
Abstract
Background and objective:
In this clinical trial, we evaluated if a short-acting nucleoside, adenosine, as a high-dose bolus injection with blood cardioplegia induces faster arrest and provides better myocardial performance in patients after bypass surgery for coronary artery disease.
Methods:
Forty-three patients scheduled for elective or urgent coronary artery bypass grafting were prospectively recruited in two-arm 1:1 randomized parallel groups to either receive 20 mg of adenosine (in 21 patients) or saline (in 22 patients) into the aortic root during the first potassium-enriched blood cardioplegia infusion. The main outcomes of the study were ventricular myocardial performance measured with cardiac index, right ventricular stroke work index, and left ventricular stroke work index at predefined time points and time to asystole after a single bolus injection of adenosine. Conventional myocardial biomarkers were compared between the two groups at predefined time points as secondary endpoints. Electrocardiographic data and other ad hoc clinical outcomes were compared between the groups.
Results:
Compared with saline, adenosine reduced the time to asystole (68 (95% confidence interval (95% CI) = 37–100) versus 150 (95% CI = 100–210) seconds, p = 0.005). With myocardial performance, the results were inconclusive, since right ventricular stroke work index recovered better in the adenosine group (p = 0.008), but there were no significant overall differences in cardiac index and left ventricular stroke work index between the groups. Only the post-cardiopulmonary bypass cardiac index was better in the adenosine group (2.3 (95% CI = 2.2–2.5) versus 2.1 (95% CI = 1.9–2.2) L/min/m2, p = 0.016). There were no significant differences between the groups in cardiac biomarker values.
Conclusions:
A high dose adenosine bolus at the beginning of the first cardioplegia infusion resulted in significantly faster asystole in coronary artery bypass grafting patients but enhanced only partially the ventricular performance.
EudraCT number: 2014-001382-26. https://www.clinicaltrialsregister.eu/ctr-search/trial/2014-001382-26/FI
Keywords
Context and relevance
Fast termination of contractions is essential for preservation of myocardial performance during cardiac surgery. Only few studies have tried to explore this in depth in atherosclerotic hearts. In this randomized feasibility trial, we could show that with a high enough (20 mg) single dose of adenosine, a faster induction of asystole was achieved, and combined with potassium-enriched blood cardioplegia, it provided significantly better myocardial function in the postoperative right ventricle in coronary artery bypass grafting (CABG). However, it did improve cardiac index (CI) or left ventricular stroke work index (LVSWI) only in the immediate recovery. This study emphasizes the importance of fast cessation of myocardial work in protection of the myocardium, especially in the right ventricle.
Introduction
Fast induction of cardiac arrest with potassium-enriched blood cardioplegia could be beneficial for the oxygen consumption of ischemia-prone hearts. Adenosine, a nucleoside compound, has been shown to produce fast cessation of ventricular contractions, but information regarding the efficacy of adenosine added to initial blood cardioplegia to assist in stopping the heart in coronary artery bypass surgery rests mainly in findings derived from a single study 1 in which a smaller adenosine bolus of 3 mg with a limited hemodynamic follow-up was used. Findings of other studies with adenosine in crystalloid cardioplegia indicate higher postoperative cardiac index (CI) and reduced need for inotropes after coronary artery bypass grafting (CABG) and a lower release of troponin I after valve surgery and CABG.2,3 In addition to an improved CI, Chauhan et al. observed lower creatine kinase MB (CK-MB) subunit values in CABG patients who received an adenosine bolus and crystalloid cardioplegia to the aortic root after aortic cross-clamping. 4 In their open randomized controlled trial, Maddali et al. witnessed initially higher CI, stroke volume, and stroke index as well as earlier recovery of sinus rhythm in patients receiving a 3 mg adenosine bolus to the aortic root just before the first cardioplegia. 1 Interestingly, when administered continuously during blood cardioplegia, adenosine did not enhance cardioprotection in aortic valve replacement patients, as evaluated by myocardial enzyme release, adenine nucleotide, and oxygen/lactate metabolism or hemodynamic performance. 5 The effects of adenosine may derive also from the shorter times to asystole, which have been recorded when adenosine was given at cardioplegic induction.1–6 To the best of our knowledge, only five randomized trials1,3,4,7,8 have been performed to study the effects of adenosine bolus at the beginning of the first cardioplegia in CABG patients, but in only two series, blood cardioplegia was used in both groups.1,7,8 In these reports, only Maddali et al. 1 measured the time to asystole after adenosine bolus, but their open study did not use placebo.
The present randomized placebo-controlled study aimed to investigate whether a 20 mg adenosine bolus into the aortic root at the beginning of the first cardioplegia infusion could provide a faster cardiac arrest and higher level of myocardial protection, as measured directly during surgery and in the early postoperative phase.
Methods
Hypothesis
Based on previous findings, we hypothesized that intra-aortic adenosine bolus at the beginning of the first potassium-enriched blood cardioplegia infusion could improve myocardial protection and induce faster cardiac arrest. A rapid cessation of myocardial work and the vasodilative properties of adenosine could result in more effective cardioplegia distribution into the myocardium in diastolic arrest and thus provide better preservation of the myocardial function.
Trial design
A randomized, double-blind, placebo-controlled superiority clinical feasibility trial was carried out in the Heart Hospital, Tampere University Hospital, Tampere, Finland, a tertiary referral center, between November 2015 and March 2018. The study protocol was inspected and approved by the National Committee of Medical Research Ethics and by the Tampere University Hospital Ethics Committee (license number ETLR14065M) and was reviewed by the Finnish Medicines Agency. The study was registered in the European Union Drug Regulating Authorities Clinical Trials Database (EudraCT number 2014-001382-26) before initiation and patient enrolment. All enrolled patients gave written informed consent for participation in the study. The ethical principles of the 1964 Declaration of Helsinki were followed.
Patients
The inclusion criterion was elective or urgent on-pump CABG for coronary artery disease with no additional cardiac procedures. The exclusion criteria were prior heart surgery, preoperative ejection fraction below 40%, severe renal impairment, implanted cardiac pacemaker, severe aortic regurgitation, a critical medical condition, and inability to use antegrade cardioplegia. All study procedures were programmed on elective basis and were performed in the morning (anesthesia preparations starting at 7:45 a.m. and the surgical procedure approximately at 8:45 a.m.). The CONSORT flow diagram is attached as Fig. 1.
