
Abstract
Background and objective:
Obesity is prevalent and has a negative impact on women’s health, including sexual dysfunction. Recent review articles suggest improvement in Female Sexual Function Index (FSFI) and proportion of female sexual dysfunction (FSD) among women with obesity after bariatric surgery.
Methods:
We pooled data from 16 observational studies involving 953 women. The study outcomes were mean FSFI scores and proportion of FSD before and after bariatric surgery. We also sub-analyzed whether age and duration of follow-up affected these outcomes.
Results:
The mean age of the subjects was 39.4 ± 4.2 years. Body mass index (BMI) showed significant reduction postoperatively (p < 0.0001). Bariatric surgery led to significant improvement in total FSFI score (p = 0.0005), and all sexual domains except pain. Bariatric surgery reduced the odds of having FSD by 76% compared with those who did not undergo operation (OR 0.24, 95% CI = 0.17, 0.33, p < 0.0001). Our sub-analysis demonstrated a significant reduction in the proportion of FSD for patients <40 years of age. The improvement of total FSFI scores and reduction in proportion of FSD remained significant within the first 12 months after surgery. Univariate meta-regression showed that BMI was not a significant covariate for improvement of FSFI scores (β = 0.395, p = 0.1, 95% CI = 0.884, 0.095).
Conclusions:
Bariatric surgery is shown to improve sexual function scores and prevalence of FSD. This is especially significant among women <40 years of age. This benefit remained significant within the first year after surgery. This appears to be an additional benefit for these patients.
Keywords
Introduction
The World Health Organization (WHO) defines overweight as having body mass index (BMI) of ⩾25 kg/m2, whereas obesity with BMI ⩾ 30 kg/m2. These cutoff values differ for Asians, as they generally have a higher percentage of body fat than Caucasians of the same age, sex, and BMI, with significantly increased cardiovascular risks. Hence, WHO recommends a lower BMI cutoff of 23 kg/m2 as overweight and 25 kg/m2 as obese for Asians. 1
Worldwide, 40% of women are overweight, and 15% are obese. 2 Obesity has a negative impact on the overall health of women as it is associated with multiple comorbidities, such as diabetes mellitus, coronary artery disease, and cancers. 3 In recent years, it has also been identified that obesity is associated with sexual dysfunction. 4 In women who are obese, orgasm was the most affected aspect in sexual function. 5 Despite that, sexual dysfunction is infrequently discussed in obesity, especially those who are morbidly obese. 6 This may constitute a great problem to the affected individual and the partner, 7 as it has a major impact on quality of life and interpersonal relationships. 8
The Sexual Function Health Council of the American Foundation for Urologic Disease classified female sexual dysfunction (FSD) into five main categories: hypoactive sexual desire disorder, sexual aversion disorder, sexual arousal disorder, orgasmic disorder, and sexual pain disorders. 9
Bariatric surgery is an effective therapeutic measure for morbid obesity and related comorbidities.10,11 It is proven to improve medical conditions, especially diabetes mellitus, dyslipidemia, and hypertension. 12 There is mounting evidence that bariatric surgery also improves health-related quality of life, 13 sex hormones, and fertility.14,15 Approximately half of women and men who were not satisfied with their sexual life experienced improvements in this aspect after bariatric surgery even at 5 years of follow-up. 16 Recent review articles suggest improvement in sexual function among women with obesity after bariatric surgery.14,17,18 However, these articles did not provide additional analyses looking at the effect of age and duration after surgery on the outcome. Moreover, the proportion of FSD was not reported. As only a limited number of studies were included in one of the meta-analyses, bariatric surgery did not lead to significant improvement in FSFI among women with obesity. 17
The authors aimed to systematically review the available literature to date and analyze the effect of bariatric surgery in FSD among women with obesity. The primary outcome of this analysis was to compare the mean FSFI score (total and its domains) of women with obesity before and after bariatric surgery. The secondary objective was to analyze the proportion of FSD among this group of patients. As previous studies have shown that FSD was more prevalent among females aged >40 years,19 –21 the authors also sub-analyzed whether age and duration of follow-up would affect these outcomes, using study-level data.
