
Abstract
Background and objective:
Colorectal cancer (CRC) can mimic acute diverticulitis and can thus be misdiagnosed. Therefore, colonic evaluation is recommended after an episode of acute diverticulitis. The aim of this study was to analyze the risk of CRC after computed tomography (CT) verified uncomplicated and complicated acute diverticulitis in short-term and, particularly, long-term follow-up to ensure the feasibility of the primary CT imaging in separating patients with uncomplicated and complicated acute diverticulitis.
Methods:
A retrospective cohort study was conducted in patients with CT-verified acute diverticulitis in 2003–2012. Data on CT findings and colonic evaluations were analyzed. The patients were divided into those with uncomplicated and complicated acute diverticulitis. Patient charts were reviewed 9–18 years after the initial acute diverticulitis episode.
Results:
The study population consisted of 270 patients. According to CT scans, 170 (63%) patients had uncomplicated acute diverticulitis and 100 (37%) had complicated acute diverticulitis. Further colonic evaluation was made in 146 (54%) patients. In the whole study population, CRC was found in 7 (2.6%) patients, but CRC was associated with acute diverticulitis in only 4 (1.5%) patients. The short-term risk for CRC was 0.6% (1/170) in uncomplicated acute diverticulitis and 3.0% (3/100) in complicated acute diverticulitis. No additional CRC was found in patients with complicated acute diverticulitis during the long-term follow-up and three cases of CRC found after uncomplicated acute diverticulitis had no observable association with previous diverticulitis.
Conclusions:
In short-term follow-up, the risk of underlying CRC is very low in CT-verified uncomplicated acute diverticulitis but increased in complicated acute diverticulitis. Long-term follow-up revealed no additional CRCs associated with previous acute diverticulitis, indicating that the short-term results remain consistent also in the long run. These long-term results confirm that colonoscopy should be reserved for patients with complicated acute diverticulitis or with persisting or alarming symptoms.
Context and relevance
Colorectal cancer can mimic acute diverticulitis. Therefore, after an attack of acute diverticulitis, colonic evaluation is needed. We studied patients with computed tomography (CT) confirmed acute diverticulitis in short- and long-term follow-up. We found that the risk of colon cancer was very low after an attack of uncomplicated acute diverticulitis, but the risk was increased after complicated acute diverticulitis in short-term follow-up. No additional cancers associated with acute diverticulitis were found in long-term follow-up period, indicating that the short-term results on separation of patients with acute diverticulitis from those with cancer remain consistent also in the long run. The risk of colorectal cancer among patients in long-term follow-up is similar to that among patients undergoing screening colonoscopies. These long-term results confirm that further colonic evaluation after CT-verified acute diverticulitis should be reserved for patients with complicated acute diverticulitis and those with uncomplicated diverticulitis with persisting or alarming symptoms.
Introduction
Colonic diverticulosis is a common condition in Western countries, and its prevalence increases with age. 1 Approximately 4% of patients with diverticulosis develop symptomatic disease, such as acute diverticulitis. 2 When diagnosing acute diverticulitis today, computed tomography (CT) imaging is commonly performed, and it is the recommended imaging technique in patients with suspected acute diverticulitis.3–5 Although CT imaging has high sensitivity and specificity, 6 colorectal cancer (CRC) may mimic diverticulitis, and therefore, colonoscopy has been recommended after an episode of acute diverticulitis.4,7,8 Risk of CRC in patients with acute diverticulitis has been studied and found to be higher than in screening population.9,10 Recently, it has been suggested that colonoscopy might not be necessary after an episode of uncomplicated acute diverticulitis, but it is indicated in patients with complicated disease.11–15 However, in the literature, there are few studies with long-term follow-up on this issue. 16
The objective of this study was to analyze whether further colonic examination is worthwhile for ruling out malignancy after CT-diagnosed acute diverticulitis. Our hypothesis was that the risk of underlying CRC is low after CT-diagnosed uncomplicated acute diverticulitis, but risk increases when diverticulitis shows signs of complications in CT. We also wanted to analyze information provided by colonic evaluations regarding other findings and, in particular, evaluate long-term CRC risk after an episode of CT-verified acute diverticulitis to ensure the consistency of the initial CT-diagnosis also in the long run.
