
Abstract
Background:
Peripheral femoro-femoral venoarterial extracorporeal membrane oxygenation (VA-ECMO) is viable for fast hemodynamic assistance during cardiogenic shock. Ultrasound-guided closure with a large-bore device (MANTA®) is a feasible option potentially replacing surgical arteriotomy closure in peripheral VA-ECMO decannulation.
Methods:
This retrospective study included patients weaning from percutaneously inserted femoro-femoral VA-ECMO at the Helsinki University Hospital, Finland in 2012–2020. The primary endpoints were access-site complications, a composite of hematomas/seromas/surgical site infections (SSIs), and the safety endpoint of vascular complications (VCs).
Results:
A total of 100 consecutive percutaneously implanted and weaned VA-ECMO patients were stratified into two groups by decannulation strategy: percutaneous ultrasound-guided MANTA device (n = 21, 21.0%) or surgical approach (n = 79, 79.0%). The mean age of the cohort was 51 ± 13 years and females represented 25.0%. The technical success rate of the percutaneous ultrasound-guided MANTA technique was 95.2%. In multivariate analysis, surgical closure was associated with a higher incidence of combined access site hematomas/seromas/SSIs compared to percutaneous ultrasound-guided deployment of MANTA device (44.3% versus 9.5%, odds ratio (OR): 7.162, 95% confidence interval (CI): 1.544–33.222; p = 0.012). Similarly, access-site complications necessitating interventions were more frequent in the surgical closure group compared to US-MANTA (ultrasound-guided MANTA) group (26.6% versus 0.0%, p = 0.005). VCs were infrequent in both groups without any significant intergroup difference (p > 0.99).
Conclusions:
Percutaneous ultrasound-guided MANTA closure of the femoral artery after VA-ECMO decannulation was associated with high technical success rate and low incidence of VCs. Compared to surgical closure, access-site complications were significantly less frequent, along with access-site complications necessitating interventions.
Keywords
Context and relevance
Peripheral venoarterial extracorporeal membrane oxygenation (VA-ECMO) decannulation is traditionally performed through femoral cut-down and purse-string closure around cannulas. However, the technique is invasive and troublesome, vascular closure devices such as the MANTA device, especially with ultrasound assistance, have increased their application in terms of safety and efficiency, potentially replacing surgical closure of femoral artery. In our study, we reviewed our institutional experience retrospectively and found significantly fewer access-site complications, composed of hematomas, seromas, and surgical site infections, requiring interventions with the ultrasound-guided MANTA technique compared to surgical arteriotomy closure. Ultrasound-guided vascular closure with the MANTA device was associated with high technical success, and only few vascular complications, implicating it can be safely used during extracorporeal membrane oxygenation (ECMO) decannulation.
Introduction
Peripheral femoro-femoral venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a salvage therapy for patients in cardiogenic shock requiring transient cardiac and ventilatory assistance. 1 Decannulation is performed when weaning from extracorporeal membrane oxygenation (ECMO) is likely or if bridging to left ventricular assist device (LVAD) or cardiac transplantation is considered. Our center previously performed large-bore arteriotomy closure using the surgical femoral cut-down technique, but since 2019, the collagen plug-based MANTA vascular closure device (VCD) (Teleflex, Morrisville, NC, USA) with ultrasound assistance has been preferred.
We reviewed our institutional experience to evaluate the safety and feasibility of the ultrasound-guided MANTA device for femoral artery closure after ECMO decannulation compared to surgical decannulation regarding bleeding, access-site complications, and complications of the femoral artery.
Methods
A total of 100 consecutive patients undergoing percutaneous VA-ECMO cannulation and weaning from ECMO between October 2012 and November 2020 at Helsinki University Hospital, Finland, were retrospectively analyzed (Fig. 1). The principal inclusion criteria were percutaneous peripheral cannulation, successful weaning from VA-ECMO, and decannulation. Based on decannulation technique, two groups were identified: (1) percutaneous decannulation with the ultrasound-guided MANTA VCD (n = 21) and (2) surgical decannulation and closure through a groin incision (n = 79). Subgroup of patients (n = 64) without LVAD or cardiac transplantation after peripheral VA-ECMO decannulation were included in the endpoint of bleeding complications. The Institutional Review Board approved this study and waived informed patient consent since data were collected from medical records without patient contact.
