
Abstract
Background and objective:
Gallbladder cancer (GBC) is a rare malignancy in the Nordic countries and no common Nordic treatment guidelines exist. This study aimed to characterize the current diagnostic and treatment strategies in the Nordic countries and disclose differences in these strategies.
Methods:
This was a survey study with a cross-sectional questionnaire of all 19 university hospitals providing curative-intent surgery for GBC in Sweden, Norway, Denmark, and Finland.
Results:
In all Nordic countries except Sweden, neoadjuvant/downstaging chemotherapy was used in GBC patients. In T1b and T2, majority of the centers (15–18/19) performed extended cholecystectomy. In T3, majority of the centers (13/19) performed cholecystectomy with resection of segments 4b and 5. In T4, majority of the centers (12–14/19) chose palliative/oncological care. The centers in Sweden extended lymphadenectomy beyond the hepatoduodenal ligament, whereas all other Nordic centers usually limited lymphadenectomy to the hepatoduodenal ligament. All Nordic centers except those in Norway used adjuvant chemotherapy routinely for GBC. There were no major differences between the Nordic centers in diagnostics and follow-up.
Conclusions:
The surgical and oncological treatment strategies of GBC vary considerably between the Nordic centers and countries.
Context and Relevance
Gallbladder cancer (GBC) is a rare malignancy and no common Nordic treatment guidelines exist. This survey study aimed to characterize the current diagnostic and treatment strategies in the Nordic countries and disclose differences in these strategies. In all Nordic countries except Sweden (neoadjuvant) and Norway (adjuvant), neoadjuvant/adjuvant chemotherapy was used for GBC. The surgical treatment strategies were similar in T1a, but there was a wide variation regarding T1b-T4 treatments. In Sweden, lymphadenectomy was extended beyond the hepatoduodenal ligament, whereas all other Nordic centers limited lymphadenectomy to the hepatoduodenal ligament. The treatment of GBC varies considerably between the Nordic countries. The results give opportunity to research the effect of different treatment strategies on the outcome of the patients and eventually form common Nordic guidelines for GBC treatment.
Introduction
Gallbladder cancer (GBC) is a relatively rare disease in the Nordic countries with an incidence of 0.39–0.89: 100,000 and only one-fifth of affected patients are candidates for curative-intent surgical resection.1–6 Because of the low incidence, no randomized controlled trials (RCTs) on diagnostic or treatment strategies for GBC exist, except for oncological treatments,7–15 hence most of the guidelines are based on weak evidence. 16 Although all Nordic countries have universal healthcare that are mostly government funded, 17 it is likely that the approaches to GBC vary between countries, and even between centers within the same country. In an effort to study possible effects of different treatment strategies, it is first necessary to map any differences in diagnostic work-up and treatment provided. However, the domains in which these approaches differ the most are currently unknown. The aim of this survey study was to characterize the current diagnostic and treatment strategies in the Nordic countries and disclose differences in these strategies and thus provide basis for common Nordic guidelines for GBC treatment in the future.
Methods
This was a survey study of all 19 Nordic tertiary referral centers, academic centers, and university hospitals providing curative-intent surgery for GBC. The participated centers are shown in Fig. 1. The survey followed the CROSS checklist. 18 The cross-sectional questionnaire included 79 questions about the center’s diagnostics, surgical and oncological treatment strategies, and follow-up for GBC patients (Supplemental material). Most of the questions consisted of prepared answer options, and for some questions, multiple answers were possible. The questions were formulated together with each country’s principal leaders. The questionnaire was pretested once by a multidisciplinary team (MDT) in Helsinki University Hospital and improved accordingly. The answers to the questionnaire were collected by each respective center-leader. The center-leaders were instructed to reflect in the answers the center’s strategy in dealing with GBC, not individual surgeon’s opinions. Centers were instructed to discuss the questions within the team treating GBC patients, preferably in a multidisciplinary manner (surgeon, oncologist, radiologist). Once the questionnaires were filled out, the center-leaders sent them by email or letter to one of the principal investigators who entered the data manually into a common database in a preformatted SPSS sheet (SPSS Statistics Version 24, IBM, Chicago, IL, USA). As a non-web-based survey, the human error was minimized due to the small number of participants. The survey’s time frame was from March 2020 to September 2020. Clarifying questions about the centers’ answers were asked until April 2021 so that there was no missing data. All 19 centers replied to the survey and all answers were representative so there was no need for adjustment. Statistics were mainly descriptive with the aim to identify key features and differences between countries and centers. This survey study was based on virtual scenarios and not real patients, hence there were no need for an ethical procedure, anonymity, or confidentiality.
