
Abstract
Background and objective:
The PhysSURG-B trial of prehabilitation before breast cancer surgery randomized patients to a nonsupervised physical activity or a control group. The effects of the intervention on short- and long-term quality of life (QoL) were examined, with a subgroup analysis of patients receiving adjuvant chemotherapy.
Methods:
Female patients planned for surgery were randomly assigned to either an intervention of 30 min of self-administered physical aerobic activity daily 2 weeks before and 4 weeks after surgery or control. QoL was assessed with questionnaires at baseline, 4 weeks and 12 months postoperatively using the instruments FACT-B, RAND-36, and EQ-VAS.
Results:
Of 354 included participants at 12 months after surgery, 287 were available for analysis. FACT- B scores at 4 weeks and 12 months showed no differences between intervention compared to control, odds ratio (OR) of 0.975 (95% confidence interval (CI) 0.636–1.495) and 0.883 (95% CI 0.581–1.342), respectively. There was no difference in EQ-VAS comparing intervention to control at 4 weeks and 12 months, respectively, OR 1.163 (95% CI 0.760–1.779) and 0.817 (95% CI 0.559–1.300). RAND-36 domains “role limitations due to physical health” and “pain” showed a decrease at 4 weeks in both groups, returning toward baseline at 12 months follow-up. The subgroup who received adjuvant chemotherapy had significantly lower QoL measured using FACT-B at 12 months compared to patients not receiving chemotherapy (OR 0.475; 95% CI 0.300–0.753).
Conclusions:
An intervention of non-supervised physical activity before and after surgery for breast cancer showed no effect on short or long-term QoL, compared to control.
Trial registration:
ClinicalTrials.gov registration number: NCT 02560662.
Introduction
Breast cancer affects more than 2 million women worldwide every year. Patient-reported outcomes, such as quality of life (QoL), are important when evaluating the effect of breast cancer treatment on survivorship, where common side-effects of treatment, such as fatigue, 1 musculoskeletal pain, and stiffness 2 are known to have a negative impact on QoL. In observational studies,3–5 regular physical activity after a breast cancer diagnosis has been associated with an increased breast cancer-specific and overall survival. In patients undergoing adjuvant treatment for breast cancer, interventions with physical exercise during or after treatment have been reported to reduce fatigue6–8 and to increase QoL.9–12
Supervised exercise trials are likely more effective but have the disadvantage of sampling bias, higher cost, and limited outreach potential. 13 A systematic review showed that home- and center-based interventions for cardiac rehabilitation were comparable, 14 and another review showed a small-to-moderate positive effect on physical activity levels even from counseling. 15 Prehabilitation with physical activity before breast surgery have the potential to improve resilience against the negative impact of breast cancer treatment, and two studies have been published regarding the feasibility of prehabilitation in this setting.16,17
To our knowledge, there are no reports of any randomized trials of prehabilitation, consisting of physical activity, before breast cancer surgery which addresses short- and long-term QoL. We have previously published the results of the PhysSURG-B trial, which randomized patients to either a nonsupervised intervention with pre- and postoperative physical activity or a control group. 18 In short, the intervention did not improve the primary endpoint of recovery, neither was there any effect on complications. However, the effects on QoL could potentially be more important, and the aim of this study was to evaluate the possible effect of this intervention on the prespecified secondary outcomes of short- and long-term QoL.
Methods
Study design and setting
We report 4 weeks and 12 months follow-up data from the randomized, controlled, prospective interventional PhysSURG-B trial, evaluating an intervention of added aerobic physical activity before and after breast cancer surgery. The study protocol and primary outcome of self-reported physical recovery at 4 weeks after surgery have been published previously. 18 Participants were recruited from three surgical departments in the Western Region of Sweden between November 2016 and December 2018. Participants were randomized to intervention with nonsupervised physical activity or control.
Participants and randomization
Female patients ⩾ 18 years, diagnosed with stage I-III breast cancer, scheduled for primary surgery were randomized into two groups, intervention and control. Exclusion criteria were male sex, stage IV disease, neoadjuvant treatment, and inability to understand the study information or perform the intervention. Neither research nurses nor participants were blinded, due to the nature of the intervention, but patient allocation was not actively briefed to healthcare personnel involved in the routine care of the patient.