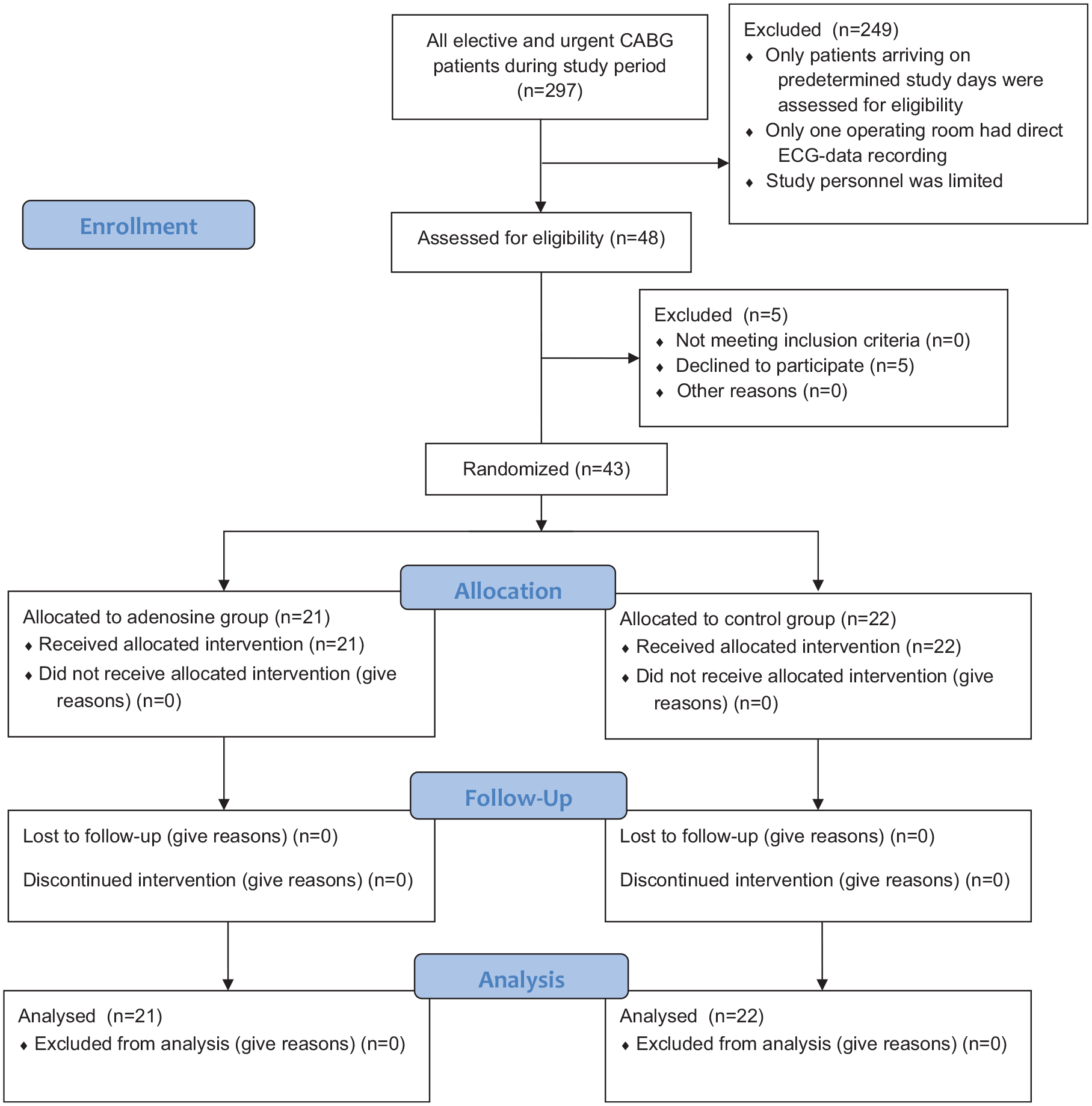
The CONSORT flow diagram.
Randomization
The patients enrolled by the research group were randomized into two arms (1:1 to the adenosine and control groups) using an unblocked randomization scheme for 43 patients. Randomization was based on computer-generated digits. Sealed non-transparent envelopes containing the study group information were produced by the research administrator, who was not involved in patient selection or the operation. This information was viewed only by a surgical nurse, who then prepared the study medication in an unlabeled syringe and delivered it to the scrub nurse to be used after aortic cross-clamping. The surgical and anesthesiologic teams were blinded to the study group information.
Interventions
All patients underwent the CABG operation with no additional cardiac procedures. The operations were performed through a midline sternotomy using cardiopulmonary bypass (CPB). The locations of anastomoses and the number and type of grafts were at the surgeon’s preference. Distal anastomoses were constructed first, and proximal anastomoses last before the de-clamping of the aorta. The left internal thoracic artery was used in situ. The anesthesia and CPB protocols are explained in Supplement 1.
All patients received cold potassium-enriched blood cardioplegia. The initial dose was 1200 mL to the aortic root, followed by doses of 300 mL after each completed coronary anastomosis. The volume of the final warm cardioplegia infusion was 600 mL. The characteristics of blood cardioplegia in the study groups are presented in Supplement 2.
In the adenosine group, 4 mL (20 mg) of adenosine (Adenosin Life Medical 5 mg/mL, Life Medical Sweden AB, Stockholm, Sweden) was injected into the aortic root by the operating surgeon after cross-clamping of the ascending aorta at the beginning of the first antegrade cardioplegia infusion. The dosage was based on our earlier studies.7,8 In the control group, 4 mL of saline (Natriumchlorid Braun 9 mg/mL, B. Braun Melsungen AG, Melsungen, Germany) was injected at the same time point in a similar fashion. Blood cardioplegia infusion started immediately after cross-clamp placement to fill the aortic root, and either adenosine or saline was injected into the aortic root cardioplegia cannula in 5 s.
Arterial blood samples were collected from the radial cannula before the surgical incision, 15 min after the de-clamping of the aorta, at 7 p.m. and at 6 a.m. on the first postoperative morning in the intensive care unit (ICU). Plasma concentrations of CK, CK-MB, and Troponin T (TnT) were measured from these samples. After anesthesia induction, a Swan-Ganz thermodilution catheter was inserted into the pulmonary artery, and hemodynamic measurements were recorded before incision, immediately after weaning from CPB in a stabile phase, at 7 p.m. and at 6 a.m. on the first postoperative morning in the ICU. Careful optimization of the hemodynamic status was achieved using institutional hemodynamic care guidelines in the operating room and in the ICU. CI at least 1.8 L/min/m2 and blood lactate < 1.7 mmol/L were the goal of treatment. Inotropic medication was used only after the targeted values for preloading the heart (central venous pressure (CVP) = 10–15 mmHg, pulmonary capillary wedge pressure = 12–18 mmHg) and for hematocrit > 0.25 were achieved.
