
Abstract
Weaning and liberation from V-A ECMO for cardiogenic shock involves complex decision-making that requires balancing multiple clinical parameters. In the absence of specific weaning guidelines, ECMO centers rely on heterogeneous, institution-specific practices, which may adversely affect outcome. To gain insights into how professionals weigh multiple factors in complex weaning decisions, a survey was designed using conjoint analysis. The survey was presented to a large cohort of international ECMO clinicians via the EuroELSO network online between February 16, 2024 and May 1, 2024. Using conjoint analysis, a set of 14 hypothetical adult weaning scenarios, incorporating combinations of different attributes with varying levels across 4 cardiogenic shock etiologies was presented. Participants had to decide on liberation from ECMO (‘yes’ or ‘no’) based on a personal trade-off weighing all presented attributes for each scenario. In total, 316 participants from 49 different countries evaluated 4424 hypothetical scenarios. Pulse Pressure ≥30 mmHg (OR 2.56 (CI 2.03–3.24), cardiac index >2.1 L/min/m² (OR 2.5 (CI 1.87–3.43) and echocardiographically assessed left ventricular outflow velocity time integral (VTI) >15 cm (OR 2.53 (95% CI 201-3.2) all favored positive weaning decisions (all p < 0.001). Vasoactive-inotropic score (VIS; 11.1%), VTI (9.7%) and the presence of peripheral and/or pulmonary edema (9.8%) had the highest relative importance to overall weaning decisions. Echocardiography was found to contribute more to weaning decisions in ECMO novices. Weaning decisions were predominantly driven by parameters reflecting cardiac recovery. Leveraging these insights may set the stage for a clinical decision-support tool to benchmark individual practice against expert consensus.
Keywords
Introduction
Veno-arterial extracorporeal membrane oxygenation (V-A ECMO) is increasingly applied in severe cardiogenic shock, enabling rapid stabilization and serving as bridge to recovery, long-term support, or heart transplantation. Although highly effective in restoring systemic perfusion, the cumulative risk of ECMO-related complications can adversely impact on subsequent therapies and overall outcome.1,2 From initiation, V-A ECMO management should prioritize individual needs towards minimally required mechanical circulatory support and timely weaning.
In current literature, varying weaning strategies propose a wealth of clinical, hemodynamic, echocardiographic and biochemical predictors for successful discontinuation of V-A ECMO.3–7 However, mortality rates of up to 70% after initially successful weaning, often referred to as the ECMO gap, underscore the difficulty of reliably predicting long-term outcome.8,9 Although prediction models such as SAVE, PREDICT VA ECMO, and ENCOURAGE10–12 assess mortality risk at ECMO initiation, their static nature cannot inform cardiac recovery and weaning readiness during ECMO support. 13 In clinical practice, weaning strategies should adhere to a structured approach, including gradual ECMO tapering and liberation.8,14 However, the lack of robust scientific evidence and detailed international guidelines has led to considerable variability in weaning practices. 15 Given the complexity of weaning decisions, shaped by clinical expertise and contextual factors, understanding how clinicians weigh multiple variables is essential for the future development of more robust and standardized weaning protocols.
To address these aspects, an international digital survey using a rating-based conjoint analysis was conducted to capture expert perspectives on weaning decisions by assessing preferences across scenarios containing multiple clinically relevant variables.
Methods
Conjoint analysis study design
This study used a clinical vignette–based rating conjoint analysis to reflect real-world weaning decision-making by incorporating dynamic clinical V-A ECMO parameters. This design was chosen to disentangle the complex trade-offs among multiple clinical and echocardiographic parameters regarding the likelihood of successful weaning.
Identification of attributes for the conjoint analysis
To represent a set of practical V-A ECMO weaning scenarios based on clinical patient profiles, the most relevant attributes influencing weaning decisions were identified. This was done by a combination of focus group interviews with ECMO specialists and a review of currently available literature14,15. A total of 14 non-overlapping ‘key attributes’ were identified as most relevant to weaning decisions. 16 A descriptive system was designed consisting of 14 attributes with 2 to 4 levels each, detailing the range of possible outcomes for that attribute. This resulted in 4*22*311 = 2,834,352 possible scenarios. Before generating the experimental design, several constraints were specified to preclude impossible or unrealistic combinations of attribute levels, e.g., a cardiac index of <1.5 L/min/m2 with an echocardiographic assessed left ventricular outflow velocity time integral (VTI) of >15 cm. Because it was impossible to elicit responses for all possible scenarios, a fractional factorial design was created to test for main effect. This consisted of 28 scenarios, of which 14 were drawn randomly for every respondent. Respondents were asked to indicate their decision after evaluating hypothetical weaning scenarios composed of multiple clinical and echocardiographic parameters. The scenarios followed an experimental design in which levels of all attributes systematically varied over the scenarios. 17 The purpose was to explore how different attribute-levels influence professionals in the final decision regarding potential liberation from V-A ECMO.
