
Abstract
Introduction:
Gastrectomy with D2 lymphadenectomy is considered standard treatment in gastric cancer (GC). Among Western patients, morbidity and mortality seem to increase in D2 relative to D1 lymphadenectomy. As elderly patients with co-morbidities are more prone to possible complications, it is unclear whether they benefit from D2 lymphadenectomy. This study aims to compare the short- and long-term results of D1 and D2 lymphadenectomy in elderly patients undergoing gastrectomy for GC.
Methods:
All elderly (⩾75 years) patients undergoing gastrectomy with curative intent for GC during 2000–2015 were included and grouped according to the level of lymph node dissection into the D1 or D2 group. Short-term surgical outcome included the Comprehensive Complication Index (CCI) and 30-day mortality. Long-term outcomes comprised overall survival (OS), disease-specific survival (DSS), and disease-free survival (DFS). Cox regression was used in multivariable analyses.
Results:
In total, 99 elderly patients were included in the study (51 in D1 group, 48 in D2 group). The median follow-up was 32.5 months. Patients in the D1 group were older and had a higher American Society of Anesthesiologist (ASA) score. Both groups had similar burden of postoperative complications (CCI 20.9 versus 22.6, p = 0.26, respectively) and 90-day mortality (2% for both groups). The OS, DSS, and DFS were similar between groups. Multivariable analysis adjusted for potential confounders detected no difference in the survival between the D1 and D2 groups.
Conclusions:
Gastrectomy with D2 lymphadenectomy can be performed with low postoperative morbidity and mortality suggesting its use also in the elderly. Long-term outcomes seem similar but need further studies.
Introduction
Although the incidence of gastric cancer (GC) in Europe is declining, a growing number of elderly patients are surgically treated for GC due to longer life expectancy. This patient group is more prone to possible complications and increased mortality after surgery for GC.1 –4 Currently, gastrectomy with D2 lymphadenectomy is considered the standard treatment for GC, 5 as it is associated with improved long-term survival and similar postoperative mortality rates relative to D1 lymphadenectomy. 6 However, this more extensive surgery might increase the risk of morbidity in elderly patients while being of oncological benefit. 7 To reduce complications of surgery, it has been proposed that elderly patients should undergo gastrectomy with a D1 limited lymphadenectomy. 8 In contrast, a few Asian studies consider a standard D2 lymphadenectomy to be safe also for selected elderly patients.9,10 Most of the published studies have compared results and mortality between younger and elderly patients. 7
To date, only a few studies have compared the results of limited and standard lymphadenectomy in elderly patients.10,11 The aim of this study was to compare the safety and effectiveness of a standard D2 versus a limited D1 lymphadenectomy regarding morbidity and mortality. Our secondary aim was to assess the long-term survival between these two groups of elderly patients.
Method
This retrospective study was performed at Helsinki University Hospital (HUH). HUH is an academic teaching hospital functioning as a tertiary level referral center for GC surgery for a population of approximately 1.7 million. Patients were selected from an electronic operating room log with the International Classification of Diseases (ICD)-10 diagnosis code C16 (malignant neoplasm of stomach) and a procedure code for gastrectomy (JCD10, JDA96, JDC00, JDC10, JDC20, JDC30, JDC96, JDD00, and JDD96). The search was for the period from January 2000 to December 2015.
Data for eligible patients were manually extracted from patient records and included patient demographics, American Society of Anesthesiologist (ASA) class, medication, co-morbidities according to the Charlson Comorbidity Index, 12 laboratory parameters, oncological treatment, surgical details, hospital stay, ICU admission, and re-operations and re-admissions within 30 days of discharge. Complications were classified according to the Clavien-Dindo criteria, 13 and total burden of complications was assessed using the Comprehensive Complication Index (CCI). 14
Data collected from the pathology report determined histology according to the Lauren classification, 15 and staging was consistent with the AJCC TNM, 7th edition. Curative intent was defined as the aim of R0 resection assessed by the surgeon intra-operatively. R0 resection was defined as a successful removal of all cancerous tissue with microscopic margins of more than 1 mm, and R1 was defined with macroscopic removal of all cancerous tissue with microscopic margins 1 mm or less. Also, patients with a TXNXM1 tumor could have undergone R0 resection if all the metastases were removed during surgery. Surgery in which R0 resection was not possible was considered palliative, and these patients were excluded from the study. Recurrence was defined as a recurrence detected either on imaging studies (usually computed tomography (CT)) or during surgery or endoscopy. In our institution, imaging studies are used in the follow-up only in cases of symptoms or suspicion of recurrence (e.g. elevated Carcinoembryonic Antigen (CEA) or CA19-9 levels). Long-term follow-up was performed by manually gathering hospital patient records and data from the Population Registry Center. The Population Registry Center is an up-to-date service provided by the government that maintains reliable records of the population. This registry provides information on whether a person is alive or deceased. The last observation date of the patient, a possible recurrence, long-term mortality, or cause of death was collected from hospital patient records. If the follow-up was not carried out at HUH, the patient records were obtained from the referring hospital.