Intervention and control
The intervention in the PhysSURG-B trial has been described in detail previously. 18 In summary, patients in the intervention group received an individual consultation with a physiotherapist and were instructed to add 30 min of daily aerobic physical activity, 2 ±1 weeks before and 4 weeks after breast cancer surgery. The intervention was instructed to be of medium intensity resulting in shortness of breath but with the ability to talk, of the participant’s own choice after suggestions from the physiotherapist, and to be performed without supervision. In addition, two follow-up telephone calls were made during the intervention period. Added physical activity was registered in a diary. Adherence to the intervention was considered if added physical activity was registered >10 days preoperatively and >20 postoperatively. This cutoff was chosen in accordance with international guidelines for recommended physical activity. 19 The participants in the control group received brief information regarding the aim of the study, being to examine if physical activity before and after surgery improves outcome, to make an informed consent. However, the control group was not aware of the amount or duration of the intervention and was not advised regarding physical activity. All patients received standard information regarding early mobilization and shoulder movement after surgery according to routine care. The baseline level of physical activity was measured with the Saltin–Grimby Physical Activity Level Scale (SGPALS). 20
Outcome measures
Patient-reported outcome measures of QoL were secondary outcomes in the PhysSURG-B-trial, reported at three time points from which change from baseline to 4 weeks and 12 months, respectively, after surgery was calculated. The following validated instruments were used (Swedish versions):
Functional Assessment of Cancer Therapy-Breast (FACT-B), including FACT-B Total Score, FACT General (FACT-G) Total Score, and FACT-B Trial Outcome Index (TOI).
RAND 36-Item Health Survey 1.0.
EuroQol-visual analogue scale (EQ-VAS).
A single-item QoL question validated and used previously asking “How would you describe your quality of life the last month?” Answering alternatives on a scale from ”0” (worst possible quality of life) to “6” (best possible quality of life).
Sample size and statistical analysis
The sample size calculation for PhysSurg-B was performed for the primary outcome measure of physical recovery 4 weeks after surgery. No sample size calculation was performed for the secondary outcome QoL. A statistical analysis plan was written before any of the analyses were performed. The analyses were according to randomization (intention-to-treat analysis). Baseline demographic data (patient and tumor characteristics and type of surgery) were described per allocated group. Total scores and subscale scores of the QoL instruments were calculated. The scores (total score for FACT-B, EQ-VAS) had skewed and multimodal distribution making a Gaussian linear model invalid. Therefore, the effect of the intervention was estimated using an ordinal regression model. The baseline measurements were included as a covariate along with fixed factors for the study group, time, and their interaction. The single-item QoL question was dichotomized into “low QoL” (scale option 1–4) and “high QoL” (scale option 5–6) before analysis. For all instruments, the primary analysis was unadjusted. Adjuvant chemotherapy was imbalanced across the study groups, and therefore, an additional analysis of adjuvant chemotherapy was adjusted for. Also, a subgroup analysis of patients given adjuvant chemotherapy was conducted.
The results are presented as odds ratios (OR) for intervention scoring higher than the control (OR > 1) with 95% confidence intervals (CIs). All tests were two-sided and a statistical significance level of 5% was used. We made no adjustments for multiple comparisons. No imputations were made. All statistical analyses were performed with SAS® 9.4.
Ethics
The Regional ethical review board in Gothenburg, Sweden approved the trial (registration numbers 522-15, T1152-16, T700-17, T160-18). The procedures used in this study adhere to the tenets of the 1964 Helsinki declaration with amendments. Informed consent was obtained from all individual participants included in the study. PhysSURG-B was registered at ClinicalTrials.gov (NCT 02560662) 25 September 2015.
Results
The participant flow throughout the trial is visualized in Fig. 1. At 12 months after surgery, 354 of 400 participants (88.5%) remained in the trial, 44 patients had withdrawn informed consent (18 in the control group and 26 in the intervention group), and one participant in each study group had died. Of 354, 297 (84%) returned their questionnaires (return rate 83-90% for the different timepoints), with no difference seen between the study groups. Complete data for QoL assessment at all three time points was reported by 81% (287/354 participants), 148 in the control group and 139 in the intervention group, respectively.
