
Abstract
Background and objective:
During the last decades, laparoscopic surgery has been introduced as an alternative to open surgery. We aimed to examine to what extent laparoscopic surgery has replaced open surgery for appendicitis in an entire nation during the last two decades. Second, we examined the effects of shifting to laparoscopic surgery for appendicitis on different quality indicators such as length of postoperative stay and mortality. We also examined age as a predictor of 30-day mortality.
Methods:
During the period 2000 to 2015, all adult patients with appendicitis and surgical removal of the appendix were identified in the Danish National Patient Register. Demographics, type of surgery, time of surgery, and duration of postoperative stay were retrieved form Danish National Patient Register. Vital status was retrieved from the Danish Civil Registration System.
Results:
A total of 58,093 patients underwent surgery for appendicitis. In 2000, a total of 274 out of 3717 (7.4%) had a laparoscopic appendectomy, and the postoperative stay was 55 (iqr: 35–88) h and 30-day mortality was 0.91%. In 2015, a total of 3995 out of 4296 (93.0%) had a laparoscopic appendectomy, and the postoperative stay was 16 (iqr: 9–56) h and 30-day mortality was 0.40%. Age as a predictor of 30-day postoperative mortality had an area under the curve of 0.93 (95% confidence interval: 0.92; 0.94).
Conclusions:
In Denmark, the standard surgical procedure for appendicitis has changed from open surgery to laparoscopic surgery during the period 2000–2015. At the same time, duration of postoperative stay and 30-day mortality has decreased.
Introduction
Surgery for appendicitis is the most common acute abdominal procedure. 1 Laparoscopic surgery has been introduced over the last two decades and laparoscopic surgery for appendicitis has been shown to reduce pain, in-hospital stay, and the return to normal activities. 2 Mortality after appendectomy is generally low, although highly dependent on age.3 -5
The extent to which the laparoscopic procedure has replaced open surgery for appendicitis in Denmark remains unknown. Furthermore, the effects on quality indicators such as delay and timing of surgery, duration of postoperative stay, and short-term mortality, remains unknown after a nationwide transition from an era of open surgery to an era of laparoscopic surgery for appendicitis.
In recent years, there has been an increased focus on acute high-risk abdominal surgical patients. Acute high-risk surgery has been defined as surgery with a 30 -day mortality above 5%.6,7 Most studies on acute high-risk abdominal surgery exclude patients with appendicitis and defines acute high-risk abdominal surgical patients solely on the type of procedure they undergo.8,9 There is increased short-term mortality among older patients after abdominal surgery. 10 Identifying patients at high risk based only on type of surgery without regards to patient characteristics may be erroneous. There is a need for individual risk assessment.
We aimed, to investigate the extent to which surgical practice has changed from open to laparoscopic surgery for appendicitis in adults over the last decades and the effect of such a transition on specific quality indicators. Finally, we examined whether surgery for appendicitis in the elder patient should be classified as acute high-risk abdominal surgery.
Material and methods
The Danish Data Protection Agency and the Danish National Health Authority approved this nationwide cohort study.
Patients
All patients aged 18 or above between 2000 and 2015 were included if they had a diagnosis of appendicitis and surgical removal of the appendix. The study is reported according to the STROBE statement. 11
Data and data sources
From the Danish National Patient Register 12 , patients with a diagnosis of appendicitis were identified using the codes for appendicitis (K35, K36, K37) according to the International Classification of Disease, version 10 (ICD-10). Information on date and time of admission, date and time of surgery, date and time of discharge, and type of surgery performed according to the NOMESCO classification was also retrieved. 12 The diagnosis of appendicitis in the Danish National Patient Register has previously been validated.13,14
Based on the ICD-10 codes, patients were classified as having uncomplicated appendicitis (K35, K35.8, K35.8A, K35.8B, K35.8 C, K35.9, K35.9A, K35.9B, K36, K36.9, K37, K37.9) and complicated appendicitis (K35.0, K35.0A, K35.1, K35.1A, K35.2, K35.3, K35.3A, K35.3B).
All patients identified through the Danish National Patient Register were linked to the Danish Civil Registration System. 15 Through the Civil Registration System, vital status of the patients (dead, alive, emigrated etc.), date of vital status, gender, and date of birth were obtained.
The annual total mid-year population and number of deaths for the general Danish population each year stratified by sex and age groups (18–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, 95+) were retrieved from Statistics Denmark.