Methods
The study was performed at Turku University Hospital, an academic institution, which serves a population of 470,000 inhabitants. A retrospective analysis was carried out in adult patients who were treated at our institution during 2003–2012 and who had the International Statistical Classification of Diseases and Related Health Problems–Tenth Edition (ICD-10) code diagnosis of K57. The studied patient population was collected from the Register of Primary Health Care Visits (HILMO) maintained by the Finnish National Institute for Health and Welfare. The study was approved by the Turku Clinical Research Center. Subjects’ informed consent was not required.
During the study period, a total of 1694 patients were treated at our institution with ICD-10 diagnosis K57 of acute diverticulitis. Overall, 270 patients had CT-confirmed acute colonic diverticulitis, and those patients were included in this study. Patients with only clinical diagnosis of acute diverticulitis (n = 1228) were excluded from the analysis. Similarly, 77 patients with diagnosis other than acute diverticulitis in CT, 62 patients with no real evidence of acute diverticulitis despite of ICD code K57, and 57 patients eventually presenting with diagnosis other than acute diverticulitis after further investigations during hospitalization were excluded.
Patient data were manually collected from electronic patient records and scrutinized. The data included each patient’s age, sex, clinical and initial laboratory findings on admission, CT findings, colonic evaluation findings, history of previous diverticulitis, and occurrence of CRC. All abdominal CT scans were performed from diaphragm to the pubic symphysis using multi-detector row helical CT scanners. A study series with contrast was performed during portovenous phase according to standard imaging protocol. The radiation dose of CT was 5–7 mSv depending on the size of the patient. Based on CT findings, the patients were divided into two subgroups: uncomplicated acute diverticulitis and complicated acute diverticulitis. The CT scans were evaluated by on-call radiologists, and the diagnosis of uncomplicated or complicated acute diverticulitis was based on these reports. The CT scans were not re-evaluated later on. Acute diverticulitis was considered complicated if CT scans showed suspicion of perforation, abscess, fistula, bowel obstruction or stricture.
Turku University Hospital is responsible for all CRC patients in the district, and therefore, all patients with CRC can be found in our electronic patient records. All patients with ICD code K57 were also searched from the same register for ICD codes C18–C20, indicating CRC. Follow-up until 1 year was considered short-term follow-up, and long-term follow-up time ranged from 9 to 18 years.
Descriptive statistics for continuous variables were reported as mean values (standard deviations) and for categorical variables as percentages. Mean differences in continuous variables between the uncomplicated and complicated diverticulitis groups were tested using two-sample t-test. Chi-square tests or Fisher’s exact tests were used to compare differences in categorical variables between the groups. We performed statistical analyses using the SAS System for Windows version 9.4 (SAS Institute Inc., Cary, NC, USA). All tests were two-sided, and we used a significance level of 0.05.
Results
The study flowchart and patient characteristics are summarized in Fig. 1 and Table 1, respectively. Of 270 patients, according to CT scans, 170 (63%) patients had uncomplicated acute diverticulitis and 100 (37%) had complicated acute diverticulitis. The patients’ mean age was 61 years in the uncomplicated acute diverticulitis group and 64 years in the complicated acute diverticulitis group, and 59% and 57% of the patients were female, respectively. The initial values of temperature, hemoglobin, and leucocytes, measured on admission to hospital, showed no statistically significant difference between the groups. The initial c-reactive protein (CRP) levels were higher (p = 0.0003) in the complicated acute diverticulitis group.