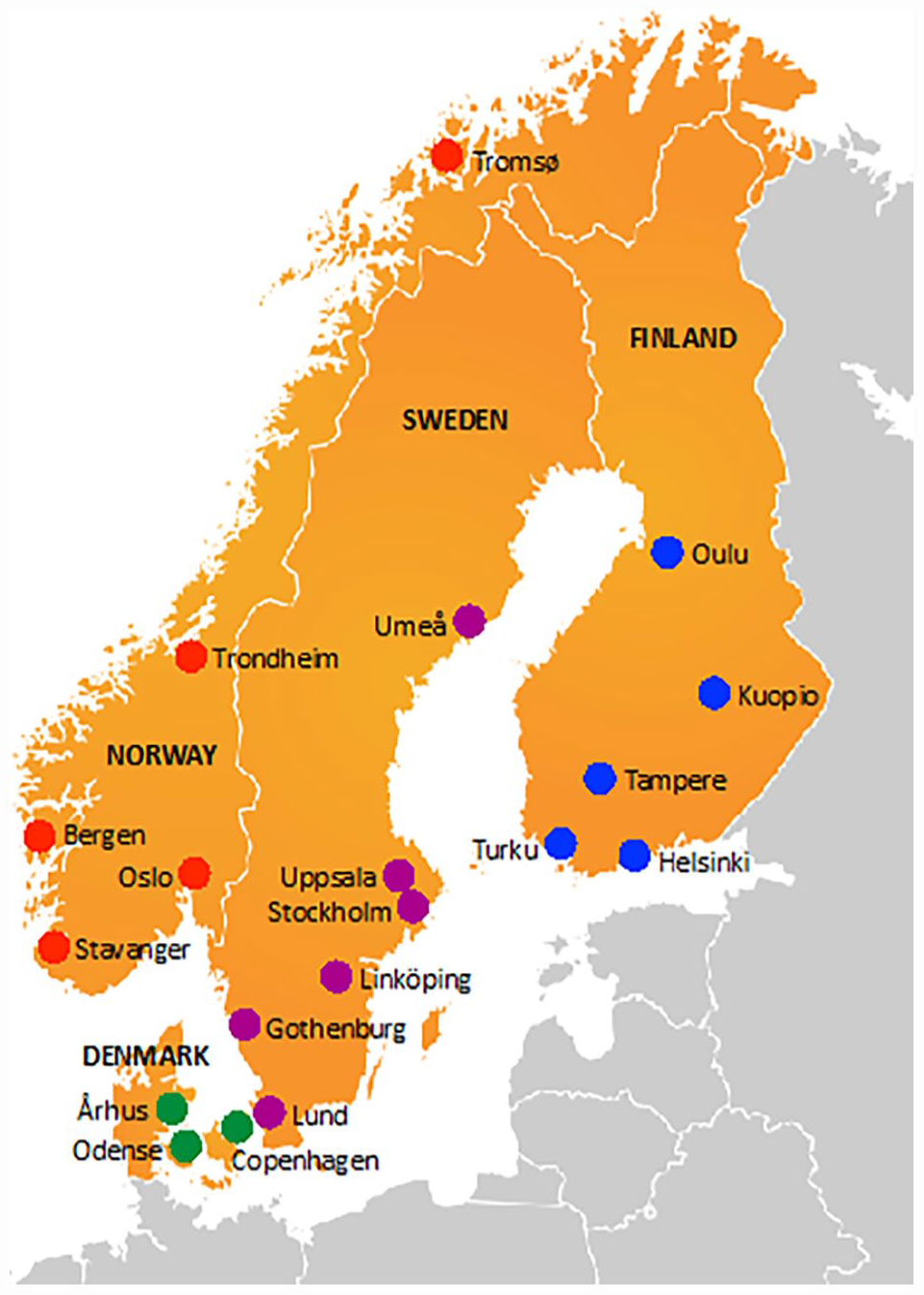
The centers that participated in the survey: Karolinska University Hospital (Stockholm), Sahlgrenska University Hospital (Gothenburg), Linköping University Hospital (Linköping), Skåne University Hospital (Lund), Umeå University Hospital (Umeå) and Uppsala University Hospital (Uppsala) in Sweden (n = 6), Oslo University Hospital (Oslo), Haukeland University Hospital (Bergen), Stavanger University Hospital (Stavanger), University Hospital of North Norway (Tromsø) and St. Olavs Hospital, Trondheim University Hospital (Trondheim) in Norway (n = 5), Rigshospitalet, Copenhagen University Hospital (Copenhagen), Odense University Hospital (Odense) and Århus University Hospital (Århus) in Denmark (n = 3), and Helsinki University Hospital (Helsinki), Kuopio University Hospital (Kuopio), Oulu University Hospital (Oulu), Tampere University Hospital (Tampere) and Turku University Hospital (Turku) in Finland (n = 5). In 2020, Sweden had a population of 10.1 million, Norway 5.4 million, Denmark 5.8 million, and Finland 5.5 million. All together they form a population of approximately 26.8 million.
Definitions
GBC was considered a non-incidental finding when no cholecystectomy had been performed but GBC was suspected preoperatively, and an incidental finding when simple cholecystectomy had been performed and histology surprisingly showed GBC that was not suspected. Neoadjuvant chemotherapy was intended preoperatively for patients with resectable GBC. Downstaging chemotherapy (downstage to resectable disease) was intended for patients with primarily unresectable GBC.
Results
All 19 centers replied to the survey and were a type of university hospital. The survey was completed by MDT in 15/19 of the centers. Two out of four centers who answered the questionnaire without MDT differed slightly in the sections of neoadjuvant chemotherapy and surgical treatment in T1b-T2 compared to the centers who answered with MDT within the same country. Basic surgical characteristics of the centers are shown in Table 1.
Basic surgical characteristics of the centers.