Outcomes
The main outcome was the annual percentage of patients undergoing surgery for appendicitis who had a laparoscopic appendectomy performed. Second, we examined the incidence of appendicitis and the effect of a shift in surgical practices on quality indicators.
The following were chosen as quality indicators based on clinical relevance and a possibility that a change in procedure could have an effect on the indicator: Delay from admission to surgery, whether the procedure was performed during daytime (08:00–16:00), in the evening (16:00–24:00), or at night (00:00–08:00), duration of postoperative stay, 30-day postoperative mortality, and standardized 30-day mortality rate.
Finally, the discriminative power of age for 30-day mortality and the discriminative power of age regarding identification of patients classified as acute high-risk surgical patients with a mortality of 5% or above were examined.
Statistical analyses
Continuous data are presented as median and interquartile range. Categorical data are presented as percentage.
The incidence was calculated as the number of new cases each year divided by the mid-year population size each year. The 30-day postoperative mortality risk was defined as the number of deaths per 100 patients undergoing appendectomy for appendicitis. The standardized 30-day mortality ratio was calculated based on the observed number of deaths among the patients divided by the expected number of deaths. The expected number of deaths was calculated by multiplying the annual age and sex-specific 30-day mortality rates in the general population with the number of patients by the same age and sex groups. These numbers were then summed to the total expected number of deaths. The age- and sex-specific 30-day mortality rates for the general population was calculated based on information retrieved from Statistics Denmark as the annual number of deaths divided by the mid-year population divided 365.24 and multiplied by 30 assuming that the mortality rate is stable throughout the year.
For the discriminate power of age regarding 30-day postoperative mortality, a receiver operating characteristic (ROC) curve was constructed and the area under the curve (AUC) calculated. 16 The optimal cut-off point for age regarding the 30-day postoperative mortality according to the Youden index and for a 5% postoperative 30-day mortality was identified, and the sensitivity and specificity were calculated. The Youden index gives equal weight to sensitivity and specificity. The ROC curve is shown with cut-off points for a 1%, 5%, and 10% 30-day mortality.
Mortality curves were constructed using a LOESS smoothing curve with a 95% confidence interval.
Analyses were performed with R (R Core Team (2015). R: A language and environment for statistical computing (R Foundation for Statistical Computing, Vienna, Austria). URL https://www.R-project.org/) using RStudio (RStudio Team (2015). RStudio: Integrated Development for R. RStudio, Inc., Boston, MA, (http://www.rstudio.com/).
Results
From 2000 to 2015, a total of 58,093 adult patients had a diagnosis of appendicitis and surgical removal of the appendix. There was some variation in the incidence of appendicitis over time (Fig. 1). The variation was most pronounced for the younger age groups and seemed to stabilize in the elder age groups. Overall the incidence was stable over time. However, there was a clear drop in the proportion of complicated appendicitis from 2011 to 2012 where after it remained stabilized. The incidence of complicated appendicitis seems unchanged during the different decades of life while the incidence of uncomplicated appendicitis decrease with increasing age. In the entire cohort, 29,713 (51.1%) patients were male, and the median age at surgery for appendicitis was 38 (iqr: 26–55) years and ranged from 18 to 100 years. The annual gender and age distributions were stable over time and the proportion of males was between 50% and 53% and the median age between 36 and 39 years.