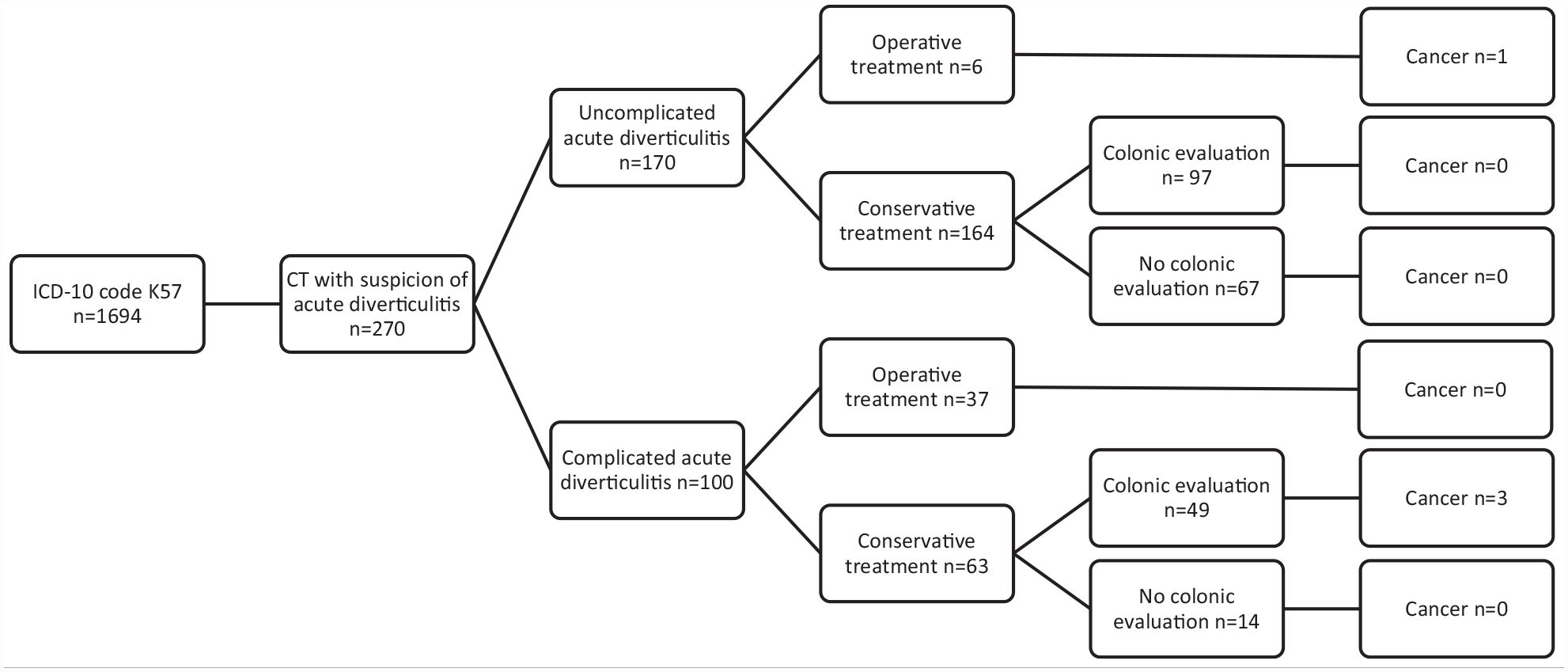
Study flowchart presenting patient distribution and occurrence of cancer in patients with uncomplicated and complicated diverticulitis.
Patient characteristics.