Clinical attributes and hemodynamic and echocardiographic attributes evaluated during a weaning trial (decreasing ECMO flow below 1 L/min).
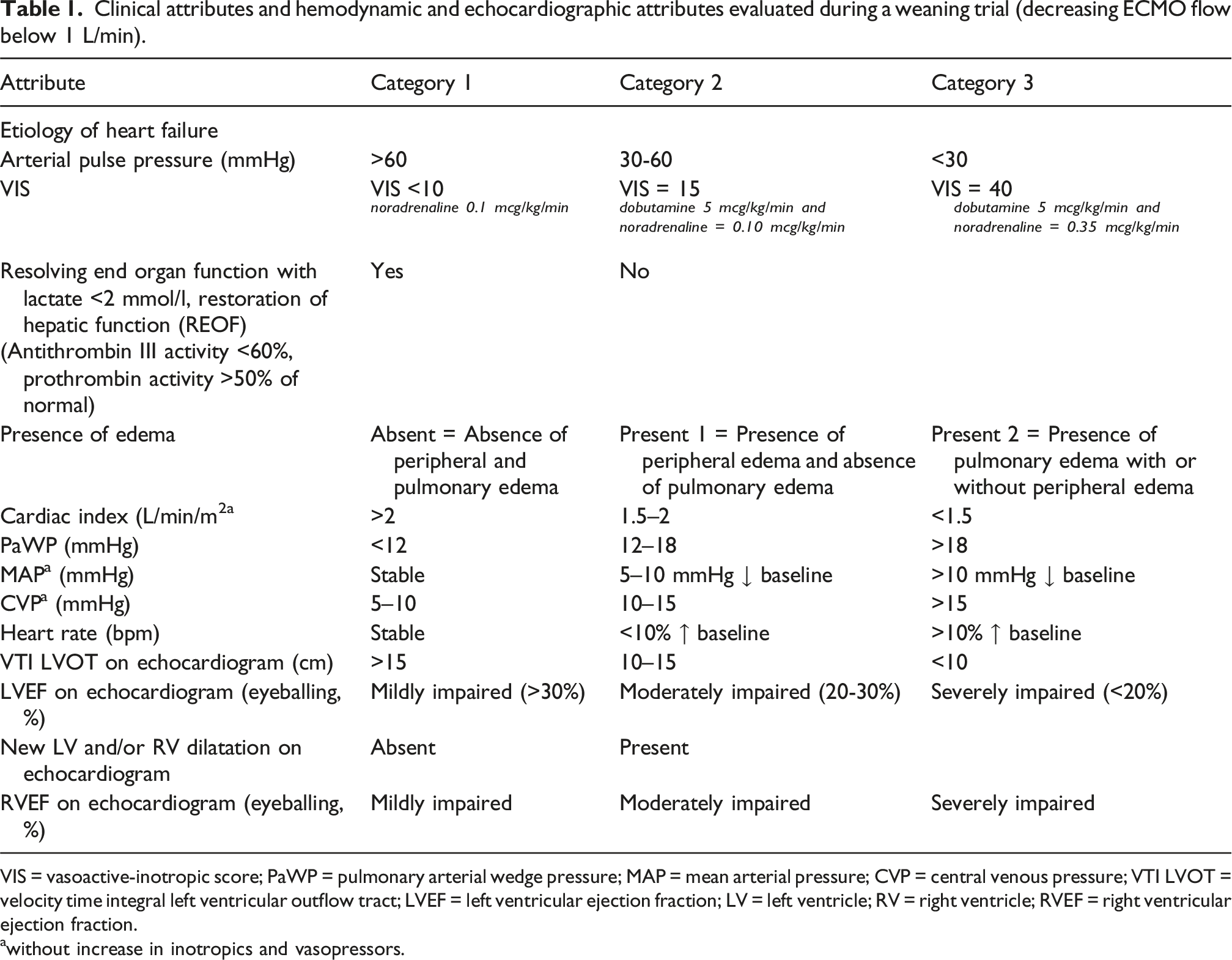
VIS = vasoactive-inotropic score; PaWP = pulmonary arterial wedge pressure; MAP = mean arterial pressure; CVP = central venous pressure; VTI LVOT = velocity time integral left ventricular outflow tract; LVEF = left ventricular ejection fraction; LV = left ventricle; RV = right ventricle; RVEF = right ventricular ejection fraction.
awithout increase in inotropics and vasopressors.
Study population and recruitment
The survey was approved by the Steering and Scientific Committees of the European branch of Extracorporeal Life Support Organization (EuroELSO) and distributed prospectively via the EuroELSO network, including 552 adult cardiac ECMO centers worldwide. Subscribers to the EuroELSO newsletter were sent a personal link to complete the survey via email. Additionally, the survey link was distributed via the EuroELSO social media channels. Follow-up reminder e-mails were sent biweekly. Ethical approval for the project was considered not mandatory as the study was a social science survey which did not contain personal data (completely anonymous survey) and no financial incentive was received. All responses were reviewed to exclude duplicates. The survey was built using the survey software Qualtrics (Seattle, Washington, US) and was online available from February 16, 2024 until May 1, 2024 (supplement A). All participants were subdivided in an ‘expert group’ (>5 years of experience with V-A ECMO, working in a tertiary center specialized in advanced heart failure care, exposure of >25 cases per center annually) and a less experienced and specialized ‘novice group’.