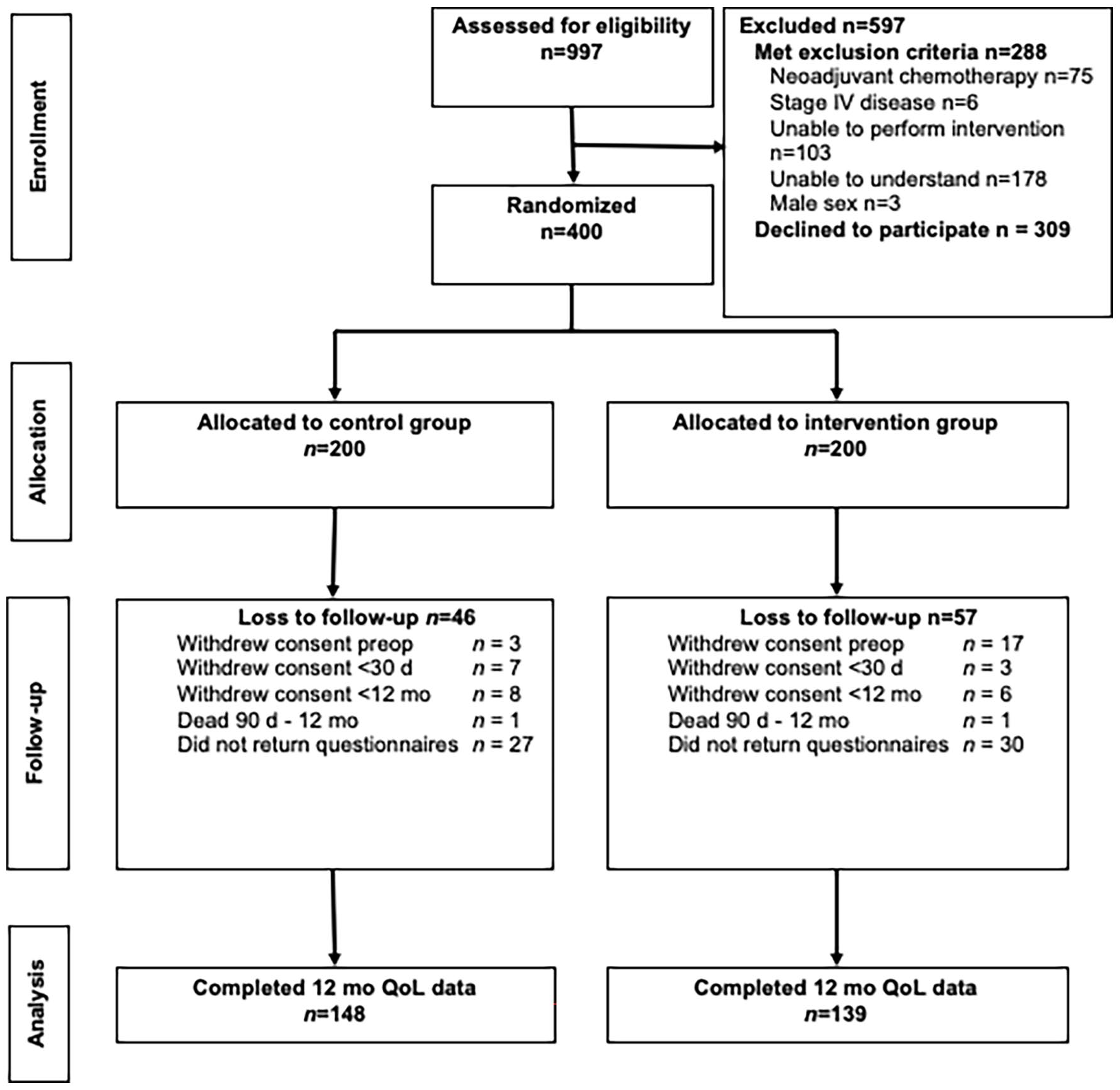
CONSORT flow diagram for the PhysSURG-B trial.
Baseline patient demographics, tumor characteristics, and type of surgery were similar in the two study groups (Table 1 and 2). Median age was 63 years (mean 62 years, range 30–89 years). More than 30% of the participants reported a risk consumption of alcohol according to Alcohol Use Disorders Identification Test (AUDIT-C), and two-thirds of the patients had at least one comorbidity where cardiovascular disease was the most frequent. The majority of patients underwent breast-conserving surgery (79%) and sentinel lymph node biopsy (95%) (Table 2). In total, 94% of the participants received any adjuvant treatment. Endocrine therapy was received by 76% in the control and 79% in the intervention groups, respectively. Radiotherapy was administered to 75% in the control and 83% in the intervention group, respectively. Adjuvant chemotherapy was given to 26% in the control compared to 37% in the intervention group. No severe adverse events related to the intervention were reported. Adherence to the intervention was less than 60% according to the physical activity diary. The physical activity level measured with SGPALS, at baseline and the end of the intervention period, showed increased physical activity in 18% of the patients in the intervention group, compared to 11% in the control group.
Baseline characteristics of study participants.