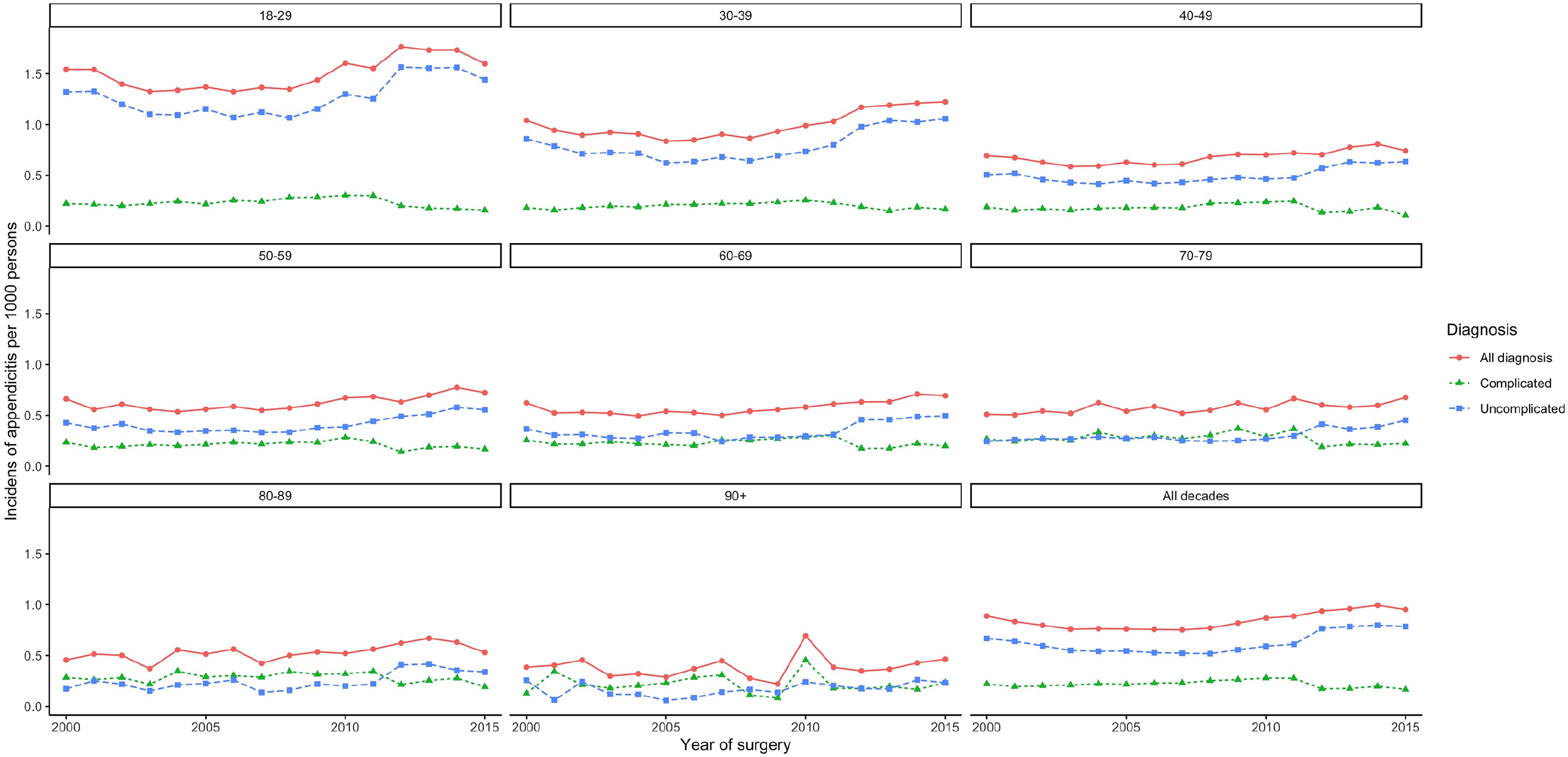
Annual incidence rate of appendicitis stratified by age from 2000 to 2015.
A laparoscopic appendectomy was performed in 274 out of 3717 (7.4%) patients having surgery for appendicitis in 2000. This changed gradually until 2015 when 3995 out of 4296 (93.0%) patients having surgery for appendicitis had a laparoscopic appendectomy performed. The ratio of appendectomies performed each year as laparoscopic appendectomies is presented in Fig. 2 stratified by age. The use of laparoscopy seems to be introduced later for elder age groups.