A laptop computer was used to record the patients’ electrocardiogram (ECG) for the duration of the operation with the Datex Ohmeda S5 Collect software (Datex-Ohmeda, Inc., Madison, WI, USA). The time to the first asystole was measured from the study medicine injection to cardiac standstill. The first asystole was defined as the cessation of the electrical activity of the heart for 10 s. A restart of cardiac activity was defined as the return of any myocardial activity within 1 min of cessation. Asystole was defined as a state where the first asystole remained for more than 1 min or, in the case of a restart, the second asystole remained for more than 30 s. The classification of cardiac rhythm after aortic declamping was as follows: (1) supraventricular (sinus rhythm, atrial fibrillation, and junctional rhythm with narrow QRS complexes (QRS deflections in the ECG)), (2) ventricular (broad QRS and no atrial activity), and (3) bradyarrhythmia (pacemaker rhythm and grade III atrioventricular block).
Study outcomes
The main objective of the trial was to compare cessation of the myocardial contractions and to evaluate myocardial function between the study groups. The predefined primary outcomes were the time to cardioplegic asystole and the difference in ventricular cardiac performance (as measured with CI, left ventricular stroke work index (LVSWI) and right ventricular stroke work index (RVSWI)). The secondary predefined outcomes were plasma concentrations of cardiac biomarkers such as creatine kinase (CK), CK-MB, and TnT. As post hoc outcomes, we compared clinical outcomes, intraoperative ECG data, additional hemodynamic measurements, and adverse outcomes between the study groups.
Statistical methods
Sample size was evaluated prior to the study with the expected superiority difference in CI of 0.25 L/min/m2 (with two-sided standard deviations (SD) of 0.25) at the earliest time point after baseline (i.e., post-CPB CI) and for a 15-s difference in the cessation of myocardial contractions (with two-sided SD of 15 s). These calculations resulted in 16 patients (for CI) and 9 patients (in cessation of contractions) required for each study group. Taking possible dropout into account, we decided to randomize a minimum of 20 patients to each study group. Actual mean values with SD observed in our previous investigations were used for sample size calculation. We aimed at a type I error level of .05 and the desired power of .80. Statistical analyses were performed comparing normally distributed continuous variables with the independent samples t test, and the Mann–Whitney U test was applied for non-normally distributed continuous variables. Categorical variables were compared using Fisher’s exact test or Pearson’s chi-square test. Two-way repeated-measures analysis of variance (ANOVA) was used for comparing continuous variables of hemodynamic parameters and serial blood samples between the groups at multiple time points. Greenhouse–Geisser correction was used for non-sphericity, and Bonferroni correction was used for multiple testing. A p value of less than 0.05 was considered significant. The 95% confidence interval (95% CI) was used as an indicator of variation. Statistical analysis was performed using SPSS software (IBM Corp. Released 2017. IBM Statistics for Macintosh, Version 25.0. Armonk, NY: IBM Corp.). Statistical analysis plan is attached as Supplement 3.
Results
During the study period, 297 elective and urgent CABG patients were operated in our unit, from which we included 48 into the study according to inclusion and exclusion criteria. We could schedule study patients irregularly depending on the availability of study personnel and limitation of single operating room equipped with technology for continuous ECG tracking and saving. Therefore, only 48 patients scheduled for pre-determined study days were assessed for eligibility, thus prolonging the study data collection period. Patients eligible to the study were given the first available study operation date. No other selection occurred if patient gave an informed consent to participate. Allocating patients to operating rooms was done by an administrative surgeon, who was not involved in the study, and when research staff was available, patients were assessed for eligibility. Five patients declined to participate. Total of 43 patients were randomized to study groups, and none of them withdrew their consent. All 43 patients completed their allocated treatment with no crossover between the groups. All patients were included in the analysis until the end of the trial time on the first postoperative morning. The trial inclusion ended when all the intended patients had been operated and the data had been obtained. To test our study population’s representativeness of the remaining 254 operated patients, we compared their characteristics and outcomes in Supplementary Table 1. There were no statistically significant differences in preoperative characteristics between the study groups (Table 1). No patient had aortic regurgitation classified as moderate.
Patient characteristics.
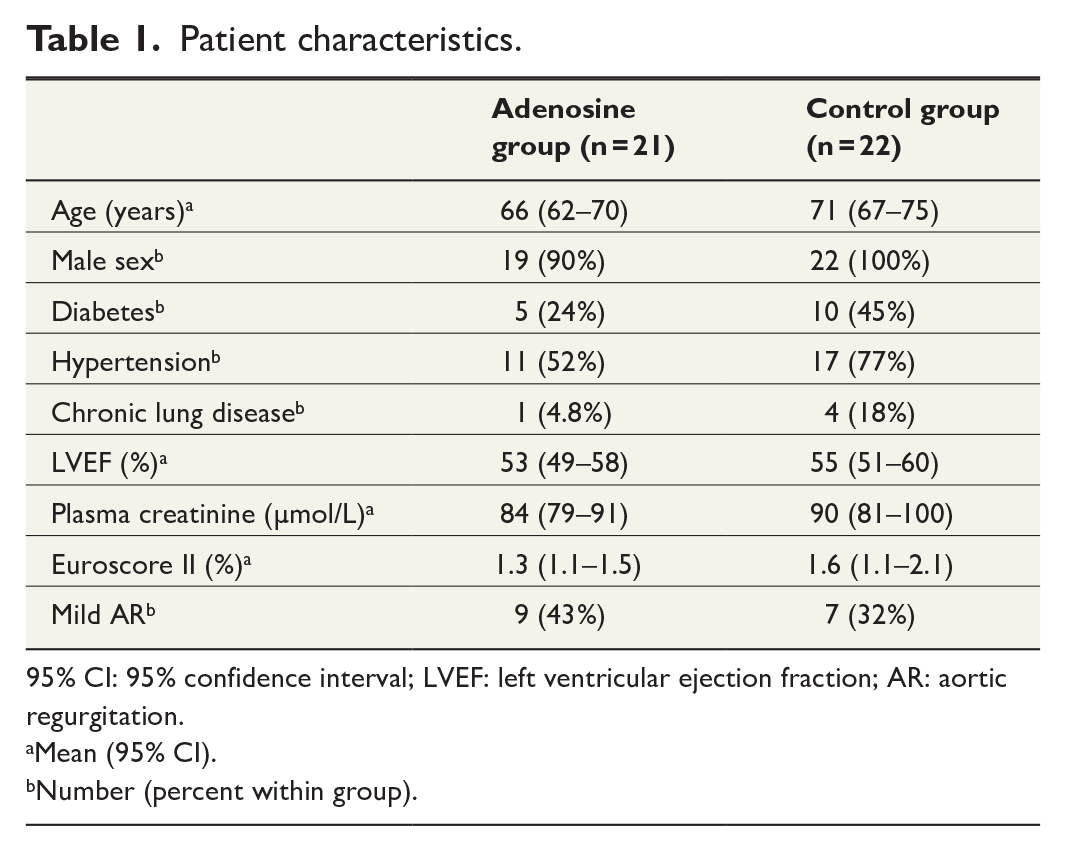
95% CI: 95% confidence interval; LVEF: left ventricular ejection fraction; AR: aortic regurgitation.