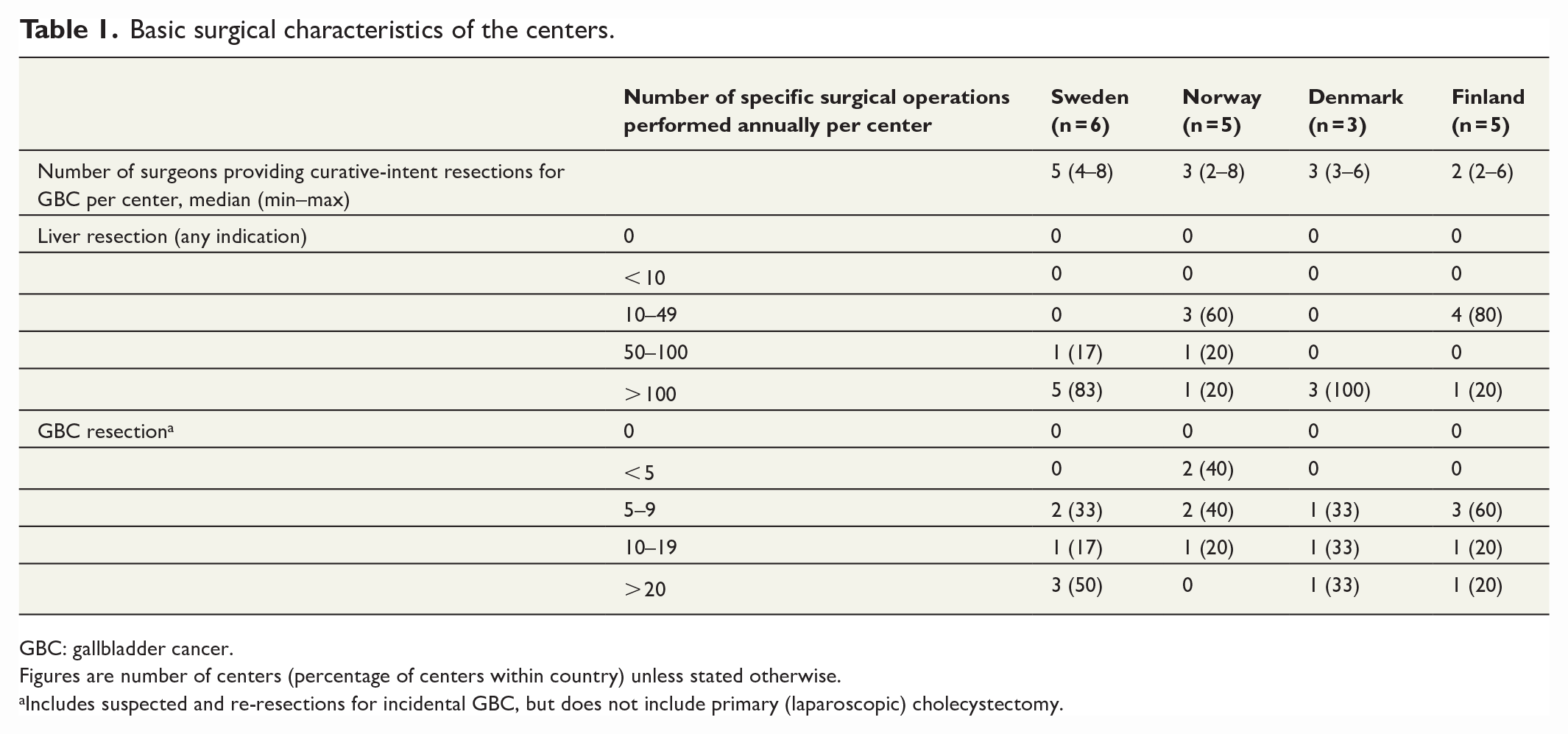
GBC: gallbladder cancer.
Figures are number of centers (percentage of centers within country) unless stated otherwise.
Includes suspected and re-resections for incidental GBC, but does not include primary (laparoscopic) cholecystectomy.
Diagnostics
Almost all (18/19) the centers used staging of TNM Classification of Malignant Tumors according to the eighth edition of the American Joint Commission on Cancer (AJCC, 2018) Gallbladder Cancer Staging System 19 to guide pretreatment decision-making. Five-sixths (16/19) of the centers used cancer antigen 19-9 (CA19-9) and 12/19 also carcinoembryonic antigen (CEA) as routine GBC tumor markers. Only four centers in Finland and one center in Denmark (5/19) included alpha-fetoprotein (AFP) as routine tumor marker in the diagnostics for GBC. Two centers in Sweden and one center in Denmark did not use any tumor markers. The main reasons for using tumor markers for GBC were diagnostics/differential (14/19) and follow-up/surveillance for recurrence (14/19). Less common reasons were follow-up/monitoring for therapy effectiveness (8/19) and staging (6/19).
Imaging for non-incidental GBC
All centers used computed tomography (CT) as routine preoperative imaging for non-incidental GBC and 15/19 also magnetic resonance imaging (MRI). Other preoperative imaging studies for non-incidental GBC included transabdominal ultrasound with contrast enhancement (CEUS; 5/19), transabdominal ultrasound (4/19), positron emission tomography-CT (PET-CT; 3/19), and biopsy (1/19). None of the centers used endoscopic ultrasound for non-incidental GBC. Five-sixths (16/19) of the centers evaluated clinical T-category (depth of invasion) with the aforementioned preoperative imaging. Other evaluation methods included intraoperative ultrasound assessment (14/19), gross morphology during operation (7/19), and routine frozen section during surgery (5/19).
Imaging for incidental GBC
Almost all (17/19) the centers used CT and 14/19 MRI for incidental GBC. PET-CT were used by 3/19 of the centers for incidental GBC. None of the centers used ultrasound of any kind or biopsy for incidental GBC.
Neoadjuvant chemotherapy
Over half (11/19) of the centers used chemotherapy as neoadjuvant/downstaging therapy selectively for GBC. Gemcitabine–cisplatin was the first-line option in all centers which gave neoadjuvant/downstaging chemotherapy. In Finland, one center used capecitabine and another center radiation therapy, in addition. The centers in Sweden generally did not use neoadjuvant/downstaging chemotherapy for GBC, except two centers in very rare cases only with young, fit patients when GBC was unresectable at the time of diagnosis (downstaging to resectable disease). Also, the centers in Norway generally did not use neoadjuvant chemotherapy and two centers also did not use downstaging chemotherapy for GBC.
Neoadjuvant chemotherapy for non-incidental GBC
According to TNM-staging when non-incidental GBC was T3 or N1 and technically resectable, only a few centers in Finland and Denmark used neoadjuvant chemotherapy (T3 3/19, N1 4/19). The rest chose upfront surgery for T3 or N1. If non-incidental GBC had grown to technically resectable T4, 7/19 of the centers chose palliative/oncological treatment, 6/19 chose upfront surgery, and 6/19 used neoadjuvant chemotherapy. In non-incidental and technically resectable N2 GBC, 10/19 of the centers chose upfront surgery and 5/19 only palliative/oncological treatment. All centers in Denmark and one center in Finland (4/19) used neoadjuvant chemotherapy in N2. If GBC was unresectable at the time of diagnosis, 12/19 of the centers used downstaging chemotherapy. The rest chose palliative/oncological treatment and no surgery regardless of response to chemotherapy.
