
Abstract
Background and objective:
Decreased skeletal muscle mass and quality are one of the several markers used for sarcopenia diagnosis and are generally associated with increased rates of post-operative infections, poorer recovery and increased mortality. The aim of this review was to evaluate methods applied to detect markers of sarcopenia and the associated outcomes for patients undergoing emergency laparotomy.
Methods:
This review was conducted with reference to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. MEDLINE, Embase and Google Scholar databases were searched. Studies detecting patients with sarcopenia or skeletal muscle decline markers and the associated outcomes after emergency laparotomy surgery were considered. The Newcastle–Ottawa Scale was used to evaluate publication quality.
Results:
Out of 103 studies, which were screened, 19 full-text records were reviewed and 7 studies were ultimately analyzed. The study cohort sizes ranged from n = 46 to n = 967. The age range was 36–95 years. There were 1107 females (53%) and 973 males (47%) across all 7 studies. All studies measured psoas muscle mass and three studies assessed psoas muscle quality using computerized tomography (CT) imaging. No study assessed muscle strength or function, while five studies showed an association between low muscle mass and increased mortality rates after emergency laparotomy. Among the three studies, which assessed muscle quality, two of three studies showed poorer 30-day survival rates.
Conclusions:
The existing literature is limited, however it indicates that low psoas muscle mass and quality markers are associated with increased 30-day mortality rates after emergency laparotomy. Therefore, muscle markers can be used as a new feasible tool to identify most at risk patients requiring further interventions.
Introduction
Emergency laparotomy is an umbrella term for a group of surgical procedures involving abdominal viscera performed for acute and life-threatening conditions. In the United Kingdom alone between 30,000 and 50,000 emergency laparotomies are performed annually. 1 Procedures requiring emergency laparotomy include small bowel resections, colectomies and exploratory laparotomies, among many others, making it a heterogeneous group of surgical interventions. Emergency laparotomy is an invasive procedure and mortality rates reported internationally range from 13% to 18% at 30 days, increasing to 25% at 24 months. 2
Despite the recognition of frailty as a risk factor for poor post-operative outcomes and the association of frailty with sarcopenia, the literature is limited regarding the effects of skeletal muscle decline or more formally diagnosed sarcopenia on patients undergoing emergency laparotomy. The presence of sarcopenia, however, has been shown to be associated with poor outcomes in other fields of surgery.3–6
The most recent European Working Group on Sarcopenia in Older People 2 (EWGSOP2) guidelines define probable sarcopenia by the presence of two parameters of muscle atrophy, including low muscle strength and low muscle mass (quantity of muscle) or quality (muscle architecture and composition). 7 Additional demonstration of low physical performance is defined as severe sarcopenia. 7
As described by Pipek et al., 8 in context of elective surgery a precise sarcopenia diagnosis using EWGSOP2 guidelines is feasible and offers prognostic information. However, in the setting of emergency laparotomy, muscle strength and function measurements may not be appropriate or may not be accurately performed. In patients who are clinically unstable, muscle mass or muscle quality radiographic measurements may be the only feasible option. For this, EWGSOP2 recommends cross-sectional imaging using computerized tomography (CT) or magnetic resonance imaging (MRI) for assessing psoas major muscle to detect low muscle mass or quality. 8
A decision to operate on frail, critically ill patients with co-morbidities can be an ethical challenge. Post-operatively, frail patients with small and weak muscles may never rehabilitate to their baseline function and quality of life after emergency intervention. This review aims, therefore, to evaluate methods employed to detect muscle decline markers in the setting of emergency laparotomy and to assess the associated outcomes after emergency laparotomy surgery.
Methods
The review was performed and reported in compliance with Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. The search was conducted in MEDLINE (US National Library of Medicine) and Embase (a registered trademark of Elsevier B.V.) via Ovid interface. Only publications in English language were considered. The search sample covered the period from the time when the earliest records were available until 7th March 2021. Grey literature was identified through Google Scholar. Single author (F.F.B.) performed the initial literature search and subsequently two authors (F.F.B. and J.I.B.) separately screened titles and abstracts from the original selection of publications. Papers underwent full review whenever there was divergence of opinions between both authors.