Elderly patients were selected either for standard D2 or limited D1 lymphadenectomy, and this was determined by the operating surgeon. Information on the extent of lymphadenectomy was derived from the operative report. The threshold for an elderly patient was set up at ⩾75 years accordingly. 16
All statistical analyses were conducted using SPSS®, Version 25 (IBM, Armonk, NY, USA). Continuous variables were analyzed with t test (normally distributed) or Mann–Whitney U-test (non-normally distributed). Normally distributed continuous variables are reported as mean (standard deviation (SD)) and non-normally distributed variables as median (interquartile range (IQR)). Categorical variables were analyzed with chi-square or Fisher exact test (if number of events per cell <5). The Cox proportional hazards model was used for multivariate analysis. Survival was calculated using the Kaplan-Meier method with log-rank test. All tests were two-sided, and p values < 0.05 were considered significant. The study was approved by the institutional and ethics review boards and the Finnish Institute for Health and Welfare.
Results
Altogether 475 patients underwent gastrectomy for GC between 2000 and 2015, and seven patients were excluded due to missing records. Of all patients, 132 were elderly (⩾75 years). In total, 33 elderly patients did not undergo gastric resection with curative intent, thus leaving 99 elderly patients in the final study cohort. Fifty-one elderly patients underwent D1 lymphadenectomy (D1 group) and 48 elderly patients underwent D2 lymphadenectomy (D2 group). The annual proportion of these procedures remained the same throughout the study period.
Basic characteristics of the patients are shown in Table 1. Patients in the D1 group were older, had higher ASA class, and had more frequently cerebrovascular disease and anticoagulation medication than patients in the D2 group, but other basic characteristics were similar between the groups. Neoadjuvant EOX therapy was received by three (5.9%) patients in the D1 group and by four (8.3%) patients in the D2 group (p = 0.71). In the D1 group, two patients received the fully scheduled 3 + 3 cycle program, and one patient received only 3 + 2 due to improper blood values. In addition, one patient received another postoperative treatment regimen. In the D2 group, only one patient received the 3 + 3 cycle perioperative treatment regimen. Two patients declined postoperative EOX therapy, and one did not receive this due to unspecified reasons. Four patients received another postoperative chemotherapy.
Basic characteristics.
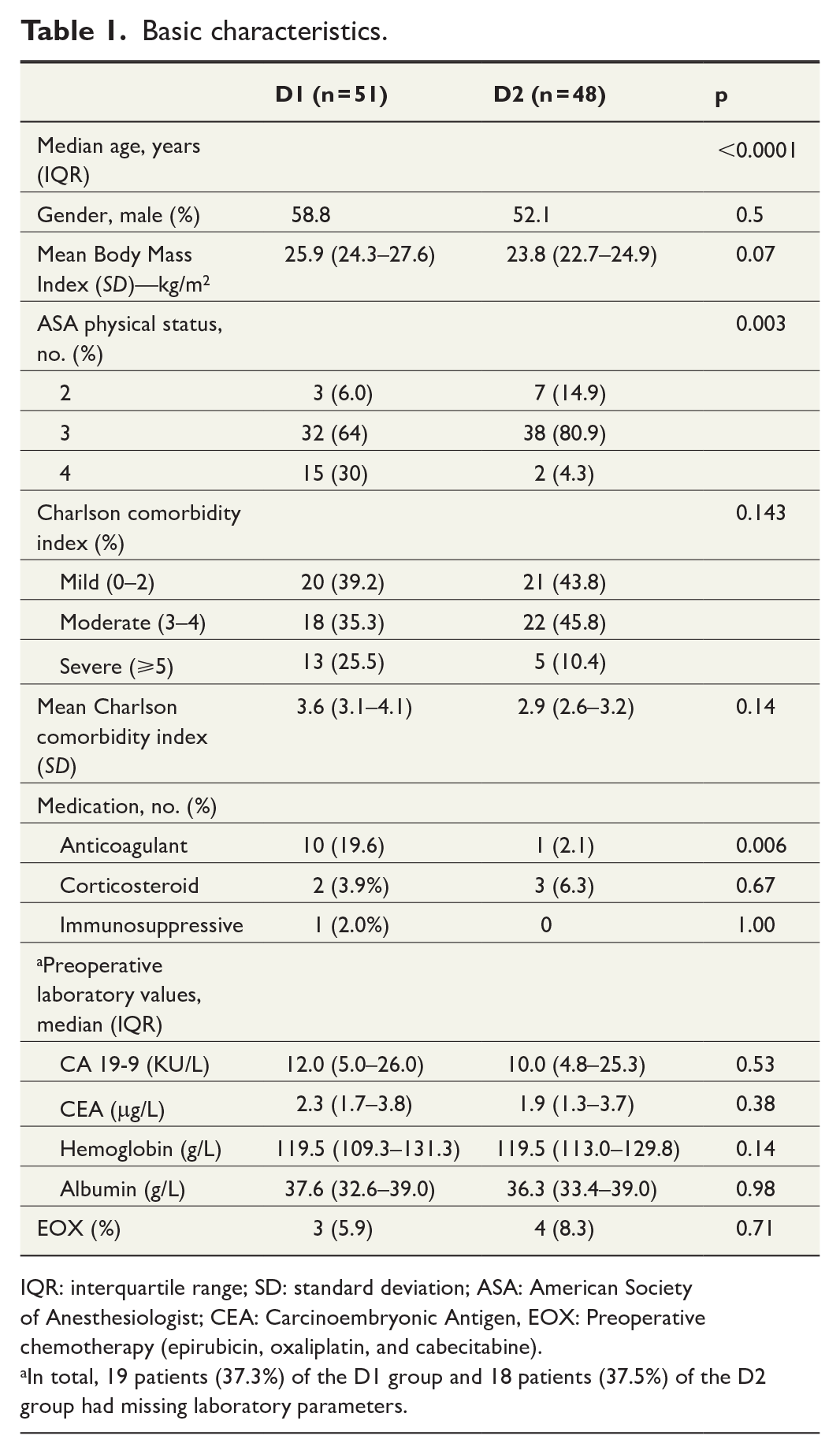
IQR: interquartile range; SD: standard deviation; ASA: American Society of Anesthesiologist; CEA: Carcinoembryonic Antigen, EOX: Preoperative chemotherapy (epirubicin, oxaliplatin, and cabecitabine).