Data analysis
All data were processed anonymously using R (R Foundation for Statistical Computer, Vienna, Austria©). A mixed-effects logistic regression model was applied to estimate the association between attribute levels (independent variables) and the weaning advice (binary outcome: “yes” vs “no”) provided by ECMO experts (dependent variable). The model included a random intercept for each individual respondent to account for clustering within experts. All categorical variables were converted to factors, with clinically relevant reference levels defined for each. These reference levels represented the most favourable clinical conditions. For each attribute level, we calculated odds ratios (ORs) with 95% confidence intervals (CIs), indicating the likelihood of a positive weaning recommendation compared to the reference category. Odds ratios >1 were interpreted as ‘in favour of weaning’, while ORs <1 indicated ‘not in favour of weaning’.
The resulting ORs and confidence intervals were visualized in a forest plot. Additionally, an analysis of variance (ANOVA) or Chi-square test was conducted to complement the regression analysis by formally assessing the significance of each attribute. The relative importance of attributes was determined using the method proposed by González et al. 18 All data were reported as mean ± standard deviation (SD) where applicable.
Decision support tool
Based on the conjoint analysis and as a proof of concept, we developed a web-based V-A ECMO Weaning Decision Support Tool implemented in R Shiny. The tool provides preference-based guidance derived from the clinicians’ responses. For a user-specified combination of the 14 attributes, the application maps each