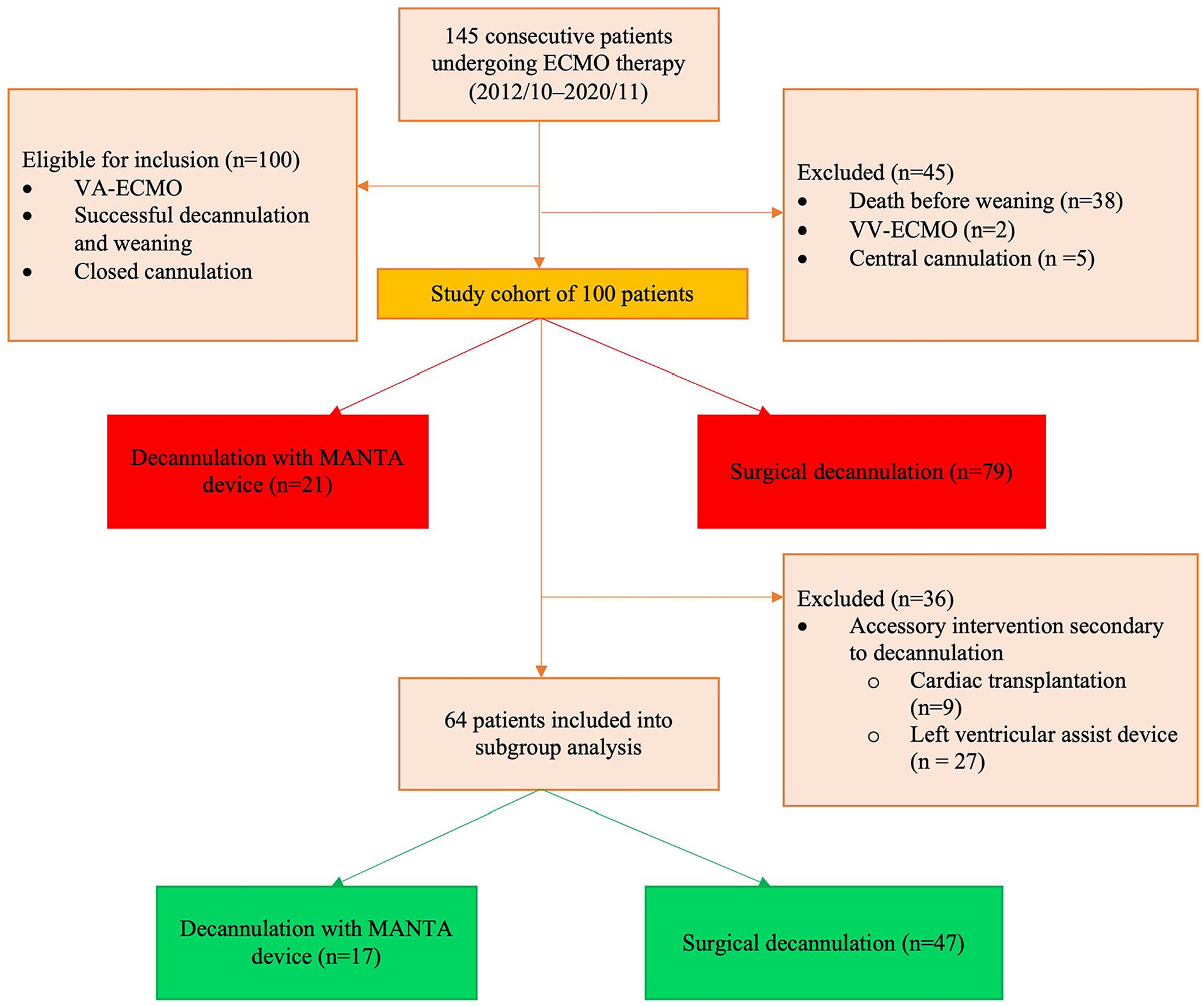
Study flow chart. The recruitment of extracorporeal membrane oxygenation (ECMO) patients divided into the surgical and percutaneous ultrasound-guided vascular closure device (MANTA) groups. Study groups marked with red boxes and substudy groups with green boxes.
ECMO installation technique
All patients (n = 100) were cannulated percutaneously by cardiothoracic surgeons using the Seldinger technique. Groin vessels were punctured with ultrasound guidance. Cannulas were advanced over guidewires and secured to skin following sequential dilatations.
Decannulation technique
Toggle placement and collagen pad compaction were confirmed by ultrasound after arterial cannula (15–17F) removal and MANTA device deployment 2 (Fig. 2). The distal perfusion sheath was removed with an Angio-Seal closure device. A deep Z-shaped thick suture was placed around the venous cannula before its removal, and a sandbag applied on the vascular access site for 4 h to prevent the venotomy site from oozing. In the surgical approach, the cannulas were exposed in the femoral artery and femoral vein, through a groin incision. After cannula withdrawal, the arteriotomy and venotomy were closed with a purse-string suture. The wound was closed in layers.