Search terms and adopted inclusion criteria
The search terms included “Sarcopenia” OR “Myopenia” OR “Muscle Atrophy” [MeSH terms] AND “Laparotomy” OR “Emergency Laparotomy” [MeSH terms] OR “Emergency Surgery” [MeSH terms]. In each database, independent searches using the same MeSH terms were conducted. The results were combined and duplicates were removed.
Primary studies assessing muscle atrophy or sarcopenic muscle changes and the associated post-operative outcomes for patients undergoing emergency laparotomy were considered for inclusion. Emergency laparotomy was defined as emergency surgery involving incision into abdominal cavity, performed in a non-elective setting by an acute care surgery team. Studies assessing abdominal emergency surgery, but not specifically emergency laparotomy, or studies assessing laparotomy in a non-emergency setting were also excluded. Studies including laparoscopic surgery were excluded. Randomized control trials, prospective and retrospective cohort studies were considered. Unpublished data, animal studies, case reports and conference publications were excluded.
Extraction of data
Data were extracted from texts by one author (F.F.B.). The extracted information included the authors, study date, study type, number of male and female participants, patient demographics (including age, body mass index (BMI), American Society of Anesthesiologists (ASA) grade), skeletal muscle measurements (CT-based psoas muscle mass and attenuation measurements) and threshold values employed to identify muscle decline (degree of psoas muscle mass or quality defined as a “low level”). Moreover, indications for an emergency laparotomy and associated surgical outcomes were exported from texts for analysis.
Risk of bias assessment
The Newcastle–Ottawa Scale (NOS) was used for the evaluation of the quality of each study’s methodology. 9 The NOS employs a system of nine criteria, which assess the selection of the study groups, the comparability of the groups and the ascertainment of the outcome of interest. The NOS appraises each study using a scoring system, which allocates stars. When relevant information that was associated with methodological quality of one of the NOS criteria was present in the study, it was awarded one star. Studies assigned 7–9, 4–6 and 0–3 stars were assessed as high quality, moderate quality and low quality, respectively. Studies, which compared the relationship between muscle markers and outcomes, but did not define a cut-off value for sarcopenia or a marker for muscle decline within the study, were classified as having inadequate ascertainment of exposure.
Results
The database search identified 131 articles in total (21 in MEDLINE and 110 in Embase). No additional studies were found using the Google Scholar search engine or on the reference list of our final records. After the removal of duplicates, 103 studies were identified for analysis. Article titles and abstracts were screened, which resulted in identification of 19 studies for further review, out of which 12 studies were removed based on non-compliance with the inclusion criteria. Ultimately, seven studies were selected (Table 1). All studies were designed as retrospective cohort studies. The cohort sizes ranged from n = 46 to n = 967. The age range in the cohort populations was 36–95 years. There were 1107 females (53%) and 973 males (47%) across all 7 studies. The main indication for emergency laparotomy was intestinal obstruction in six articles. Imamura et al. 10 study specifically investigated outcomes for patients after emergency laparotomy surgery for bowel perforation only and Simpson et al. 11 study assessed outcomes following emergency laparotomies, most commonly for small bowel resections. Use of diagnostic laparoscopies was not discussed in any study. Five studies assessed outcomes on European cohorts, one study measured outcomes in a Middle Eastern cohort and one in an Asian cohort.
Study design and cohort characteristics.