In total, 19 patients (37.3%) of the D1 group and 18 patients (37.5%) of the D2 group had missing laboratory parameters.
With respect to gastrectomy or operative time, no significant difference between the groups was observed. Laparoscopic approach was more common in the D1 group, with a conversion rate of 33% (p = 0.013). Moreover, splenectomy rate (p = 0.001) and intra-operative bleeding (p = 0.003) were significantly higher in the D2 group (Table 2).
Operative details.
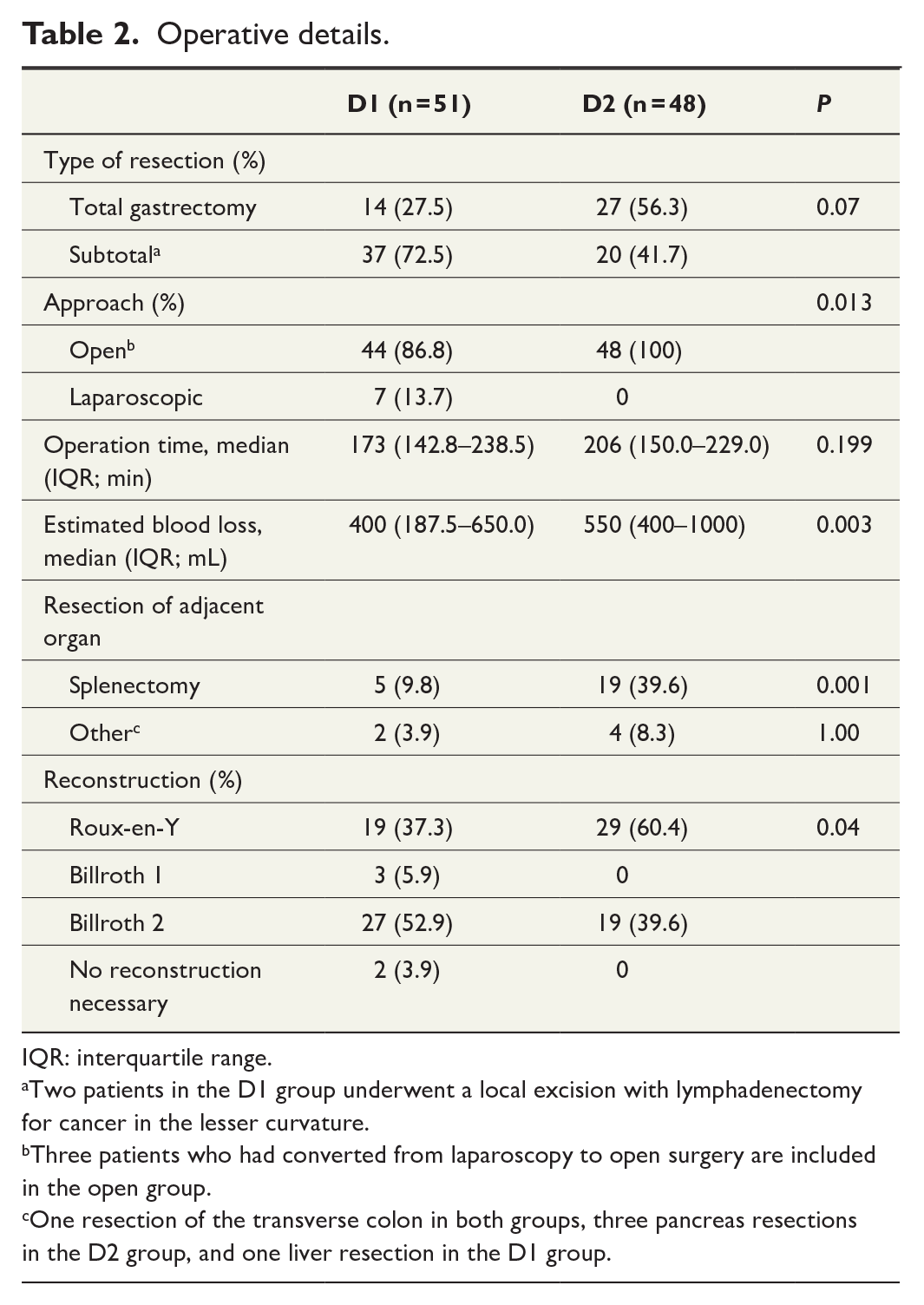
IQR: interquartile range.
Two patients in the D1 group underwent a local excision with lymphadenectomy for cancer in the lesser curvature.