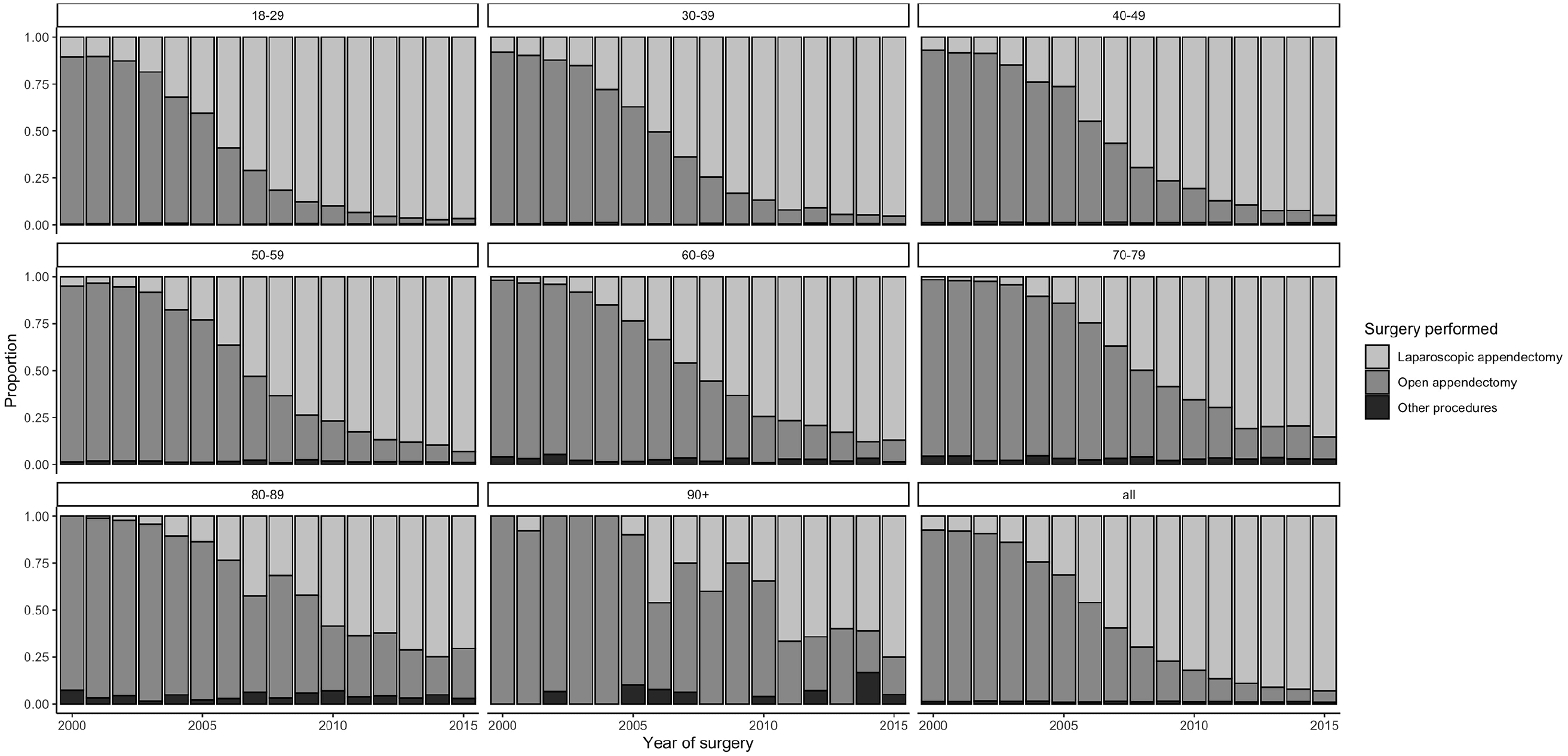
Type of surgery performed in patients operated for appendicitis from 2000 to 2015.
The delay from admission to surgery was 7 (iqr: 4–12) h in 2000 and increased to 10 (iqr: 6–17) h in 2010 and then declined to 9 (iqr: 4–14) h in 2015 (Fig. 3A).
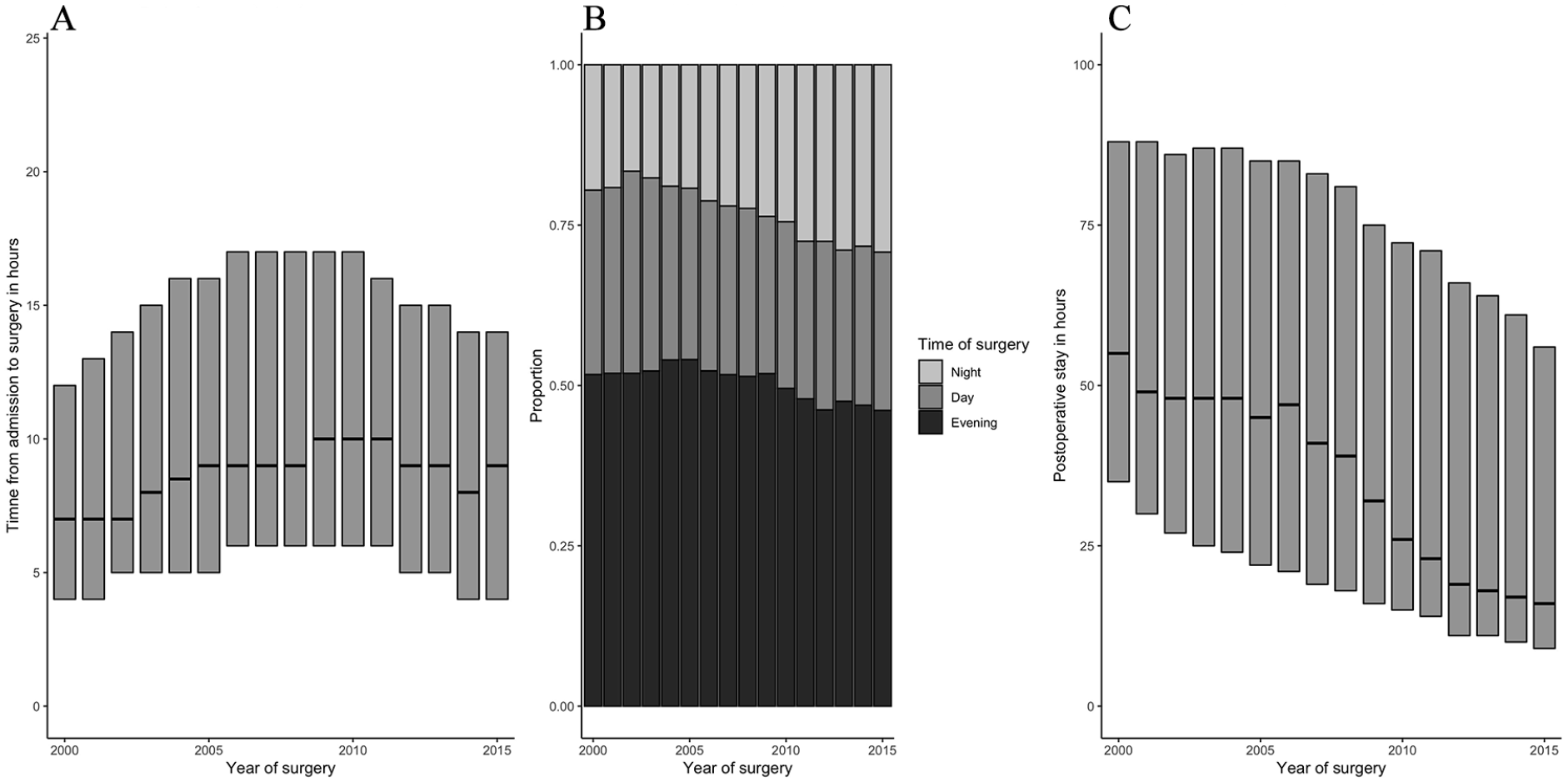
The timing of surgery for appendictis and duration of postoperative stay: (A) Delay from admission to surgery in hours presented as median and interquartile range. (B) Time of day for surgery is defined as night is 00:00 to 07:59, day is 08:00 to 15:59, and evening is 16:00 to 23:59. (C) Duration of postoperative stay in hours presented as median and interquartile range.
There seems to be a slight increase in the number of procedures performed at night and a slight decline in the number of procedures performed in the evening and daytime (Fig. 3B).
The duration of postoperative in-hospital stay declined from a median of 55 (iqr: 35–88) h in 2000 to 16 (iqr: 9–56) h in 2015 (Fig. 3C).
During the period 2000–2015, a total of 374 out of 58,093 patients died within 30 days after surgery for appendicitis, and the overall mortality risk was 0.64%. The 30-day mortality risk following surgery for appendicitis showed a clear decline from 0.91% in 2000 to 0.40% in 2015 (Fig. 4A). The standardized 30-day mortality ratio showed a similar decrease in mortality (Fig. 4D). For uncomplicated appendicitis, the mortality rate was 0.25% in 2000 and 0.20% in 2015 and constant over time (Fig. 4B and E) while the mortality for complicated appendicitis decreased from 2.93% in 2000 to 1.34% in 2015 (Fig. 4C and F). The largest absolute changes in mortality were seen in the elderly population above 70 years (Fig. 4G, H, and I).
