
Abstract
Background and aims:
Parastomal hernia (PSH) is a common complication after the creation of a colostomy, with a prevalence of approximately 50%. Despite the high frequency, little is known how PSH affects the cost of colostomy care.
The hypothesis in this study was that PSH increases the cost of colostomy care compared with not having a PSH.
Methods:
Two groups with (N = 61) and without (n = 147) PSH were compared regarding costs of stoma appliances and visits. The population from a large randomized trial comparing construction of colostomy with or without prophylactic mesh (STOMAMESH) was used and cross-matched with health economic data from the National Pharmaceutical Register, 1 year after initial surgery.
Results:
Patients with and without a PSH were similar in basic demographic data. No difference in cost of stoma appliances (with PSH 2668.3 EUR versus no PSH 2724.5 EUR, p = 0.938) or number of visits to a stoma therapist (p = 0.987) was seen, regardless of the presence or not of a PSH.
Conclusions:
PSH appears not to affect costs due to colostomy appliances or the need to visit a stoma therapist, in the first year. The lesson to be learnt is that PSHs are not a driver for costs. Other factors may be determinants of the cost of a colostomy, including manufacturers’ price and persuasion, means of procurement, and presence of guidelines.
Introduction
Sustainability of the healthcare system is a critical issue reaching far beyond the regional perspective. Rises in healthcare costs together with restrictions in resources available increase pressure on healthcare budgets worldwide.1 Decision-makers in healthcare organizations are continuously pressed to achieve a balance between cost and benefit. To improve allocation of resources, we must strengthen our understanding of the implications of our decisions, particularly the way in which resources are utilized. In this study, we specifically investigate the impact of parastomal hernia (PSH) on healthcare economy in the hope that our results will assist decision-makers leading to more effective utilization of the resources available.
PSH is a common complication after colostomy presenting as a protrusion or a bulge of the stoma that contains bowel or other content of the abdominal cavity. Sometimes it is hardly noticeable and difficult to diagnose while in other cases it is large and obvious.1,2 In retrospective studies, the prevalence of PSH has been reported to be a few percent up to 7%.3–5 Recent randomized controlled trials, however, have shown figures between 4.5% and 50%.6–8 In Sweden, approximately 40,000 individuals live with a stoma. 9 Despite this, only a small fraction of individuals with PSH receive corrective surgery for several reasons including lack of healthcare resources, poor results of surgery itself, and a high complication rate.10,11 PSH is known to cause many problems for the patient such as episodes of intestinal obstruction, skin problems, pain, problems with appliances, limitation of activity, difficulty in finding suitable clothing, social restrictions, erratic function of the stoma, and cosmetic embarrassment.12,13 Symptoms range from none to debilitating, for example, some studies report that more than 50% of patients waiting for corrective surgery suffer at least one symptom, while others report that more than 25% of patients with a PSH have no symptoms at all.13,14
What is known about the cost of a colostomy for the healthcare system? The cost of stomal appliances depends on level of dispensing, which can be national, regional, local, or individual, that is, delivery from the manufacturer to the national dispensary, the regional healthcare provider, or to the private individual. In view of the complexity involved, one would expect some degree of variation in price. In Sweden, most healthcare is public, provided by the National Health Service, and we know from a large review carried out by the Swedish Dental and Pharmaceutical Benefits Agency that costs associated with ostomies vary more than 50% between different regions even though healthcare providers are all non-profit government funded organizations. 9 The reason for this, however, is not known. The prescription of stomal appliances is a complex procedure and there are seldom guidelines to help reduce costs. 15 It is known that peristomal skin problems increase the cost of a colostomy due to more complex and expensive stomal appliances required and more frequent visits to the stoma therapist.16,17 Little is known of other factors that determine the cost. Depending on the system of reimbursement, the financial burden for the individual also varies with the degree of complication, which is yet another reason to map the factors that increase the cost of appliances. 18 The market for stomal appliances and associated products in Sweden alone is worth over 49.2 million euros (EUR) and rising, the reason being unknown. 9 The global market for colostomy products was worth 2.4 billion EUR in 2017 and projected to increase to 3.1 billion EUR in 2022. 19
The hypothesis of this study was that in the short-term perspective, PSH increases the cost of stoma care in terms of material and visits to a stoma nurse, compared with not having a PSH.