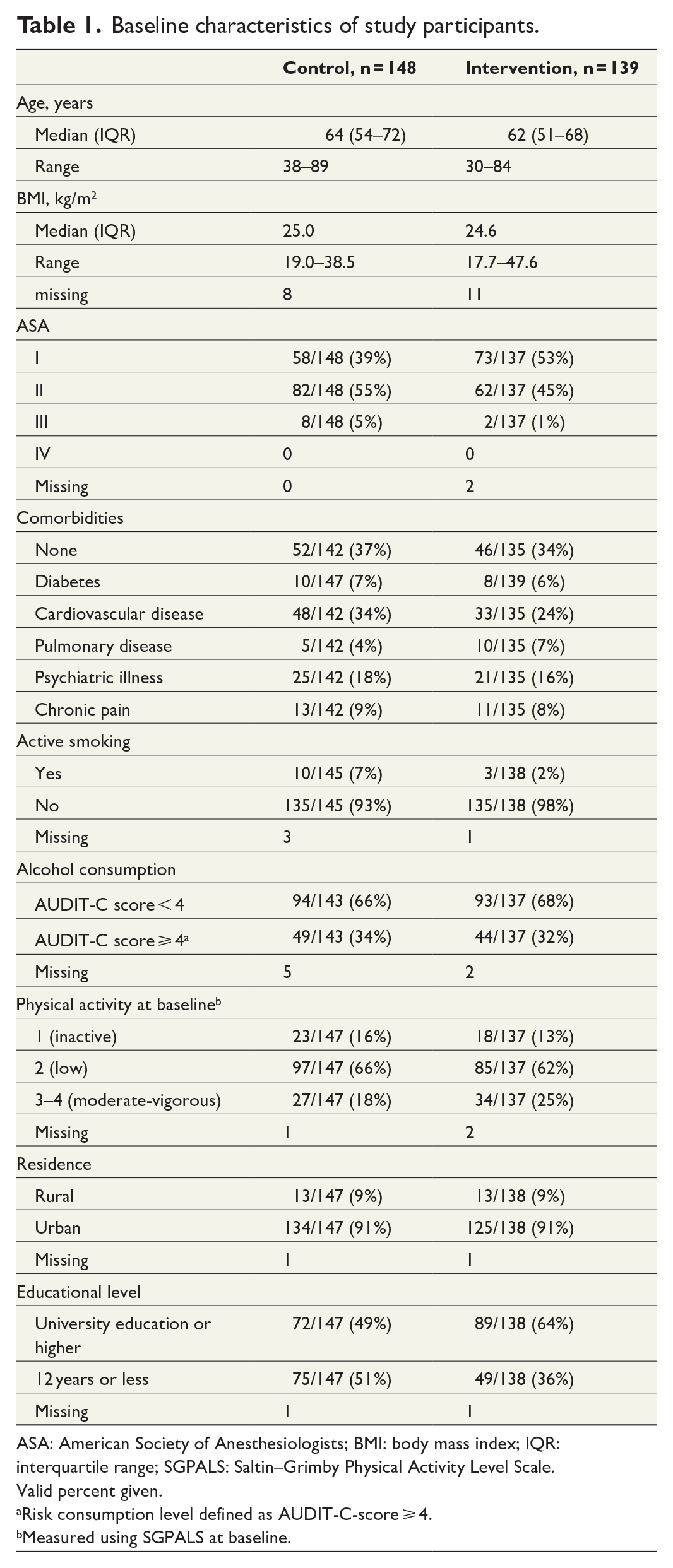
ASA: American Society of Anesthesiologists; BMI: body mass index; IQR: interquartile range; SGPALS: Saltin–Grimby Physical Activity Level Scale.
Valid percent given.
Risk consumption level defined as AUDIT-C-score ⩾ 4.
Measured using SGPALS at baseline.
Tumor characteristics and treatment.
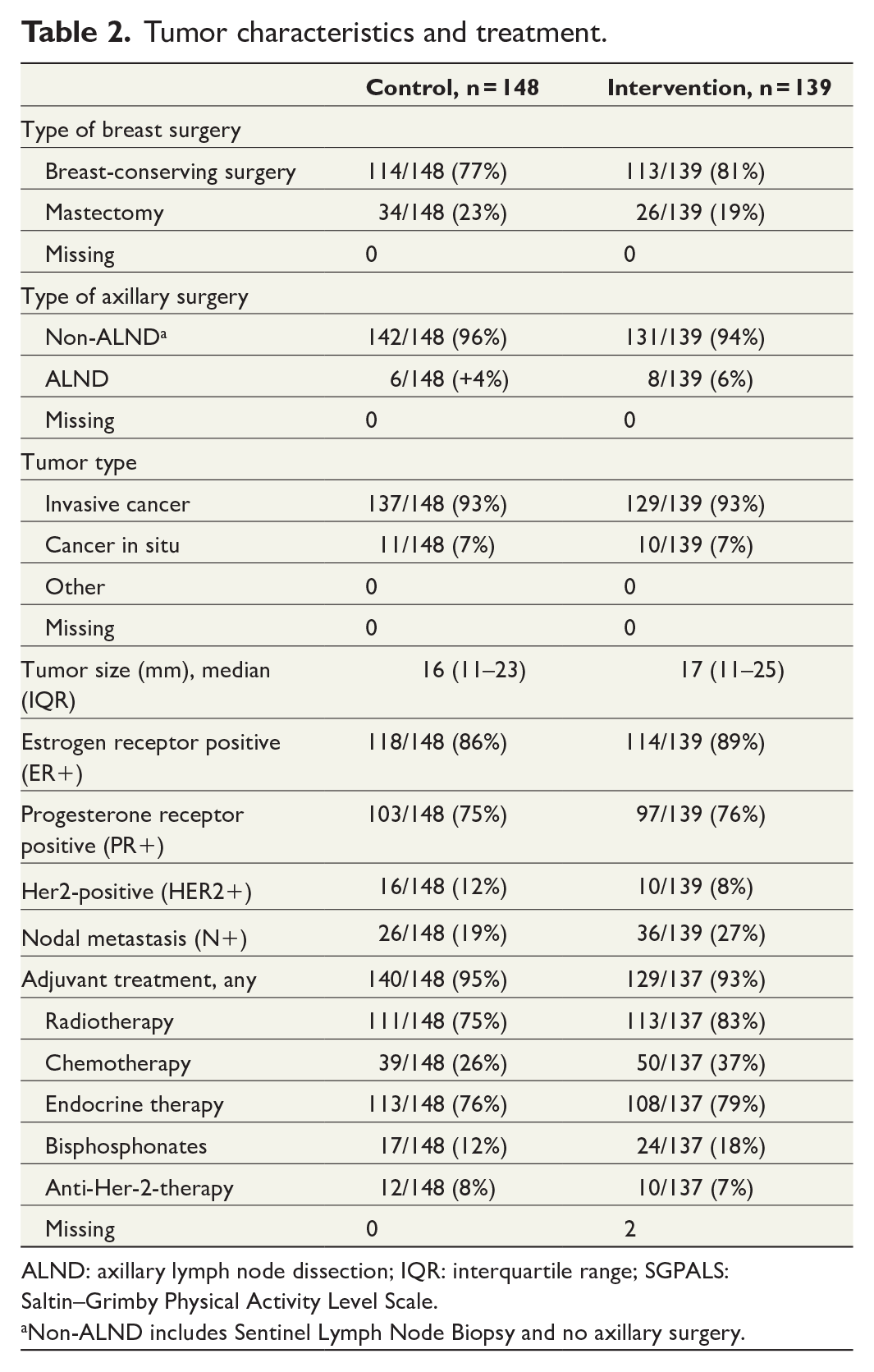
ALND: axillary lymph node dissection; IQR: interquartile range; SGPALS: Saltin–Grimby Physical Activity Level Scale.
Non-ALND includes Sentinel Lymph Node Biopsy and no axillary surgery.
FACT-B
At baseline, 4 weeks, and 12 months, the median FACT-B scores were 116.8, 121.5, and 121.9 in the control group, compared to 117.5, 121.0, and 119.1 in the intervention group (Supplementary Table 3). Comparing the intervention to the control group, the OR for FACT- B score at 4 weeks was 0.975 (95% CI 0.636–1.495) and at 12 months 0.883 (95% CI 0.581–1.342) (Table 3). When adjusted for adjuvant chemotherapy, the OR at 12 months was 0.997 (95% CI 0.654–1.520). For the subset of patients who received adjuvant chemotherapy, a significantly lower FACT-B score at 4 weeks and 12 months was seen, with an OR of 0.418 (95% CI 0.260–0.670) and 0.475 (95% CI 0.300–0.753), respectively, when compared to those who did not receive chemotherapy (Supplementary figure 1), but with no significant difference based on the study group. The FACT-G scores and the breast cancer subscales showed no difference over time or between the study groups (Supplementary Table 3). FACT-G mean baseline scores were 86.2 for control and 85.7 for intervention (median 87.8 and 87.6, respectively).
Results for FACT-B total score, EQ-VAS, and General QoL question as randomized at 4 weeks and 12 months.