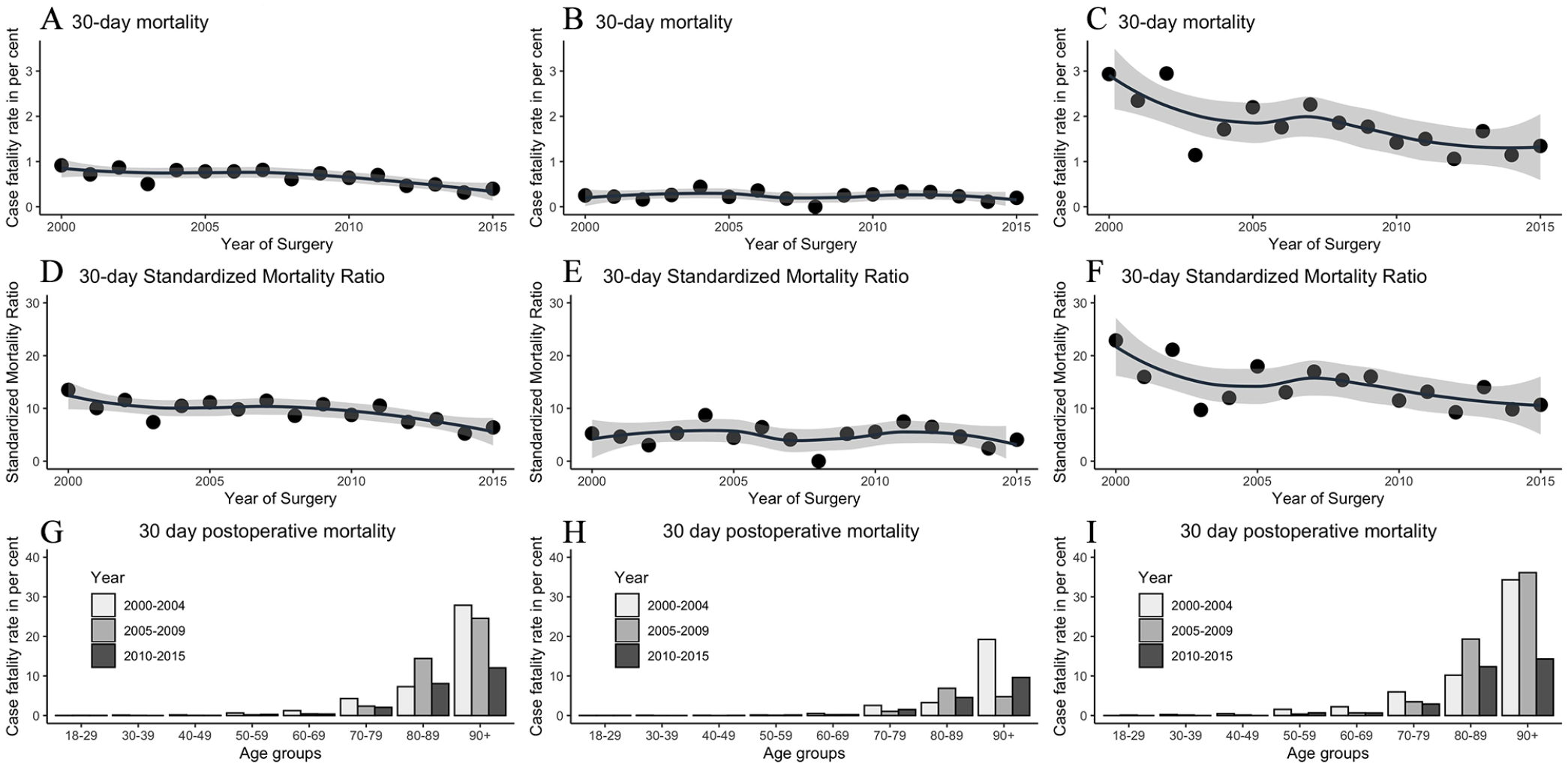
The 30-day postoperative case fatality rate in percentage during the period 2000–2015 for all diagnosis(A), uncomplicated appendicitis (B), and complicated appendicitis (C). The 30-day postoperative standardized mortality ratio from 2000 to 2015 for all diagnosis (D), uncomplicated appendicitis (E), and complicated appendicitis (F). The 30-day postoperative case fatality rate in percentage for age groups divided into decades for all diagnosis (G), uncomplicated appendicitis (H), and complicated appendicitis (I).
Increased age was associated with increased mortality risk (Fig. 4G, H, and I). The 30-day mortality risk was almost zero until the sixth decade of life after which it starts to increase and reaches almost 10% at the ninth decade of life and 19% during the tenth decade of life in the era of open appendectomies. For most age groups, there was a decrease in postoperative mortality during the study period (Fig. 4G, H, and I). The AUC was 0.93 (95% confidence interval (CI): 0.92; 0.94) for age as a discriminant for the 30-day mortality risk. The optimal cut-off point according to the Youden index was 67 years, giving a sensitivity of 0.84 (95% CI: 0.80; 0.88) and a specificity of 0.89 (95% CI: 0.88; 0.89). The cut-off point for a 30-day postoperative mortality of 5% was at the age of 69 years yielding a sensitivity of 0.81 (95% CI: 0.77; 0.85) and a specificity of 0.90 (95% CI: 0.90; 0.91). The ROC curve for age as a discriminant for 30-day mortality is shown in Fig. 5 together with cut-points for 1%, 5%, and 10% mortality within 30-days after surgery.
