
Abstract
Introduction:
Hypoparathyroidism is the most common complication following thyroidectomy, and various algorithms for early detection have been suggested. The aim of this study was to evaluate the predictive value of measuring the parathyroid hormone level 2 h after thyroidectomy and whether determination of the perioperative decline in parathyroid hormone added diagnostic value.
Methods:
Patients subjected to thyroidectomy for benign thyroid disorders were analyzed in (1) a retrospective register-based study (366 consecutive patients treated during 2015–2016) and (2) a prospective observational study (39 patients treated during 2018). Optimal cut-off values for postoperative parathyroid hormone and perioperative decline (%) in parathyroid hormone were determined by receiver operating characteristics and area under the curve. Sensitivity, specificity, positive and negative predictive values were calculated using cross tabulation.
Results:
The prevalence of hypoparathyroidism the first day after thyroidectomy was higher among patients treated for hyperthyroidism (30% vs 20%; P = 0.03). The optimal cut-off level for postoperative parathyroid hormone was 1.1 pmol/L (area under the curve = 0.887, 95% confidence interval: 0.839–0.934; positive predictive value: 88%, negative predictive value: 93%) for the entire cohort. When the groups were analyzed separately, the optimal cut-off was 1.05 for the non-hyperfunctioning group and 1.55 pmol/L for the group with hyperthyroidism. Twelve months after thyroidectomy, 3% were defined as having permanent hypoparathyroidism. Measurement of parathyroid hormone decline added diagnostic value for one patient with preoperative parathyroid-hormone-elevation associated with vitamin D deficiency.
Conclusions:
For patients with vitamin D sufficiency, the diagnostic accuracy of a single measurement of parathyroid hormone 2 h after thyroidectomy is an excellent indicator for predicting transient hypoparathyroidism.
Introduction
Hypoparathyroidism is the most common complication after thyroidectomy and may be either transient or permanent. Recently, it has become clear that the incidence of permanent hypoparathyroidism is much higher than previously reported. A systematic review of the literature, including 89 publications from 2010 to 2017, reported incidences up to 20% 1 . The variation depends upon several factors such as indication for surgery, surgical technique, the surgeon’s experience, and patient-related factors 2 . Comparative analyses of incidence between different cohorts are hampered by the fact that a dozen different definitions of hypoparathyroidism are included in the literature. The American Thyroid Association defines it as a disorder in which the production of parathyroid hormone (PTH) is inadequate for maintaining a normal plasma calcium concentration 3 . Symptoms of hypocalcemia are usually not manifested until 24–72 h after thyroidectomy. The degree varies widely from paresthesias and muscle ache to more severe forms involving tetany, seizures, cardiac arrhythmia, and bronchospasm 4 . Today, patients are often discharged from hospital within 24 h after thyroidectomy and thus early prediction of hypoparathyroidism is essential to ensure patient safety. Various algorithms, intended to prevent and/or predict hypoparathyroidism early on, after thyroidectomy, have been proposed. Most algorithms include postoperative measurements of PTH, but the diagnostic accuracy has recently been questioned5,6. Differences in the time interval between the end of thyroidectomy and PTH measurement contribute to differences in prognostic value6 –8. Several risk factors for transient hypoparathyroidism have been proposed: female gender, toxic goiter, hungry bone syndrome, and vitamin D deficiency, yet published data have been contradictive9,10. Measurement of the perioperative decline in PTH has been preferred by some authors for detecting relative parathyroid insufficiency among patients with postoperative PTH within the normal range 11 . The aim of this study was to evaluate the reliability and optimal cut-off values for PTH, measured 2 h after thyroidectomy, in order to predict early postoperative hypoparathyroidism and to evaluate whether determination of the perioperative decline in PTH added diagnostic accuracy, as compared to a single postoperative PTH measurement.
Material and Methods
The study was started as a retrospective analysis of all patients subjected to total thyroidectomy for benign disorders at the Karolinska University Hospital, Sweden, during 2015–2016. The primary endpoint was the diagnostic accuracy of a single PTH, rutinously measured 2 h after thyroidectomy, to predict early postoperative hypoparathyroidism. Secondary endpoints were risk factors for transient and permanent hypoparathyroidism. The retrospective study was followed by a prospective study, aimed to evaluate the added value of determination of the perioperative decline in PTH as compared to a single measurement.