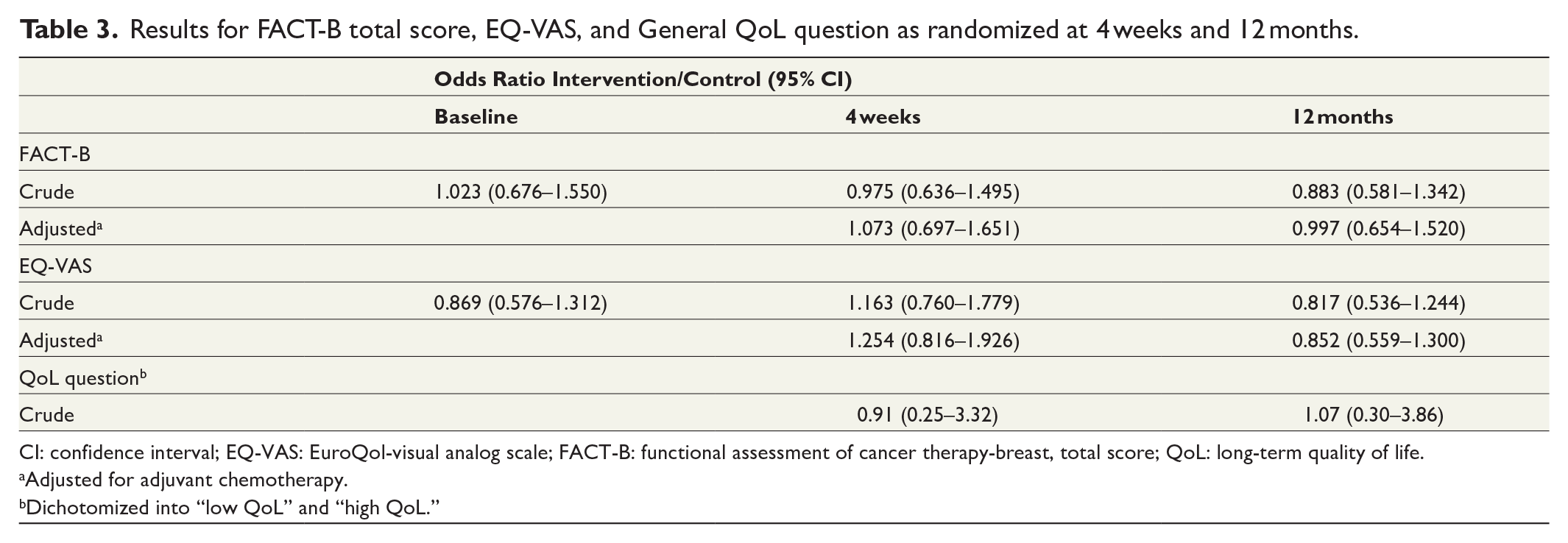
CI: confidence interval; EQ-VAS: EuroQol-visual analog scale; FACT-B: functional assessment of cancer therapy-breast, total score; QoL: long-term quality of life.
Adjusted for adjuvant chemotherapy.
Dichotomized into “low QoL” and “high QoL.”
EuroQol-visual analog scale
EQ-VAS median score was 80 at all three timepoints, and there were no differences seen between the study groups (Supplementary Table 2). During the active part of the intervention (from baseline to 4 weeks postoperative), the OR was 1.163 (95% CI 0.760–1.779) for the intervention compared to the control group. At 12 months, the OR was 0.817 (95% CI 0.536–1.244) and adjusted for chemotherapy 0.852 (95% CI 0.559–1.300) (Table 3). For all participants, regardless of the study group, given chemotherapy, the EQ-VAS at 4 weeks had an OR of 0.557 (95% CI 0.350–0.886), and at 12 months an OR of 0.656 (95% CI 0.417–1.032) compared to no chemotherapy.
RAND-36
When analyzing the RAND-36 questionnaire, there was a decline in the domains “role limitations due to physical health” and “pain” at 4 weeks postoperatively, with no difference between the study groups. At 12 months, participants had to a large extent resumed their baseline QoL (Fig. 2 and Supplementary Table 1).
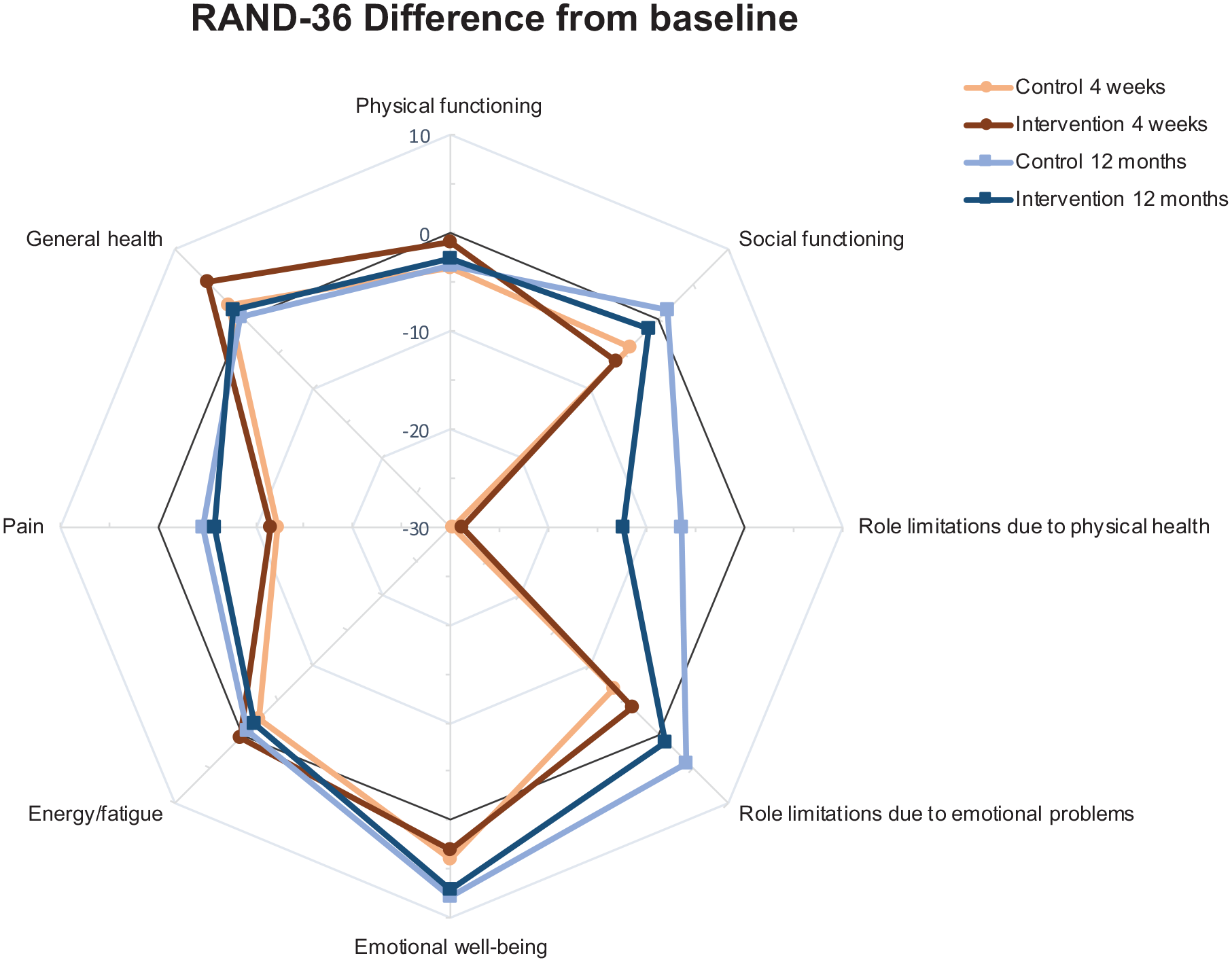
Difference from baseline to 4 weeks and 12 months as randomized for the eight domains of RAND-36.
General QoL question
Analysis of the dichotomized QoL question, “How would you describe your quality of life the last month?” resulted in no difference between the intervention and control group, neither at 4 weeks (OR 0.91, 95% CI 0.25–3.32) nor at 12 months (OR 1.07, 95% CI 0.30–3.86) (Table 3).
Discussion