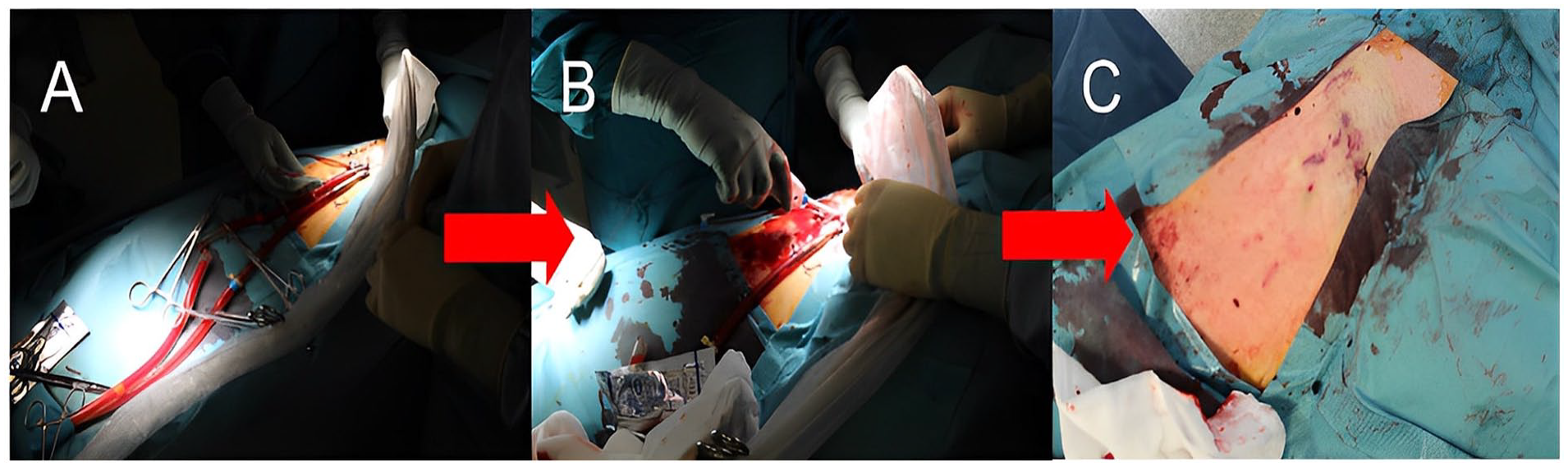
(A) Arterial line puncture for stiff guidewire insertion, (B) percutaneous femoral arteriotomy closure with MANTA device, and (C) groin after decannulation.
Technical success was defined as percutaneous ultrasound-guided vascular closure with the MANTA device without consequential endovascular or surgical intervention. VCD failure was defined to be failure of MANTA (18 F) to achieve hemostasis at the arteriotomy site, requiring alternative treatment to manual compression.
Bleeding, vascular, and other complications
Bleeding complications and blood product use were studied only for the subgroup (n = 64) weaned from VA-ECMO without additional intervention. Data on bleeding and blood product use were collected on decannulation day and the following day (48 h), reflecting the decannulation-induced bleeding, and as recommended by the Valve Academic Research Consortium (VARC)-3 criteria. 3 Bleeding severity was categorized as minor (VARC type 1), major (VARC type 2), life-threatening (VARC type 3), or leading to death (VARC type 4). 3
VARC-3 criteria 3 were used to define complications of the femoral artery (pseudoaneurysm, arteriovenous fistula, distal embolization, and VCD failure). They were considered major if they were associated with death, VARC type ⩾2 bleeding, that is, transfusion of over 2 units of packed red blood cells (RBCs) or perioperative hemoglobin drop >3 g/L, limb ischemia, or irreversible focal or global neurologic impairment. Otherwise, they were considered minor. Non-overt bleeding not fulfilling the VARC type 1-4 criteria was categorized as a hematoma/seroma complication.
Complications were quantified by imaging or clinical examination. Post-decannulation surveillance was not protocolized but was rather driven by clinical concerns. Pseudoaneurysms were not screened, but ultrasound was delicately requested, if clinically suspected.
Type 4 device failure 2 was defined as aberrant collagen pad placement inside the vessel.
Statistical analysis
Statistical analyses were conducted with SPSS (version 26.0, IBM SPSS Statistics, IBM Corp., Armonk, NY, USA). Categorical data are reported as counts and percentages and evaluated using Pearson’s χ2 test or Fisher’s exact t test. Continuous variables are reported as mean and standard deviation or median and interquartile range and analyzed using Student’s t test or Mann–Whitney U test depending on distribution normality. Favorable variables with p less than 0.2 in univariate analysis were selected for multivariate binary logistic regression. Risk estimates were reported as odds ratio (OR) with 95% confidence interval (CI). Statistical significance was set at p < 0.05.
Results
Patients’ characteristics
There were 100 (mean age: 51 ± 13 years and females: 25.0%) peripheral femoro-femoral VA-ECMO patients that underwent decannulation and closure of femoral artery with the percutaneous ultrasound-guided MANTA technique (n = 21, 21.0%) or surgical approach (n = 79, 79.0%). The study groups differed in the incidence of atrial fibrillation (p < 0.001) and hypertension (p = 0.011). The groups did not differ regarding preoperative medications. There was no significance difference in preoperative bleeding markers; thrombocyte level, thrombin time (TT-%, creatinine level; Table 1). ECMO indication and extracorporeal cardiopulmonary resuscitation for ECMO initiation also did not differ statistically significantly between groups (Table 2).
