
Abstract
Introduction:
Incidences of different tibia fractures are not well reported. Possible changes in the operative treatment methods have also not been studied. The aim of this nationwide registry study is to determine the incidence of operatively treated tibia fractures and investigate the possible changes in treatment methods in Finland between 2000 and 2018.
Methods:
All patients aged 16 years or older with operatively treated tibia fractures in Finland from 2000 to 2018 were included. The incidence of operatively treated proximal, diaphyseal, and distal tibia fractures per 100,000 person years by age, sex, mechanism of injury, and study year was calculated. Data were extracted from the Finnish National Hospital Discharge Register.
Results:
A total of 5996 proximal, 6874 diaphyseal, and 5658 distal tibia fractures were reported during the 18-year study period, resulting in incidences of 7.2/100,000, 8.1/100,000, and 6.9/100,000 person years for operatively treated proximal, diaphyseal, and distal tibia fractures, respectively. Over the study period, a clear change in fixation method in distal tibia fractures was found as plating became popular in the beginning of the 21st century. During the last 5 years of the study period, nailing and plating were equally used.
Conclusions:
Operatively treated proximal tibia fractures are most common among older females while diaphyseal fractures are most frequent in young male patients. Distal tibia fractures occur most often among middle-aged people.
Introduction
Tibia fractures are common injuries in all age groups. These fractures are divided into proximal, diaphyseal, and distal fractures according to the Arbeitsgemeinschaft für Osteosynthesefragen/ Orthopedic Trauma Association (AO/OTA) classification system. 1 In previous studies, the incidence of diaphyseal tibia fractures was estimated to be 14–22 per 100,000 person years.2–6 Unlike diaphyseal fractures, studies investigating the incidence of proximal or distal tibia fractures are scarce. Existing studies reported the incidence of proximal tibia fractures to be 10–32 per 100,000 person years6–8 and of distal tibia fractures to be 9 per 100,000 person years. 6 These figures were mostly based on a single center fracture register.
Surgical treatment options for tibia fractures include nailing, plating, or an external fixator. The fixation method is most commonly determined by the fracture morphology and soft tissue condition. Anatomically contoured locking plates and minimally invasive plating techniques were introduced in 1995 and became more common in the beginning of the 21st century. The design and development of intramedullary nails have evolved considerably since early days, making it technically more feasible to nail very proximal and distal tibia fractures nowadays. The suprapatellar nailing technique has become popular. 9 The benefits of this technique are more precise reduction when nailing very proximal and distal tibia fractures,10–12 Evidence about impact on incidence of anterior knee pain has found to be either beneficial or at least not inferior.12,13
Since the introduction of newer innovations, possible changes in implant and method selection in Finland have not been studied. The purpose of this nationwide registry study is to determine the incidence of operatively treated tibia fractures and investigate the possible changes in treatment methods in Finland from 2000 to 2018. The main outcome variables were the incidence of operatively treated tibia fractures and operations for proximal, diaphyseal, and distal tibia fractures per 100,000 person years by age, sex, mechanism of injury, and study year. Secondary outcomes were how the incidence of different operative treatment methods varied during the study period and the length of hospital stay.
Materials and methods
Patient data were collected from the Finnish National Hospital Discharge Register (NHDR). Data collection by the NHDR is obligatory for all public and private hospitals and other institutions providing health care in Finland. The NHDR database was searched for patients aged 16 years or older with tibia fractures (The International Classification of Diseases-10 code, ICD-10 S82.1-S82.3) and with a procedural code of NGJ45, NGJ60, NGJ62, NGJ64, NGJ70, or NGJ99 according to the Nordic Classification of Surgical Procedures (NCSP) between 1 January 2000 and 31 December 2018. Age limit of 16 years was set as after that age epiphysis generally does not have an impact on the decision-making of tibial fracture treatment method. The collected patient data included age, sex, ICD-10 primary and secondary diagnoses, external cause for injury and type of accident codes, NCSP procedural codes, hospital providing care, and dates of admission and discharge. Only the first hospitalization that had both diagnostic and procedural codes was considered and hospital stay was counted from that treatment period. If same patient had several procedural codes concerning tibia fracture fixation method, only the first one was considered. We used a clearance period of 1 year. All subsequent records with tibia fracture diagnosis code after 1 year from the first included record were considered to be re-visits or reoperations due to the same fracture and were excluded in order to include only acute tibia fracture operations for the incidence calculations. The validity of the NHDR is found to be good in both coverage and accuracy of the data, especially in orthopedic traumas concerning first time hospitalization due to a certain fracture and first procedure.14–16
Incidence rates were calculated using the annual adult population size (persons 16 years of age or older) obtained from Official Statistics of Finland, a statutory electronic national population register (Statistics Finland. Population structure, www.stat.fi).