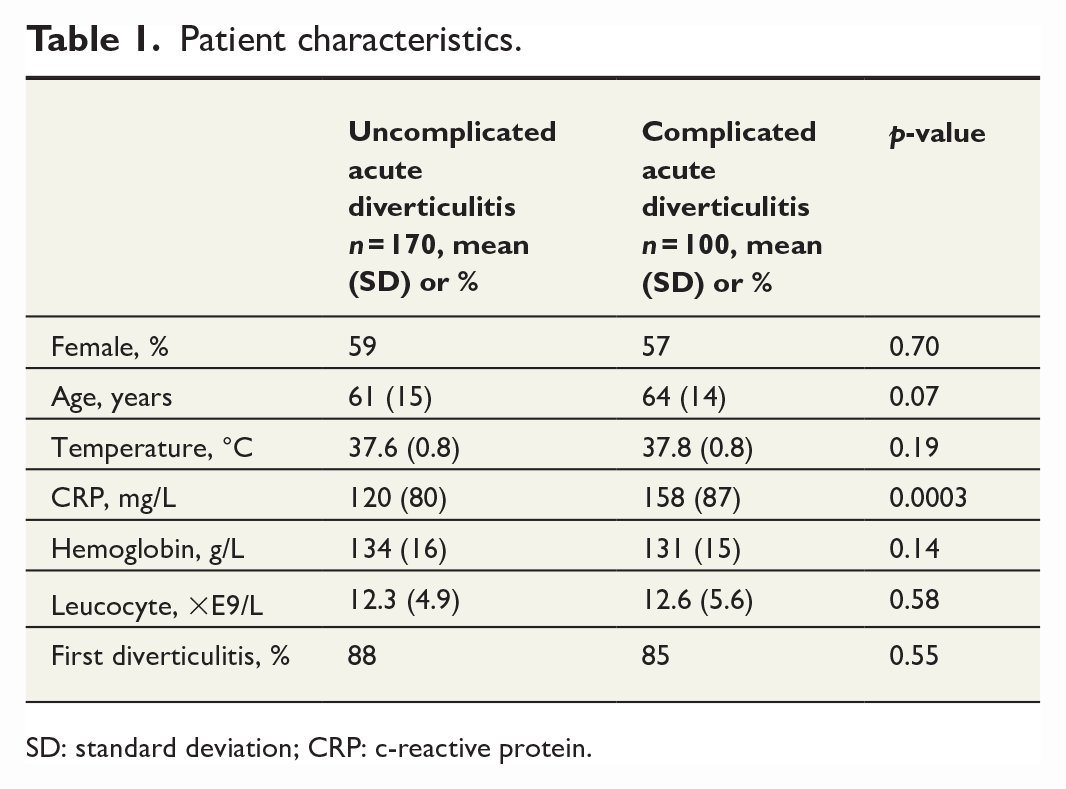
SD: standard deviation; CRP: c-reactive protein.
Among complicated disease cases, an abscess was found in 27 patients, pericolic air was found in 28 patients, distant air was found in 29 patients, obstruction was found in 5 patients, and fistula was found in 3 patients. In eight patients, tumors could not be ruled out because there was a stricture and a significant wall thickening or mass. In both study groups, most of the patients had their first acute diverticulitis attack.
After CT verification of acute diverticulitis, 146 (54%) patients had further evaluation of the colon. Of these, 65 patients underwent endoscopy, 26 underwent CT colonography, 66 underwent barium enema and 5 underwent abdominal CT, and 16 had more than one examination, mainly due to inadequate first examination. Only one complication, perforation in colonoscopy, was recorded in further evaluations. No further follow-up investigation was made in 124 (46%) patients. The various reasons for not completing further colonic evaluation are listed in Table 2.
Reasons why colonic evaluation was not made after CT-verified acute diverticulitis.