Clinical characteristics of peripheral venoarterial extracorporeal membrane oxygenation patients (n = 100).
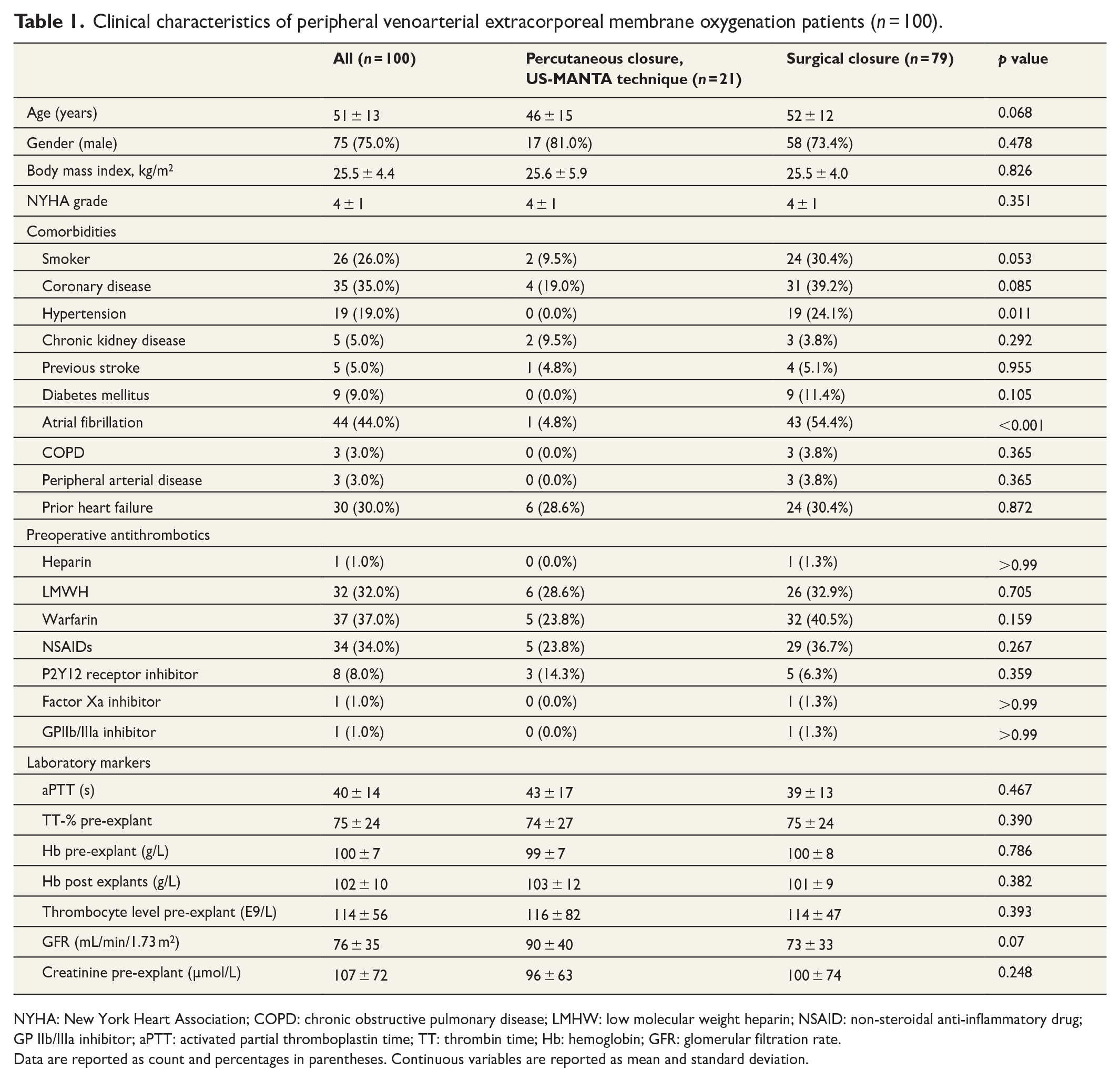
NYHA: New York Heart Association; COPD: chronic obstructive pulmonary disease; LMHW: low molecular weight heparin; NSAID: non-steroidal anti-inflammatory drug; GP IIb/IIIa inhibitor; aPTT: activated partial thromboplastin time; TT: thrombin time; Hb: hemoglobin; GFR: glomerular filtration rate.
Data are reported as count and percentages in parentheses. Continuous variables are reported as mean and standard deviation.
Procedural characteristics of peripheral venoarterial extracorporeal membrane oxygenation patients (n = 100).