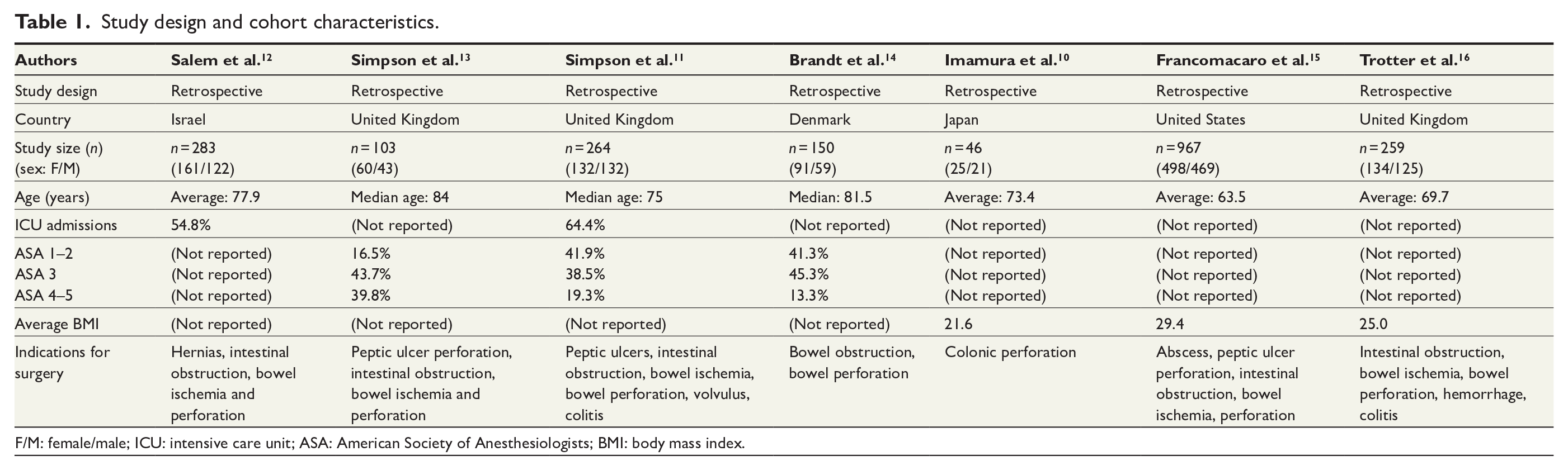
F/M: female/male; ICU: intensive care unit; ASA: American Society of Anesthesiologists; BMI: body mass index.
All studies utilized CT scanning for muscle mass quantification of the psoas muscle (Table 2), whereas five studies described performing CT imaging and calculating psoas muscle measurements between the patient admission and emergency laparotomy, one study performed CT imaging within 30 days of emergency laparotomy and only one study did not specify how close to emergency laparotomy CT imaging was performed. Muscle decline or sarcopenia status was explicitly defined based on muscle size in five of seven studies and based on psoas muscle quality or attenuation in two studies. Six studies used L3 and one study used L4 as the level for psoas muscle measurements. Three of seven studies assessed crude psoas cross-sectional area by total psoas area (TPA) or perpendicular cross-sectional diameter of psoas (PCSD) measurements. Muscle size was additionally evaluated by normalizing psoas muscle area to patient’s lumbar vertebra area in two studies, to patient’s height in two studies and body surface area in further two studies. Muscle quantity was not determined in any study using dual energy X-ray absorptiometry (DXA) or bioelectrical impedence analysis (BIA) methods. No study assessed muscle strength or muscle function; therefore, no study formally defined sarcopenia based on EWGSOP2 guidelines.