Materials and methods
Data sources and extraction
A systematic search of all English-language medical literature published from inception till December 2019 was performed using PubMed, CINAHL, Cochrane, and OVID with the MESH headings: “female sexual dysfunction” or “female sexual function” and “bariatric surgery,” “metabolic surgery,” “obesity surgery” or “weight loss surgery.” References of the selected papers were also looked into. When papers were not available or information was inadequate, attempts were made to contact the respective authors to obtain the full paper and more detailed data. Inclusion criteria are articles that studied effect of bariatric surgery on female sexual function, via reporting the FSFI scores or the proportion of FSD. They are excluded if comparison data pre- and postoperatively were not available. Case reports, review articles, meta-analyses, and letters to editors were also excluded. The titles and abstracts obtained through the search were screened followed by analysis of the full-text articles by two independent reviewers (H.H.L. and H.S.L.). All duplicates were removed. Data were extracted using a standardized data extraction form. Wherever data were not provided numerically, they would be read off as graphs. Data from eligible studies were extracted by H.H.L. and were reviewed by A.Y. Any discrepancies were resolved by the third reviewer (H.S.L.).
Quality assessment
H.H.L. and A.Y. independently assessed the methodology quality and reporting of the studies using the Newcastle-Ottawa Scoring (NOS) Scale for case–control studies and the adapted scale for cross-sectional studies. Any discrepancies were sorted out by the second reviewer (M.A.S.). The NOS scale was developed to assess the quality of nonrandomized case–control studies for meta-analysis result interpretation. It uses a “star system” which judges the studies in three categories: selection of study group, group comparability, and ascertainment of outcome of interest. The maximum total score is 10.
Female Sexual Function Index
Female Sexual Function Index (FSFI) is a validated, 19-item self-report scale that evaluates sexual function of women within a 4-week window. The FSFI has been shown to have good psychometric properties22,23 and has been used to assess sexual function in women with diverse medical conditions. 24
It has six domains, namely, desire, arousal, lubrication, orgasm, satisfaction, and degree of pain. The maximum score is 6 for each domain, and 36 for the total. A higher total score indicates better sexual function. A total score of <26 defines sexual dysfunction. 25
Statistical analysis
Qualitative
All abstracted information was tabulated. A qualitative meta-analysis was conducted to summarize, compare, and contrast the abstracted data.
Quantitative
All data analyses were performed using Stats Direct (version 2.7.9). The presence of heterogeneity between the trials was tested using the I-squared (I 2 ) statistic. I 2 of >40% indicated significant heterogeneity. If the I 2 was significant, data were pooled using random effects (DerSimonian-Laird); otherwise, fixed effects (Mantel-Haenszel, Rothman Boice) were used. Publication bias was assessed using both Begg–Mazumdar and Egger tests to increase the sensitivity of detecting bias. For dichotomous data (proportion of FSD), pooled odds ratio (OR) with 95% confidence intervals (CI) were estimated based on the random effects model. Continuous outcomes were analyzed with 95% CI using the effect size (weighted mean difference) meta-analysis if the mean and standard deviation of endpoint measures were presented in the original articles. The adverse effects risk was calculated by the proportional rate with 95% CI.
Results
A total of 843 articles (292 from PubMed, 32 from CINAHL, 37 from Cochrane, and 560 from OVID) were identified in the initial search. After screening the titles, abstracts, and full texts, followed by elimination of duplicate publications, 16 articles were included into the systematic review and meta-analysis (Fig. 1).