Methods
Basis
The basis of this healthcare economy study was the STOMAMESH trial, from which our population was extracted. 8 STOMAMESH is the largest randomized controlled multicentre trial studying the possible benefits of prophylactic mesh reinforcement when constructing a stoma. The trial protocol adheres to the Helsinki Declaration and was approved by the Regional Ethics Committee at Umeå University, Sweden (DNR 07-081M). The STOMAMESH trial is registered at ClinicalTrials.gov (Identifier: NCT00917995) and adheres to the CONSORT 2010 criteria for RCTs. It is a two-armed trial where patients receiving an end-colostomy are randomized to standard colostomy or colostomy with mesh reinforcement. All patients were carefully followed for a year, including registration of all visits to a stoma therapist, complications, and reoperations. Patients in the STOMAMESH trial were divided into two groups, PSH or not, and healthcare economy data were collected for both groups.
Data collection
The primary endpoint of this study was total cost of stomal material (i.e. stoma bags and skincare products) and the total number of visits to a stoma therapist during the first year after surgery. The STOMAMESH trial from which the present population was extracted was designed as follows: The primary endpoint was PSH 1 year after initial surgery, assessed by computerized tomography using the Moreno-Mathias scale, and by clinical examination. 1 The reason for choosing the follow-up at this specific time point was because it coincided with the routine follow up after cancer surgery. The initial randomization in the STOMAMESH trial was stratified per hospital in blocks of four, to ensure balance between the two arms and was found to be evenly distributed in the original trial. A secondary endpoint was registration and detection of complications; all individual patient data were collected prospectively with individual case report forms. Complications were divided in surgical complications and other complications. The surgical complications were further divided into wound infection, deep infection, intestinal obstruction, stoma necrosis and reoperation within 30 days. Tertiary goals were quality of life and need for healthcare resources, during follow-up, all visits to a stoma therapist were registered along with measures regarding recurrence, complications, and health-related quality-of-life data. To access the cost of stomal appliances, we used the National Pharmaceutical Register (NPR), managed by the Swedish Board of Health and Welfare. All medicines prescribed in Sweden are registered as well as all consumables where prescription is required (for example products related to stoma care). The register has 100% coverage and contains information regarding sex, age, anatomical therapeutic chemical (ATC) codes, costs (for the individual and for the provider), and profession of prescriber. The calculated loss of data at validation was 0.2% of all data. 20 All stoma care products are prescribed and registered in the register including accessories, skin care paste and removers, according to legal regulations. Alterations or purchase of garments are not covered by the healthcare system and thus not included in the register. Our STOMAMESH data were cross-matched with data from NPR using social security number as the link between the registers, thus giving us the total cost for all products during the first year after construction of the colostomy. The number of visits to a stoma therapist during the first year after surgery was retrieved from the STOMAMESH data base. All patients had a routine follow-up, a visit to a stoma nurse, within 2–4 weeks after discharge, further visits were on a need basis. Telephone or email contacts were not registered.
Statistics
All data were entered in a secure protected database. IBM SPSS Statistics 26 software was used. Analyses of group variables were performed with the chi-square test, and all analyses of continuous variables were performed with the independent Student’s t-test. A p-value < 0.05 was considered significant. The initial power analysis from the STOMAMESH trial assumed PSH rates of 20% without and 5% with a mesh. Assuming 50% loss to follow-up, motivated by the malignant nature of the underlying disease, sample sizes of 110 patients in each group were required to achieve a power of 80%. The groups with and without PSH, from the STOMAMESH trial, were tested for skewness and kurtosis and had normal distribution regarding body mass index (BMI), American Society of Anaesthesiologists (ASA) classification, and so on (see Table 1), thus parametric tests were used for all analyses. We also expanded the inclusion period for costs to 357 days to avoid calculation problems due to a leap year. This study was approved by the Regional Ethics Committee at Umeå University, Sweden (DNR 07-081M (addition 2018-224-32M)).
Basic demographic data in the trial population, at randomization in STOMAMESH.