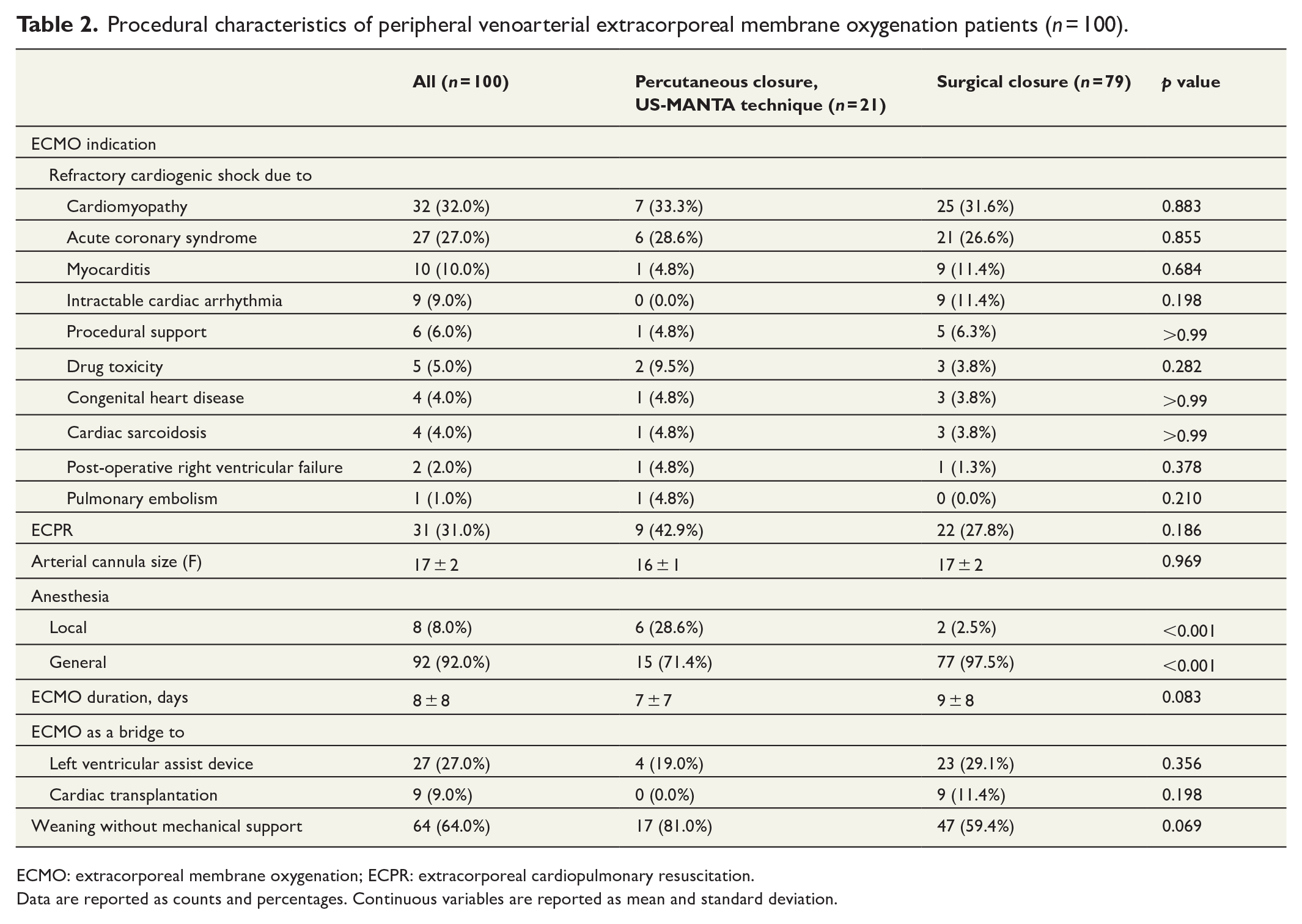
ECMO: extracorporeal membrane oxygenation; ECPR: extracorporeal cardiopulmonary resuscitation.
Data are reported as counts and percentages. Continuous variables are reported as mean and standard deviation.
Safety and feasibility of US-MANTA technique
Technical success was 95.2% in the percutaneous group. The patient with MANTA vascular device failure had peripheral VA-ECMO cannulas for 25 days, and hemostasis achievement required additional endovascular anchor ballooning due to type 4 closure device failure. 2 Concurrently, and with the same mechanism, the Angio-Seal (Terumo Medical Corporation, Somerset, NJ, USA) VCD’s hemostatic sponge occluded the superficial femoral artery, requiring surgical repair.
In the subgroup analysis (n = 64), decannulation strategy was not associated with life-threatening bleeding complications (Table 3). Three patients suffered major bleeding and vascular complications (VCs) requiring unplanned surgical or endovascular intervention, two from the surgical group (one requiring suture closure and one patch angioplasty), and one from the ultrasound-MANTA group (aforementioned technical failure case).
Groin complications after peripheral venoarterial extracorporeal membrane oxygenation (n = 100).