Patients fulfilling two of the following three criteria were defined as having postoperative hypoparathyroidism: PTH ⩽ 1.1 pmol/L, ionized calcium (iCa2+) <1.15 mmol/L, or clinical symptoms of hypocalcemia documented in the patient’s medical records. Patients still in need of medication with active vitamin D and/or calcium at 1 year after thyroidectomy were defined as having permanent hypoparathyroidism.
Part 1: Retrospective Study
A cohort consisting of 379 consecutive patients treated between 2015 and 2016 was identified in The Scandinavian Quality Register of Thyroid, Parathyroid and Adrenal Surgery. The register contains data regarding indication for surgery such as age, calcium levels prior to surgery, postoperative day 1, 6 weeks, and 6 months after surgery, the result of histopathological examination of the excised thyroid, and postoperative complications. Additional basic, clinical characteristics, and postoperative data were collected from the patient files. Following the local routine, PTH was analyzed 2 h after completion of thyroidectomy and if <1.1 pmol/L, treatment with alfacalcidol was initiated directly. Calcium substitution, usually calcium carbonate, was initiated if symptoms of hypocalcemia occurred or were later dependent upon measured iCa2+. All journal entries after surgery were carefully reviewed to investigate whether the patient had sought medical attention for symptoms of hypocalcemia and if the patient had a need for calcium and/or active vitamin D supplement at 6 weeks, 6 months, and 12 months postoperatively. Thirteen patients were excluded: 10 of those were younger than 18 years of age and 3 had a protected identity and medical records could not be accessed. The final cohort consisted of 366 patients, 243 with hyperthyroidism and 123 with non-functional goiter. The clinical characteristics are presented in Table 1.
Patients subjected to thyroidectomy for benign disorders—register-based study.
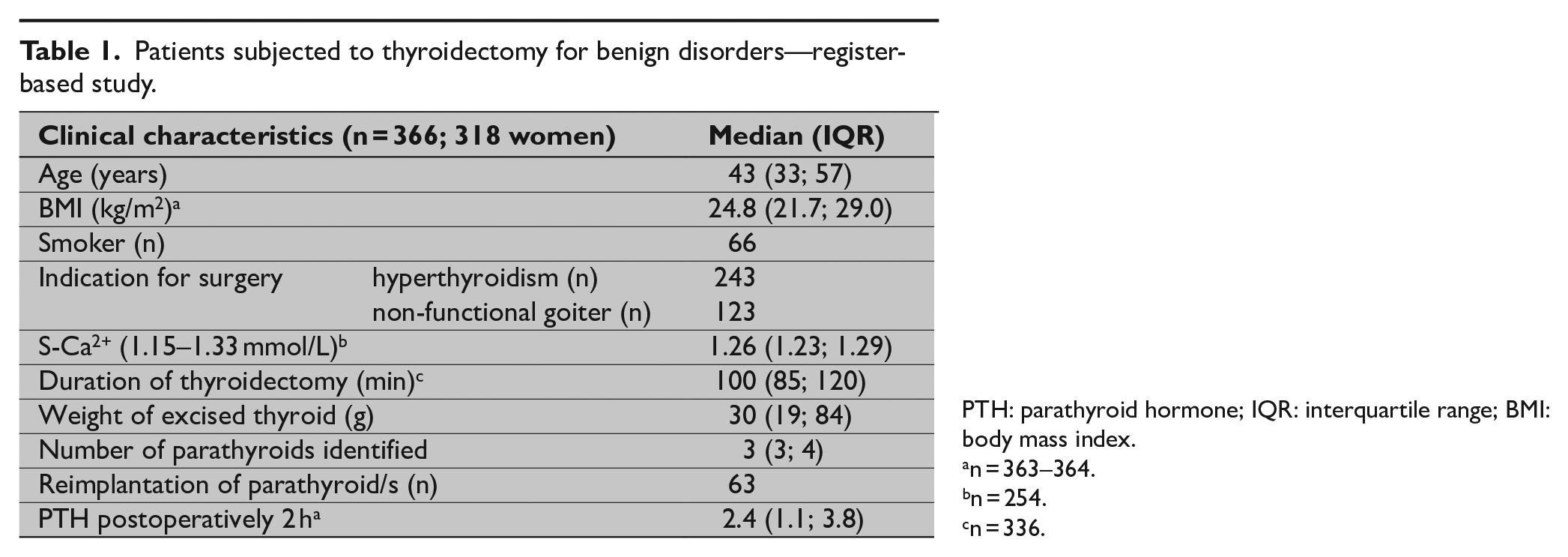
PTH: parathyroid hormone; IQR: interquartile range; BMI: body mass index.