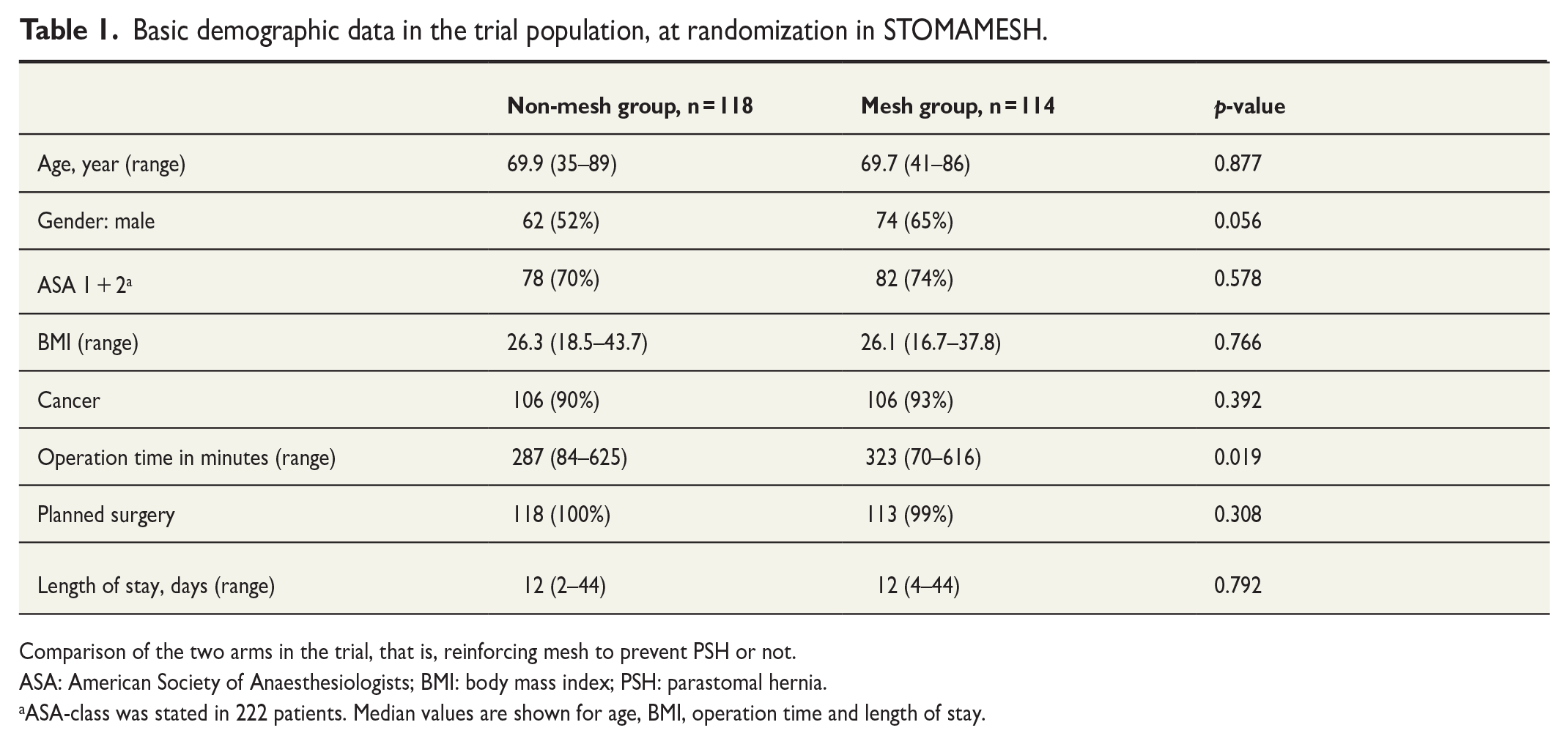
Comparison of the two arms in the trial, that is, reinforcing mesh to prevent PSH or not.
ASA: American Society of Anaesthesiologists; BMI: body mass index; PSH: parastomal hernia.
ASA-class was stated in 222 patients. Median values are shown for age, BMI, operation time and length of stay.