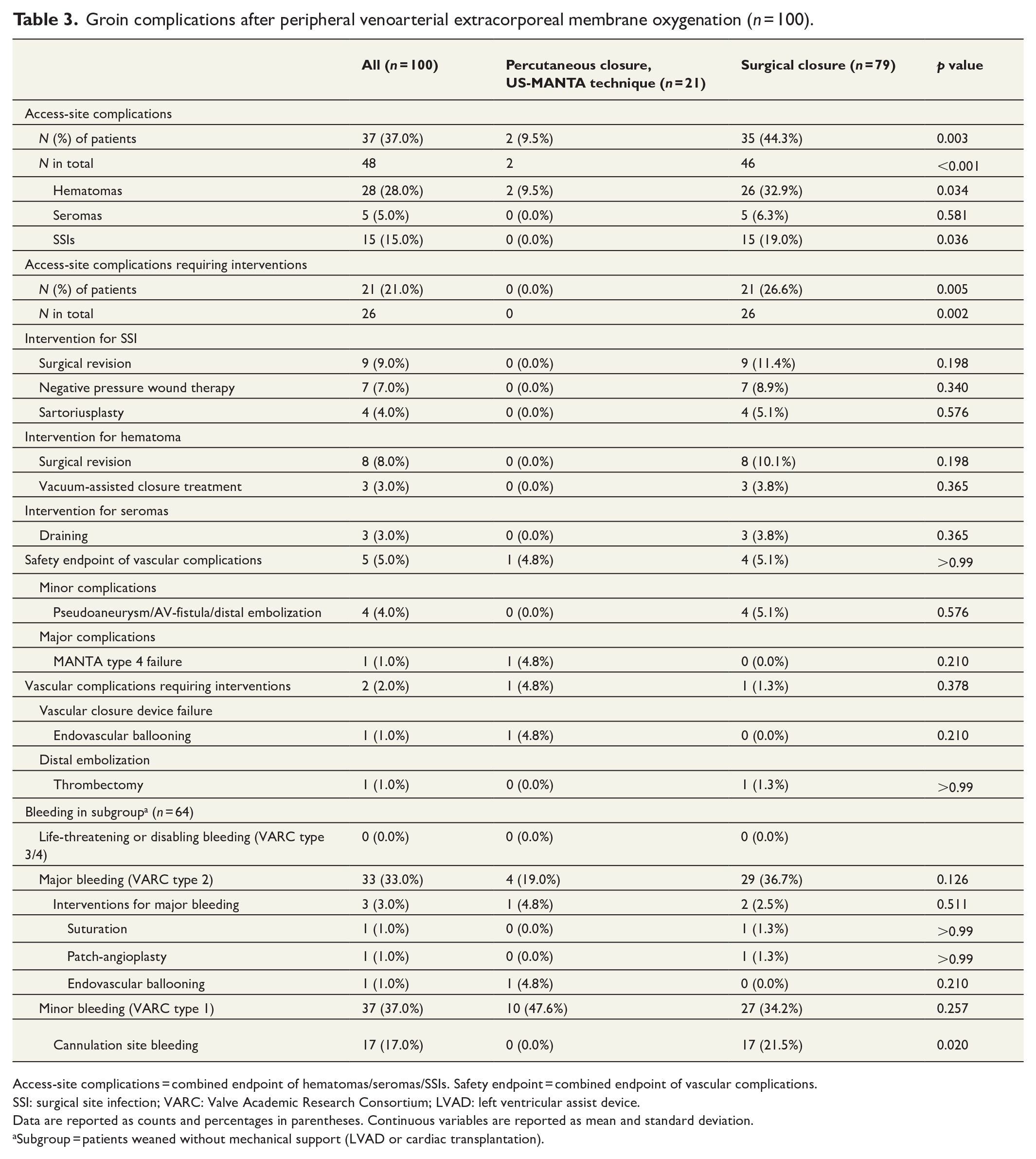
Access-site complications = combined endpoint of hematomas/seromas/SSIs. Safety endpoint = combined endpoint of vascular complications.
SSI: surgical site infection; VARC: Valve Academic Research Consortium; LVAD: left ventricular assist device.
Data are reported as counts and percentages in parentheses. Continuous variables are reported as mean and standard deviation.
Subgroup = patients weaned without mechanical support (LVAD or cardiac transplantation).
There was no significant difference in RBC (p = 0.239) or thrombocyte transfusions (p = 0.227) between study groups in the subgroup analysis. Similarly, there was no significant difference in periprocedural hemoglobin drop (ΔHb) between the surgical group and percutaneous group (p = 0.249) (Supplementary Table 4). Minor bleeding, predominantly clinically significant cannulation site bleeding after weaning, was detected only in the surgical group. The intergroup difference was statistically significant (21.5% versus 0.0%; p = 0.02) (Table 3).