chosen attribute level to the corresponding regression term and applies the fitted logistic regression coefficients (intercept + attribute-level estimates) to compute the modelled probability of a weaning recommendation. The output is reported as a probability (%) and a binary recommendation (“wean” vs “do not wean”) using a 0.5 threshold.
Results
In total, 17.875 surveys were distributed through the EuroELSO network. Responses were received from 664 ECMO experts across 49 countries, with 316 participants completing the survey (completion rate of 47.6%). The database comprised clinicians with various experience levels and background including consultants in cardiology and heart failure, cardiothoracic surgery, cardiac anesthesiology, intensivists and perfusionists. Analyses included only fully complete responses. Among participants, 79% were male and 63% were working in a tertiary center specialized in advanced heart failure care. Of all participants, 52% had a mean professional experience in clinical care for V-A ECMO supported patients of >10 years.
Baseline characteristics of participants and characteristics involving care for VA ECMO patients.
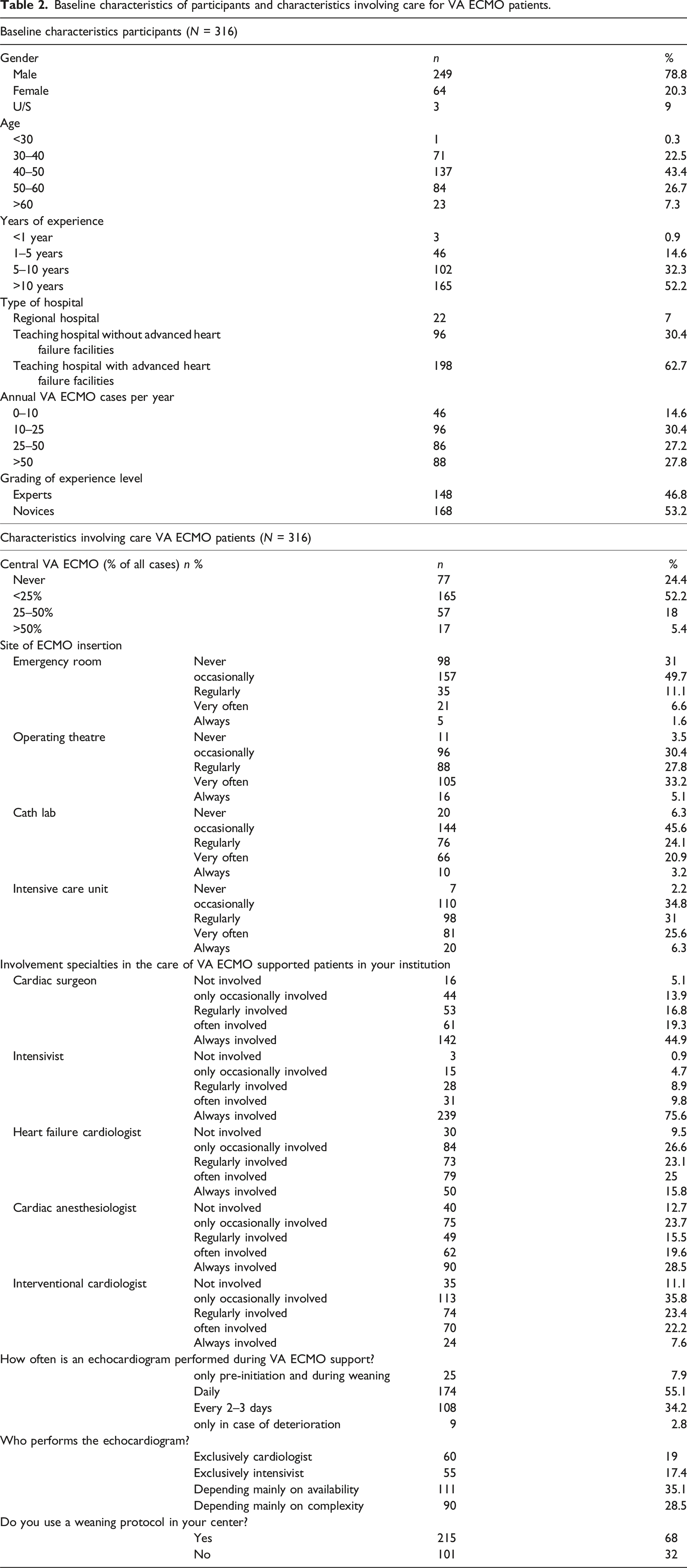
Figure 1 presents the main results of the logistic regression analysis in the overall respondent group presented in an odds plot (Odds ratio (OR) and confidence intervals (CI). Of the 14 attributes, only pulmonary artery wedge pressure did not significantly influence weaning preferences. In terms of etiology, respondents were significantly more likely to favor weaning in ‘myocarditis’ and significantly less likely to favor weaning ‘post-cardiotomy’ compared to ‘anterior wall infarction’. The likelihood of