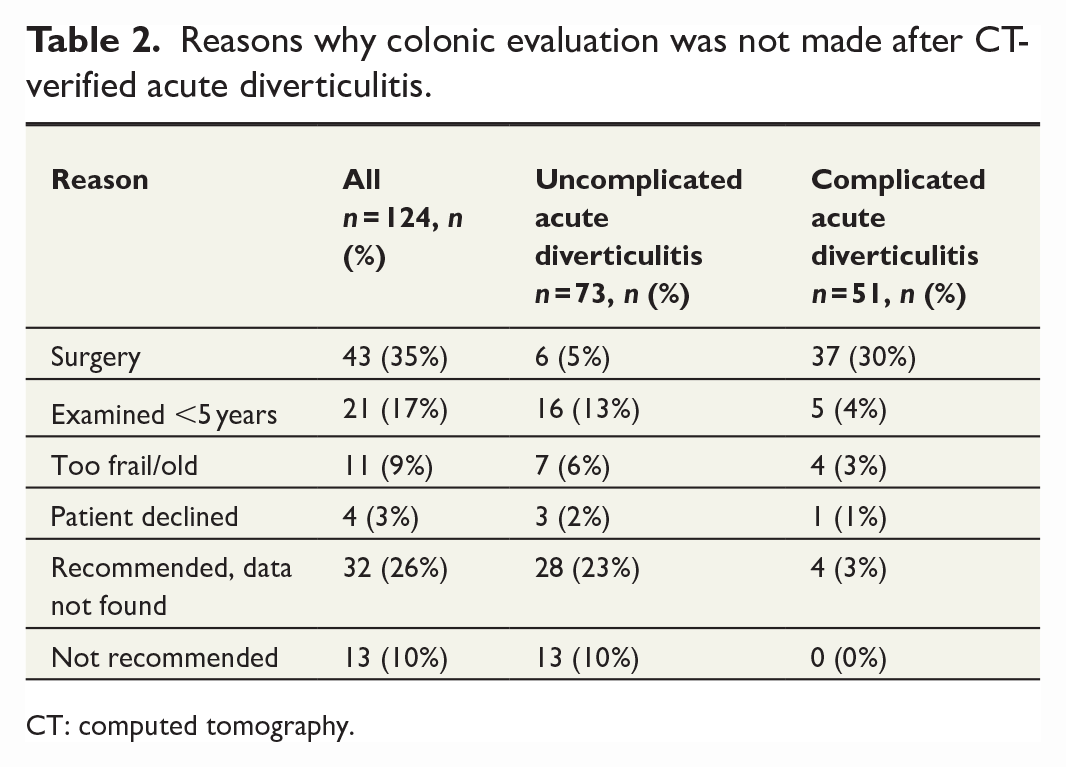
CT: computed tomography.
Table 3 illustrates the findings in colonic evaluations of 146 patients after an attack of CT-confirmed acute diverticulitis. Diverticulosis was found in 92 (95%) patients and 43 (88%) patients after uncomplicated and complicated acute diverticulitis, respectively. No cancers were found in patients with uncomplicated acute diverticulitis. Two cancers and one stricture with a suspicion of cancer, later confirmed as cancer during surgery, were found in patients with complicated acute diverticulitis. In the uncomplicated acute diverticulitis group, one patient had stricture, which proved to be benign. Only 5 patients had adenomas in colonic evaluations, and none of them were advanced.
Findings of colonic investigations in 146 patients after an attack of CT-verified acute diverticulitis.
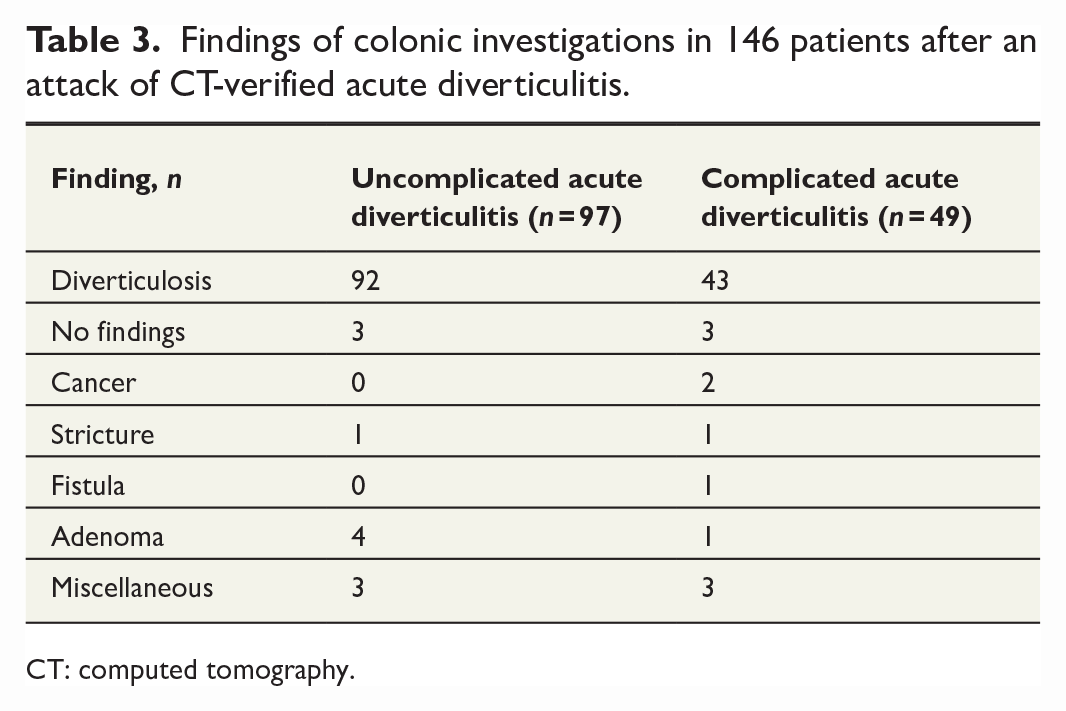
CT: computed tomography.
