interval.
Discussion
This large retrospective cohort study investigated the rates of ostomy-related complications according to the type of surgery and the risk factors associated with specific complications in the early postoperative period. Early ostomy complications, except for PICD, occurred more frequently after emergency surgery. Several risk factors for PICD and mucocutaneous separation were identified.
Interestingly, PICD was more common in elective surgery patients. The etiology and pathophysiology of PICD are partially understood, and its etiology is multifactorial,20,21 but leakage of fecal ostomy output onto the skin and prolonged skin moistness are the main factors. Factors related to the patient, such as the duration of the pouching systems on the skin and cutting skin barriers larger than the diameter of the ostomy, contribute to the development of PICD. 22 Due to the fluid nature of feces, ileostomy patients may be more exposed to leakage. One reason for PICD being more common after elective surgery in this study may be that many of these patients have a loop ileostomy (Supplementary Table 3). In addition, inappropriate placement of the ostomy due to a lack of site marking is the most important cause of stool leakage.5,23 In this study, the stoma site was marked in only one-third of patients. PICD may also be high in patients who underwent elective surgery due to the lack of stoma site marking.
Mucocutaneous separation was more common in patients undergoing emergency surgery compared with elective surgery in this study. Due to the combination of elective and acute surgery in the other studies,12,13,17,19,24 a direct comparison could not be made. Mucocutaneous separation occurs more frequently in end ostomy patients. 4 In this study, the higher frequency of end ostomy patients undergoing emergency surgery may have contributed to a higher rate of separation in this cohort. The reason for more mucocutaneous separation in emergency surgery may also be derived from the differences in surgical techniques, such as the tension placed on the bowel when an ostomy is created and the excessive cautery usage on the intestinal mucosa. Due to the development of more necrosis in patients undergoing emergency surgery, this may have also triggered separation. 25
Necrosis was more common in patients undergoing emergency surgery in this study. Lindholm et al. 4 reported that the incidence of necrosis was high in a prospective study conducted only on patients who had undergone emergency surgery. Vascular disruptions may occur in the superficial portion of the stoma or at the level of the fascia, which may lead to necrosis in the early postoperative period.25,26 Similarly, bleeding was more common in emergency surgery in this study. In most cases, bleeding may occur because of an abrasion to the ostomy, which is usually caused by poorly fitted or overly tight appliances. More substantial bleeding may be seen in patients with peristomal varices and portal hypertension. 25
Surgical technique plays an important role in preventing complications. Unfortunately, the creation of an ostomy, the final step of emergency surgery, is generally regarded as the least significant aspect of the procedure and can be delegated to less experienced surgeons. The process of creating an ostomy should be regarded as one of the most important aspects of the operation. Having a certified colorectal surgeon who regularly performs ostomy surgery is essential for better results.
Finally, this study determined the risk factors for specific complications in emergency and elective colorectal surgery. Risk factors for ostomy complications show diversity. Many patient-related risk factors have been identified, including age more than 65 years, sex (especially female), obesity, comorbid conditions, stoma site marking, abdominal malignancy, and the type, location, and height of the ostomy.3,8,17,27,28 In parallel with the results of other studies, this study found comorbidity, malignancy, and a loop ostomy to be predictors of PICD in patients who underwent elective surgery in the early periods. Moreover, female sex, preoperative neo-adjuvant therapy, and having an ileostomy influenced the likelihood of PICD in patients who underwent emergency surgery. In both elective and emergency surgeries, the type of ostomy was a risk factor. A prospective study conducted with patients who had both emergency and elective surgeries supports the results of the present study. 17 It showed that patients with a loop ostomy or ileostomy had more skin problems in the early period. Furthermore, an ostomy height of less than 10 mm was a predictor of mucocutaneous separation in both emergency and elective surgeries in this study. The height of the ostomy protrusion is inversely proportional to the likelihood of ostomy complications.12,29,30 In this study, ostomy height was measured at the first evaluation within 24 h after the ostomy creation. Therefore, if technically feasible, the surgeon should avoid an ostomy that is flush with the skin. Malignancy and end ostomy were also risk factors of mucocutaneous separation in the elective surgery. However, it is difficult to compare our results with the results of the other studies because we investigated the risk factors affecting all ostomy complications instead of evaluating the factors affecting mucocutaneous separation and PICD.8,13,19,23 Some risk factors cannot be changed, but some variables can be optimized to reduce complication rates. It is recommended that the height of an ostomy be 10 mm for better results.
Limitations
This study had several limitations, including its retrospective design and single-institution structure. It only disclosed the results for a specific period. Therefore, the results of this study cannot be generalized. In the design of retrospective cohort studies, uncontrolled exposures and conditions may result in unmeasured confounding and bias. It was challenging to identify a disease-exposed cohort and a matched control group, and losses in follow-up may introduce bias. Because not every patient visits postoperatively, the rate is possibly lower or higher than the actual rate. However, the inclusion of the patient group treated at the dedicated colorectal surgical center more than a 9-year period and determining the risk factors for the most common complications according to the type of surgery are the study’s strengths. This study could be utilized to generate a hypothesis that could be prospectively tested and utilized for initiatives to enhance quality.
Conclusion
Early ostomy complications were more likely to occur after emergency colorectal surgery than in an elective setting. Malignant disease, comorbidity, and loop ostomy increase the risk of PICD in elective surgery, whereas female sex, neo-adjuvant therapy, and ileostomy were risk factors for PICD in the emergency setting. The height of the ostomy (less than 10 mm) was a modifiable risk factor for mucocutaneous separation in both emergency and elective surgeries.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231190291 – Supplemental material for Risk factors for early ostomy complications in emergency and elective colorectal surgery: A single-center retrospective cohort study
Supplemental material, sj-docx-1-sjs-10.1177_14574969231190291 for Risk factors for early ostomy complications in emergency and elective colorectal surgery: A single-center retrospective cohort study by Cahide Ayik, Tayfun Bişgin, Deniz Cenan, Berk Manoğlu, Dilek Özden and Selman Sökmen in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969231190291 – Supplemental material for Risk factors for early ostomy complications in emergency and elective colorectal surgery: A single-center retrospective cohort study
Supplemental material, sj-docx-2-sjs-10.1177_14574969231190291 for Risk factors for early ostomy complications in emergency and elective colorectal surgery: A single-center retrospective cohort study by Cahide Ayik, Tayfun Bişgin, Deniz Cenan, Berk Manoğlu, Dilek Özden and Selman Sökmen in Scandinavian Journal of Surgery
Footnotes
Author contributions
Made a substantial contribution to the concept or design of the work; acquisition, analysis, or interpretation of data: CA, TB, DC.
Drafted the article or revised it critically for important intellectual content: All authors, and especially SS and DÖ.
Approved the version to be published: All authors.
Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.