weaning was similar in ‘acute heart failure’ and ‘anterior wall infarction’. A VTI >15 cm and cardiac index >2.1 L/min/m2 were attributes that increased the likelihood of a positive decision to wean a patient from V-A ECMO (all p < 0.001; Figure 1). Unresolved organ failure, a pulse pressure (PP) < 30 mmHg or > 60 mmHg, the presence of pulmonary edema with or without peripheral edema, severely impaired left ventricular (LV) and right ventricular (RV) function, a CVD >15 mmHg and high (>15) vasoactive-inotropic score (VIS) all increased the likelihood of a negative decision to wean a patient from V-A ECMO (all p < 0.05; Figure 1). Also, both an increase or decrease of more than 10% in heart rate (HR) or the presence of LV/RV dilation during the weaning trial were found more often to be associated with a negative decision for ECMO weaning (all p < 0.001). The contribution of each attribute in the decision to liberate a patient from VA ECMO is shown in Figure 2. VIS (11.1%), resolution of organ failure (REOF: 10.1%), VTI (9.7%) and the presence of peripheral and/or pulmonary edema (9.8%) were found to have the highest relative importance in weaning decisions. Logistic regression analysis overall respondent group presented in an odds plot. Represents the likelihood (Odds ratio (OR) and confidence intervals (CI) of a positive or a negative decision to wean a patient from VA ECMO based on parameters during a weaning trial ECMO. Factors determining the decision to weaning from ECMO. Represents the contribution of each attribute in the decision to liberate a patient from VA ECMO.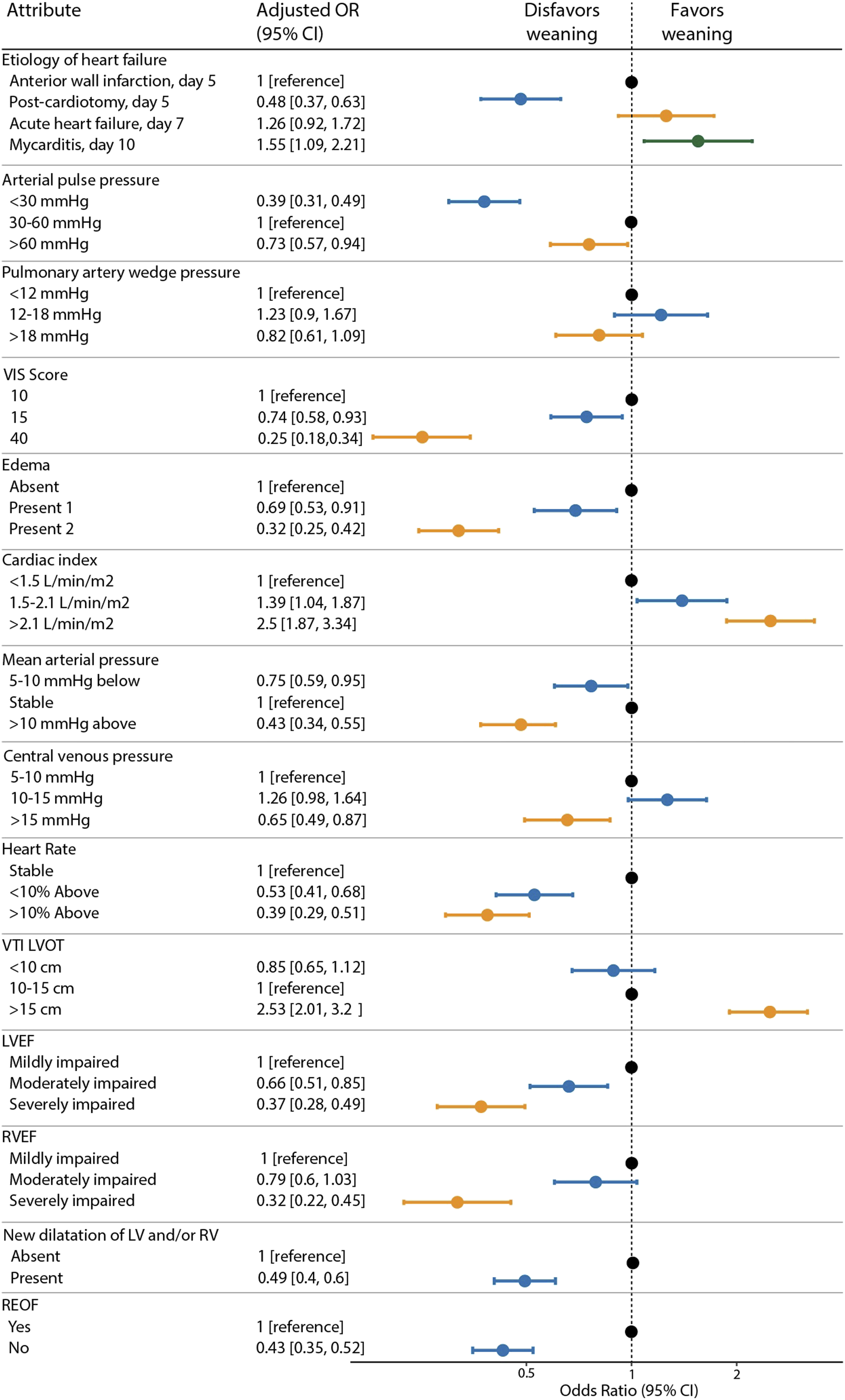
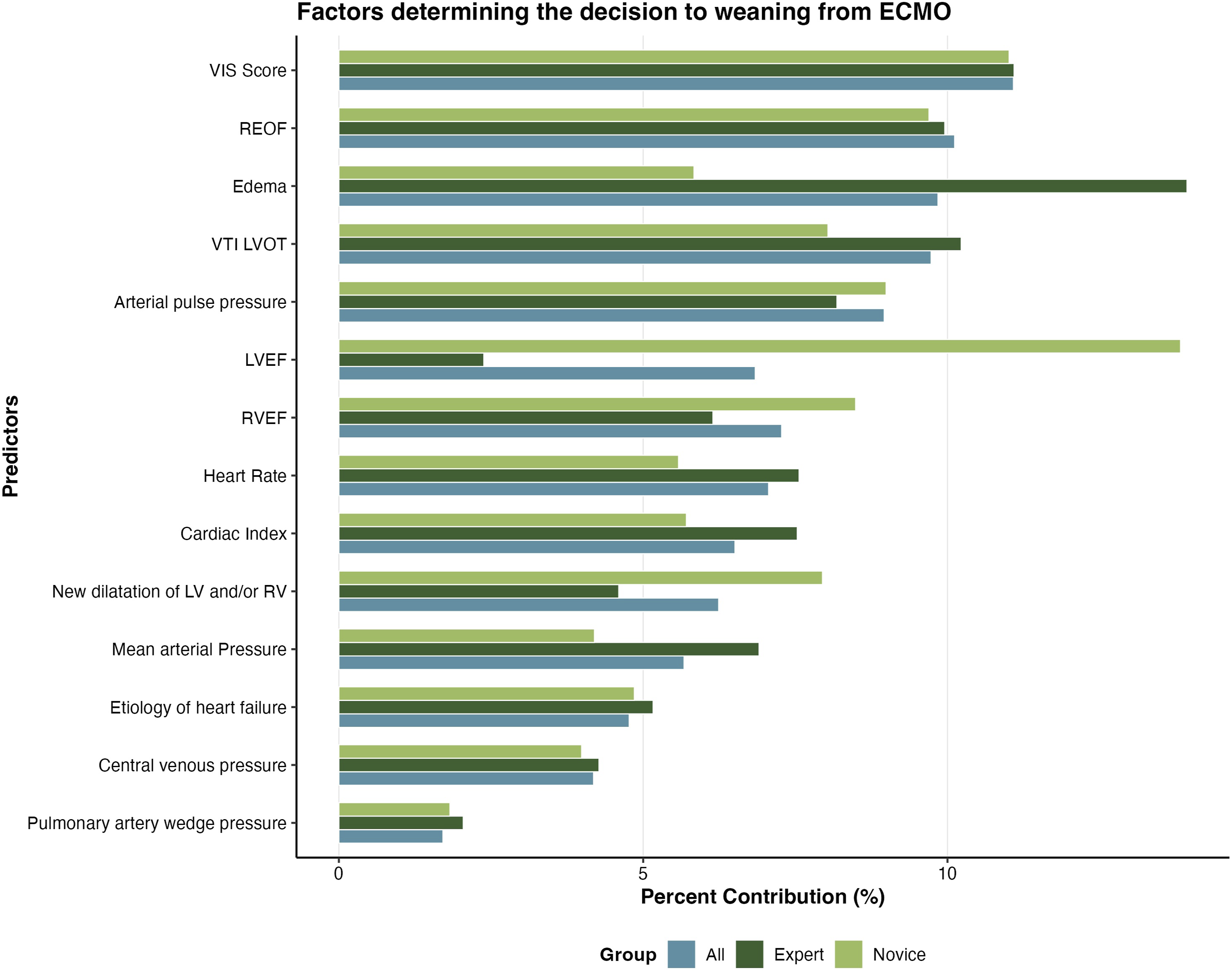