Neoadjuvant chemotherapy for incidental GBC
When incidental GBC was T3 or N1, 7/19 of the centers used neoadjuvant chemotherapy before re-resection. The rest chose upfront re-resection for T3 or N1. In incidental T4, 12/19 of the centers chose palliative/oncological treatment, 2/19 chose upfront re-resection, and 5/19 used neoadjuvant chemotherapy routinely. In incidental N2 GBC, 9/19 of the centers chose upfront re-resection, 5/19 palliative/oncological treatment, and 5/19 used neoadjuvant chemotherapy. If incidental GBC was deemed unresectable for re-resection, 11/19 of the centers used downstaging chemotherapy. The rest chose palliative/oncological treatment and no surgery regardless of response to chemotherapy.
If resection margins of simple cholecystectomy were positive, imaging studies showed residual disease after simple cholecystectomy or encountering gallbladder perforation during simple cholecystectomy, majority of the centers chose upfront surgery and only a few centers in Finland, Denmark, and Norway (one who answered the questionnaire without MDT) used neoadjuvant chemotherapy (margins 5/19, residual 6/19, perforation 5/19).
Timing of surgery
In case of an acute cholecystitis and radiological suspicion of operable GBC, 17/19 of the centers chose conservative treatment of acute cholecystitis with antibiotics, and later proper work-up and radical resection. Only Denmark differed: one center chose emergency/priority radical extended cholecystectomy with liver resection and lymphadenectomy, and another center either elective or emergency radical resection depending on the severity of the cholecystitis and patient performance. After simple cholecystectomy, if the specimen had a GBC that required re-resection, 12/19 of the centers chose to perform re-resection as soon as possible and 7/19 waited 1–2 months before re-resection.
Surgical approach
Seven of 19 of the centers used laparoscopic access only for simple cholecystectomy in suspected GBC and 10/19 used open approach always. In Sweden, one center used laparoscopy for simple cholecystectomy, liver resection, and lymphadenectomy, and another center only for liver resection and lymphadenectomy. For laparoscopic approach, 10/19 of the centers found cT1/2-categories suitable, one center in Sweden and one center in Norway (2/19) found cT3 and cT4 suitable, and the rest 7/19 did not perform GBC surgery laparoscopically.
Surgical treatment for non-incidental GBC
In non-incidental T1a GBC with location on the peritoneal/hepatic side, majority of the centers chose simple cholecystectomy (peritoneal 16/19, hepatic 10/19), with 3/19 also taking frozen section on the cystic duct. The rest chose cholecystectomy with a small rim (1–2 cm) of liver parenchyma (peritoneal 3/19, hepatic 7/19). On the hepatic side, one center in Finland and one center in Sweden (2/19) chose cholecystectomy with liver bed excision (i.e. only fibrous bed without liver parenchyma resection).
In non-incidental T1b GBC on the peritoneal/hepatic side, majority of the centers chose cholecystectomy with a small rim of liver parenchyma (peritoneal 13/19, hepatic 15/19). The rest chose simple cholecystectomy (peritoneal 3/19, hepatic 1/19), cholecystectomy with the liver bed (peritoneal and hepatic 1/19) or cholecystectomy with resection of segments 4b and 5 (peritoneal and hepatic 2/19 including one who answered the questionnaire without MDT).
In non-incidental T2a (peritoneal side) and T2b (hepatic side) GBC, majority of the centers chose cholecystectomy with a small rim of liver parenchyma (T2a 11/19, T2b 13/19). The rest chose simple cholecystectomy (T2a 3/19), cholecystectomy with the liver bed (T2a 1/19), or cholecystectomy with resection of segments 4b and 5 (T2a 4/19, T2b 5/19, both including one who answered the questionnaire without MDT). In T2b, one center in Denmark chose multiple options from cholecystectomy with a small rim of liver parenchyma to right hemihepatectomy as necessitated by the extent of the tumor.
In non-incidental T3 GBC, 13/19 of the centers chose cholecystectomy with resection of segments 4b and 5. Some centers in Norway (3/19) chose cholecystectomy with a small rim of liver parenchyma. Two centers in Sweden and one center in Denmark (3/19) chose multiple options from cholecystectomy with resection of segments 4b and 5 to extended right hemihepatectomy (and frozen section) as necessitated by the extent of the tumor in non-incidental T3 GBC.
In non-incidental T4 GBC, majority of the centers chose palliative/oncological care (12/19). The rest performed surgery (7/19).
Surgical treatment for incidental GBC
In incidental T1a GBC on the peritoneal/hepatic side, all centers deemed simple cholecystectomy sufficient, and no re-resection was deemed necessary.
In incidental T1b GBC on the peritoneal/hepatic side, majority of the centers chose re-resection with a small rim of liver parenchyma (peritoneal 11/19, hepatic 14/19). The rest chose re-resection with the liver bed (peritoneal 2/19, hepatic 1/19) or re-resection of segments 4b and 5 (T1b peritoneal and hepatic 2/19 including one who answered the questionnaire without MDT). For T1b tumors on the peritoneal side, only a few centers (4/19) found cholecystectomy sufficient, and even fewer (2/19) found it sufficient when tumor was found on the hepatic side.
In incidental T2a and T2b GBC, majority of the centers chose re-resection with a small rim of liver parenchyma (T2a 12/19, T2b 13/19). The rest chose re-resection of segments 4b and 5 (T2a 4/19, T2b 5/19, both including one who answered the questionnaire without MDT). In T2a, only centers in Norway (3/19) deemed simple cholecystectomy sufficient. In T2b, one center in Denmark chose multiple options from re-resection with a small rim of liver parenchyma to right hemihepatectomy as necessitated by the extent of the tumor.