Results
Recruitment
Between December 2007 and October 2015, 240 patients were enrolled into the trial (20 extra to compensate for drop-outs; see Fig. 1). Eight Swedish hospitals participated in the trial: four university hospitals, two regional hospitals, and two county hospitals. The total catchment area of these hospitals is equivalent to 15% of the total population of Sweden. Basic demographics of the trial population, at inclusion, were similar and the only significant difference was operation time, which was to be expected due to the insertion of a reinforcement mesh in one arm (see Table 1). When grouping basic demographic data of patients with PSH or not, no differences were found (see Table 2).
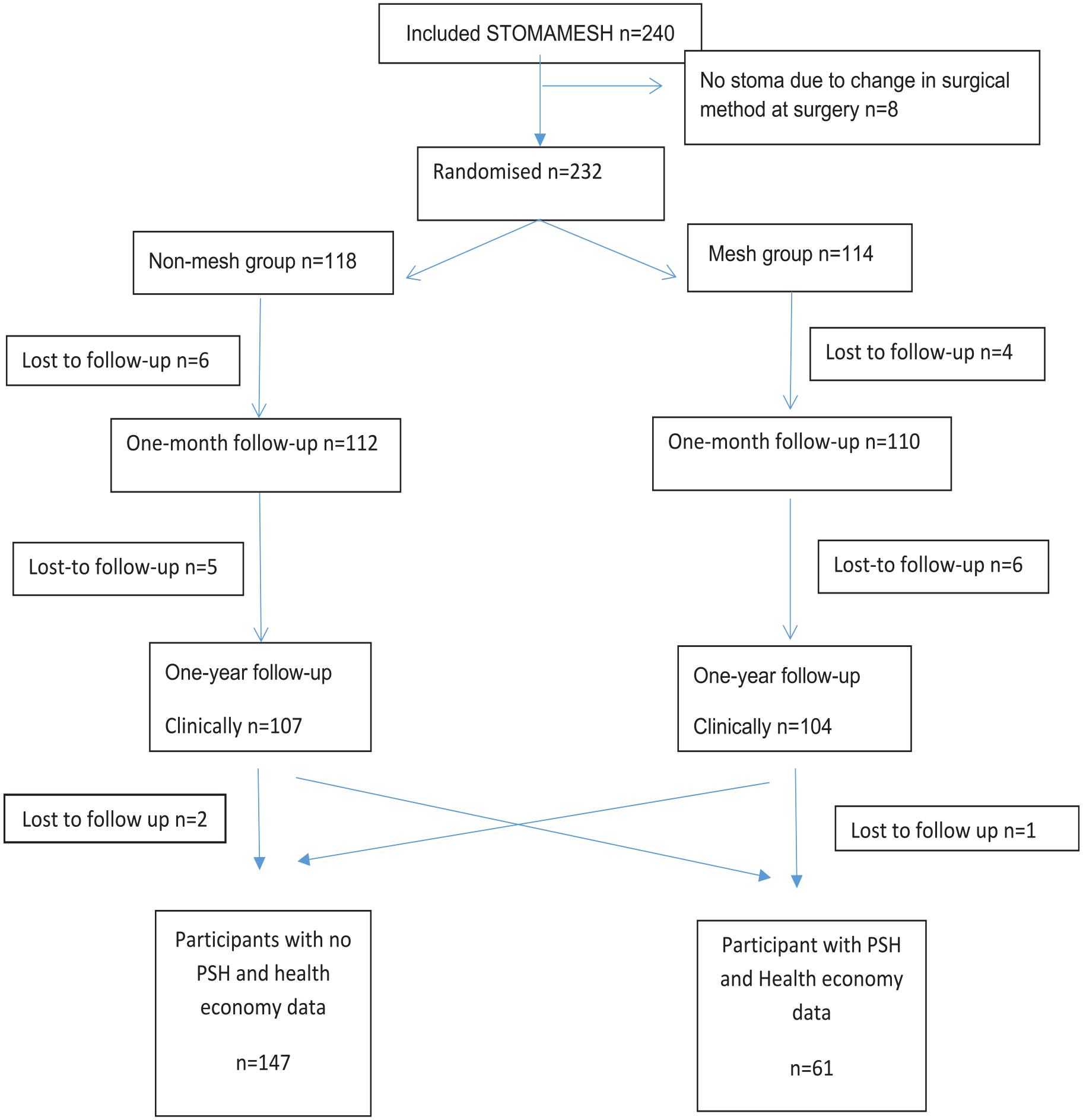
Consort diagram showing parastomal hernia does not impact the cost of colostomy care.