Injury mechanism codes related to patients’ fractures were analyzed according to the ICD-10 external cause for injury codes and then grouped into four categories: fall on the same level (W00, W01), fall from height (W06, W10, W11, W19), traffic accidents (V01–V99), and other injury (all other codes for causes of external injuries grouped together). Continuous variables were compared using Welch t-test. Analyses were with RStudio 1.2.5033 (version 4, standard packages used).
Results
A total of 5996 proximal, 6874 diaphyseal, and 5658 distal tibia fractures that were treated operatively were reported during the 18-year study period. Concurrently, there were 83,421,524 person years in Finland, resulting in overall annual incidences of 7.2/100,000 (95% confidence interval (CI) 7.0–7.4), 8.1/100,000 (8.0–8.4), and 6.9/100,000 (6.6–7.0) for operatively treated proximal, diaphyseal, and distal tibia fractures, respectively. Total incidence of operatively treated tibia fractures divided by the fracture location is presented in Fig. 1. The incidence of operatively treated proximal tibia fractures was highest at 40–60 years of age among men and at 60–80 years among women (Fig. 2). The incidence of operatively treated diaphyseal tibia fractures was dominating in men under 20 years of age (Fig. 3). The incidence of operatively treated distal tibia fractures was highest among both men and women at 40–60 years of age (Fig. 4). Additional detailed information acquired and analyzed from the NHDR database is found in the supplementary files (Supplementary Tables 1 to 6, Supplementary Figures 6 to 11).
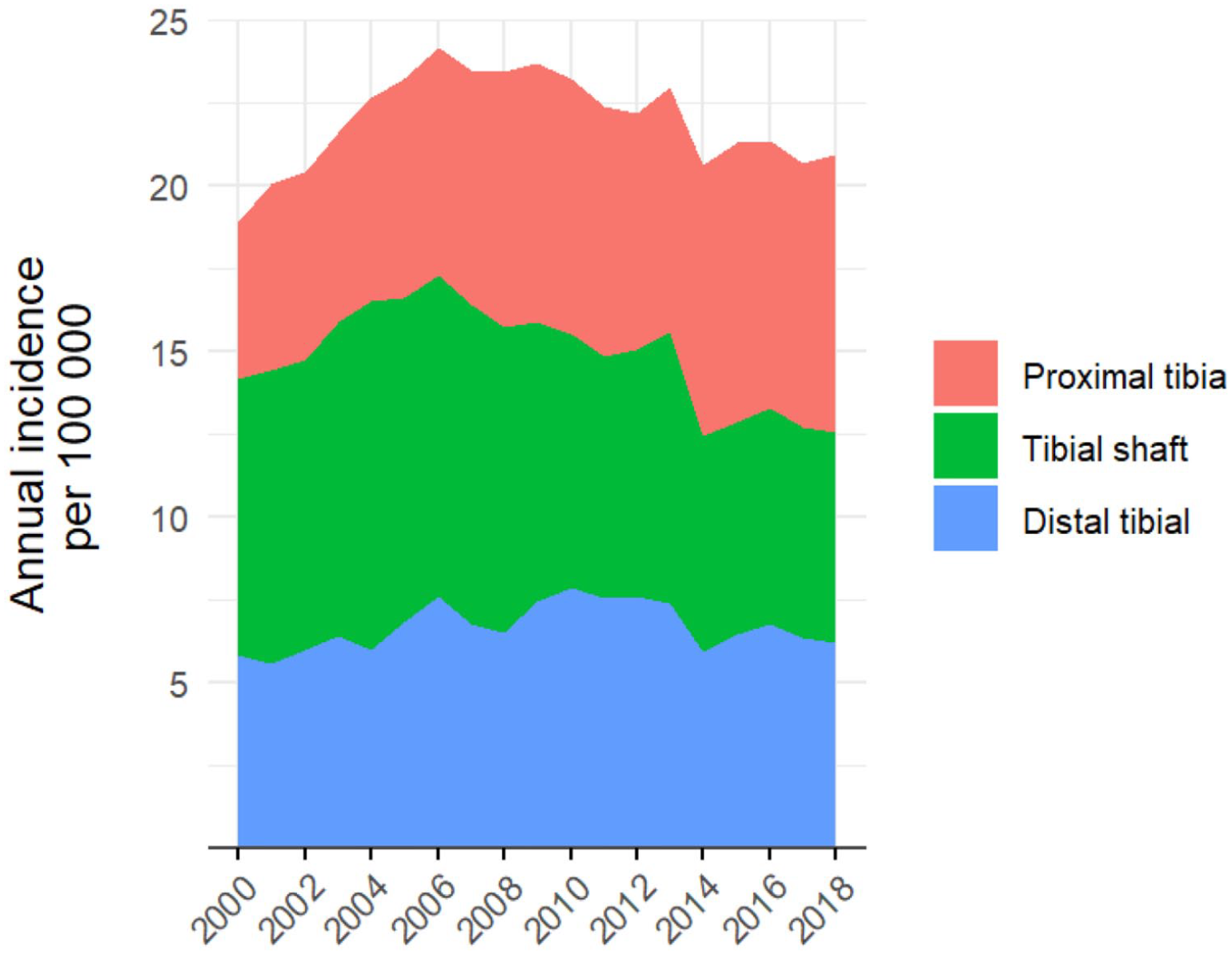
Total incidence of operatively treated tibia fractures divided by fracture location.
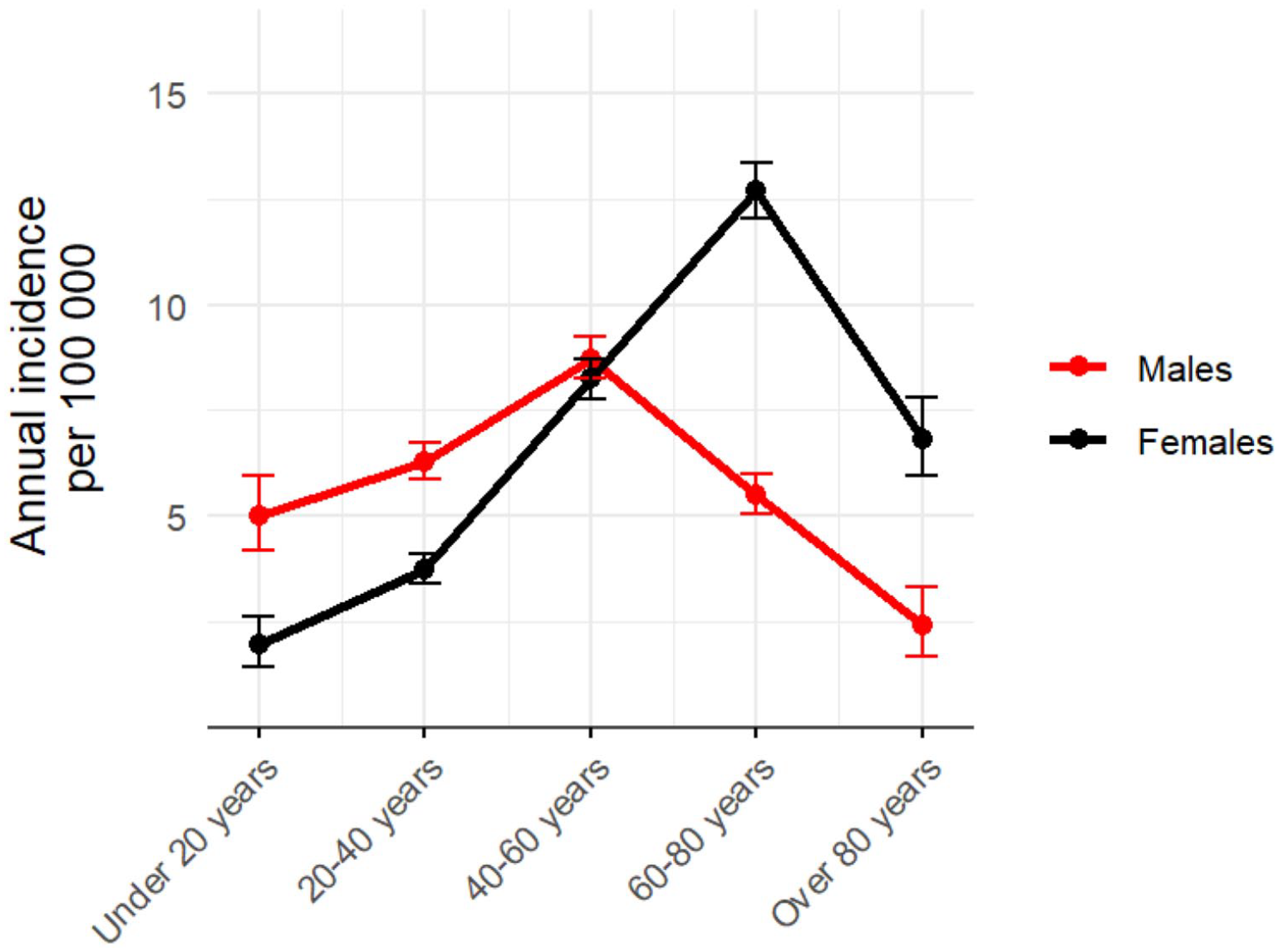
Incidence of operatively treated proximal tibia fractures in different age groups.
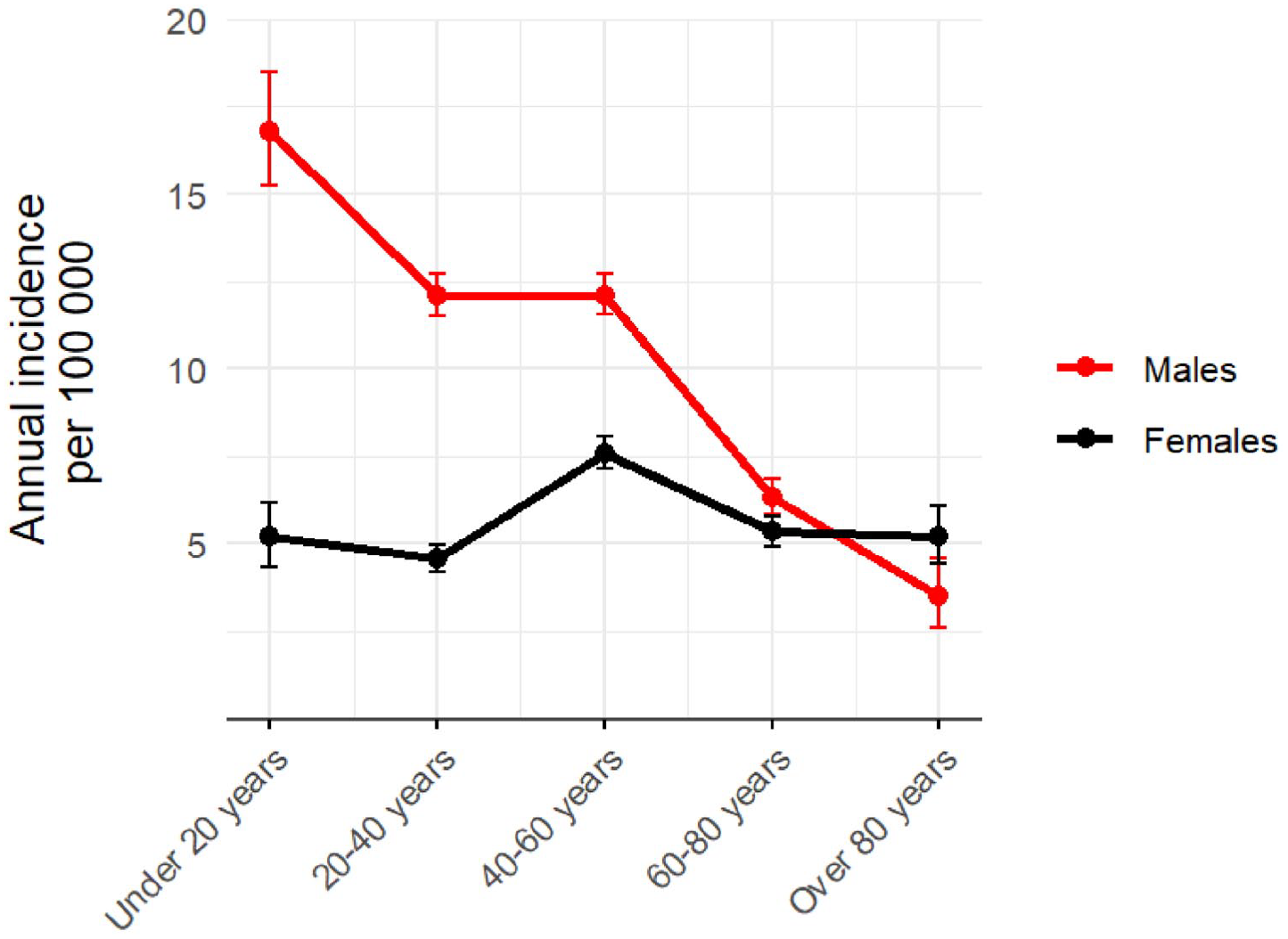
Incidence of operatively treated diaphyseal tibia fractures in different age groups.