Three patients who had converted from laparoscopy to open surgery are included in the open group.
One resection of the transverse colon in both groups, three pancreas resections in the D2 group, and one liver resection in the D1 group.
Morbidity and mortality were similar in both groups (Table 3). Rate of severe complications (Clavien-Dindo Grades III, IV, and V) was 17.6% in the D1 and 20.8% in the D2 group. ICU admissions were 19.6% and 6.3%, respectively. The number of ICU days was significantly higher in the D1 group (p = 0.04). Re-operation was performed on two patients (3.9%) in the D1 group and on three patients (6.3%) in the D2 group. All re-operations were due to anastomotic leakage. Length of stay and re-admissions did not differ between the groups (Table 3).
Postoperative details.
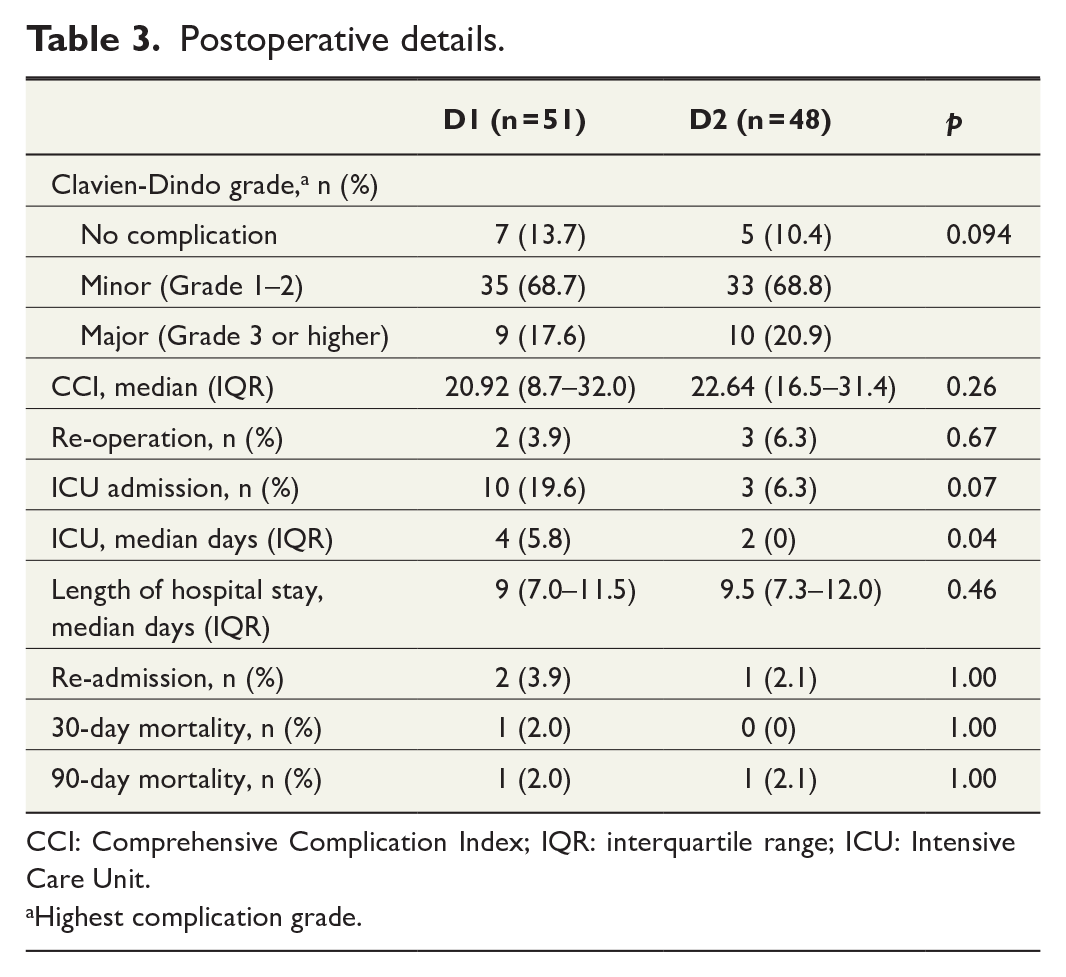
CCI: Comprehensive Complication Index; IQR: interquartile range; ICU: Intensive Care Unit.
Highest complication grade.
One patient (2.0%) died of oesophago-jejunal anastomosis leakage in D1 group within 30 days. In the D2 group, one patient treated for anastomotic leak died for unknown reason within 90 days of discharge.
Histology, tumor location, and depth of invasion were not significantly different between the groups (Table 4). Lymph node involvement and tumor stage did not differ between the two groups. However, tumor size (p = 0.03) and the number of harvested lymph nodes (p = 0.0001) were significantly greater in the D2 group (Table 4).
Pathological details.