In incidental T3 GBC, 13/19 of the centers chose re-resection with segments 4b and 5. Some centers in Norway (3/19) chose re-resection with a small rim of liver parenchyma. Two centers in Sweden and one center in Denmark (3/19) chose multiple options from re-resection of segments 4b and 5 to extended right hemihepatectomy (and frozen section) as necessitated by the extent of the tumor in incidental T3 GBC.
In incidental T4 GBC, majority of the centers chose palliative/oncological care (14/19). The rest performed surgery (5/19).
Extra resections
Five-sixths (16/19) of the centers resected the extrahepatic bile duct if the cystic duct margin frozen section was positive. Two centers in Norway and one center in Sweden (3/19) resected it only if there was macroscopic growth to the extrahepatic bile ducts and positive frozen section. If earlier cholecystectomy had been performed, 10/19 of the centers never resected earlier laparoscopic port sites/laparotomy incisions. The rest resected port sites only if gross tumor growth/imaging showed disease in these sites. No centers routinely resect port sites in absence of evidence of disease at the sites. If direct growth was detected (in fit patients where tumor and nodal status appeared favorable), the most common adjacent organs/structures to resect (and reconstruct) were duodenum (18/19), colon (17/19), and common hepatic/bile duct (16/19). Other resected organs are shown in Table 2.
Resection (and reconstruction) of the adjacent organs/structures if direct growth was detected (in fit patients where tumor and nodal status appear favorable).
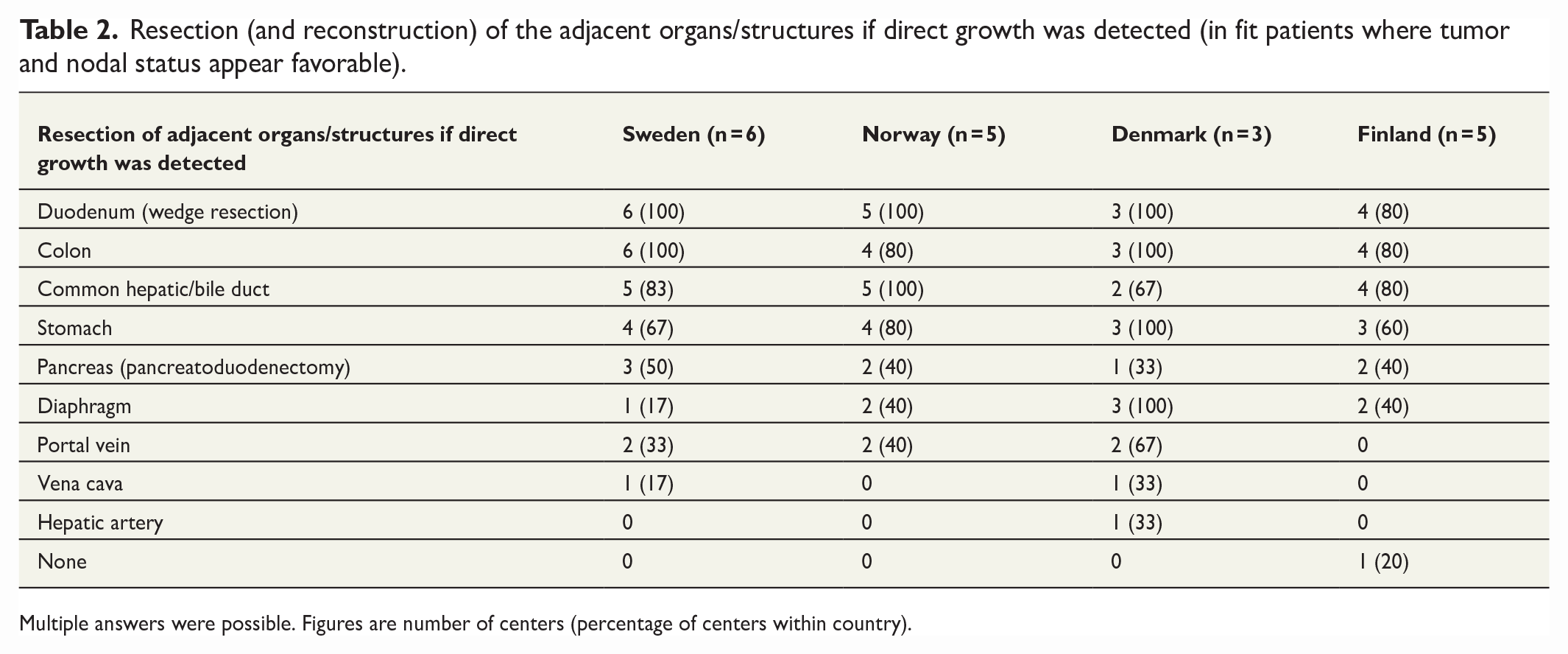
Multiple answers were possible. Figures are number of centers (percentage of centers within country).
Lymphadenectomy
Lymphadenectomy based on presumed T- and N-status (clinical, radiological, or histological) differed significantly between countries. The centers in Sweden resected more extensively and centers in Finland refrained from lymphadenectomy more often. Lymphadenectomy characteristics are shown in Fig. 2.

Lymphadenectomy based on presumed T-status and N-status (clinical, radiological, or histological).
Metastases on radiology
If a GBC primary was still intact and showed metastases on radiology in the right lobe of the liver, only two centers in Sweden and one center in Norway (3/19) chose resection, whereas all other centers chose palliative/oncological treatment. In situations such as liver metastases in the left lobe or both lobes, single lung metastasis, or a few small peritoneal metastases, all centers chose palliative/oncological treatment.
Intraoperative decision-making
Almost all (17/19) the centers took routinely frozen sections from the cystic duct to guide intraoperative treatment decisions. Other sites for possible frozen sections were lymph nodes beyond the hepatoduodenal ligament (12/19), lymph nodes of the hepatoduodenal ligament (6/19), and hepatic resection line (5/19). One center in Norway and one center in Denmark did not take frozen sections routinely. Almost all (17/19) the centers used intraoperative ultrasound without contrast media (9/19), with contrast media (6/19), or both aforementioned (2/19) to guide intraoperative decision-making. Two centers in Norway did not use intraoperative ultrasound.