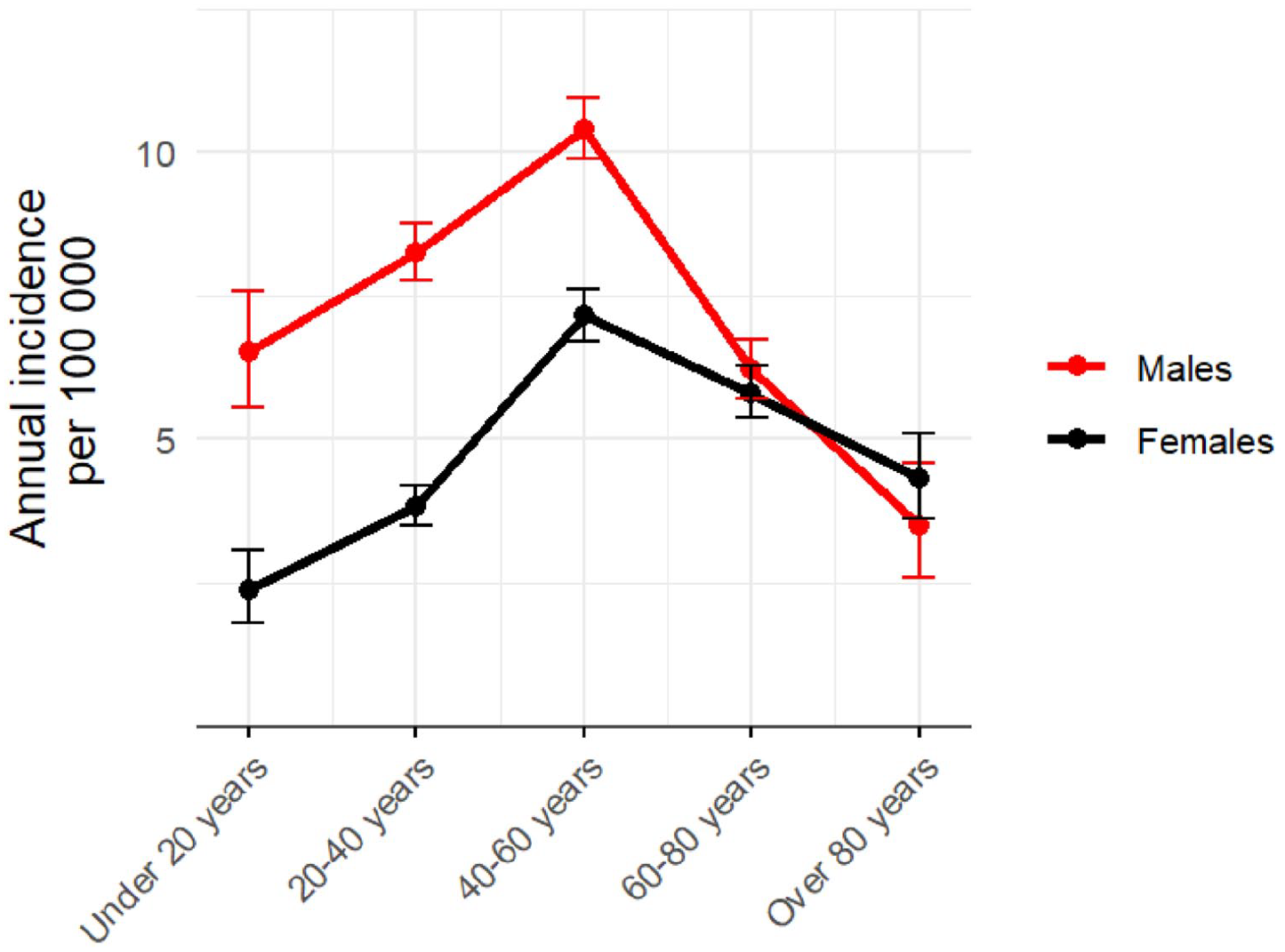
Incidence of operatively treated distal tibia fractures in different age groups.