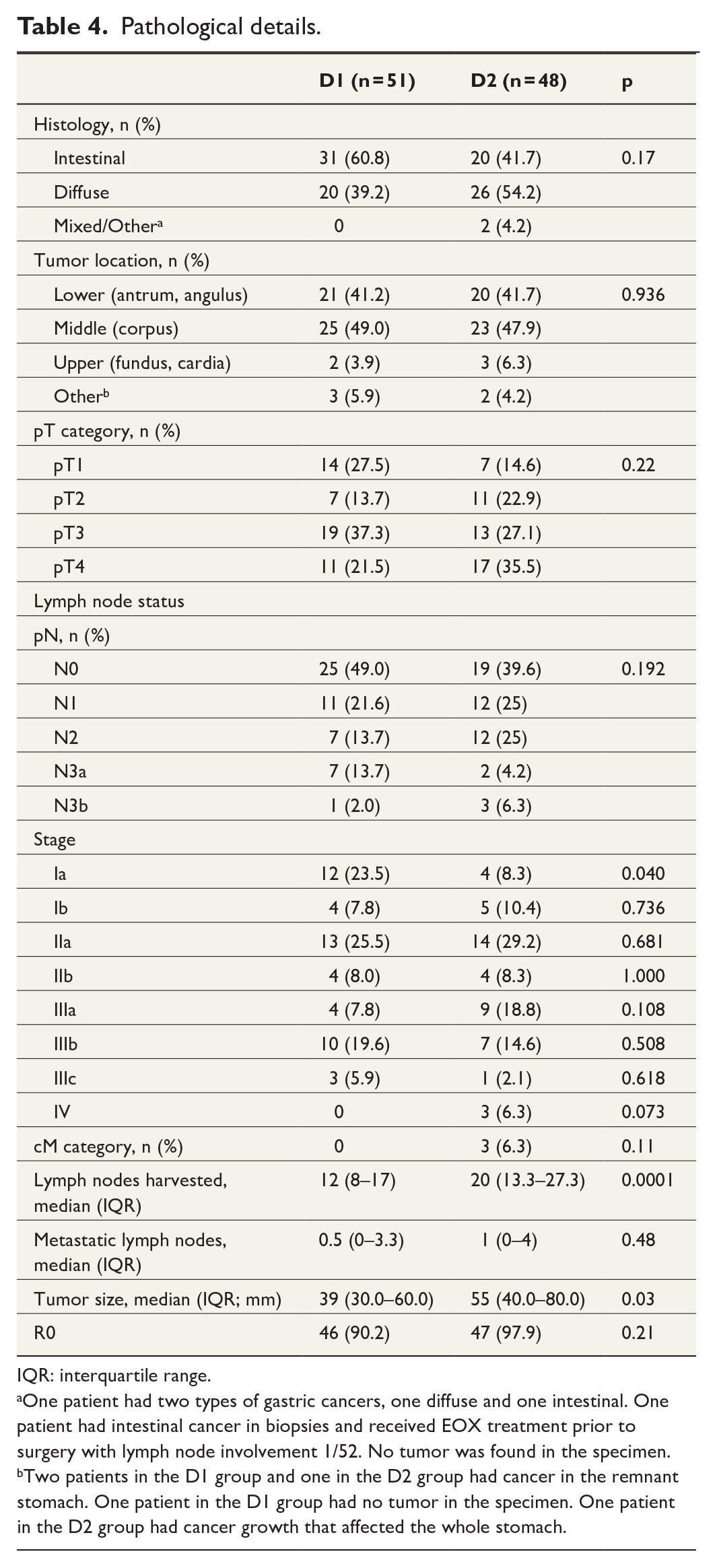
IQR: interquartile range.
One patient had two types of gastric cancers, one diffuse and one intestinal. One patient had intestinal cancer in biopsies and received EOX treatment prior to surgery with lymph node involvement 1/52. No tumor was found in the specimen.
Two patients in the D1 group and one in the D2 group had cancer in the remnant stomach. One patient in the D1 group had no tumor in the specimen. One patient in the D2 group had cancer growth that affected the whole stomach.
Overall survival (OS), disease-specific survival (DSS), and disease-free survival (DFS) were similar between D1 and D2 groups (Figs. 1 to 3). The median follow-up time was 32.5 months (IQR = 14.9–65.7): 31.7 months (IQR = 15.0–65.0) for the D1 group and 34.0 months (IQR = 13.9–70.4) for the D2 group. Median estimated OS was 32.7 months (95% confidence interval (CI) = [16.1, 49.0]) in the D1 group and 31.7 months (95% CI = [6.2, 57.2]) in the D2 group. Median estimated DSS was 65.2 months (95% CI = [27.6, 102.7]) in the D1 group and 69.5 months (95% CI = [36.1, 102.9]) in the D2 group. Median estimated DFS was 31.7 months (95% CI = [9.5, 53.9]) in the D1 group and 32.5 months (95% CI = [21.0, 44.1]) in the D2 group. The D1 and D2 groups were similar in OS, DSS, and DFS. In a sensitivity subgroup analysis for patients with N– or N+ categories, there was no statistical difference in OS, DSS, or DFS between D1 and D2 groups. Furthermore, in T1–2 and T3–4 patients, no difference in DFS emerged.