Mean (95% CI).
Number (percent within group).
Adenosine treatment had no statistically significant overall effect on CI; although in time-related pairwise assessments corrected for the multiple comparisons, CI was statistically significantly higher immediately after CPB in the adenosine group. Primary outcome hemodynamic measurements of CI, RVSWI, and LVSWI are presented in Table 2.
Primary outcome hemodynamic measurements.
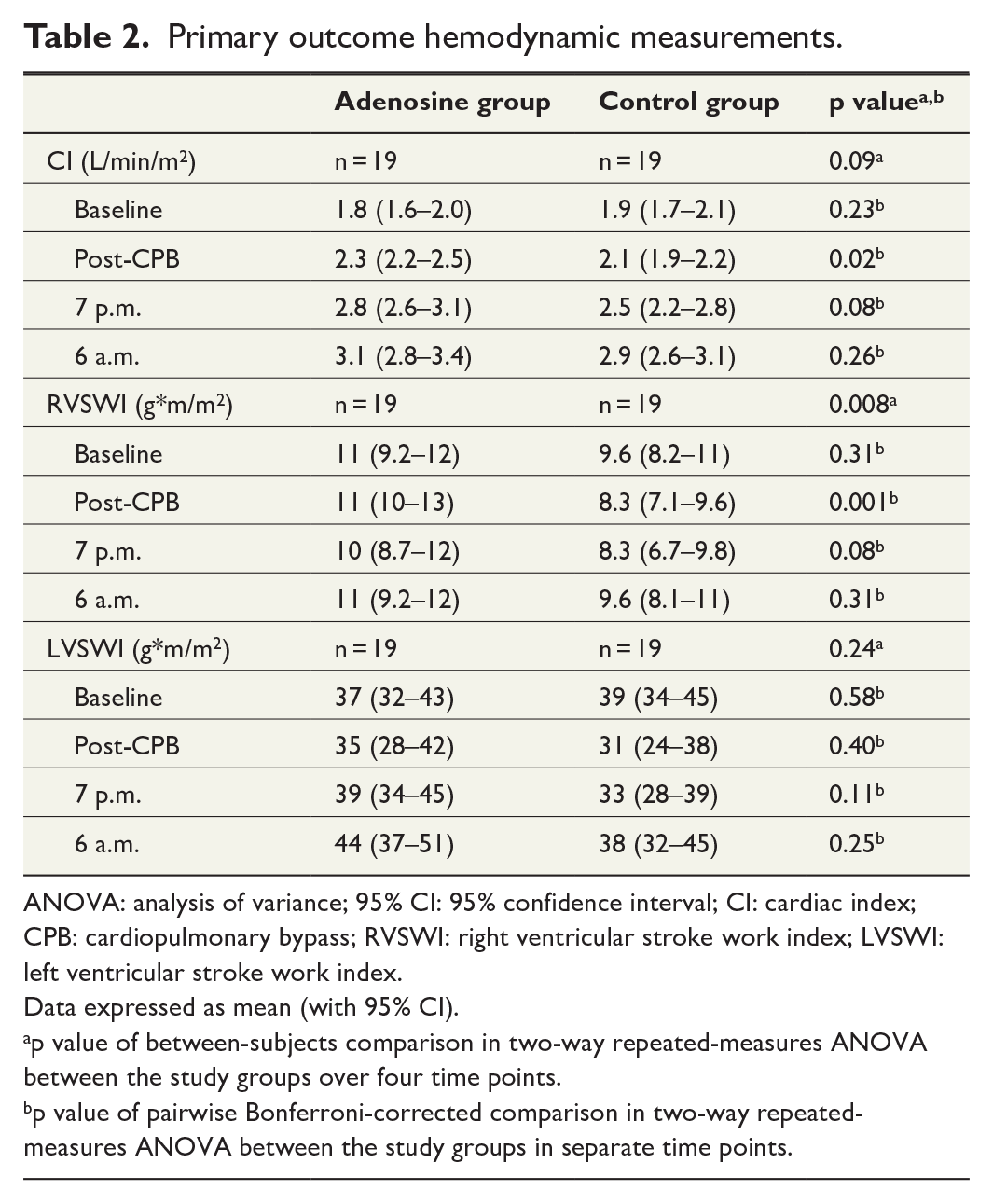
ANOVA: analysis of variance; 95% CI: 95% confidence interval; CI: cardiac index; CPB: cardiopulmonary bypass; RVSWI: right ventricular stroke work index; LVSWI: left ventricular stroke work index.
Data expressed as mean (with 95% CI).
p value of between-subjects comparison in two-way repeated-measures ANOVA between the study groups over four time points.
p value of pairwise Bonferroni-corrected comparison in two-way repeated-measures ANOVA between the study groups in separate time points.
The time to asystole was significantly faster in the adenosine group (68 s (95% CI = 37–100) versus 150 s (95% CI = 100–201), p = 0.005) although there was a high restart rate in the adenosine group (13 (62%) versus 5 (23%) patients, p = 0.009) after the first asystole (15 s (95% CI = 7–24 s) versus 122 s (95% CI = 80–165 s), p < 0.001) which was also significantly faster in the adenosine group.
Adenosine treatment improved post-perfusion right ventricular contractility with a statistically significant overall effect on RVSWI in the repeated-measures ANOVA. The adenosine group also had slightly higher LVSWIs at three time points after surgery, but the main result in the repeated-measures ANOVA was not statistically significantly different from the control group.