Overall, of the 270 patients in this study, cancer was found in a total of 7 (2.6%) patients. In short-term follow-up, four (1.5%) patients with CT-confirmed acute diverticulitis were found to have cancer: one (0.6%) patient in the uncomplicated group and three (3.0%) patients in the complicated group. The patient with uncomplicated acute diverticulitis was operated on during the same hospital admission. In a retrospective view, a significant wall thickening and obstruction in the sigmoid colon could be found at preoperative CT, and emergency operation revealed that there was a malignant tumor in the sigmoid colon. Among the three patients with complicated acute diverticulitis in which cancers were found in further evaluations, the patients later had surgery.
In the long-term follow-up, two patients had cancer 2 years after uncomplicated acute diverticulitis, and one patient had cancer 16 years after uncomplicated acute diverticulitis, but the cancers were found in other parts of the colon than where the diverticulitis had occurred. Two of these patients had colonic evaluations with no signs of cancer after the primary attack of acute diverticulitis. The patient who had cancer 16 years after acute sigmoid diverticulitis had cancer in the cecum and had undergone no further colonic investigations after the acute diverticulitis episode. In patients with complicated acute diverticulitis, no additional cancers were found during long-term follow-up.
Discussion
The results of this study indicated that in short-term follow-up, the risk of CRC is very low in CT-verified uncomplicated acute diverticulitis but increased in CT-verified complicated acute diverticulitis. Long-term follow-up revealed no additional CRCs associated with previous acute diverticulitis, neither in patients with CT-verified uncomplicated acute diverticulitis nor in those with CT-verified complicated acute diverticulitis, indicating that the short-term results on separation of patients with acute diverticulitis from those with cancers remain consistent also in the long run.
The need for colonic evaluation after an attack of acute diverticulitis has been under debate. Previously, it was advised to do a colonoscopy after CT-proven acute diverticulitis to confirm the presence of diverticulosis and exclude cancer.8,17 However, there is evidence that further colonic evaluation might not be necessary in all cases.11–15,18–20 In previous studies, the prevalence of CRC after CT-diagnosed acute diverticulitis has varied from 0% to 8%.13,21,22 However, when acute diverticulitis is stratified according to the disease’s severity, a clear discrepancy can be seen: if uncomplicated acute diverticulosis is detected in a CT scan, the risk of malignancy is very low, but the risk is higher in cases of complicated acute diverticulitis.11–15,18–20 The risk of CRC after uncomplicated acute diverticulitis has been reported to be similar to the risk found in screening colonoscopies, in which the prevalence of CRC is under 1%.23,24 However, it should be emphasized that patients with abdominal symptoms are often overrepresented in patient groups willing to participate in screening colonoscopies, and, therefore, any results based on screening colonoscopies do not necessarily reflect findings in general population. In this study, the risk of underlying CRC after a CT-verified acute diverticulitis was 1.5%. When the patients were divided into uncomplicated or complicated acute diverticulitis, cancer was found in 0.6% and 3.0% of the patients, respectively. Thus, the results of this study align with those reported in earlier literature. Moreover, the novel finding of this study was that the conclusions remain consistent in the long-term follow-up period.