Adjuvant chemotherapy
Three-quarters (14/19) of the centers used adjuvant chemotherapy in general for GBC and 12/19 most commonly capecitabine. When the use of adjuvant chemotherapy was divided according to TNM-staging, half (10/19) of the centers used adjuvant chemotherapy for T3 disease; 9/19 for T4, N1, N2, and R1; 7/19 for T2; and 3/19 always regardless of stage. None of the centers in Norway used adjuvant chemotherapy routinely for GBC. The duration of adjuvant chemotherapy in the 13 centers of the 14 who used it routinely was 6 months.
Follow-up
Three-quarters (14/19) of the centers used CT as routine follow-up of patients who had undergone curative-intent resection for GBC. Over half (11/19) of the centers used CA19-9 and 8/19 clinical examination and symptoms as routine follow-up. Interval for the first year of follow-up was usually 6 months (9/19) or 3 months (7/19). Most common interval for the second year of follow-up was 6 months (15/19) and after the second year 6 months (10/19) or 1 year (6/19). One center in Norway and one center in Denmark stopped follow-up after 2 years. One center each in Finland, Sweden, and Denmark stopped follow-up after 3 years. Two-thirds (13/19) of the centers continued follow-up until 5 years. One center in Norway did no follow-up.
Recurrence
Two-thirds (12/19) of the centers considered surgical resection of recurrence. The most usual scenarios for resection were local resectable recurrence (8/19), single resectable liver metastasis (5/19), and resectable lymph node metastases (3/19). In half (10/19) of the centers, time-to-recurrence altered the decision to proceed to surgical