Access-site complications
In multivariate analysis, when categorizing hematomas, seromas, and surgical site infections (SSIs) to a composite endpoint, surgical decannulation was independently associated with risk of hematoma/seroma/SSIs, compared to percutaneous ultrasound-guided MANTA closure (OR: 7.162, 95% CI: 1.544–33.222; p = 0.012) (Supplementary Table 3).
In the US-MANTA group, no hematomas necessitated surgical intervention. The surgical group had five (19.2%) hematomas requiring surgical revision only, and another three patients (11.5%) required surgical revision and vacuum-assisted closure (VAC) (Supplementary Table 1). Seromas were observed only in the surgical group, and 3/5 were drained (60%) (Table 3 and Supplementary Table 1). SSIs requiring intervention in addition to antibiotic treatment occurred only in surgical group patients, of which 9/15 (60%) required surgical revision, 7/15 (47%) VAC therapy, and 4/15 (27%) additional sartoriusplasty to cover femoral vessels (Supplementary Table 2).
Discussion
According to our study, percutaneous ultrasound-guided MANTA closure of femoral arteriotomy compared to surgical closure during ECMO decannulation is (1) safe in terms of bleeding and VCs, (2) feasible (technical success rate 95.2%), and (3) results in significantly less hematomas/seromas/SSIs necessitating intervention.
Ultrasound-guided MANTA deployment became the mainstay closure technique after becoming available at our institution in 2019; previously, patients were surgically decannulated only. All the percutaneous decannulations in this series were executed with ultrasound assistance. As our previous studies have shown, the role of ultrasound in MANTA deployment is of crucial importance,2,4 especially in verifying the sandwiching of the toggle/anchor and the collagen plug around the anterior vessel wall. X-ray fluoroscopy was never needed. There were no changes in protocols such as the compression technique or transfusion threshold during the study period (2012–2020).
We have surgeons on call that are not familiar with the US-MANTA technique, and in those instances that decannulation had to be performed out of hours without anybody having knowledge of MANTA VCD, surgical exposure of the arterial cannulation site and purse-string suture were used. During this study’s time period, three cardiothoracic surgeons used MANTA closure, and the previous experience of MANTA users is estimated to be at least 50 applications per surgeon. Also, different preferences of surgeons affected the decannulation method.
Decannulation of peripheral VA-ECMO is typically accomplished through surgical closure or by manual and device compression (Femostop™ Gold, Abbott Vascular, Santa Clara, CA, USA). Compared to surgical cannulation and decannulation, the former technique is invasive and time-consuming, whereas the latter technique had more VCs and persistent bleeding. 5
In previous studies using MANTA in transcatheter aortic valve implantation (TAVI), ultrasound-guided MANTA closure of femoral arteriotomy results in significantly fewer major VCs than MANTA without ultrasonography.2,4 Thus, ultrasound-guided MANTA for VA-ECMO decannulation was employed as well, and a case report was published recently. 6 Since, several case series employing MANTA for ECMO decannulation have been published7,8 and two comparative studies: one with MANTA versus surgical technique 9 and one with MANTA versus ProGlide (Abbott Vascular, Santa Clara, CA, USA). 10
Au et al. 10 have demonstrated that the use of MANTA is feasible and results in less blood loss compared to ProGlide during ECMO decannulation. Their 100% success rate utilizing MANTA is concordant with ours 95.2%. In comparison, the ProGlide device’s technical success has been reported to be 84.0%–95.8%.10 –13 The single VCD failure in our study was likely caused by weakened vessels due to prolonged ECMO duration and indwelling of cannulas (25 days). Angio-Seal used for limb perfusion arteriotomy closure in the superficial femoral artery failed similarly (type 4 VCD failure), 2 supporting the theory. Therefore, we recommend not applying ultrasound-guided MANTA, or application carefully considered if ECMO duration exceeds several weeks. Femoral cut-down and thrombectomy, for long indwelled cannulas, are justified given the propensity for the femoral artery portion (dead space) between the arterial and limb perfusion cannulas to thrombose, if ECMO run is prolonged. 11
We did not observe any bleeding tendency after percutaneous ultrasound-guided MANTA closure. According to Hwang et al., 12 employing the suture based ProGlide for percutaneous decannulation, a higher bleeding tendency apparently contributed to lower hemoglobin in surgically decannulated patients after weaning than in percutaneously decannulated patients. There are however contradictory findings using ProGlide—Danial et al. 5 reported increased site VCs and persistent bleeding requiring surgical revision in the percutaneous group after VA-ECMO decannulation. In our center, anticoagulants and antiplatelets are discontinued during ECMO therapy initiation with heparinization. Hence, preoperative medication differences, determined primarily by underlying diseases, would not considerably affect bleeding at the time when the patient is mature for weaning and decannulation. Our center’s first-line anticoagulant is low-dose heparin during ECMO therapy and coagulation is monitored by activated clotting time (goal 160–180 s). Heparin infusion is ceased 1 h before decannulation if weaning is anticipated.