In colonoscopies performed after acute diverticulitis, the detection rate for adenomas and advanced adenomas has varied between 9%–15% and 3%–5%, respectively.18,19,25 In recent meta-analyses by Meyer et al. 21 and Rottier et al., 22 the prevalence of advanced adenomas among patients who underwent colonoscopy after an attack of acute diverticulitis was similar, 4.4% and 6.9%, respectively. In a multi-center study, the detection rate of adenomas during colonoscopy after acute diverticulitis was similar to control patients undergoing a screening colonoscopy. 23 Another retrospective cohort study has also suggested that patients with CT-proven acute diverticulitis are not at increased risk of colonic neoplastic lesions compared to patients undergoing screening colonoscopy. 26 In this study, the detection rate for adenomas was very low (3.4%), probably because, unfortunately, some of the evaluations were made with barium enema, which cannot detect small polyps.
Although our data showed no statistically significant difference in cancer prevalence in patients with uncomplicated acute diverticulitis and those with complicated acute diverticulitis, our results are in concert with earlier findings. Sharma et al. 13 conducted a systematic review and meta-analysis and found that the risk of underlying malignancy is 1.6% in patients who had colonic evaluation after radiologically confirmed acute diverticulitis. The risk was higher in complicated acute diverticulitis than in uncomplicated acute diverticulitis (10.8% and 0.7%, respectively). The researchers concluded that the patients with complicated acute diverticulitis have a significant risk for CRC and, therefore, should undergo colonic evaluation after an attack of acute diverticulitis. A more recent meta-analysis of observational studies of patients with uncomplicated and complicated acute diverticulitis showed similar results, the prevalence of cancer was 1.3% and 7.9%, respectively. 21 Similar results were reported also by Andrade et al. 25 who retrospectively analyzed 252 patients who had undergone colonoscopy after an episode of CT-proven acute diverticulitis. In patients with Hinchey 1a diverticulitis, only 0.5% of patients had cancer, but if CT showed abscess, the cancer risk was as high as 16.3%. The researchers also recommended colonoscopy for only patients with complicated acute diverticulitis. Furthermore, in another retrospective study comprising 249 patients, the CRC risk differed between patients with uncomplicated acute diverticulitis and those with complicated acute diverticulitis (0% and 5.4%, respectively). 11
A retrospective study conducted by Sallinen et al. 12 concluded that follow-up colonoscopy should be reserved for patients with diverticular abscess in CT. In their study, 536 patients were treated conservatively, and of those, 394 had colonoscopy. No cancer was found in patients with uncomplicated acute diverticulitis. For patients with abscess in CT, the malignancy risk was 11.4%. In this study, an abscess was found in 27/270 (10%) of the studied patients, and one of those patients had cancer. Two patients in this study’s complicated acute diverticulitis group who had cancer also had significant bowel wall thickening visible in CT images. It has been demonstrated that if significant bowel wall thickening is seen in CT imaging, the risk of underlying pathologic condition is high, thus warranting colonoscopy. 27
Westwood et al.’s 18 retrospective study in 292 patients with CT-confirmed acute diverticulitis showed that out of 175 patients who underwent further colonic evaluation, only one (0.5%) patient with uncomplicated disease had cancer. When the CT was retrospectively reviewed by an independent radiologist, the cancer was, in fact, visible in the CT. Moreover, in this study, one case of CRC was found in a patient who was initially diagnosed with uncomplicated acute diverticulitis. After reviewing the CT scan, a clear thickening of the bowel wall and a stricture were detected, and the patient should have been classified as having complicated rather than uncomplicated acute diverticulitis. The patient developed bowel obstruction a few days after hospital admission and underwent an operation. The original CT report was provided by a resident radiologist. Although the specificity and sensitivity of CT in the diagnosis and severity assessment of acute diverticulitis are high, false negative results and mistakes in interpreting CT scans may occur.28,29 In a large population-based cohort study, 155 patients from a total of 7473 patients with acute diverticulitis had CRC within 1 year after an attack of acute diverticulitis. 29 Of these, 80 patients had had CT imaging at index admission, and 41 had uncomplicated acute diverticulitis and 39 had complicated acute diverticulitis. The authors suggested that increased risk of CRC is probably due to misdiagnosis in CT in uncomplicated and complicated diverticulitis cases. Therefore, colonoscopy should also be performed after CT-verified uncomplicated acute diverticulitis with alarming or persisting symptoms.5,30,31