resection of the recurrence. One-quarter (5/19) of the centers went for resection of recurrence only if time-to-recurrence was more than 1 year, and 5/19 only if it was more than 2–3 years. In one-fifth (4/19) of the centers, time-to-recurrence did not alter the decision.
The consensus of the countries’ treatment strategies of GBC is shown in Table 3.
Consensus of the countries’ treatment strategies of GBC according to TNM-staging.
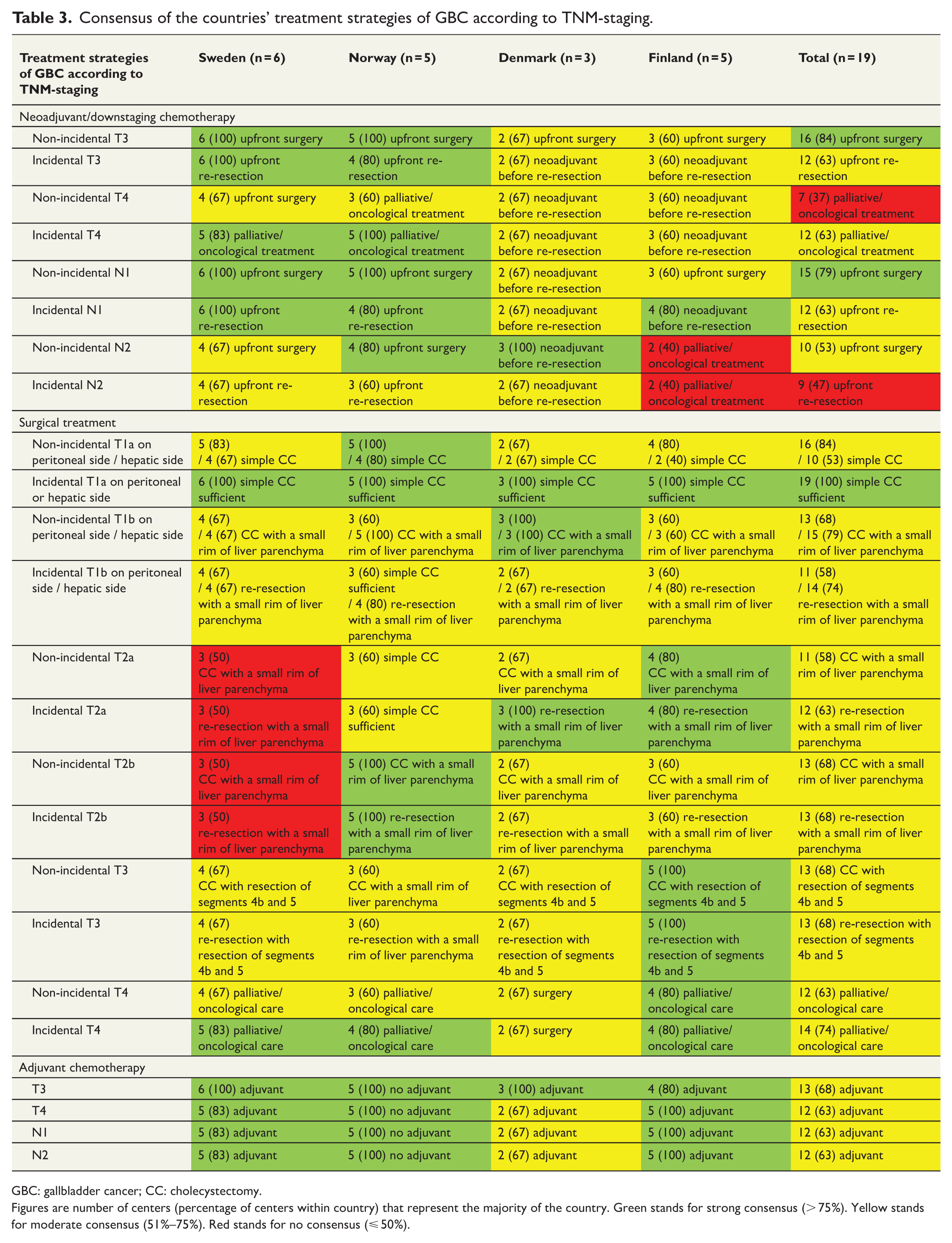
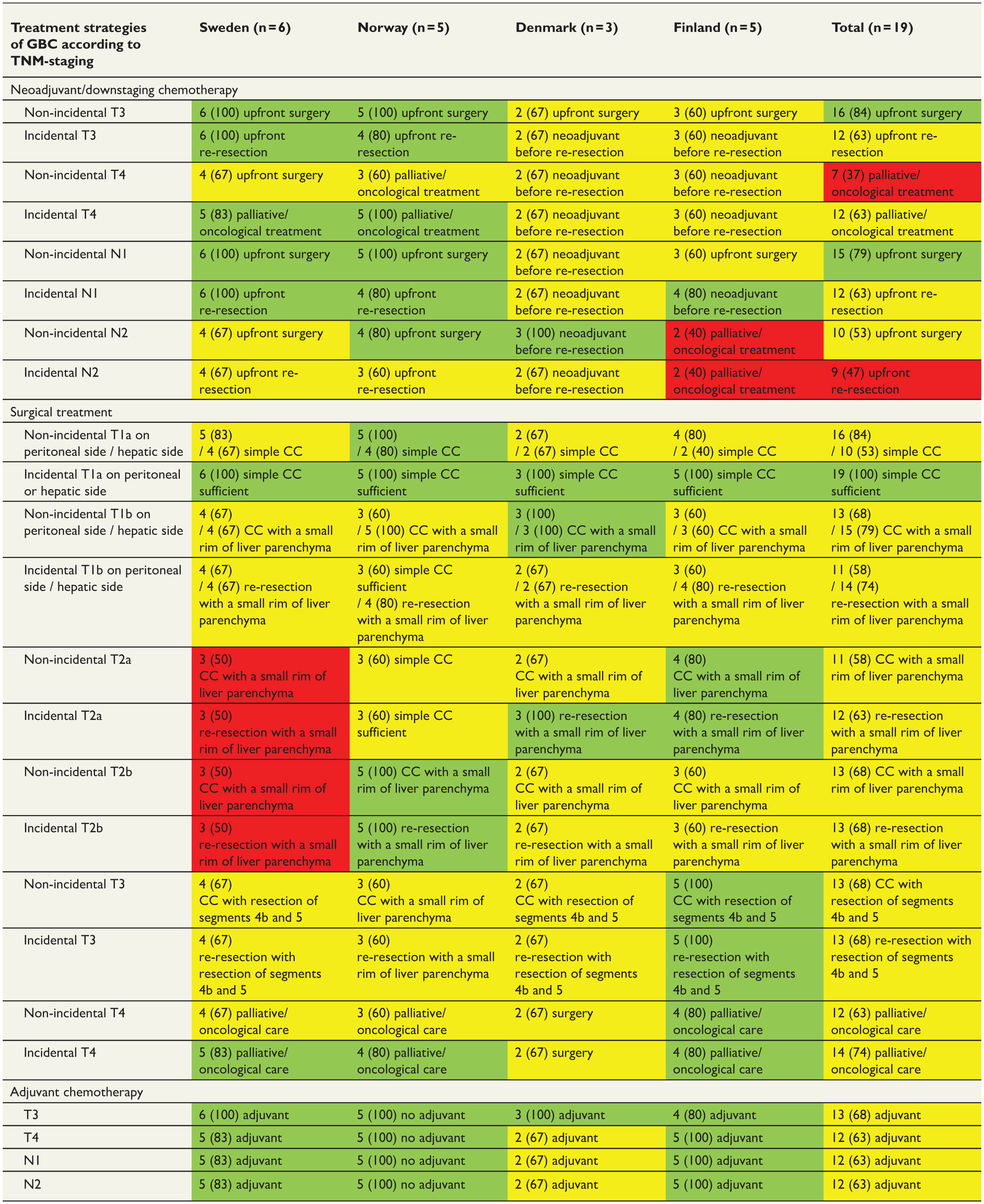
GBC: gallbladder cancer; CC: cholecystectomy.
Figures are number of centers (percentage of centers within country) that represent the majority of the country. Green stands for strong consensus (> 75%). Yellow stands for moderate consensus (51%–75%). Red stands for no consensus (⩽ 50%).
Discussion
This study revealed considerable differences between the Nordic countries in neoadjuvant and adjuvant treatments as well as surgical strategies of GBC as assessed in a survey. In all Nordic countries except Sweden, neoadjuvant/downstaging chemotherapy was used in selected patients (primarily gemcitabine–cisplatin). All Nordic centers except those in Norway used adjuvant chemotherapy routinely for GBC (most commonly capecitabine). The surgical treatment was unanimous among all centers only in incidental T1a on peritoneal/hepatic side (consensus 100%). In T1b-T4, there was a wide variation in surgical treatment strategies (consensus 58%–74%). The centers in Sweden extended lymphadenectomy beyond the hepatoduodenal ligament, whereas all other Nordic centers usually limited lymphadenectomy to the hepatoduodenal ligament.