A Chi-squared test (χ2 = 0, df = 27, p = 1) confirmed that clinical cases were evenly distributed between expert and novice groups, indicating no bias in case assignment. All above-described results from the logistic regression analysis were equally observed in both groups, however echocardiographic parameters (LV and RV ejection fraction) were found to contribute for a larger part in weaning decisions in the novice group (13.8%/8.5% vs 2.4%/6.1% in the expert group Figure 2. The presence of peripheral and/or pulmonary edema (9.8%) was found to have the highest relative importance in weaning decisions in the expert group. The proportion of “yes” responses to weaning was similar between experts (34.5%) and novices (35.9%). Likewise, the mean confidence scores (on a scale from 1 (very certain) to 4 (very uncertain)) were identical: 1.79 for experts and 1.79 for novices. No statistically significant differences were found between the groups in either weaning decisions (p = 0.99) or confidence levels (p = 0.99).
The fitted conjoint model was translated into an interactive decision support application. The tool is publicly accessible as a proof-of-concept demonstration at https://medicaldigitaltwin.shinyapps.io/ecmoweanadvise. (Figure 3). Proof-of-concept clinical decision tool.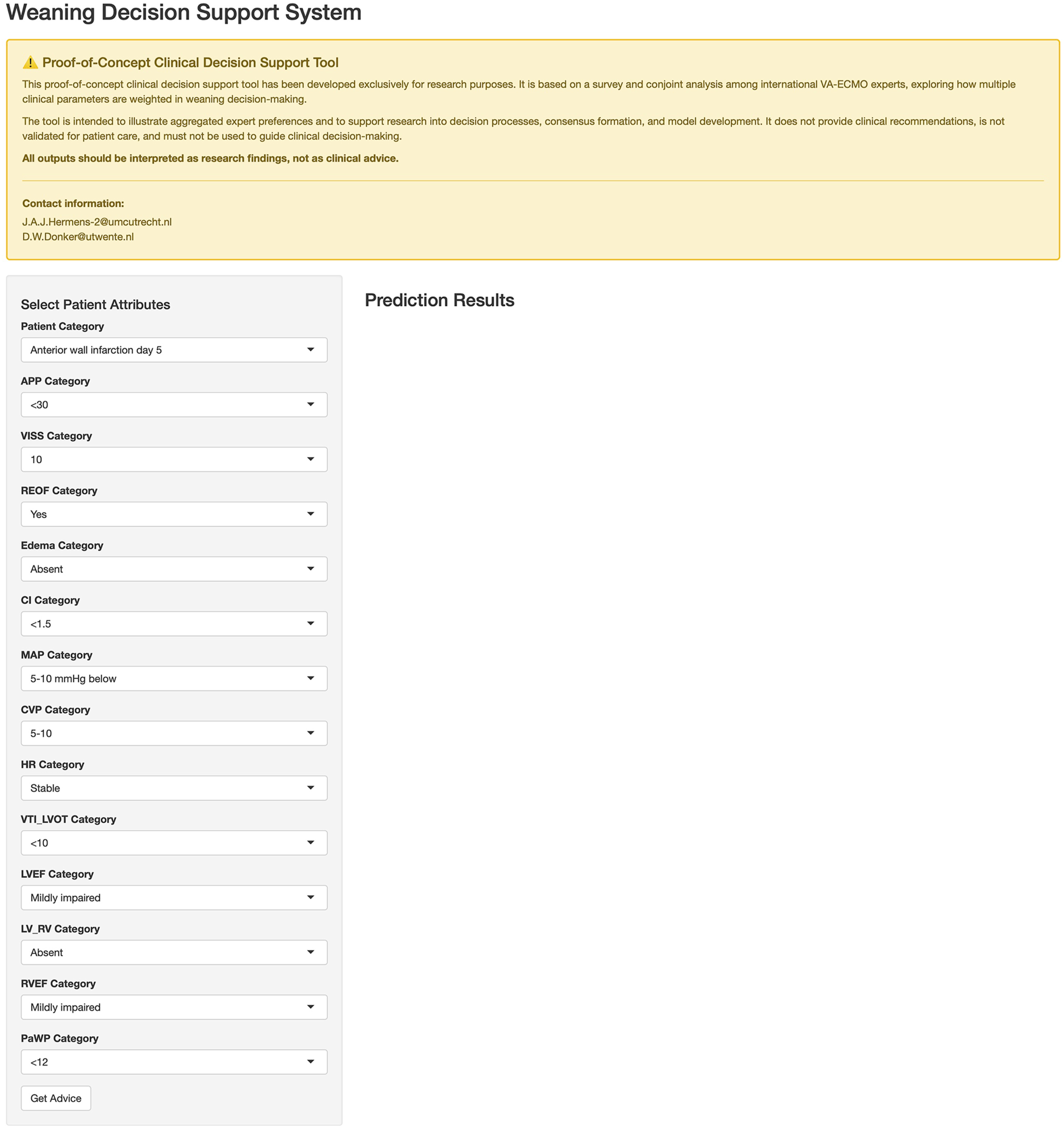
Discussion
Decisions surrounding V-A ECMO weaning represent one of the most complex challenges in critical care, requiring careful assessment of myocardial recovery in the context of dynamic physiological conditions. By engaging a broad cohort of international ECMO experts, a conjoint analysis comprising 14 hypothetical cases revealed that predominantly parameters representing cardiac recovery shaped these decisions.