Summary of markers and reference values used to detect low muscle mass and quality.
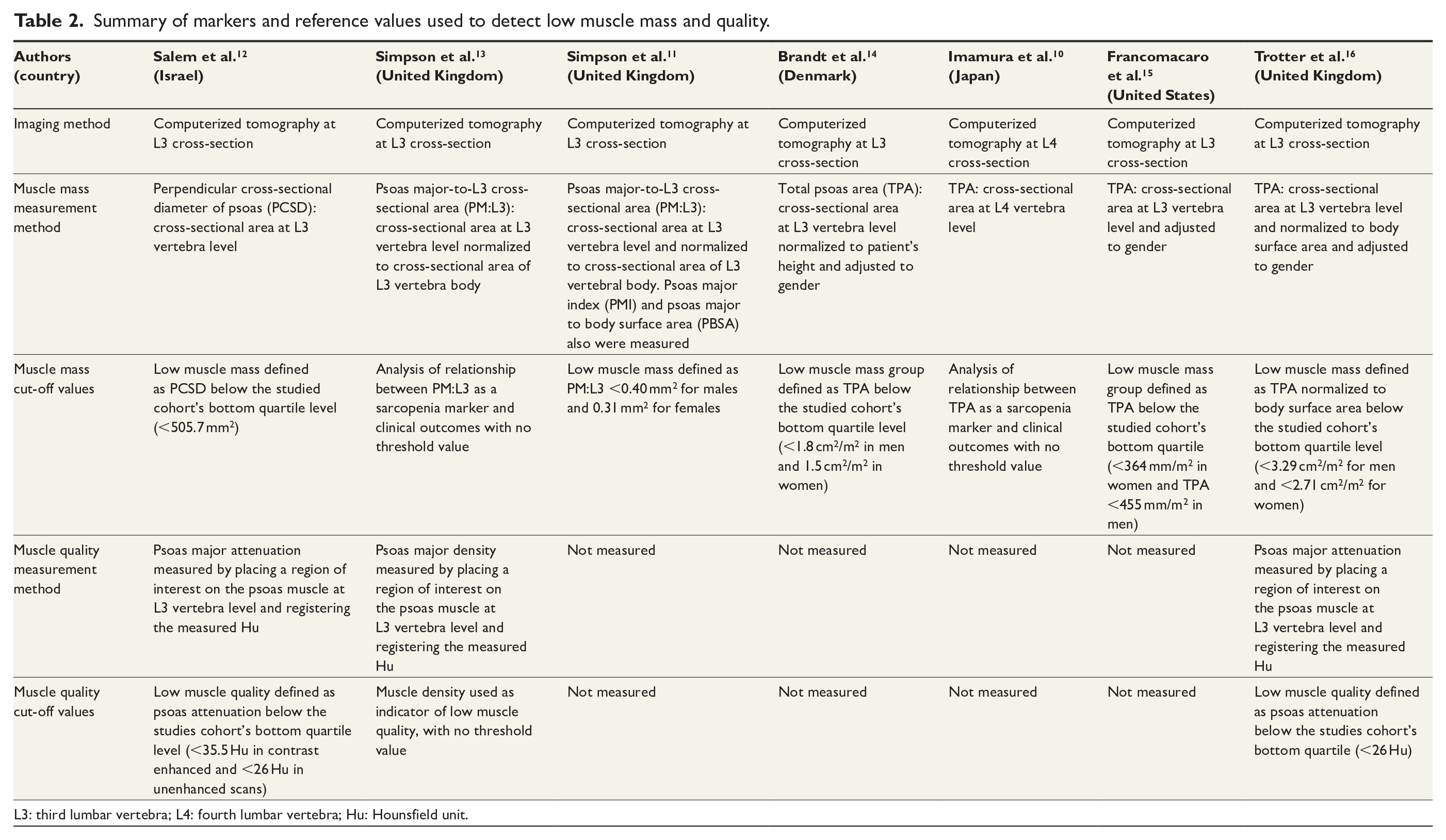
L3: third lumbar vertebra; L4: fourth lumbar vertebra; Hu: Hounsfield unit.
All seven studies assessed clinical outcomes after emergency laparotomy in patients with likely muscle decline determined by muscle mass measurements. Five of seven studies showed association between low muscle mass and increased mortality rates after emergency laparotomies (Table 3). Specifically, three studies compared the 30-day mortality rate in low muscle mass and control groups using TPA at L3 level. Average mortality rate from these studies in the low muscle mass group was 26.6% (standard deviation (SD) = 25.9) and 13.3% (SD = 15.8) in the control group. Brandt et al. also used TPA and showed a 90-day mortality rate of 60.5% in the low muscle mass cohort and 36.6% in the control cohort (p = 0.01). Finally, using TPA Francomacaro et al. showed that low muscle mass patients had higher post-operative complication rates (p < 0.0001) and based on multivariate analysis, these patients had longer length of stay (p < 0.04) and a lower rate of favorable discharge destination (p < 0.0001).
Summary of measured clinical outcomes.