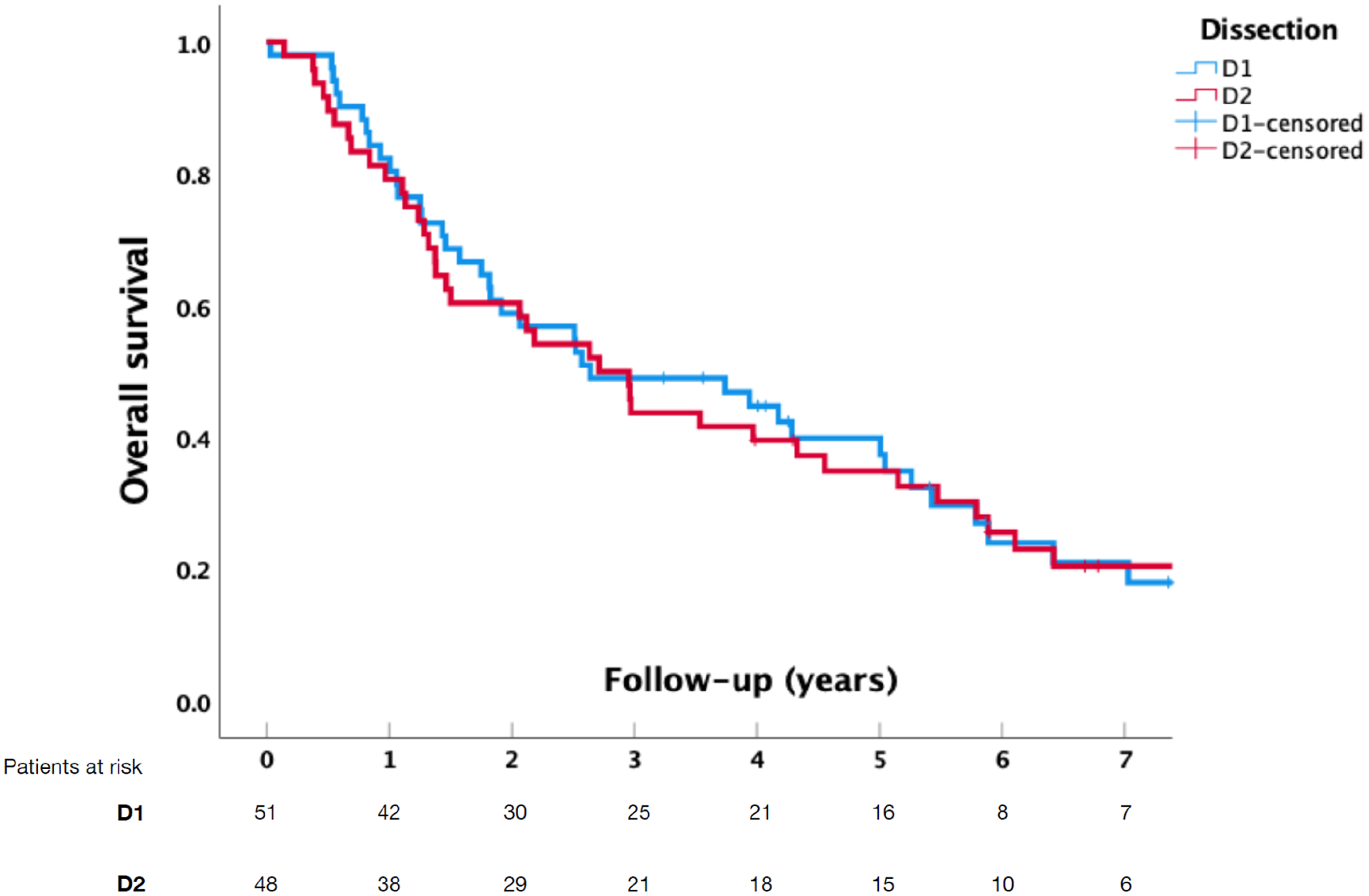
Overall survival in patients undergoing D1- or D2-lymphadenectomy for gastric cancer (p = 0.817).
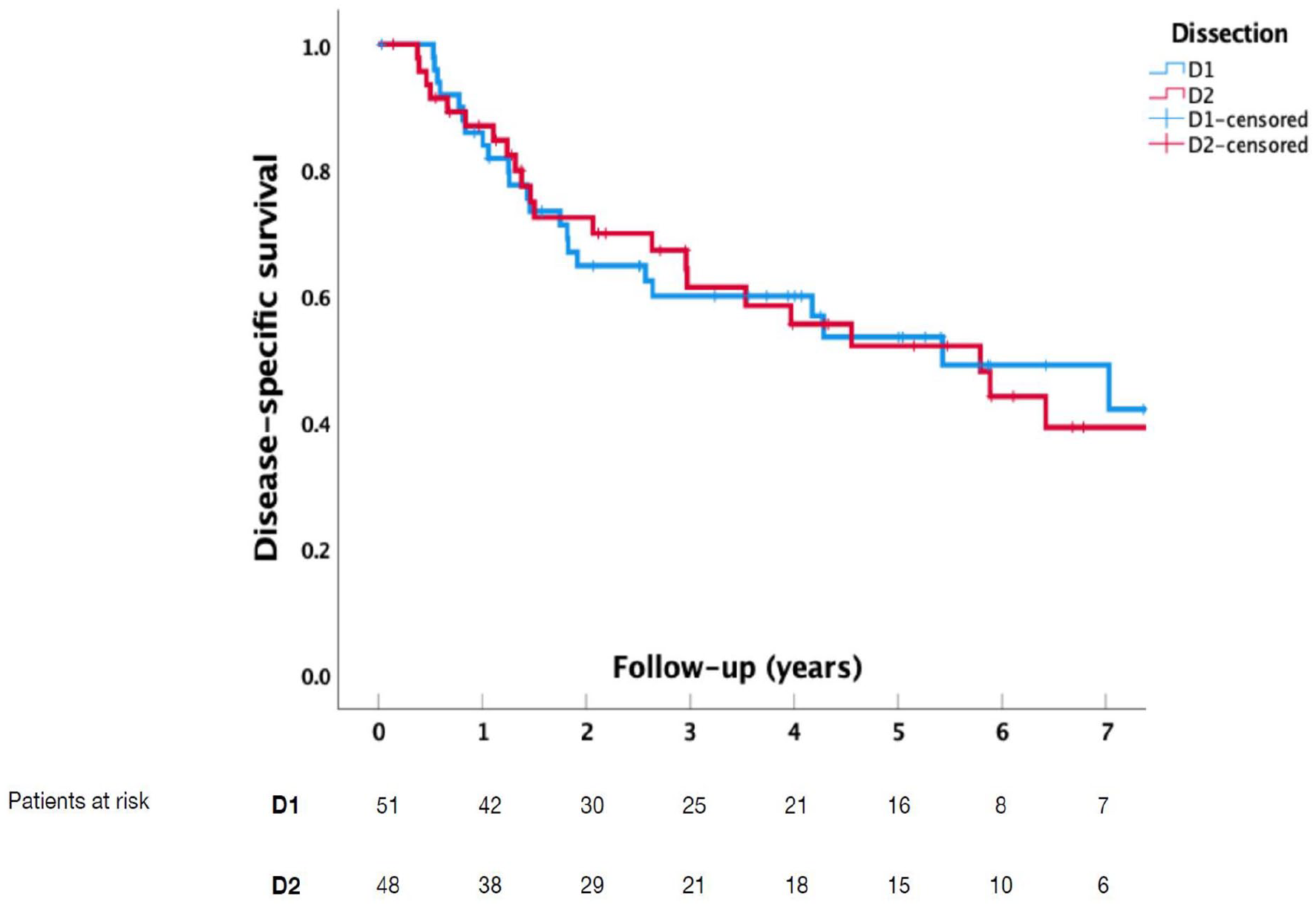
Disease-specific survival in patients