Operatively treated proximal tibia fractures
Out of all 5996 operatively treated proximal tibia fractures, 5316 (89%) were treated with internal plate fixation, 150 (3%) nailing, and 530 (9%) external fixation. In this group, proximal tibia fractures were slightly more common in women than in men (54% versus 46%). Mean age at injury was significantly lower in men than in women (95% CI 46.7 versus 58.2 years, p < 0.001). The incidence in women increased sharply from 40 years of age to 80 years (Fig. 2). However, in men, the incidence was stable in younger age groups and decreased after 60 years of age. Mean hospital stay was 6.9 days (standard deviation (SD) 5.0, 0–64 days). Operative treatment rates slightly increased during study period. Out of proximal tibia fractures, most common injury mechanisms were fall on the same level (32%), other injury (22%), and traffic accidents (22%). Among patients under 40 years of age, other injury was the most frequent cause of injury whereas in older age groups fall on the same level was the most common.
Operatively treated diaphyseal tibia fractures
Of all 6874 operatively treated diaphyseal tibia fractures, 5810 (85%) were treated with intramedullary nailing, 696 (10%) plating, and 368 (5%) external fixation. In this group, diaphyseal fractures were clearly more common in men than in women (64% versus 36%). Mean age at injury was lower in men than in women (95% CI 42.6 versus 51.3 years, p < 0.001). Mean hospital stay was 6.0 days (SD 4.0, 0–65 days). The rate of operatively treated tibia fractures remained stable during the 18-year study period. The most common injury mechanisms in diaphyseal fractures were fall on the same level (47%), other injury (22%), and traffic accidents (16%). Simple fall was the main injury mechanism in all ages but in patients under 20 years of age traffic accident was the most common cause of injury.
Operatively treated distal tibia fractures
Of all 5658 operatively treated distal tibia fractures, 2770 (49%) were treated with intramedullary nailing, 1896 (34%) with internal plate fixation, and 966 (16%) with external fixation. In this group, distal tibia fractures were more common in men than in women (59% versus 41%), and mean age at injury was lower in men (95% CI 46.2 versus 53.3 years, p < 0.001). Mean hospital stay was 6.5 days (SD 5.0, 0–54 days). Operations particularly using internal plate fixation grew in number from the year 2001 onwards and the rate of plating markedly accelerated from 2004 onwards, but since 2013 plating and nailing were almost equally used (Fig. 5). The most common injury mechanisms were fall on the same level (49%), fall from height (20%), and other injury (17%). Simple fall was the main injury mechanism in all ages but in patients under 20 years of age traffic accident was the most common cause of injury. During the whole study period in Finland, the incidence of operatively treated distal tibia fractures was quite steady, except in age groups of 60 years and older, a tendency of a slight increase in incidence was noted.