n = 363–364.
n = 254.
n = 336.
Part 2: Prospective Study
Forty consecutive patients subjected to thyroidectomy for benign cause during 2018 were included in an observational study. The cohort consisted of 26 patients treated for hyperthyroidism and 14 treated for non-functional goiter. A Case Report Form, containing all parameters included in the study protocol, was established for each study participant. One patient was excluded from analysis (not completed thyroidectomy). The biochemical analyses included measurement of plasma intact PTH, iCa2+, P-creatinine, P-phosphate, thyroid-stimulating hormone (S-TSH), and 25-OH-vitamin D (25-OHD). PTH was analyzed on four occasions: within 1 week before thyroidectomy, at initiation of, 2 h, and finally 6 weeks after thyroidectomy; s-iCa2+ was collected three times, within 1 week prior, 1 day after, and 6 weeks after thyroidectomy. The clinical characteristics are presented in Table 2. The perioperative decline in PTH was defined as the ratio between the perioperative decline in PTH and the PTH at start of thyroidectomy as follows
Ethical approvals were obtained from the Regional Ethical Committee in Stockholm (Dnr 2015/959-31 and 2018/674-32).
Patients subjected to thyroidectomy for benign disorders—prospective cohort.
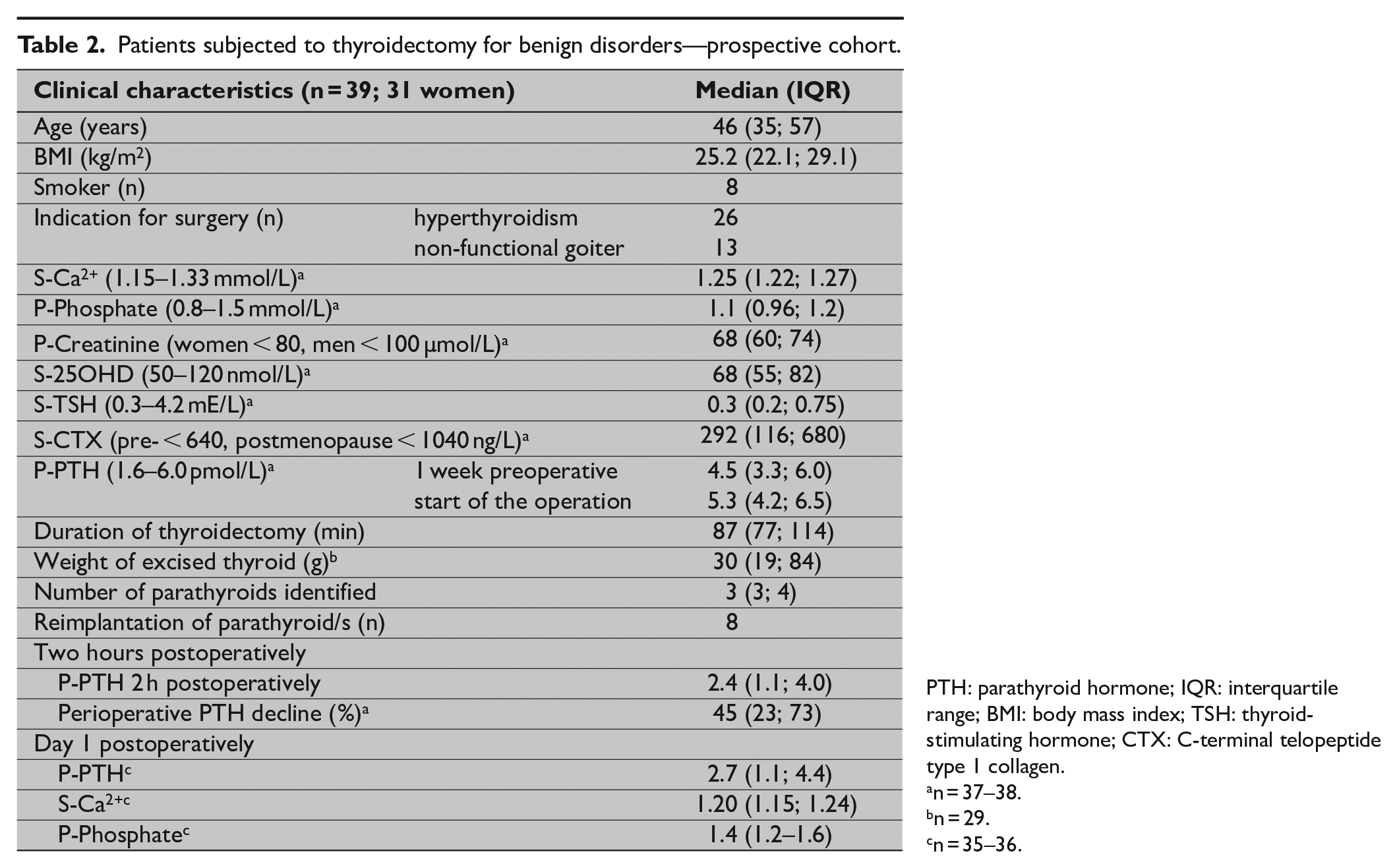
PTH: parathyroid hormone; IQR: interquartile range; BMI: body mass index; TSH: thyroid-stimulating hormone; CTX: C-terminal telopeptide type 1 collagen.
n = 37–38.
n = 29.
n = 35–36.
Statistics
All statistical analyses were performed using IBM SPSS Statistics® version 24.0 (IBM, Armonk, NY, United States). Based on the distribution of data, nonparametric methods were used and data are presented as the median, quartiles, and interquartile range in text and tables. Wilcoxon signed rank test was used for intraindividual analyses, Fisher’s exact test for comparisons of categorical data, and Mann Whitney U for continuous and ordinal data. Correlations were analyzed with the Spearman rank correlation test. Sensitivity, specificity, positive predictive values (PPVs), and negative predictive values (NPVs) were calculated using cross tabulation. Receiver-operating characteristic (ROC) curves and area under curve (AUC) were used to define the optimal cut-off value for postoperative PTH and PTH decline in order to predict early postoperative hypoparathyroidism. The cut-off corresponding to the highest combined sensitivity and specificity was chosen. Binary logistic regression testing was used to identify independent risk factors. The size of the prospective cohort was determined based on a previous study to guarantee a power level of 80% at a confidence level of 95%, to detect relative hypoparathyroidism 10 .