Indicators of cardiac recovery are key determinants in guiding weaning decisions
Quantitative measures of improving cardiac performance, notably PP, CI and VTI, all emerged as indicators of weaning readiness favoured by clinicians. It underscores that clinicians consistently identify “clinical evidence of cardiac recovery” as the main prerequisite for weaning and liberation from V-A ECMO, which is consistent with previous findings.3–5,14,19 This result aligns with established physiological principles given that native cardiac function must guarantee adequate systemic perfusion once mechanical support is withdrawn. PP values >30 mmHg were highly appreciated within the context of positive weaning decisions, reflecting the high clinical value of this readily available bedside parameter. Derived from continuous arterial pressure monitoring, PP captures the dynamic interaction between the recovering native heart and the ECMO circuit through ventriculo-arterial and ECMO-arterial coupling. The resulting pulsatility likely reflects the combined influence of contractility of the recovering heart, aortic compliance, peripheral resistance, and ECMO blood flow. 20 At the bedside, arterial PP may serve in this sense as a practical surrogate of the patient's own cardiac function which has previously been found to correlate with positive weaning outcome in V-A ECMO supported cardiac arrest patients.19,21 Although guidelines recommend a minimal PP of 10 mmHg to ensure adequate LV ejection and transpulmonary flow, no specific threshold reliably defines cardiac recovery. 22 It is plausible however that an increase in PP over time during ECMO support is indicative of a greater stroke volume and improving myocardial contractility. For this reason, respondents may appreciate this parameter as a meaningful surrogate marker of recovering cardiac pump function. 23 However, ECMO flow, intravascular volume status, and the use of vasoactive agents all influence the pressure waveform. Therefore, its precise clinical significance within this context requires further investigation. 20
A stable or rising cardiac index (>2.1 L·min/m2) during flow reduction was also strongly associated with perceived weaning readiness and highly valued by clinicians. While continuously measured via pulmonary artery catheterization, cardiac index shows good agreement with echocardiographic estimates and provides an objective, real-time reflection of the native heart’s contribution to systemic output, with increases indicating improving LV recovery during V-A ECMO support.24,25 Although no definitive thresholds exist and its interpretation must account for dynamic loading conditions and vasoactive therapy, its use is broadly recommended during support.22,26,27 For these reasons, cardiac index emerged as a highly valued continuous and objective measure of cardiac performance complementing intermittent echocardiographic assessment, while VTI, as a Doppler-derived surrogate for stroke volume, was also highly valued in weaning decisions by our respondents. Clinicians likely valued VTI because it can be obtained rapidly at the bedside, even with limited echocardiographic expertise, and provides direct insight into recovery of intrinsic cardiac function. VTI values >10 cm at minimal ECMO flow have been associated with successful liberation from support, reinforcing its clinical relevance.3,8,22 Although interpretation may be challenging in the presence of variable ECMO flows or ventricular unloading devices, VTI is recommended in ECMO monitoring and weaning guidelines and is now widely adopted in clinical practice.22,28 By complementing continuously available parameters such as PP and cardiac index, VTI meaningfully enhances the assessment of myocardial recovery. Beyond these quantitative indicators of cardiac recovery, many clinicians also highly valued qualitative echocardiographic “eyeballing” of LV and RV function when deciding on VA ECMO weaning. Originating from early postcardiotomy practice, this subjective approach still remains widely used in clinical decision-making despite its lack of formal objectivity.4,29
Altogether, these findings underscore the need of the responding clinicians to integrate both quantitative, modern parameters like VTI and semi-quantitative, traditional parameters like “eyeballing” LV ejection fraction, cardiac index and PP. Obviously, this combined assessment provides a multidimensional view on cardiac recovery, forming a more robust basis for estimating weaning readiness at the bedside. This insight led to further exploration of whether the level of clinical experience influences preferences for specific weaning parameters.