Basic demographic data in the trial population grouping on non-PSH or PSH, at 1 year follow-up.
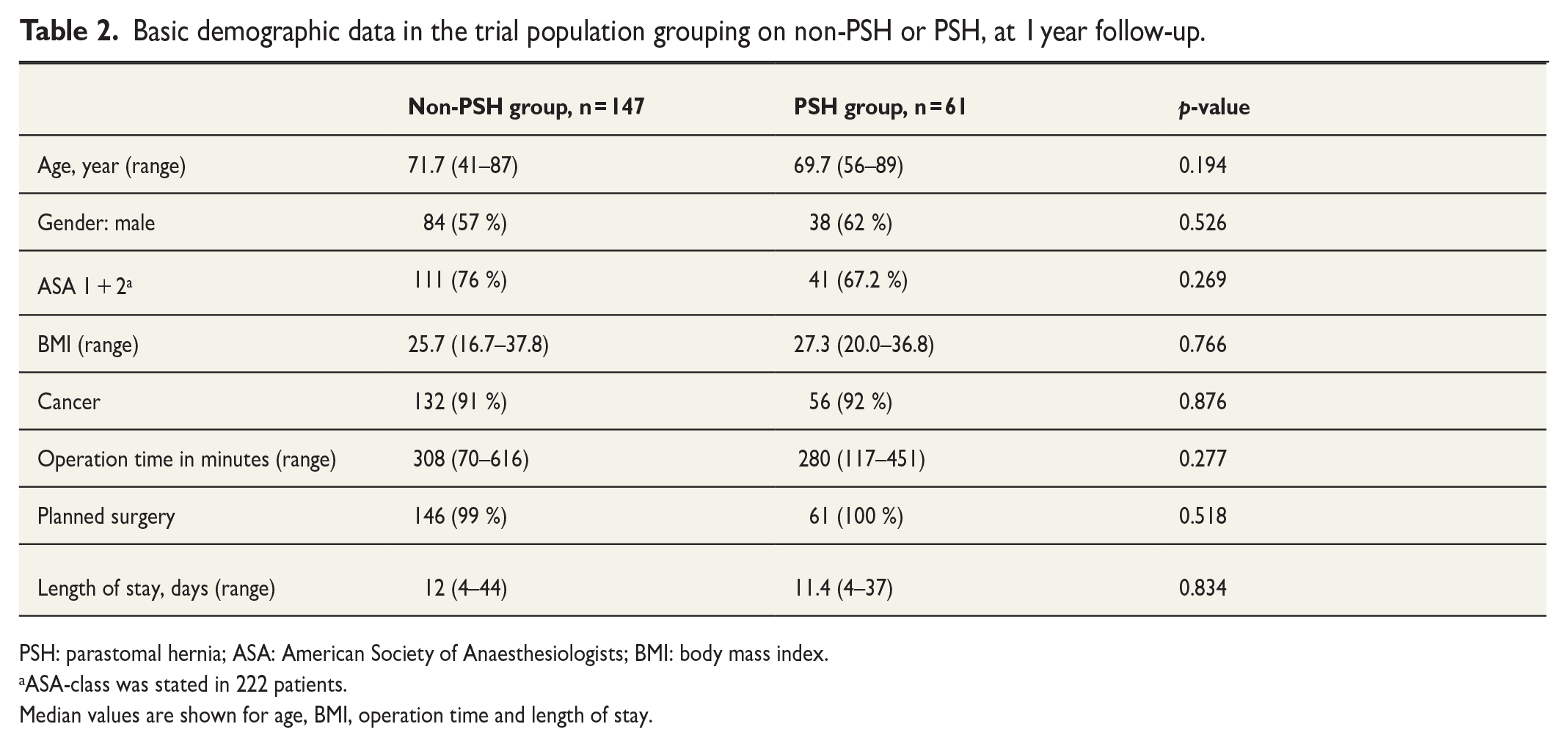
PSH: parastomal hernia; ASA: American Society of Anaesthesiologists; BMI: body mass index.