In our previous study, comparing the US-MANTA technique to MANTA deployment without ultrasound, ultrasound assistance was shown to be the sole independent predictor of lower rates of MANTA-related major VCs. 2 We found 4.8% VCs in our US-MANTA study group. Several observational studies9,14 –16 and two randomized controlled trials17,18 (RCTs) investigating outcomes of percutaneous decannulation with conventional MANTA deployment without systematic ultrasound guidance report higher rates of VCs: Pingpoh et al., 9 comparing surgical and percutaneous MANTA closure, observed 13% VCs in their percutaneous MANTA group, and the corresponding rates in MANTA study groups in other reports comparing plug-based MANTA VCD and suture-based ProGlide ranged from 8% to 10.7%.14 –17 The multicenter CHOICE-CLOSURE RCT comparing MANTA and ProGlide 18 observed 19.4% access site VCs in MANTA patients. They utilized ultrasound in only 18.2% of decannulations. In our opinion, ultrasound assistance during decannulation may be associated with lower VCs, but our different results from the reports by Pingpoh et al. 9 and the CHOICE-CLOSURE RCT 18 may also be explained by the higher prevalence of peripheral arterial disease, an established risk factor predisposing to MANTA-related VCs, in their patient cohort.
We believe that ultrasound should also be used during ECMO cannulation since a puncture too distal from femoral artery bifurcation can cause vessel stenosis during MANTA closure, and a paramedian puncture failure of achieving hemostasis.8,19 Moccetti et al. 20 reported comparable results in a 100-patient cohort receiving TAVI or Impella-CP cardiac mechanical support: reduced MANTA-related vascular and bleeding complications with ultrasound assistance. However, learning curve utilizing ultrasound-guided endovascular devices must be considered.
Study limitations
This study has the limitation of being retrospective and observational. Second, the lack of randomization and follow-up data after hospital discharge leaves this study susceptible to patient and decannulation method selection bias. Third, our study was a small single-center study with only 21 patients undergoing percutaneous ultrasound-guided MANTA closure. Finally, limited patient numbers prevented matched comparative analyses.
Conclusion
We report that percutaneous ultrasound-guided MANTA closure of the femoral artery is safe and feasible after peripheral venoarterial ECMO decannulation provided that ECMO duration is reasonable. Access-site complications (hematomas/seromas/SSIs) are significantly fewer after utilizing percutaneous MANTA closure device after ECMO decannulation compared to surgical decannulation.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231181232 – Supplemental material for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device
Supplemental material, sj-docx-1-sjs-10.1177_14574969231181232 for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device by Tasnia Rahman, Johanna Herajärvi, Henri Ahonen, Mikko Jormalainen, Simo Syrjälä, Tommi Järvinen, Tatu Juvonen and Sebastian Dahlbacka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969231181232 – Supplemental material for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device
Supplemental material, sj-docx-2-sjs-10.1177_14574969231181232 for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device by Tasnia Rahman, Johanna Herajärvi, Henri Ahonen, Mikko Jormalainen, Simo Syrjälä, Tommi Järvinen, Tatu Juvonen and Sebastian Dahlbacka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969231181232 – Supplemental material for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device
Supplemental material, sj-docx-3-sjs-10.1177_14574969231181232 for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device by Tasnia Rahman, Johanna Herajärvi, Henri Ahonen, Mikko Jormalainen, Simo Syrjälä, Tommi Järvinen, Tatu Juvonen and Sebastian Dahlbacka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-4-sjs-10.1177_14574969231181232 – Supplemental material for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device
Supplemental material, sj-docx-4-sjs-10.1177_14574969231181232 for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device by Tasnia Rahman, Johanna Herajärvi, Henri Ahonen, Mikko Jormalainen, Simo Syrjälä, Tommi Järvinen, Tatu Juvonen and Sebastian Dahlbacka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-5-sjs-10.1177_14574969231181232 – Supplemental material for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device
Supplemental material, sj-docx-5-sjs-10.1177_14574969231181232 for Ultrasound-guided closure of the femoral artery during venoarterial decannulation using a large-bore closure device by Tasnia Rahman, Johanna Herajärvi, Henri Ahonen, Mikko Jormalainen, Simo Syrjälä, Tommi Järvinen, Tatu Juvonen and Sebastian Dahlbacka in Scandinavian Journal of Surgery
Footnotes
Author contributions
S.D. contributed to concept and design.
H.A., S.S., and T.R. contributed to data collection.
S.D., J.H., and T.R. contributed to writing the article.
S.D., J.H., H.A., T.J., M.J., and S.S. gave critical revision to the article.
S.D., J.H., H.A., T.J., M.J., S.S., T.J., and T.R. gave final approval to the article.
T.R. and T.J. were responsible for statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to publication
The Institutional Review Board approved conduction of this study and waived informed patient consent requirements.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.