Cardiac biomarker levels remained low, and there were no statistically significant differences in the plasma concentrations of CK, CK-MB, or TnT between the study groups in the two-way repeated-measures ANOVA (Table 3).
Cardiac biomarkers.
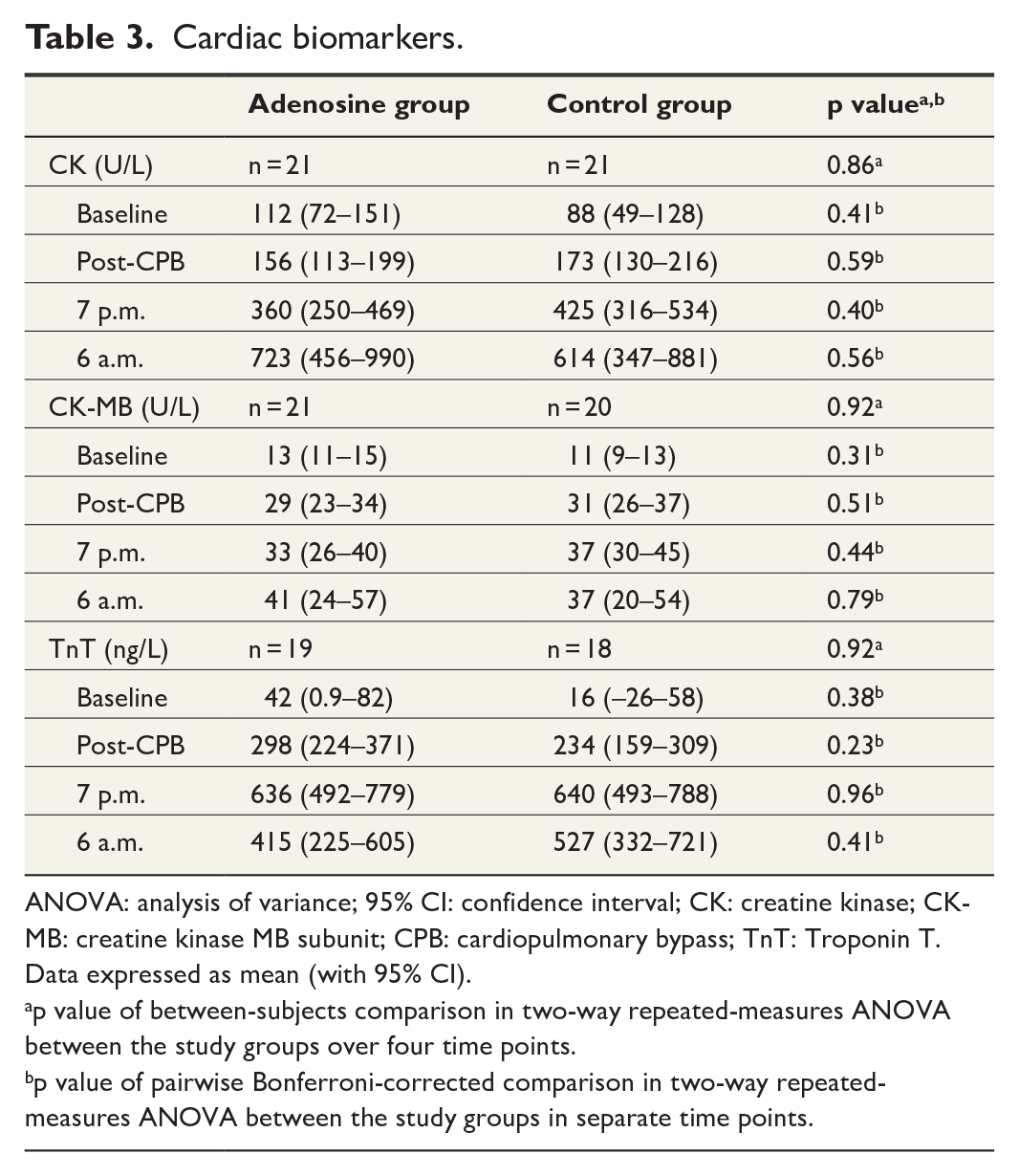
ANOVA: analysis of variance; 95% CI: confidence interval; CK: creatine kinase; CK-MB: creatine kinase MB subunit; CPB: cardiopulmonary bypass; TnT: Troponin T.
Data expressed as mean (with 95% CI).
p value of between-subjects comparison in two-way repeated-measures ANOVA between the study groups over four time points.
p value of pairwise Bonferroni-corrected comparison in two-way repeated-measures ANOVA between the study groups in separate time points.
The parameters of the two-way repeated-measures ANOVA are summarized in Supplementary Table 2. No significant interactions between the hemodynamic measurements over time and the study group were observed. We investigated for potential correlations between preload or heart rate (HR) but could not find any significant correlation between CI and HR or CI and CVP after weaning from CPB or early in the ICU in either of the study groups (Supplementary Table 3).
In 12 patients (28%), the surgery was urgent and in 31 (72%) elective, but this did not influence the CI; baseline: 1.9 (95% CI = 1.6–2.1) versus 1.8 (95% CI = 1.7–2.0) L/min/m2, post-CPB: 2.2 (95% CI = 2.0–2.4) versus 2.2 (95% CI = 2.1–2.3) L/min/m2, 7 p.m.: 2.4 (95% CI = 2.1–2.8) versus 2.7 (95% CI = 2.5–3.0) L/min/m2, 6 a.m.: 2.7 (95% CI = 2.3–3.1) versus 3.1 (95% CI = 2.8–3.3) L/min/m2, p = 0.16, in urgent and elective groups, respectively. Urgent status did not influence the RVSWI either; baseline: 9.9 (95% CI = 8.0–12) versus 10 (95% CI = 9.0–11) g*m/m2, post-CPB: 11 (95% CI = 8.8–13) versus 9.6 (95% CI = 8.4–11) g*m/m2, 7 p.m.: 9.2 (95% CI = 6.9–11) versus 9.3 (95% CI = 8.0–11) g*m/m2, 6 a.m.: 10 (95% CI = 7.8–12) versus 10 (95% CI = 9.0–12) g*m/m2, p = 0.89, in urgent and elective groups, respectively.
Post hoc outcomes
There were no differences in clinical outcomes between the study groups (Table 4). Excluding the restart of cardiac activity after the first asystole and times to first and final asystole, there were no significant differences in intraoperative ECG data between the groups (Table 5). No differences were found in post hoc hemodynamic outcomes (Table 6). Because this was an intervention study with a pharmacological agent, adverse events during hospital stay were compared between the study groups, and no statistically significant differences were found (Supplementary Table 4).