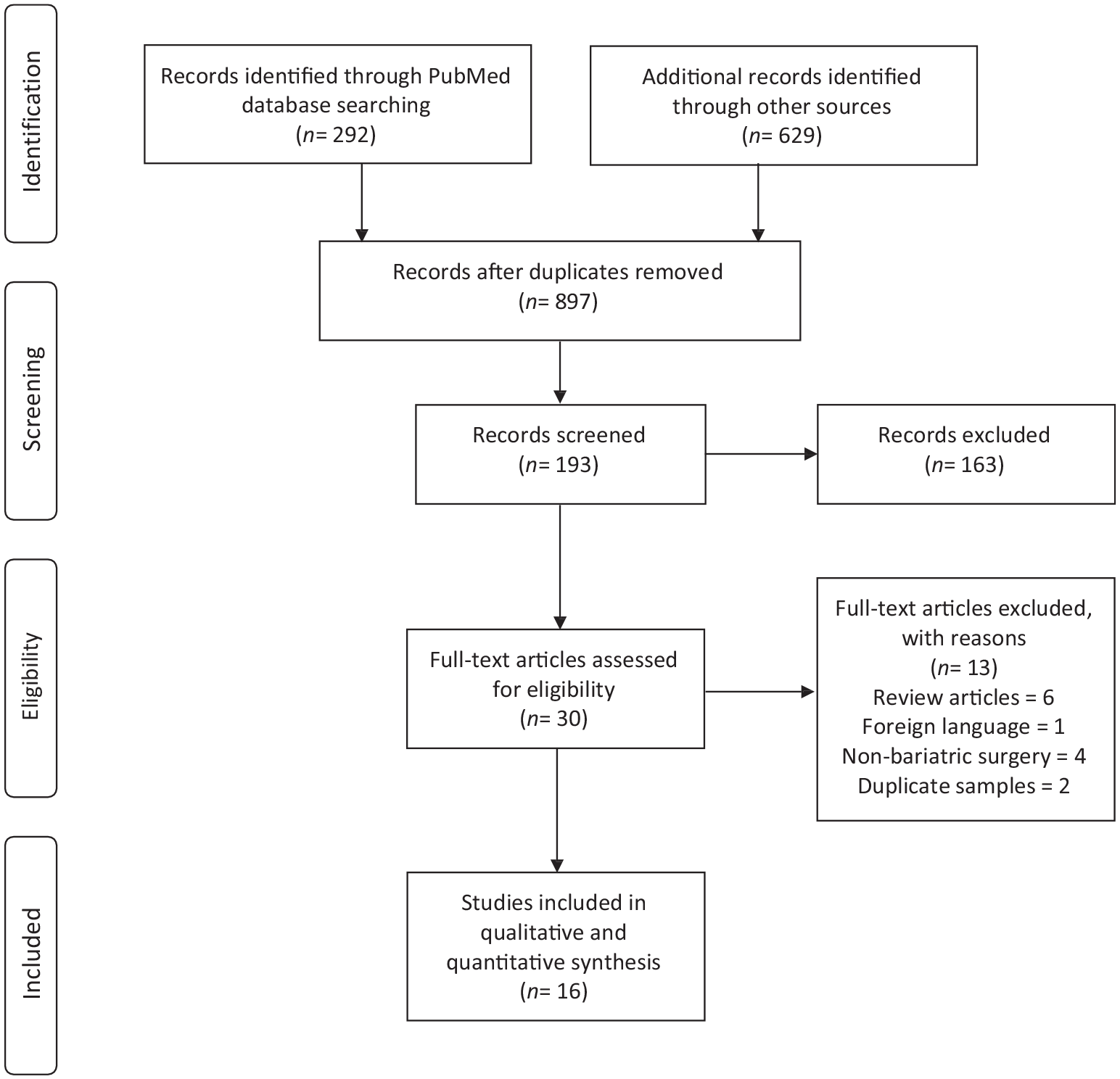
Study flow diagram.
Data synthesis
A total of 953 subjects from 16 articles were included into this study. The baseline characteristics of all studies are described in Tables 1 and 2. The sample size ranged between 28 and 116. There were 15 prospective studies with follow-up duration ranging between 6 and 48 months6,26 –39 and one cross-sectional study. 40 All were cohort studies except for one case–control study, 40 which compared FSD in the preoperative and postoperative group of subjects.
Baseline characteristics of study participants.