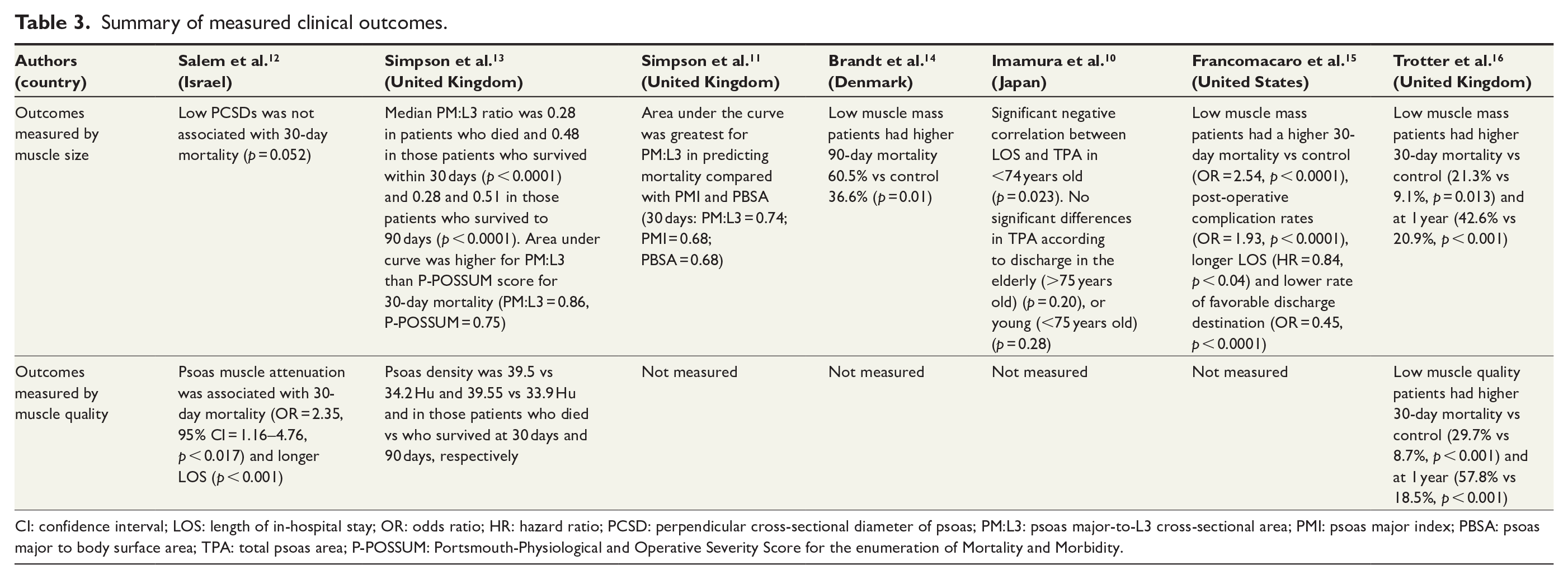
CI: confidence interval; LOS: length of in-hospital stay; OR: odds ratio; HR: hazard ratio; PCSD: perpendicular cross-sectional diameter of psoas; PM:L3: psoas major-to-L3 cross-sectional area; PMI: psoas major index; PBSA: psoas major to body surface area; TPA: total psoas area; P-POSSUM: Portsmouth-Physiological and Operative Severity Score for the enumeration of Mortality and Morbidity.
Three studies assessed muscle attenuation and associated clinical outcomes. Two of three studies showed poorer 30-day survival in low psoas attenuation groups. Salem et al. 12 showed that psoas muscle attenuation, but not PCSDs, was an independent risk factor for 30-day post-operative mortality (p < 0.017) and longer length of stay in hospital after emergency laparotomy surgery (p < 0.001). Trotter et al. 16 demonstrated that psoas density was associated with increased mortality compared with patients who had healthy muscle density at 30 days (29.7% vs 8.7%, p < 0.001).
Four studies were considered to be of high quality by scoring 7 or more on the NOS, while three studies had moderate quality by scoring between 4 and 6 (Table 4). Five studies defined muscle decline groups based on low muscle size or quality, whereas two studies assessed the relationship between muscle size and associated clinical outcomes. No article reported independent blind assessment of measured outcomes, where separate assessors were determining presence of sarcopenia and the outcomes of interest. However, the follow-up period was considered sufficient in six of seven studies, in particular where mortality outcomes were measured at or after 30 days.
Quality assessment of the included papers using the Newcastle–Ottawa Scale.