It has been suggested that diverticular disease does not increase the risk of CRC in long-term follow-up. 31 In a recent meta-analysis by Mortensen et al., 16 no long-term risk of CRC was found after an attack of acute diverticulitis. Twelve studies were included in the meta-analysis and follow-up time ranged from 6 months to 27 years. In this meta-analysis, the data did not include information on CT verification of acute diverticulitis. Furthermore, a retrospective analysis of 402 patients with CT-verified acute diverticulitis and with further colonoscopy did not show increased risk of CRC in long-term follow-up. 32 However, the follow-up time, that is, time to colonoscopy, ranged from 1 month to 5 years, and most of the patients had their colonoscopy within 1 year. In two retrospective cohort studies with CT-diagnosed acute diverticulitis, the risk of CRC was not increased within 1-year follow-up.33,34 Also, a nationwide population-based retrospective cohort study showed that diverticulitis was not associated with an increased risk of CRC in long-term follow-up; however, the diagnosis of diverticulitis had not been done by CT imaging. 35 However, due to difficulties in primary differential diagnostics, the risk of CRC has been found increased after diverticulitis, especially if colonoscopy is not performed afterwards. 10 In this study, all patients with acute diverticulitis were diagnosed with CT imaging and follow-up time ranged from 8 to 19 years. In this study, in long-term follow-up, only three (1.1% of the 270 patients) cases of CRC were found, in addition to four CRCs found shortly after episodes of acute diverticulitis. This is comparable to findings in screening colonoscopies, in which the risk of CRC is below 1%.23,24 It seems that if acute diverticulitis is diagnosed with CT imaging and uncomplicated acute diverticulitis found, there is no need for further investigations, if alarming or persisting symptoms do not exist.
This study had some limitations. The data are retrospective. Further colonic evaluation was achieved using not only colonoscopy, which is currently advised, but also barium enema, which was more easily available at our institution during the study period. The number of further investigations was relatively small; only 54% of studied patients underwent further evaluation of the colon after the diagnosis of acute diverticulitis. Some additional patients underwent evaluation, but, unfortunately, we lacked the information because evaluations occurred elsewhere. However, because all CRCs in the district are treated at our institution, we can trust that no additional cancers were found in our district within the follow-up period. This study’s strength is that, to our knowledge, this is the first report on this issue with long-term follow-up on patients with CT-verified acute diverticulitis.
Our results support earlier findings that in short-term follow-up, the colon cancer risk is low after CT-confirmed uncomplicated acute diverticulitis but that it is higher after complicated acute diverticulitis. Long-term follow-up revealed no additional CRC cases associated with previous diverticulitis, indicating that the short-term results remain consistent also in the long run; thus, the risk for CRC in long-term follow-up is similar to that in screening colonoscopies. These novel long-term results confirm that colonoscopy should be reserved for patients with complicated acute diverticulitis and those with uncomplicated diverticulitis with persisting or alarming symptoms.
Footnotes
Author contributions
Study conception and design were performed by L.M.M., J.G., and J.K. L.M.M. collected and interpreted the data and wrote the manuscript. Statistical analysis was performed by T.V. and M.R. Revision and editing of the manuscript were done by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Finnish government research funding (EVO).