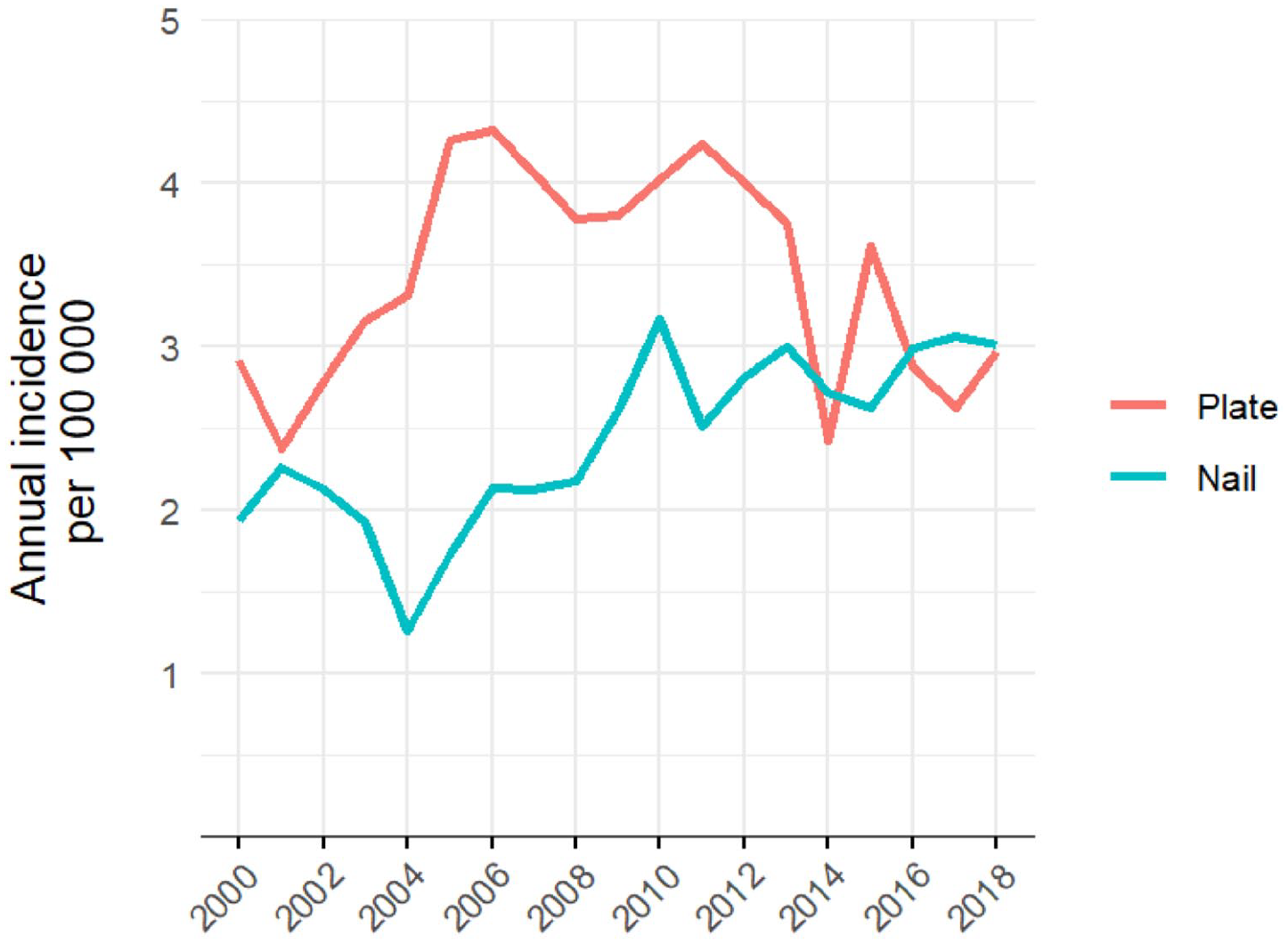
Incidence progression of different operative methods in distal tibia fractures.
Discussion
The main findings of this study were the very different patient profiles in each fracture type. Regarding injury mechanisms, we found simple falls to be the most common cause for all tibia fracture types. This finding was especially clear in the older age groups. Our results for injury mechanisms are consistent with those of previous studies.4,6
We omitted conservatively treated tibia fractures from our study, as reliable data to examine them within the chosen timeframe do not exist in Finland.