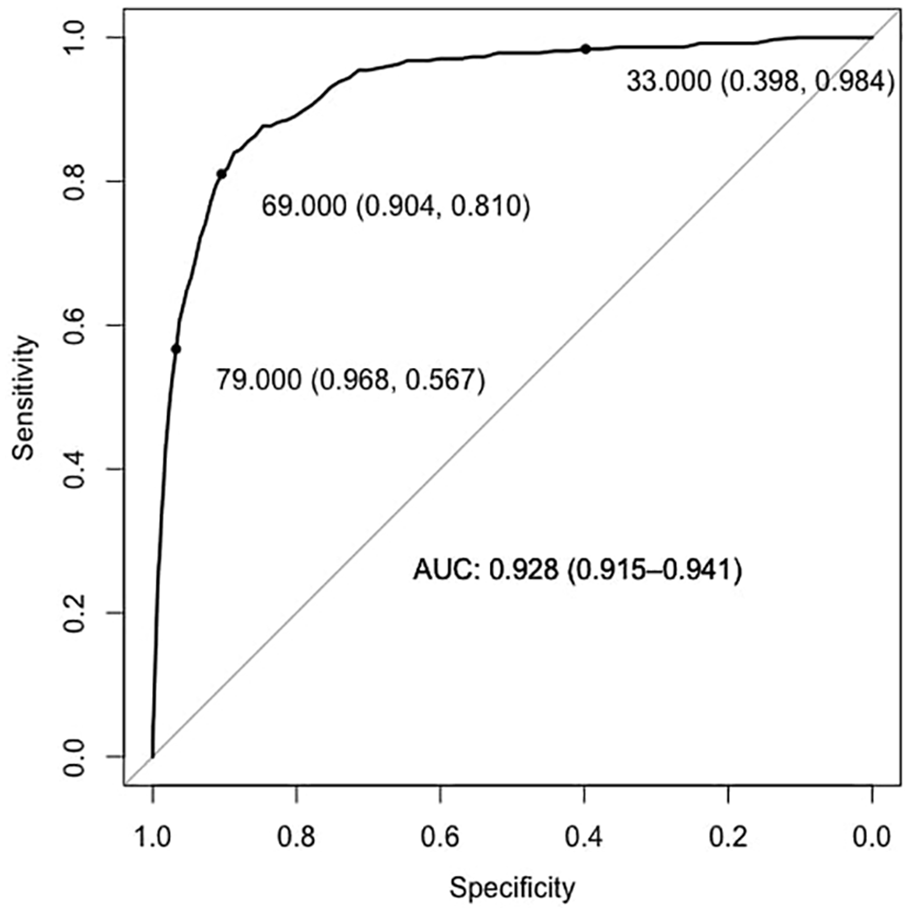
ROC curve for age as a discriminant of 30-day postoperative mortality.
Discussion
During the last decades, laparoscopic appendectomy has become the standard choice of surgical care for patients with appendicitis in Denmark. At the end of the study period, more than 90% of patients with appendicitis had a laparoscopic appendectomy. There is no clinical significant change in delay or timing of surgery as a consequence of the shift from open to laparoscopic surgery. The transition from open to laparoscopic surgery was associated with a reduction in the median postoperative hospital stay from 55 to 16 h and a reduction in the 30-day mortality from 0.91% to 0.40%. Age was an excellent predictor of mortality (AUC: 0.93) and patients aged 69 years of age or above could be regarded as acute high-risk abdominal surgical patients.
The overall incidence of appendicitis remained more or less stable over time. The clear drop in the incidence of complicated appendicitis from 2011 to 2012 could likely be caused by the fact that the ICD-10 codes for appendicitis in the DNPR (Danish National Patient Register) were changed from the ICD-10 version 2008 to the ICD-10 version 2010 the 1 January 2012. In support, the incidence of complicated appendicitis was stable in the period 2000–2011 and 2012–2015. We have no other explanation for the clear and sudden drop in the incidence of complicated appendicitis seen with same magnitude in all decades of life. Most interesting, the incidence of uncomplicated cases dropped with increasing age while the incidence of complicated cases remained constant all through life. We have no good explanation for this finding, but it raises the question of whether there are different aetiologies for complicated and uncomplicated cases.