ASA-class was stated in 222 patients.
Median values are shown for age, BMI, operation time and length of stay.
Missing data
One year after inclusion, 211 patients in the STOMAMESH trial were followed up clinically. We were able to retrieve data from the NPR for all except three patients. Furthermore, 32 patients did not complete the STOMAMESH trial due to illness within 1 year or patient refusal to participate in the follow-up. It is not clear why the three patients with missing data were not registered in the NPR.
Findings
There were no differences regarding frequency of PSH or complications from the stoma between the two groups in the STOMAMESH trial. 7 In the non-mesh group, the PSH rate was 30% (measured clinically) and 34% (measured radiologically). In the mesh group, the PSH rate was 29% (measured clinically) and 32% (measured radiologically). 7 The overall complication rate was similar, 32% in the non-mesh group and 34% in the mesh group. No significant differences were found regarding minor complications (wound infection) or major complications (reoperations, stoma necrosis, and deep infections) between the group with PSH and the group without, including stoma complications. When analyzing stomal appliance costs, no significant difference was found between the PSH group and the group without PSH (see Table 3) and no statistically significant difference was found regarding number of visits to a stoma therapist. No sub-analyses were made grouping the stoma appliance costs into different categories (bags and accessories, for example). Patients with PSH had 3.96 (standard deviation 1.48, range 1–12) visits to a stoma nurse and those without, 3.95 (standard deviation 2.86, range 1–6) visits (see Table 3). The difference in the cost of dressings and appliances between the groups was small. The mean cost per patient over the 1 year period was 2668.3 EUR in the PSH group and 2724.5 EUR in the group without (see Table 3) and was not statistically significant. If the mean cost was grouped either on gender (male 2446.6 EUR versus female 2975.0 EUR, p-value = 0.16) or BMI over or under 25 instead (BMI < 25 2501.0 EUR versus BMI > 25 2789.1 EUR, p-value = 0.153), no significant difference was found. No difference was seen if the mean cost was grouped on patients with high frequency of visits to the stoma nurse compared to patients with few visits, during the first year after index surgery. We considered three or less visits to be a low frequency (three or less visits 2273.2 EUR versus visits more than three 2619.6, p-value = 0.145). When grouping the cost according to the original randomization to prophylactic mesh versus no prophylactic mesh, in the STOMAMESH trial, no difference could be found either (no mesh 2659.7 EUR versus mesh 2676.1 EUR).
The cost of stoma dressings and number of visits to a stoma therapist, at 1 year.
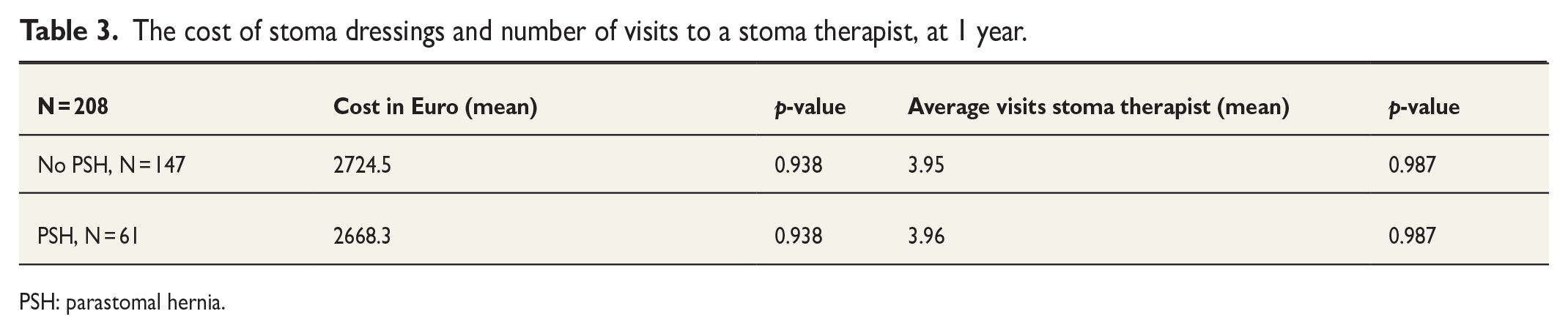
PSH: parastomal hernia.