Clinical outcomes.
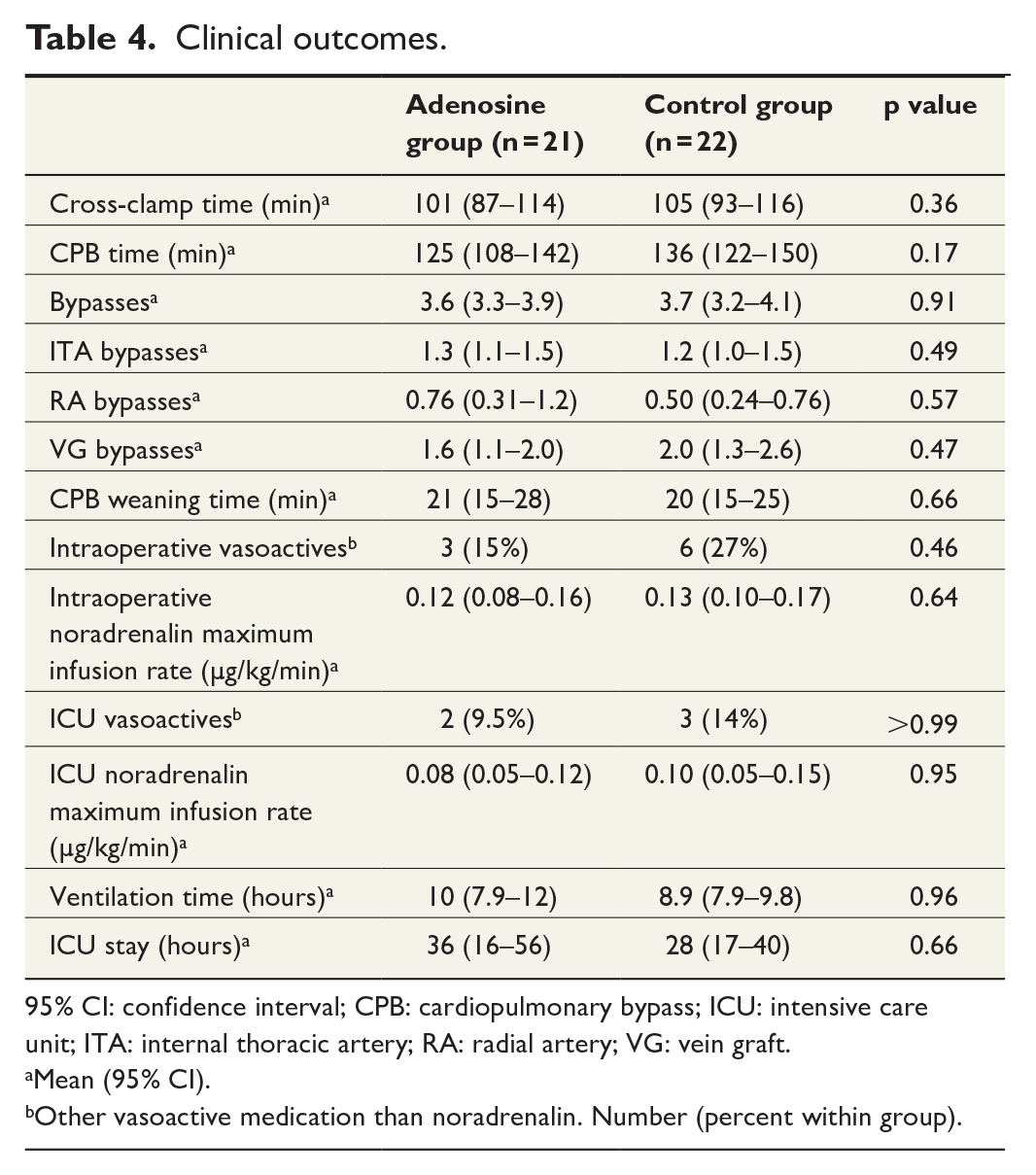
95% CI: confidence interval; CPB: cardiopulmonary bypass; ICU: intensive care unit; ITA: internal thoracic artery; RA: radial artery; VG: vein graft.
Mean (95% CI).
Other vasoactive medication than noradrenalin. Number (percent within group).
Intraoperative ECG data, post hoc analysis.
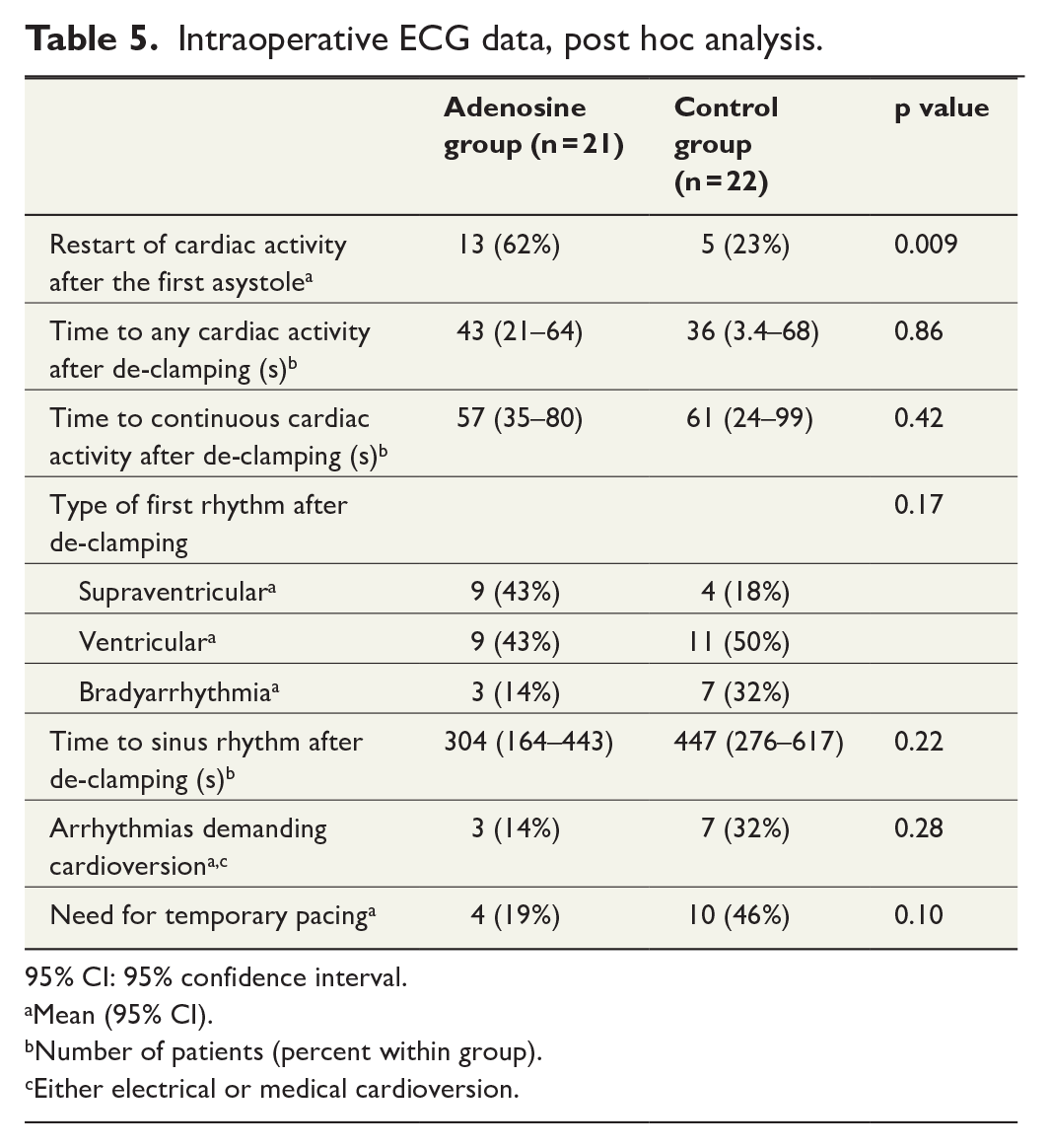
95% CI: 95% confidence interval.