The results from this randomized trial examining the effect of moderate physical activity as a prehabilitation in women undergoing breast cancer surgery did not show any effect on QoL at 4 weeks or 12 months after surgery. This may in part be explained by a high baseline level of QoL in breast cancer patients, as also seen in our trial, and difficulties to detect and/or discriminate improvements from this level. Previous studies on quality of life during adjuvant treatment12 have primarily investigated effects following supervised, high-intensity exercise interventions for a longer period of time.8 Even with such intense exercise interventions, significant improvements in quality of life have not been reported. 8 Our results, showing that 12 months after surgery, most patients returned to their baseline level of QoL, are regarded reassuring.
The aim of our trial was to investigate the effect of a simple nonsupervised intervention, in keeping with national and international recommendations regarding physical activity for the general population. 19 The intervention was designed based on two primary aims. The first aim was to design an intervention with a high external validity, being easily implementable in the care pathway for breast cancer treatment with a minimum of economic and organizational impact. Most studies so far have used extensive supervised physical exercise programs with limited possibility of implementation in routine health care, where specifically organizational matters have been identified as main barriers. 21 Second, we aimed to investigate the effect of introducing the intervention at the time of diagnosis. We considered the interval between diagnosis and start of treatment a window-of-opportunity for changes in habits, as described, 22 and an opening for increased physical activity. However, the results showed a very modest increase in physical activity, 18% of the patients in the intervention group compared to 11% in the control group. This is important information when designing future trials, where even more research is needed on how to motivate patients to increase their levels of physical activity.