The reduction in postoperative hospital stay during the transition from open to laparoscopic appendectomy was to be expected as laparoscopic appendectomy has been shown to reduce postoperative stay when compared to open appendectomies. 2 The median postoperative stay during the end of the study period corresponds well with the median postoperative stay reported in clinical trials on adult patients undergoing surgery for appendicitis during the same period in Denmark.17 -19
The reduced mortality was mostly driven by a reduced mortality for complicated cases and for elder patients. The increased use of minimal invasive surgery during the study period seems to have benefited the more fragile patients. This could partly be a consequence of the reduced surgical trauma associated with minimal invasive surgery, and it has been shown that laparoscopic colorectal surgery reduces mortality in the elderly. 20 The improved short-term outcomes after surgery for appendicitis could also be partly caused by a reduced morbidity in the elder population during the study period, and it is unlikely that only the increased use of laparoscopy accounts for the reduced mortality.
In concordance with previous studies, we found that mortality increased significantly with increasing age.3 -5 Age as a prediction model for 30-day postoperative mortality in patients undergoing surgery for appendicitis had an AUC of 0.93, which is superior to most other prediction models validated in heterogeneous surgical populations.21 -23 Patients aged 69 or above had mortality of 5% or above and could be classified as acute high-risk abdominal surgical patients. The fact that age alone is an excellent predictor of 30-day postoperative mortality challenges our current practice defining acute high-risk abdominal surgical patients based on procedure alone rather than on patient characteristics. In future trials and care pathways, defining patients as acute high-risk abdominal surgical should be based on validated prediction models.
We cannot separate improvements in anesthesia and perioperative care from choice of surgery. However, the most apparent change in the treatment of appendicitis during the last decades has been the introduction of laparoscopic surgery and advances have clearly reduced mortality and postoperative hospital stay. During the study period, the removal of a non-inflamed appendix has been reported to be almost constant and should not have biased our results. 14 We have low level of missing data, and the study included an entire nation across a long time period. The incidence of appendicitis and demographics at time of surgery for appendicitis were unchanged and should not bias our results. Furthermore, we have tried to take into account advances in general public health through the 30-day standardized mortality ratio, which also shows a clear decrease in 30-day mortality after surgery for appendicitis during the transition from open to laparoscopic surgery for appendicitis. The improved short-term outcomes after surgery for appendicitis could also be partly caused by a reduced morbidity in the elder population during the study period. The diagnosis of appendicitis in the DNPR has been validated. The distinction between complicated and uncomplicated cases based on ICD-10 codes in the DNPR has not been validated, and this should be taken into account regarding the specific incidence curves for complicated and uncomplicated cases.
The medical care provided by the Danish health care system should be comparable to other high-income countries. Health care is free of charge and hospitals in Denmark are publicly funded and reimbursed based on disease and procedure, while the actual duration of hospital stay and resource utilization does not affect reimbursement. We believe that this makes the results of this study generalizable since there should be no confounding regarding postoperative hospital stay or preferred surgical procedure.
Many previous nationwide population studies on surgery for appendicitis only included patients undergoing open or laparoscopic appendectomy. We included patients based on a diagnosis of appendicitis and any surgery performed to remove the appendix. Hereby we also included patients having more extensive surgery for appendicitis. We believe that this makes our results more generalizable regarding the adult population undergoing surgery for appendicitis.
Laparoscopic surgery for appendicitis can be completed for more than 90% of patients in a nationwide cohort. The transition from an era of open to laparoscopic appendectomy is associated with reduced postoperative hospital stay and reduced mortality. Taken into account the results of randomized clinical trials supporting the use of laparoscopic surgery and the results of this nationwide cohort study, institutions and healthcare providers should aim at completing surgery for appendicitis as laparoscopic surgery for the majority of patients.
Despite overall low mortality after surgery for appendicitis, age is an excellent predictor of short-term mortality. Patients aged above 69 undergoing surgery for appendicitis could be classified as acute high-risk abdominal surgical patients and it may be erroneous to exclude these patients from acute high-risk abdominal surgery pathways aiming to reduce mortality after emergency surgery.
Footnotes
Authors contributions
J.K. contributed in study design, data collection, data analysis and interpretation, drafting of the article, revision and final approval of the article. L.T. contributed in study design, interpretation, revision, and final approval of the article. I.G. contributed in study design, interpretation, revision, and final approval of the article. All authors agree to be accountable for all aspects of the work presented.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Center for Surgical Science, Department of Surgery, Zealand University Hospital. The primary author received a research grant from North Zealand Hospital and financial support from the Department of Surgery, North Zealand Hospital, Copenhagen University Hospital.