Previously reported proximal tibia fracture incidences have been varying between 10.3 and 32 per 100,000,6–8 figures including also conservatively treated fractures. We found the annual incidence of operatively treated proximal tibia fractures to be 7.2 per 100,000. In our study, operatively treated proximal tibia fractures were markedly more common in females in older age groups than males. Despite differences in study designs, this trend is very similar to those in previous studies.6–8 The difference in incidence regarding age between men and women could be explained by fragility fractures2,17 while osteoporosis and osteoporotic fractures affects more aging females than males.18,19
In this study, the annual incidence of operatively treated diaphyseal tibia fractures was 8.2 per 100,000, which is lower than the incidence in previous nationwide studies.4,5 Leliveld et al. 4 reported incidences of 13.3 and 5.6 per 1000,000, respectively, in men and women in The Netherlands, and Weiss et al. 5 reported 17 per 100,000 in Sweden. However, both studies included children, which likely explain the difference as unlike in adults most of pediatric diaphyseal tibia fractures are treated conservatively. A previous study from Finland reported the annual incidence of hospitalizations due to diaphyseal tibia fractures to be 13.5 per 100,000 and decreasing, figures including also non-operatively treated fractures. 3 We found diaphyseal tibia fractures to be most common in young adults and working aged population, steadily decreasing after 40 years of age in men (Fig. 3), whereas the incidence remained stable in women in all age groups. Similar trend was clear in the two recent nationwide studies as well.4,5 However, in Sweden, the incidence starts to grow in women over 70 years of age. 5 This trend was not evident in the present study which excluded conservatively treated diaphyseal fractures, nor was it in the study by Leliveld et al. 4 which included them.
The annual incidence of operatively treated distal tibia fractures in Finland was 6.9 per 100,000, which is lower than the previously reported incidence of 9.1 by Wennergren et al. 6 Operatively treated distal tibia fractures have the highest incidence in middle-aged patients, both in men and women. Noted increase in plating of distal tibia fractures between 2004 and 2013 (Fig. 5) could be explained by the recently introduced anatomical locking plates that gained popularity in the beginning of the 21st century. During the latest study years, nailing and plating seemed to be used as often. One can hypothesize that this change might be due to the increasing use of the suprapatellar nailing technique with more precise control of alignment also when nailing distal tibia fractures compared to infrapatellar nailing technique. 10 However, these statements cannot be proved by register study, as procedural codes are constant, regardless of plating or nailing technique used. Nevertheless, similar suppositions have been made concerning increasing incidence of proximal humerus plating after invention of locking plates.20,21 External fixation as primary treatment was used in 16% of patients with distal tibia fracture. The distal tibia has delicate soft tissue coverage and blood supply, 22 which is why these fractures, especially in case of open fractures and high energy traumas, are more often managed with staged treatment strategy or with a modern ring fixator. Both operations are under the same procedural code, which makes information about the portion of external fixation as definitive treatment method inaccessible in this setting of registry study. Although NHDR data are very accurate in first time hospitalization due to a certain fracture and procedure, this is unfortunately not the case regarding reoperations of that same injury. Therefore, conclusions cannot be made about rate of conversions from external fixation to plating or nailing.
This is an observational study based on registry data, reporting the incidence of operatively treated fractures in all segments of the tibia and the changes in treatment methods over time, including the whole Finnish nation. To the best of our knowledge, no other study with this design has been conducted. Variations in the methods of surgical treatment of tibia fractures have not been studied before.
A limitation of this study is that we did not include conservatively treated tibia fracture patients. Hence actual incidence rates, especially regarding proximal tibia fractures, could therefore be slightly higher than reported.
Conclusion
Operatively treated proximal tibia fractures are most common among older females, while diaphyseal fractures are most frequent in young male patients. Distal tibia fractures occur most often among middle-aged people. It would benefit clinical practice to further study the effect of fracture morphology and soft tissue injury on implant selection. Also added research is needed on how soft tissue injury and implant selection correlates with complications such as deep infection and nonunion.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-1-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-10-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-10-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-11-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-11-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-12-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-12-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-2-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-3-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-4-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-4-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-5-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-5-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-6-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-6-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-7-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-7-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-8-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-8-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-9-sjs-10.1177_14574969221111612 – Supplemental material for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study
Supplemental material, sj-docx-9-sjs-10.1177_14574969221111612 for Changes in operative treatment of tibia fractures in Finland between 2000 and 2018: A nationwide study by Antti A.J. Ylitalo, Kalle A. Dahl, Aleksi Reito and Elina Ekman in Scandinavian Journal of Surgery
Footnotes
Authors’ contributions
EE designed and coordinated the study and helped to draft the manuscript. AY and KD collected the data and drafted the manuscript. AR calculated the statistics and drew the figures. AY, KD, AR, and EE contributed to the interpretation of the data and results and the preparation of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. Permission to use register was given by Finnish Institute for Health and Welfare (Dnro THL/1777/5.05.00/2019).
Code availability
Available on reasonable request
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.