The duration of physical activity is another important factor to consider. Ideally, a phase of prehabilitation should probably be longer than 2–3 weeks; however, this is less feasible in patients scheduled for cancer treatment where waiting time for treatment should be kept short. Also, the intensity of physical activity, and whether it is supervised or not, are important factors. Previous studies showed that a higher volume of exercise did not necessarily give a greater effect. Aerobic training for 300 min/week did not lead to a better result than the public health recommendation of 150 min/week, the same recommendation that is the base for the intervention in this trial. 23 Yet another trial showed that there was no difference between a higher volume of combined aerobic and resistance training for 50–60 min and a lower volume of only aerobic training for 25–30 min in a general breast cancer population. 24
The FACT-G score in our trial cohort revealed a higher level of QoL, with a mean baseline score of 86, compared to 77 in the normative data for the general Swedish female population sample (pro-rated mean FACT-GP scores). 25 The FACT-G minimally important difference (MID) is considered to be approximately 5–6 in a breast cancer population, with a MID 7–8 for the total FACT-B score. 26 The higher FACT-G score in our sample of breast cancer patients could suggest a sampling bias, where individuals with lower QoL declined participation. Another possible explanation is the difference in age distribution in our study sample (mean 62 years) compared to the previously published population sample with a mean age of 49 years,25 as a higher age was positively correlated to higher FACT-GP score. Moreover, the FACT-G and FACT-B scores that we present are similar to previously published results for breast cancer patients.27–29 Over time, the FACT-B scores were stable regardless of the study group and treatment factors, except for the subgroup of patients receiving adjuvant chemotherapy, where a significant decline was seen. Interestingly, this was not only seen at 12 months but also at 4 weeks, when the participants had not yet started their adjuvant chemotherapy but had gained information about the projected start of treatment.
EQ-VAS median scores were stable regardless of the study group and time for assessment, and all changes seen in mean scores were less than the MID of 8 suggested for EQ-VAS. 30 RAND-36 showed a temporary decline in the domains “Pain” and “Role limitations due to physical health” at 4 weeks, these changes were not seen at 12 months where participants had resumed their QoL. Interestingly, the domain “Emotional well-being” showed even better results at 12 months compared to baseline, possibly as a result of improved adaptive strategies and response shift over time. The domain “General health” improved during the active intervention period at 4 weeks after surgery, but at 12 months returned to baseline.
The consistency in FACT-B and EQ-VAS scores from baseline to 4 weeks after surgery could indicate an inability of the instruments to encompass or discriminate changes resulting from the surgical insult, or that breast cancer diagnosis and surgery alone in fact has low impact on QoL. A significant difference was only seen for patients receiving adjuvant chemotherapy, compared to patients not receiving adjuvant chemotherapy, suggesting that this is a subgroup of patients that may benefit more from interventions aimed at improving QoL.
The strengths of the current study include the randomized controlled design, the use of several validated QoL instruments, both generic and disease-specific, as well as both short- and long-term follow-up. Limitations include the lack of objective measures of physical activity regarding type, duration, and/or intensity. Low adherence to the intervention, restrict the effects of this nonsupervised intervention and point to the drawbacks of recommendations regarding exercise, in line with previous studies.8,31 In addition to the reported intention-to-treat analyses we have also performed per-protocol analyses (not reported) with similar results. Our results, in accordance with previous findings seem to suggest the need for improved strategies and additional support to achieve the recommended physical activity level for patients with breast cancer.
Based on our results and previously presented outcomes of this trial, we cannot advocate for including unsupervised physical activity in prehabilitation guidelines for patients awaiting surgery for breast cancer. Based on the findings from this trial, one of the most important aims for future prehabilitation research is to identify implementable interventions that will improve the outcome. Also, the knowledge gained from this trial concerning QoL before and after breast cancer treatment, using different questionnaires, gives additional support for future research.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221123389 – Supplemental material for The effect of nonsupervised physical activity before and after breast cancer surgery on quality of life: Results from a randomized controlled trial (PhysSURG-B)
Supplemental material, sj-docx-1-sjs-10.1177_14574969221123389 for The effect of nonsupervised physical activity before and after breast cancer surgery on quality of life: Results from a randomized controlled trial (PhysSURG-B) by Jenny Heiman, Aron Onerup, David Bock, Eva Haglind and Roger O. Bagge in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We extend our gratitude to the participants in the PhysSURG-B trial, the physiotherapists involved in the intervention, as well as the research nurses and all personnel involved in conducting the trial at the including hospitals.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jenny Heiman, Eva Haglind, and Roger Olofsson Bagge. The first draft of the manuscript was written by Jenny Heiman and all authors commented, read, and approved the final manuscript.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Sahlgrenska University Hospital (ALFGBG-4307771, ALFGBG-718221), AFA Insurance (150072), The Swedish Cancer Society (CAN 2016/362, 2020/ 19 0303), The Gothenburg Medical Society (GLS 779001, GLS 879101), Lions Cancer Research Fund of Western Sweden (LCV2018:28), Anna-Lisa and Bror Björnssons Foundation and Knut and Alice Wallenberg Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.