Variation in weaning preferences between novices and experts
While novices and experts in general prioritized similar weaning attributes, novices valued echocardiography more and experts mainly emphasized clinical parameters. Although confidence levels did not differ significantly between the groups, experts appear to assess weaning readiness within a broader clinical context, whereas novices appear to adhere more to objective imaging parameters. These findings could suggest that, with increasing experience, clinicians appear to shift from analytical reasoning toward a more intuitive, holistic approach, with novices focusing on physiological details and experts on the broader clinical context.30–32 These findings suggest that variability in weaning practices may reflect not only institutional routines and logistical factors, but also differences in individual experience, preferences, and technical expertise. They also indicate that a multidisciplinary team with mixed experience levels may be beneficial, as novices and experts can offer complementary perspectives in complex weaning decisions. 33
Practical implications and the role of decision support tools in daily weaning practice
The in-depth insights into weaning decisions gathered in this study served as a proof-of-concept development of a decision support tool that could potentially provide clinicians with patient-specific, expert-informed recommendations for ECMO withdrawal. In clinical practice, where weaning decisions are shaped by experience, logistics, ethics, and uncertainty, decision-support tools may enhance confidence when guidelines are lacking. Over the past few years, several ICU decision-support systems, including ventilator-integrated weaning tools using real-time physiological data, have been developed. 34 Although still preliminary, they show potential to reduce practice variation, ventilation duration, and ICU length of stay.35–37 Whereas the application of comparable systems to ECMO weaning is not yet established, clinical decision-support tools have the potential to promote greater uniformity in the weaning process. Ultimately, the extensive availability of continuous hemodynamic data during ECMO support may foster the future development of multifaceted models which are capable of predicting weaning outcomes and identifying the optimal timing for liberation from support 38
Limitations and future perspectives
These study results should be interpreted with some caution. Weaning decisions were derived from hypothetical scenarios that may not fully reflect the complexity, time pressure, and contextual factors of real-world clinical decision-making. The analysis reflects stated clinician preferences rather than patient outcomes, limiting causal inference and assuming independence between physiologically interrelated attributes. Further, a challenge not addressed in this study is the increase in use of concomitant unloading LV devices, e.g., Impella, intra-aortic balloon pump, or surgical vent. By altering native cardiac loading conditions, these devices may obscure true myocardial recovery, confound interpretation of weaning parameters such as PP and VTI, and complicate decisions regarding the sequence of device removal. Although the added value of unloading devices during V-A ECMO support in general remains under debate, future studies and protocols should acknowledge and address the complexity of weaning in these scenarios.39,40
Nevertheless, the study provides valuable insight into expert ECMO weaning trade-offs and may serve as a basis for a future clinical decision-support tool. This will require retrospective and prospective validation before clinicians can benchmark decisions against consolidated expert consensus.
Conclusion
This conjoint analysis provides detailed insights into the parameters clinicians value when making complex V-A ECMO weaning decisions. Indicators of cardiac recovery, particularly PP, cardiac index, and VTI, emerged as main appreciated determinants of weaning readiness and highlight the need for integrating hemodynamic and echocardiographic assessments. Differences between novices and experts suggest that also experience shapes the balance between clinical judgment and protocol-driven evaluation. These findings may foster the development of a clinical decision-support tool aiming at improving consistency, confidence, and uniformity in ECMO weaning. Substantial further validation and refinement are needed before any clinical implementation can be envisaged.
Supplemental material
Supplemental material - Guiding complexity in V-A ECMO weaning decisions for cardiogenic shock: Insights from a conjoint analysis
Supplemental material for Guiding complexity in V-A ECMO weaning decisions for cardiogenic shock: Insights from a conjoint analysis by J. A. J. Hermens, J. A. Van Til, L. Van Loon, N. A. Barrett, J. Swol, R. Lorusso, D. Van Dijk, C. L. Meuwese, D. W. Donker in Perfusion
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. A. J. H. Speaker fees from Abbot, paid to the University Medical Center of Utrecht C. L. M. research funding from Charity foundation Stichting Gezondheidszorg Spaarneland and the Dutch Heart Foundation. Speaker fees from Abbot and AOP Health Institutional consultancy in a collaboration with Getinge. D. W. D. is involved in an institutional research cooperation with Maquet Critical Care AB, part of Getinge, Solna, Sweden, and Sonion BV, Hoofddorp, the Netherlands, and research and educational consultancy to HBOX Therapies, Aachen, Germany, and Abiomed, Aachen, Germany. All financial compensation is paid to the University of Twente. D. W. D. does not receive any personal fees.
Supplemental material
Supplemental material for this article is available online.