Mean (95% CI).
Number of patients (percent within group).
Either electrical or medical cardioversion.
Post hoc hemodynamic measurements.
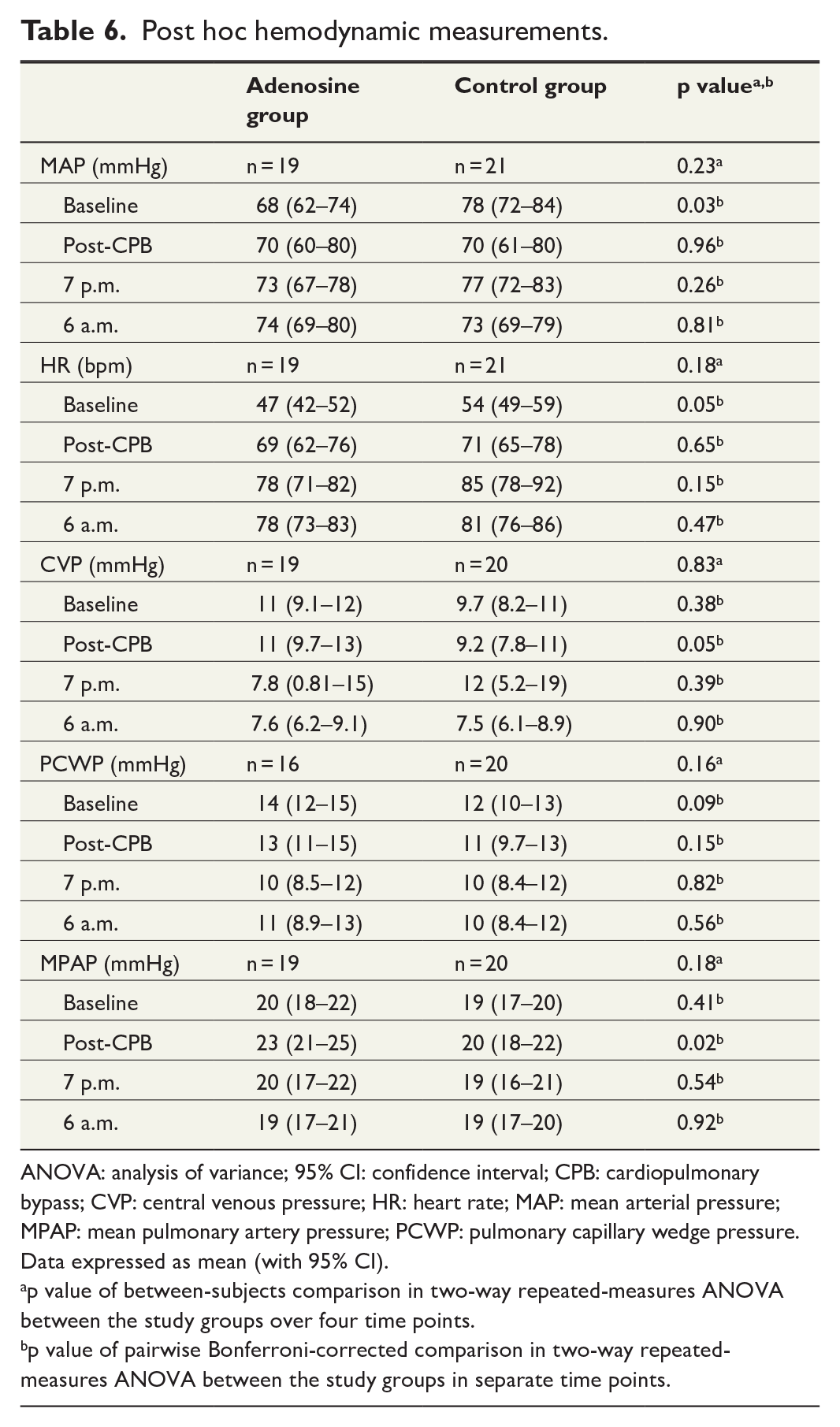
ANOVA: analysis of variance; 95% CI: confidence interval; CPB: cardiopulmonary bypass; CVP: central venous pressure; HR: heart rate; MAP: mean arterial pressure; MPAP: mean pulmonary artery pressure; PCWP: pulmonary capillary wedge pressure.
Data expressed as mean (with 95% CI).
p value of between-subjects comparison in two-way repeated-measures ANOVA between the study groups over four time points.
p value of pairwise Bonferroni-corrected comparison in two-way repeated-measures ANOVA between the study groups in separate time points.
Discussion
This is the first randomized placebo-controlled trial in CABG to investigate the effects of adenosine bolus on time to asystole and postoperative ventricular function, when using potassium-enriched blood cardioplegia. The main finding of the study was that adenosine did not improve CI significantly compared to placebo. The second main finding was a significantly faster cardiac arrest in the adenosine group. The third main finding was that adenosine significantly improved RVSWI and that it did not improve LVSWI.