Results
Clinical characteristics and biochemical data for the retrospective cohort are summarized in Table 1. Postoperative PTH data were available for 363 patients. The prevalence of hypoparathyroidism the first day after thyroidectomy was higher among patients treated for hyperthyroidism (30% vs 20%; P = 0.03) and tended to be higher among women (28% vs 17%; P = 0.06). The prevalence of hypoparathyroidism decreased to 16% after 6 weeks, 4.7% after 6 months, and 3.3% after 12 months. Compared to patients with transient hypoparathyroidism, patients defined as having permanent hypoparathyroidism (persisting beyond 12 months) had lower PTH levels 2 h after thyroidectomy (0.60 (0.32–1.30) vs 0.76 (0.38–3.0); P = 0.027) and lower iCa2+ 6 weeks (1.08 (0.93; 1.29) vs 1.19 (0.81–1.32)) and 6 months after thyroidectomy (1.04 (0.95; 1.21) and 1.16 (1.12–1.21) mmol/L; P < 0.010). The optimal cut-off level for PTH measured 2 h after completion of thyroidectomy, defined as the maximal combined value of sensitivity and specificity, was 1.1 pmol/L for the entire cohort (AUC = 0.887; 95% confidence interval (CI): 0.839–0.934; Table 3). When the groups were analyzed separately, the optimal cut-off was 1.05 for the non-functional group (AUC: 0.944 (95% CI: 0.891–0.998)) and 1.55 pmol/L for the group with hyperthyroidism (AUC: 0.884 (95% CI: 0.832–0.936)). In Supplementary Table, a more detailed presentation of relationships, stratified by different PTH levels, is presented. Around 10% of patients with a postoperative PTH level between 1.1 and 1.6 pmol/L needed temporary calcium and/or vitamin D substitution.
The predictive values of a single measurement of parathyroid hormone (PTH) level 2 h after parathyroidectomy and the perioperative decline in PTH.
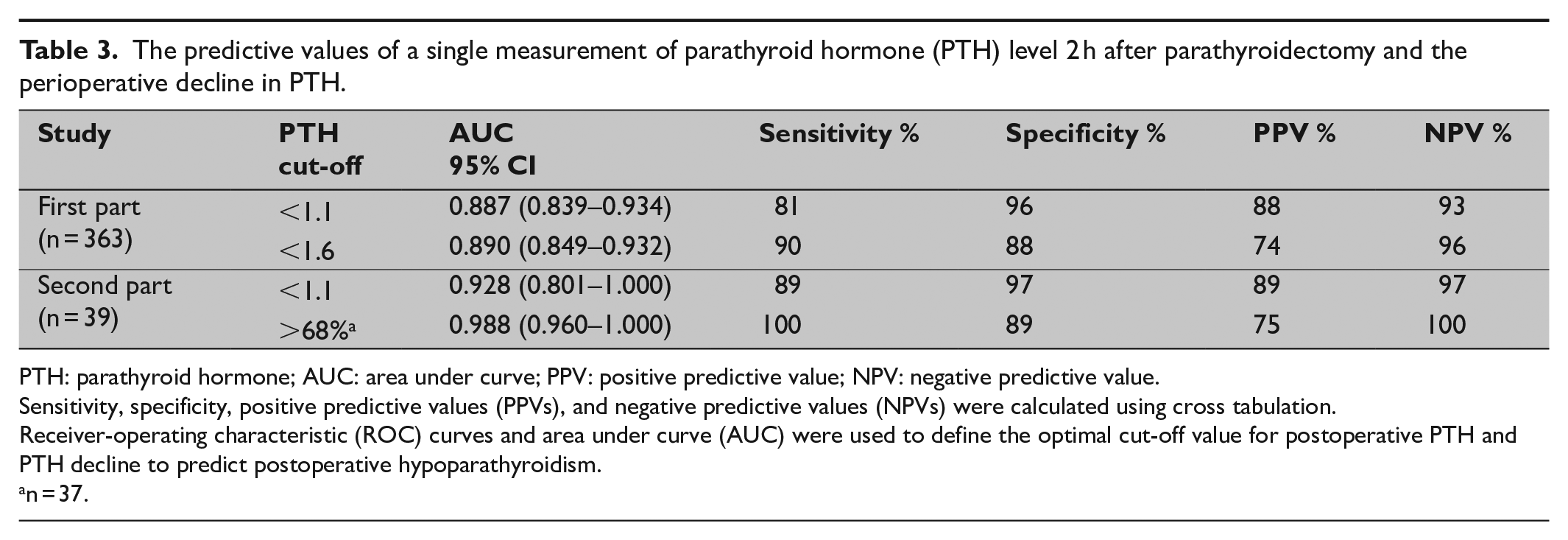
PTH: parathyroid hormone; AUC: area under curve; PPV: positive predictive value; NPV: negative predictive value.