Any differences in neoadjuvant and adjuvant therapy between centers treating GBC has not been studied before. The role of neoadjuvant chemotherapy in survival from GBC is currently based on weak evidence as no RCTs have to date been published.20,21 For adjuvant therapy, two RCTs in phase III have been reported since 2017; both recruited patients with resected biliary tract cancer who were randomized to observation or adjuvant chemotherapy of gemcitabine and oxaliplatin (PRODIGE 12-ACCORD 18) 7 or capecitabine (BILCAP). 8 The PRODIGE 12-ACCORD 18 failed to show any benefit for adjuvant chemotherapy compared with surveillance, but the BILCAP study provided evidence that adjuvant capecitabine can improve overall survival with resected biliary tract cancer in prespecified sensitivity and per-protocol analyses, although the intention-to-treat analysis failed to show any statistically significant survival benefit. Because of the low incidence of GBC, no adequate subgroup RCT analyses for GBC have been conducted. Also, the limited use of adjuvant treatments complicates the retrospective studies. 22
The current National Comprehensive Cancer Network guidelines (NCCN, 2022) 23 in the United States support the use of adjuvant chemotherapy and chemo-radiotherapy for GBC, regardless of R and N status. American Society of Clinical Oncology guidelines (ASCO, 2018) 24 also recommend adjuvant capecitabine for a period of 6 months for resected GBC patients. The Japanese Society of Hepato–Biliary–Pancreatic Surgery guidelines (JHBPS, 2019) 25 advise that adjuvant chemotherapy may be considered, although an optimal regimen has not yet been established in Japan. The Korean practical guidelines (2014, no newly updated version) 26 suggest fluoropyrimidine or gemcitabine or their combinations with local radiotherapy as adjuvant strategy for resected GBC, except for patients with T1 GBC who have undergone radical resection. The European Society of Medical Oncology guidelines (ESMO, 2016) 27 and The British Society of Gastroenterology guidelines (BSG, 2012) 28 have not yet been updated to include the latest evidence and therefore advise that adjuvant therapy may be offered for patients with GBC. In Sweden, there is a national guideline for GBC, which recommends the use of adjuvant chemotherapy in patients with increased risk of recurrence, uncertain R status after resection and in lymph node metastatic disease. Neoadjuvant treatment is not recommended. In Norway, routine use of adjuvant chemotherapy is not recommended, but it may be used on an individual basis. In Denmark, neoadjuvant/downstaging chemotherapy is recommended for locally advanced GBC tumors. In Finland, no national guidelines for GBC exist.
Surgical treatments in T1b-T2b, T3-T4, and N2 GBC differed between the Nordic centers. In T1b and T2a, majority of the centers performed extended cholecystectomy in non-incidental GBC and re-resection in incidental GBC. Few centers performed simple cholecystectomy in non-incidental GBC and deemed simple cholecystectomy sufficient in incidental GBC. Re-resection is recommended for incidental T1b or above, but the type, extent, and timing of re-resection remain controversial.29,30 In T3, majority of the centers performed cholecystectomy with resection of segments 4b and 5 in non-incidental GBC and re-resection of segments 4b and 5 in incidental GBC, but a minority resected less extensively or more extensively. In T4, majority of the centers chose palliative/oncological care in both non-incidental and incidental GBC, but a minority advocated surgery. In N2 GBC, majority of the centers would choose the surgical approach, but a few centers, especially in Finland, chose palliative/oncological treatment. The extent of lymphadenectomy differed significantly between the Nordic countries. Lymphadenectomy of the hepatoduodenal ligament and extended lymphadenectomy beyond the hepatoduodenal ligament may both improve survival of patients with GBC compared to no lymphadenectomy. 31 The NCCN guidelines 23 recommend that lymphadenectomy should be performed to clear all lymph nodes in the porta hepatis. The AJCC Gallbladder Cancer Staging System 19 recommends six or more lymph nodes to be evaluated at the time of surgical resection for patients with T1b or greater GBC. The observed wide variation in surgical treatment options for the primary tumor and for the lymphadenectomy is likely explained by the fact that there are no randomized prospective studies assessing these options for GBC and the treatment patterns and guidelines are based on weak evidence 16 leading to wider differences in interpretation of the guidelines. In Norway, for example, the adjuvant treatment strategy stems from a conservative statement in the previous version of the national recommendation. However, this wide variation has not been captured before due to previous lack of sufficiently large surveys.
There are some limitations to be noted. For one, the survey was based on virtual scenarios and not real patients, hence the response is based on a given information and the management intent to said situation. Whether real-life decisions differ to the response, is not known. Four of the centers (21%) did not discuss the survey questions with MDT and answers from those centers might not represent the treatment or diagnostic choices of all medical disciplines involved in the treatment of GBC. Only a limited number of different scenarios were offered in the survey and the answers in this study should be interpreted more as general treatment strategies rather than rigorous treatment recommendations for all patients. In the everyday clinical practice, treatment for GBC is likely to be more individualized because of a rare cancer entity. The questions were mostly closed, which was a limitation in a partly qualitative research setting. Open questions could have brought additional information about the use of molecular pathology, for example. Another limitation is that some of the scenarios presented in the survey occur very rarely in clinical practice. For example, in the last decade in Sweden, only 15/79 (19%) of the incidental T3 GBC patients underwent curative-intent re-resection and only one (1/6) incidental T4 GBC patient was re-resected successfully. 32 A strength of the study was that all hospitals providing curative-intent surgery for GBC in Sweden, Norway, Denmark, and Finland participated.
In conclusion, treatment of GBC varies considerably between the Nordic countries. The results give opportunity to research the effect of different treatment strategies on the outcome of the patients, hopefully also in RCTs, and eventually form common Nordic guidelines for GBC treatment. Given the relatively small number of GBC cases, integration and coordination of national and international clinical research efforts remain critical to continued progress in the field of treating GBC patients.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231181228 – Supplemental material for Practice patterns in diagnostics, staging, and management strategies of gallbladder cancer among Nordic tertiary centers
Supplemental material, sj-docx-1-sjs-10.1177_14574969231181228 for Practice patterns in diagnostics, staging, and management strategies of gallbladder cancer among Nordic tertiary centers by Sini Takala, Kristoffer Lassen, Kjetil Søreide, Ernesto Sparrelid, Jon-Helge Angelsen, Erling A. Bringeland, Malin S. Eilard, Oskar Hemmingsson, Bengt Isaksson, Heikki Karjula, Jukka-Pekka Lammi, Peter N. Larsen, Maija Lavonius, Gert Lindell, Frank V. Mortensen, Kim Mortensen, Arno Nordin, Torsten Pless, Per Sandström, Oddvar Sandvik, Yrjö Vaalavuo, Christina Villard and Ville Sallinen in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Helsinki University Research Grants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.