We found no significant differences in plasma cardiac biomarker release between the groups, indicating similarly low levels of myocardial cell injury.
We assume that reduced myocardial metabolism, oxygen demand, and use of nutrients, caused by faster cardiac arrest in the adenosine group, might result in a lower level of myocardial stunning and faster myocardial recovery, visible in higher RVSWIs and marginally higher CIs after CPB. There were more restarts of cardiac activity during the first cardioplegia infusion in the adenosine group, potentially because of the short half-life of adenosine. We think that our specific criteria for asystole in this study yielded a longer time to asystole than has been reported by other authors.1–4,6,9
The authors’ hypothesis was that a faster cardiac arrest might lead to better myocardial protection from ischemia. In a rapidly arrested heart, cardioplegia could be better distributed into the myocardium during diastolic arrest, and myocardial work under ischemic conditions after aortic closure could be reduced. We were particularly interested in the fast induction of myocardial functional arrest with adenosine and believed that it could provide improved overall myocardial protection. The evidence of improved cardioprotection for adenosine-induced arrest is limited in the literature. This study adds to the potential benefits of adenosine-induced cardioplegic arrest in postoperative myocardial recovery. According to our knowledge, only our research group has compared adenosine induction to placebo using blood cardioplegia in both groups in a double-blinded randomized controlled trial in CABG patients. Failure in cardioprotection may result in myocardial damage and provoke postoperative morbidity. 9 Septal dysfunction and the need for hemodynamic support are common after cardiac surgery, even with current cardioplegia techniques and a variety of solutions. 10 Postoperative myocardial stunning is not unusual, and it is associated with increased morbidity and mortality, especially in patients with decreased myocardial reserve. 11 The optimal composition of the cardioplegia solution has been a matter of debate, and several modifications have been used over the years. 12 Previously, adenosine has been shown to decrease infarct size and attenuate myocardial stunning in animals.13,14 In humans, as an additive to cardioplegia solution, adenosine has shown advantages to cardioprotection.1–4,6,9,11 Ammar et al. 15 witnessed better clinical recovery, lower cardiac troponin I and CK-MB release, and less arrhythmia in the post-bypass period when adenosine infusion was given before aortic cross-clamp removal. There is no consensus regarding the adenosine application strategy, and the variability in results among the published studies might be related to differences in administration protocols. 2
In this study, the adenosine regimen was relatively simple to manage and easily repeatable. There was no increase in cross-clamp or operation time, and adenosine did not cause clinically significant side effects when compared with saline administration.
Limitations
The main limitation of the study is the small number of patients. Another major limitation is that only a minority of all the elective and urgent CABG patients could be recruited to this study and the study population became biased in relation to sex and bypass count. Study patient recruitment and study time were influenced by the availability of research staff during the workweek and the limitation of only one operating room equipped with continuous ECG data capture and download technology. Forty-three patients were non-selectively recruited from a source population of 297 patients that were operated during the study period. Men were overrepresented in our study population when compared to other elective and urgent CABG patients during the time of study. We think that coincidentally having more men (95% versus 81%) in the study population might be because of no sex-matched randomization of the study groups to our operative flow of CABG patients. However, we think that sex might not be as strong factor in myocardial protection as, for example, cross-clamp time, CPB time, or left ventricular ejection fraction (LVEF) is. It also seemed that more bypasses on average had been performed to the study patients (3.7 (95% CI = 3.4–3.9) versus 3.4 (95% CI = 3.2–3.5) than to other elective and urgent CABG patients during the time of study. We think that this is a random effect because it would be hard to predict how many bypasses are needed at the time of the study enrollment. More bypasses might mean that the coronary artery disease was more severe in the study population compared to remaining source population. Other parameter frequencies did not differ between the source and the study populations (Supplementary Table 1). Our results can be generalized only to patients who resemble the study population.
Although the trial was blinded, the surgical team could have observed the shorter time to asystole in patients receiving adenosine as compared to saline administration. However, we have no reason to believe that this would have had any effect on the surgeons’ decisions during the operation. The physicians and nurses in the surgical and anesthesiologic teams varied in our medium-size unit, which brought some variability in operative and anesthesiologic procedures and study measurements. There was human-dependent imprecision in the injection speed and time of the study medicine boluses. There were minor inaccuracies in the selections of time points for CI measurement or of blood sample withdrawal, which are not easy to avoid in a clinical study setting. Some perioperative ECG data were lost due to computer malfunction, and solitary hemodynamic measurements failed in some patients due to problems related to the pulmonary artery catheter.
Conclusion
In this randomized study of 43 CABG patients, a high dose adenosine bolus at the first cardioplegia infusion did not enhance CI. Adenosine caused faster cardiac arrest and better RVSWI compared to the control group. The authors hypothesize that the partially enhanced ventricular performance in the adenosine group might be associated with a shorter time to cardiac arrest and thereby better delivery of blood cardioplegia into the myocardium in diastolic arrest. However, we need larger studies involving different types of procedures and larger variety of patients in order to understand and establish the benefits related to faster induction of cardiac arrest.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-1-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-2-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-3-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-4-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-4-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-5-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-5-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-6-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-6-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-7-sjs-10.1177_14574969221116943 – Supplemental material for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial
Supplemental material, sj-docx-7-sjs-10.1177_14574969221116943 for High-dose adenosine versus saline-induced cardioplegic arrest in coronary artery bypass grafting: A randomized double-blind clinical feasibility trial by Mikko S. Mattila, Kati M. Järvelä, Timo T. Rinne, Kjell C. Nikus, Markku J. Rantanen, Juho A.A. Siltanen, Jenna-Juulia Heleä and Jari O. Laurikka in Scandinavian Journal of Surgery
Footnotes
Author contributions
M.S.M. contributed to data curation, formal analysis, funding acquisition, investigation, project administration, and writing—original draft; J.O.L. contributed to conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, and writing—review and editing; K.M.J. contributed to validation and writing—review and editing; J.-J.H. contributed to data curation and investigation; J.A.A.S. contributed to data curation and investigation; T.T.R. contributed to validation and writing—review and editing; K.C.N. contributed to formal analysis, validation, and writing—review and editing; M.J.R. contributed to resources and methodology.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Heart Hospital, the Finnish Foundation for Cardiovascular Research, the City of Tampere Research Fund, the AK Foundation (Medical) Helsinki, the Finnish Cultural Foundation, and the Finnish Medical Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.