Sensitivity, specificity, positive predictive values (PPVs), and negative predictive values (NPVs) were calculated using cross tabulation.
Receiver-operating characteristic (ROC) curves and area under curve (AUC) were used to define the optimal cut-off value for postoperative PTH and PTH decline to predict postoperative hypoparathyroidism.
n = 37.
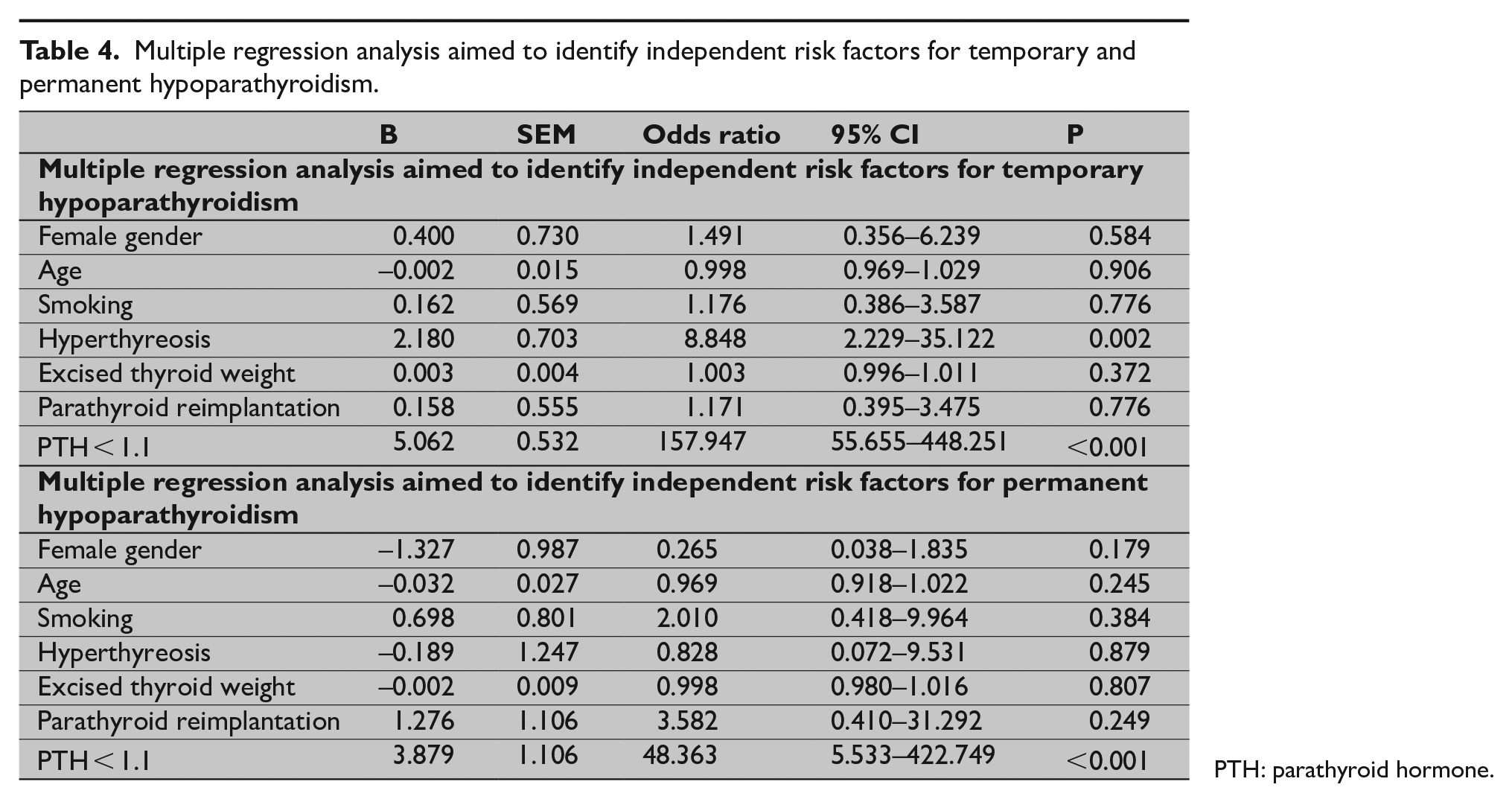
Multivariable analyses including gender, smoking, disorder (hyperthyroidism and non-functional goiter), reimplantation of parathyroid tissue and PTH level <1.1 pmol/L 2 h after thyroidectomy, identified hyperthyroidism, and a low PTH level as independent risk factors for early transient hypoparathyroidism. PTH < 1.1 pmol/L was the only independent risk factor for permanent hypoparathyroidism (odds ratio: 54; 95% CI: 6.4–451; Table 4). Only one patient with permanent hypoparathyroidism had had parathyroid reimplantation during the procedure.