undergoing D1- or D2-lymphadenectomy for gastric cancer (p = 0.911).
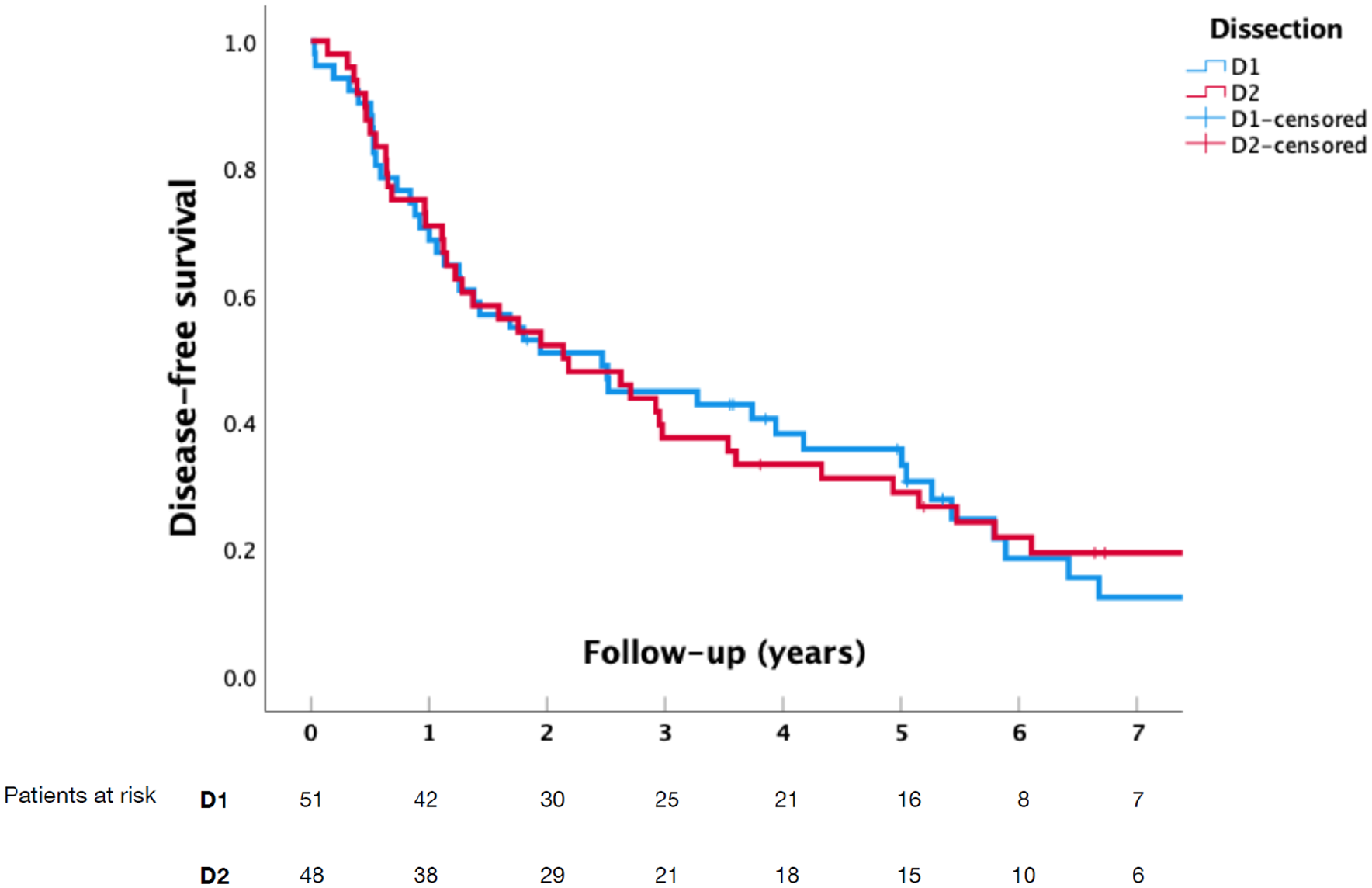
Disease-free survival in patients undergoing D1- or D2-lymphadenectomy for gastric cancer (p = 0.852).