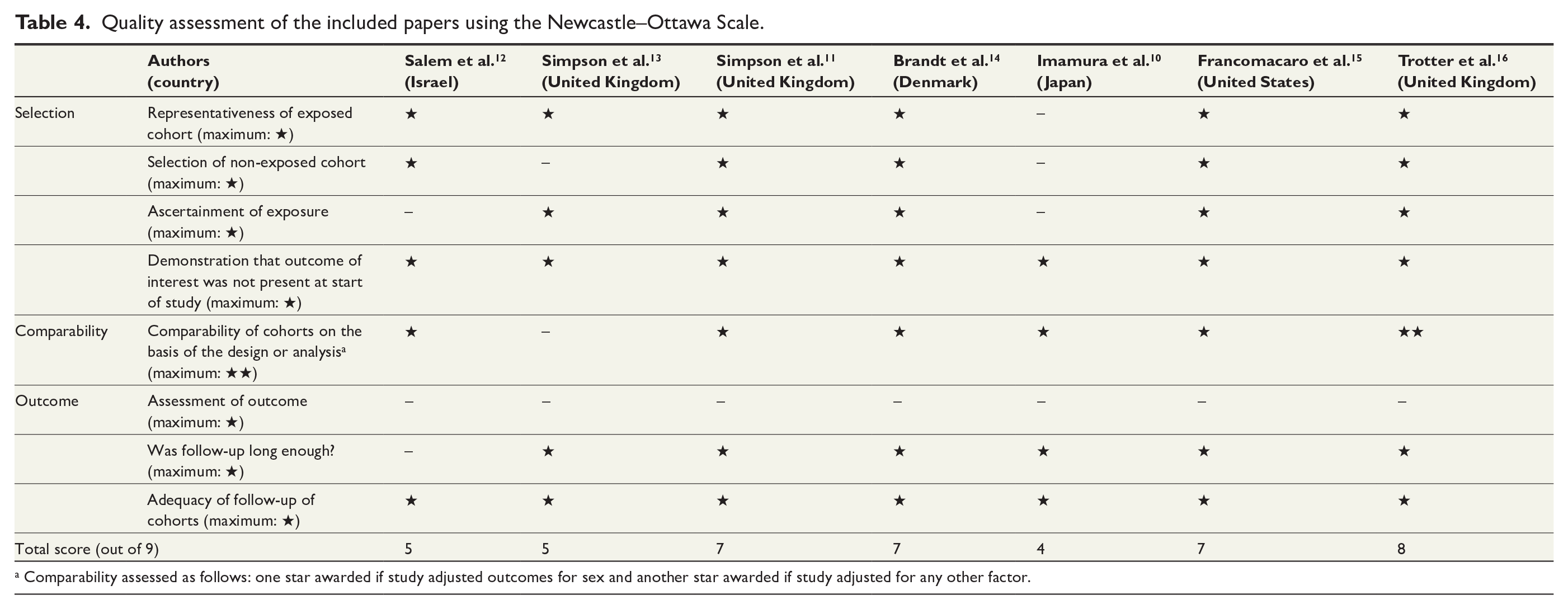
Comparability assessed as follows: one star awarded if study adjusted outcomes for sex and another star awarded if study adjusted for any other factor.
Discussion
This review has systematically appraised and summarized the literature on the use of sarcopenia markers and their predictive role in patients undergoing emergency laparotomy surgery. All studies used either muscle mass or muscle quality measurements as sarcopenia markers, which based on EWGSOP2 guidelines is an inadequate number of measured parameters to diagnose sarcopenia. 7 Measurements of low muscle mass and quality alone are, however, associated with increased 30-day mortality and poorer post-operative outcomes.