Multiple regression analysis aimed to identify independent risk factors for temporary and permanent hypoparathyroidism.
PTH: parathyroid hormone.
Clinical characteristics and biochemical data of the 39 patients who completed the prospective study protocol are summarized in Table 2. The immediate preoperative PTH was higher compared to the measurement within 1 week prior to surgery (5.3 (4.2; 6.5) vs 4.5 (3.3; 6.0) pmol/L; P = 0.011), yet decreased postoperatively (2.4 (1.1; 4.0) 2 h after and 2.7 (1.1; 4.4) pmol/L the day after completion of thyroidectomy; P < 0.001). The iCa2+ was lowered the day after thyroidectomy (1.20 (1.15; 1.24) vs 1.25 (1.22; 1.27) mmol/L) and the phosphate level went up (1.4 (1.2; 1.6) vs 1.1 (0.96; 1.2) mmol/L; P < 0.001).
Nine patients, all females, were defined to have hypoparathyroidism. The optimal cut-off value for PTH decline was 68%. The iCa2+ levels remained within the normal range in four out of nine of these patients.
The diagnostic accuracy for the different measurements is presented in Table 3. Measurement of PTH decline added diagnostic value for one patient with preoperative vitamin D deficiency (39 nmol/L; normal range: 50–250 nmol/L; PTH preoperatively 10 vs 1.1 pmol/L 2 h after thyroidectomy, PTH decline 79%).
Six weeks after thyroidectomy, all but one patient had normalized parathyroid function and the median PTH level did not differ from the preoperative level (4.4 (3.0; 5.2); P = 0.220). The patient with persistent hypoparathyroidism was later diagnosed with vitamin D deficiency (25OHD: 33 nmol/L; iCa2+: 1.09 mmol/L; PTH: 2.2 pmol/L).
Discussion
The main result of this study was the high accuracy of a single PTH measurement 2 h after thyroidectomy for predicting temporary hypoparathyroidism. The optimal cut-off was defined as being higher in patients treated for hyperthyroidism, <1.6 vs <1.1 pmol/L. A postoperative PTH level <1.1 pmol/L was an independent risk factor for permanent hypoparathyroidism. Measurement of the perioperative decline added diagnostic value for one patient with vitamin D deficiency.
Hypoparathyroidism is the most common complication after thyroidectomy, and it has become clear that the incidence is much higher than previously reported. Early detection of hypoparathyroidism is essential in order to prevent discomfort and to guarantee patient safety. The reported prevalence of hypoparathyroidism after thyroidectomy differs widely, and incidences of temporary hypoparathyroidism, between 10% and 38%, have been reported5,12 –14.
Differences in definition of hypoparathyroidism and different diagnostic and treatment algorithms make comparisons between different cohorts difficult 2 . It is important to recognize that an iCa2+ below normal range does not necessarily manifest symptoms 15 . The recommended definition of hypoparathyroidism by the American Thyroid Association is a disorder in which the production of PTH is inadequate for maintaining a normal plasma calcium concentration 3 . Permanent hypoparathyroidism is defined as hypoparathyroidism at 6 months postoperatively but recovery may occur beyond 6 months, in some cases even after many years16 –18.