Discussion
In this study, the occurrence of a PSH after an end colostomy is fashioned did not affect the costs of stomal dressings and related products, nor did it affect the number of visits to a stoma therapist. This was unexpected since we know PSH increases the burden of symptoms. It must be remembered that when following up colostomy creation, PSH is a long-term complication, and the one-year follow-up in this study may not have adequately captured patients with a PSH or the associated costs. Longer follow-up times are advisable.
This study attempts to analyze any increase in cost of colostomy care associated with the occurrence of a PSH. Patient data were taken from the largest multicentre randomized trial (STOMAMESH), on complications and the occurrence of PSH after creation of the colostomy. In all, 208 patients were followed up at 1 year, the largest study population on this topic so far described and the rate of missing data was low (13% measured as intention to treat). It is also known from the STOMAMESH trial that the study population reflects routine healthcare. 7
A weakness of this study is that we have no knowledge whether the patients used all the products prescribed even though they were picked up from the pharmacy. However, there was nothing to suggest any difference in pattern of consumption between the groups.
The costs of surgery for incarcerated PSH or corrective surgery were not considered since no such event occurred during the study period. Inevitably some patients will undergo surgery for incarceration with its high cost and morbidity rate. 9 Other patients with PSH are likely to demand treatment for reasons previously described. 13 Hospital visits, other than to a stoma nurse, for PSH-related issues were not considered and this would have increased costs in the PSH group.
It might have been more pertinent to only consider PSHs with clinically significant symptoms since a small PSH detected on CT scan could be purely incidental.
The lesson to be learned from this study is that factors other than PSH determine the cost of stoma care. Such factors include individual demands, preferences of the prescribing stoma nurse, and how the distribution of stoma dressings is organized. Having a colostomy negatively affects a person’s quality of life; the occurrence of a PSH even more so. 21 The avoidance of skin problems should be given highest priority in our attempt to improve life for the patient and reduce costs. An important factor is that low stomata lead to more skin problems and thus higher costs. 22 Furthermore, repairing a PSH has no effect on skin problems. 23 In Sweden, almost all stoma dressings and associated products are prescribed by approximately 120 stoma therapists, and the total value of the market in 2016 was 49.2 million EUR, rising by 3% per year. This implies that each stoma therapist on average prescribes products worth 410,000 EUR each year. A prime intervention to change prescription patterns and reduce costs would be the issue of national, regional, and local guidelines for stoma therapists to follow. This would also ensure equality of care regardless of place of residence. Another factor that dictates costs is how stomal appliances are obtained and distributed. This differs between countries, regions, and local care providers, and few studies have been published on the subject.16,24 It is important that decision-makers at all levels understand that the procurement and selection of colostomy care products probably has a greater impact on costs than surgical problems such as PSH.
This study provides new insight into the costs of stoma care that constitute a considerable portion of our increasing healthcare expenditure. The impact of stoma complications on healthcare economy has not been sufficiently explored in the literature. This study sheds some light on the issue, strengthening our understanding of the implications of healthcare decisions, particularly how resources available are used. Contrary to the hypothesis of this study, the presence of PSH did not affect the cost of stomal appliances or the number of visits to a stoma therapist in the short-term perspective.
A lesson to be learned from this study is that factors other than PSH determine the cost of stoma care such as individual demands, preferences of those prescribing stomal dressings, and how stomal appliances are obtained and distributed. There is a great need for guidelines on the prescribing of stomal material (stoma-bags and skincare products) and visits to the stoma therapist.
Further research in needed to determine the factors behind the costs of stoma care and how these develop over time. A qualitative interview study to determine factors affecting how stoma therapists decide on which products to prescribe, and/or a study on how stoma appliances are obtained and distributed are two candidates for future research. Results from such studies could form the basis for the construction of guidelines to be followed by stoma therapists in the future.
Footnotes
Acknowledgements
The authors would like to thank the research nurse Lisa Eskilsson, Department of Surgery, Sunderby hospital, Region Norrbotten and Robert Lundqvist, statistician, Region Norrbotten.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was received from the Swedish Research Council 214-7196, ALF support RV-927121, and The Department of Research and Development, Region Norrbotten.