The majority of patients undergoing emergency laparotomy will receive a pre-operative CT scan to assess the underlying abdominal pathology. 17 CT scan derived sarcopenia marker detection may be a convenient and practical tool, which could be incorporated into surgical pathways, providing pre-operative predictive information. Salem et al. 12 highlight that psoas area muscle measurements are relatively easy to perform, not requiring much additional training to obtain these measurements. Future research and development of an automated software system could further standardize CT-based assessment of sarcopenia markers. Our review highlights that L3 was the most frequently used level for total abdominal muscle area measurements. Literature also shows that L3 has the highest correlation with whole-body skeletal muscle and visceral fat volumes.18–20
Five of seven studies showed association between low muscle mass and increased mortality rates after emergency laparotomy surgery and the average 30-day mortality rate in the low muscle mass group as defined by low TPA was 26.6% (SD = 25.9) compared with 13.3% (SD = 15.8) in the control high TPA groups. Brandt et al. 14 also showed a clear separation in mortality on day 30 after emergency laparotomy surgery between the investigated low and high muscle mass groups. Overall, low muscle mass was associated with poorer recovery outcomes such as increased length of hospital stay, operative complication rates and increased discharge to nursing or care homes.12,15 Simpson et al. 13 has shown that increasing ASA score like psoas major-to-L3 cross-sectional area (PM:L3) ratio was predictive of mortality and in a receiver operator characteristic tests, PM:L3 ratio had greater predictive power in assessing 30- and 90-day mortality compared to both ASA and Portsmouth-Physiological and Operative Severity Score for the enumeration of mortality and morbidity (P-POSSUM) scores. These findings are consistent with publications suggesting that muscle mass measurements are superior at predicting outcomes to ASA and Eastern Cooperative Oncology Group (ECOG) status. 21 These findings suggest that muscle mass measurements may play a role in augmentation of already existing prognostic scoring systems such as P-POSSUM and the National Emergency Laparotomy Audit (NELA) risk prediction models. 22 Further advantage of prognostic information from CT images alone is that it does not require an input of other measurements, which are unlikely to be freely available in an emergency setting (e.g. P-POSSUM). Muscle measurements may identify the most at-risk patients, they may also further guide surgical care and help select patients who may benefit from additional early post-operative interventions as proposed by the American College of Surgeons Program for Geriatric Surgery Verification.23–25
Muscle quality has been tested in various emergency surgery fields and the results suggest that it also has predictive role. 26 Only three studies in this review evaluated outcomes for patients with low muscle quality by determining low psoas muscle attenuation, albeit two of three studies showed poorer 30-day survival in low psoas attenuation groups.
All included studies were published after 2017, which explains the small number of available publications, which has contributed to several limitations in this review. There was variation in the methods used to define cut-off values for low muscle mass and quality. Park et al. review study previously analysed the effects of sarcopenia on emergency laparotomy outcomes, however we highlight the variation in sarcopenia marker cut off values and how sarcopenia was defined in each study. 27 Furthermore, most studies in our review also relied on the investigated cohort’s lowest quartile values, which in itself may be subject to sampling bias. Finally, the various country origins of the investigated suggest that the cohorts were likely composed of different ethnicities, requiring differing threshold values of sarcopenia markers. Suggested cut-off values for specific populations are reported in the literature, however what actually constitutes a different sarcopenic population is a problematic issue. 28
The variations in study design and the small number of the included studies in consequence make further synthesis of data and a meta-analysis unfeasible to conduct.29–31 Nevertheless, methodological quality of the studies using NOS was generally considered to be high. We used NOS rather than the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework, because as discussed by Luchini et al., 32 NOS is a standard tool used in systematic reviews to assess individual studies and their individual internal validity. Moreover, studies, which included small populations, were marked down in NOS representativeness of exposed cohort. Future research should assess the predictive role of muscle sarcopenia markers in larger cohort studies, which could also help set specific population-based threshold values for diagnostic criteria.
In conclusion, this systematic review highlights that the presence of sarcopenia markers including low muscle mass and low muscle quality is associated with increased 30-day mortality after emergency laparotomy surgery and that CT-based psoas muscle measurements are a potential new tool to identify the most at-risk patients, guiding their surgical care and post-operative interventions to optimize patient recovery. The nature of emergency laparotomies requires acknowledgment that precise diagnosis of sarcopenia following EWGSOP2 guidelines may not be feasible and muscle mass or muscle quality measurements alone may have to be accepted as the best alternative. The current literature on this novel topic is still scarce and heterogeneous with findings that are challenging to formulate firm conclusions. Further research will help to identify standardized and practical methods for emergency pre-operative sarcopenia detection.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221133198 – Supplemental material for Markers of sarcopenia increase 30-day mortality following emergency laparotomy: A systematic review
Supplemental material, sj-docx-1-sjs-10.1177_14574969221133198 for Markers of sarcopenia increase 30-day mortality following emergency laparotomy: A systematic review by Filip F. Brzeszczyński and Joanna I. Brzeszczyńska in Scandinavian Journal of Surgery
Footnotes
Availability of data materials
Template data collection forms, data extracted from included studies, data used for all analyses, analytics code and any other materials used in the review are not publicly available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article: No competing interests of review authors are declared.
Ethical approval
This systematic review was not registered in PROSPERO database and review protocol was not prepared.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.