The consequence of untreated hypocalcemia is more serious compared to the risk of temporary overtreatment. From a clinical perspective, it is important to minimize the risk of false negatives. Thus, the NPV should be high but a moderate PPV is acceptable. The American Thyroid Association recommends a PTH measurement 1–2 h after surgery. Calcitriol supplementation is recommended for patients with postoperative PTH < 15 pg/mL (corresponding to about 1.6 pmol/L) 3 . However, the diagnostic accuracy of PTH measurement to predict hypoparathyroidism after thyroidectomy has been questioned. Sahli et al. measured PTH within 1 h after completion of thyroidectomy and found unacceptable, false-negative rates in predicting hypocalcemia 6 . The PTH decrease after thyroidectomy has been shown to be prolonged7,19. The results in this study are similar to the findings reported by Sywak et al. more than 10 years ago 8 . They defined a PTH limit of 10 pg/mL (corresponding to about 1.1 pmol/L and AUC: 0.90; CI: 0.81–0.96) 4 h after completed thyroidectomy where they felt comfortable discharging patients on the first postoperative day.
The occurrence of relative parathyroid insufficiency is another problem, and measuring of the perioperative decline in PTH has been reported to be preferable to a single postoperative measurement 11 . In a prospective study on 103 patients undergoing total thyroidectomy between 2009 and 2012, Schlottmann et al. showed that PTH decline, determined 3 h postoperatively, was a reliable predictor of hypocalcemia and a decline of >80% had a 100% specificity 20 . In our study, one patient would have been diagnosed based on perioperative decline in PTH, only. This diagnostic failure could probably have been avoided by preoperative optimizing treatment of 25-hydroxy vitamin D deficiency before thyroidectomy, as is recommended in the guidelines 5 . Our assessment is that a single postoperative measurement of PTH has cost and logistical advantages.
Several risk factors for hypoparathyroidism have been suggested, but the data are not fully consistent21 –26. Auto-transplantation of parathyroid glands has been associated with increased incidence of temporary hypoparathyroidism, and the protective effect against permanent hypoparathyroidism has been questioned12,27. In order to improve the chances for recovery from hypoparathyroidism, aggressive monitoring and replacement of calcium and activated vitamin D have been suggested 28 . It is advisable to maintain calcium levels in the low-normal or mildly subnormal levels given the risk of hypercalciuria, nephrocalcinosis, and deposits of calcium-phosphate complex in other soft tissues5,16. More research focusing on clinically relevant outcomes is necessary in order to receive higher-quality evidence for optimal management of postsurgical hypoparathyroidism 29 .
This study has limitations. Our algorithm to start treatment prior to analyzing the postoperative calcium level can be questioned as it may involve the risk of overtreatment and also the risk of underdiagnosis. Around 10% of patients with a postoperative PTH level between 1.1 and 1.6 pmol/L needed temporary calcium and/or vitamin D substitution, highlighting the importance of awareness and responsiveness to clinical symptoms of hypocalcemia. Furthermore, available data in the retrospective portion are limited and not all patients defined as having permanent hypoparathyroidism based on continuous prescription of active vitamin D and/or calcium have had a recent evaluation of parathyroid function. The strengths of the study are the systematic measurement of PTH 2 h after completed thyroidectomy and the validated diagnostic accuracy of the chosen cut-off, allowing early start of prophylactic treatment and postoperative monitoring aimed at minimizing symptoms and complications from hypoparathyroidism. The additive value of measurement of the perioperative PTH decline should be evaluated further in prospective studies.
Supplemental Material
sj-pdf-1-sjs-10.1177_1457496920913666 – Supplemental material for A single parathyroid hormone measurement two hours after a thyroidectomy reliably predicts permanent hypoparathyroidism
Supplemental material, sj-pdf-1-sjs-10.1177_1457496920913666 for A single parathyroid hormone measurement two hours after a thyroidectomy reliably predicts permanent hypoparathyroidism by David Palmhag, Jacob Brydolf, Jan Zedenius, Robert Bränström and Inga-Lena Nilsson in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Stockholm County Council and Karolinska Institutet.
Informed consent
Informed consent was obtained from all individual participants included in the study. Ethical approval for the study was received from the Regional Ethics Committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.