When adjusted for age, Charlson comorbidity index, ASA class, N-positivity, and T-category (T1, T2, T3, or T4), D2 dissection (compared with D1 dissection) was not associated with OS (hazard ratio (HR) = 1.239, 95% CI = [0.712, 2.158], p = 0.448), DSS (HR = 1.224, 95% CI = [0.584, 2.564], p = 0.592), or DFS (HR = 1.160, 95% CI = [0.675, 1.994], p = 0.592).
Discussion
This is one of the few studies to compare the outcomes of D1 and D2 lymph node dissection in elderly GC patients. The findings suggest that standard D2 lymphadenectomy is safe in selected elderly patients concerning postoperative mortality and morbidity. Regarding OS, DSS, or DFS, no difference emerged between the two groups.
Traditionally, D2 lymphadenectomy for GC in Europe has been linked to higher postoperative morbidity and mortality. 17 This undoubtedly leads to caution regarding surgery in elderly patients. However, during the past decade, the trend has shifted in Europe toward more extensive surgery even in the elderly.7,18,19 This might be due to aging of the population in Europe and surgery becoming more centralized in several countries. Simultaneously, safer, minimally invasive, and spleen- or pancreas-preserving techniques have been introduced.20,21 Consequently, more elderly people with co-morbidities are undergoing GC surgery and are susceptible to complications. In the elderly, surgery is risky partially due to lack of functional reserves. 2
We did not detect any difference in complications or mortality between the D1 and D2 groups. This may be due to the fact that D1 patients were older and frailer despite laparoscopy being more commonly used in this group. The 90-day mortality rate was 2.0% for both groups. Our study demonstrates that GC surgery in the elderly is possible, with low postoperative morbidity and mortality rates. This is concordant with previous studies reporting low morbidity and mortality when comparing young and old GC patients.22,23 In a recent Dutch publication, 24 mortality was not considered to be significantly influenced by age. However, ASA grade, chemotherapy, and type of resection were associated with morbidity and mortality. 24 Mikami et al. 10 divided elderly patients according to the type of surgery into limited (D1) or standard (D2) groups. They concluded that standard surgery is safe in the elderly regarding morbidity and mortality. Male gender and poor nutritional status were associated with worse outcomes. Hence, these individuals were considered candidates for limited surgery. 10
Long-term results in our study were similar for both groups. To reduce complications of surgery, few studies suggest a D1 limited lymphadenectomy in elderly patients undergoing GC surgery.8,25 Rausei et al. 11 could not detect a significant improvement of the OS due to a high complication rate in the elderly GC patients undergoing D2 lymphadenectomy. They concluded that D1 lymphadenectomy should be considered in these patients. In our study, D2 lymphadenectomy seemed not to improve OS or DSS compared with D1 lymphadenectomy. Mikami et al. 10 reported a significantly lower overall 5-year survival rate in the limited group; this became increasingly evident as the stage of the disease advanced. We conducted a multivariate analysis to overcome the issue of any imbalance between the groups. However, this failed to uncover any long-term differences between the two groups. Furthermore, total gastrectomy and splenectomy were more common in the D2 group, which are related to increased postoperative and long-term morbidity.20,21,24
The main strengths of this single-center study are a reliable long-term follow-up. The patients were gathered over a 16-year period. This study also has some limitations. First, the sample size is small, and the nature of the study is retrospective. This is due to the incidence of GC being low in Finland, on average just less than 700 cases a year distributed over five university hospitals. This is, however, a limitation common to all Western series due to the rarity of GC. Second, our study groups did not match in relation to age, ASA class, cerebrovascular disease, and anticoagulative medication. We also understand the potential risk of a selection bias regarding the extent of the lymphadenectomy.
Our results demonstrate that gastrectomy with D2 lymphadenectomy in selected elderly patients is possible, with low postoperative morbidity and mortality rates suggesting its use. D2 lymphadenectomy had morbidity and mortality similar to D1 lymphadenectomy. However, long-term outcomes did not differ between D1 and D2 lymphadenectomy groups of elderly GC patients. Further prospective, preferably randomized studies are required to assess the benefits of D2 lymphadenectomy for GC in elderly patients.
Footnotes
Acknowledgements
The authors thank Alli Leppä, Phd, for the contribution to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Abdominal Surgery, Helsinki University Hospital and University of Helsinki, Hyvinkää Hospital Area, The Medical Society of Finland.