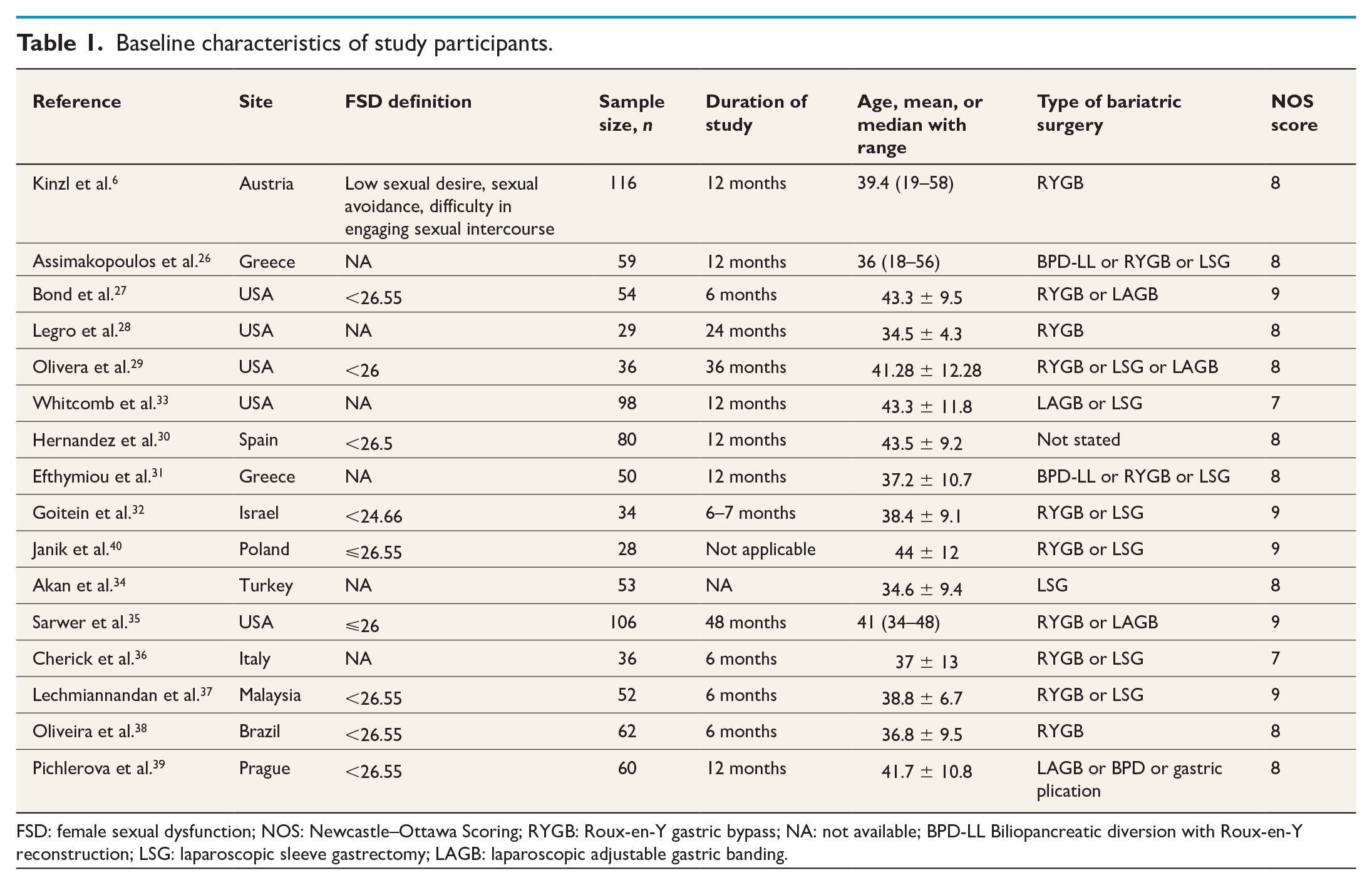
FSD: female sexual dysfunction; NOS: Newcastle–Ottawa Scoring; RYGB: Roux-en-Y gastric bypass; NA: not available; BPD-LL Biliopancreatic diversion with Roux-en-Y reconstruction; LSG: laparoscopic sleeve gastrectomy; LAGB: laparoscopic adjustable gastric banding.
Pre- and postoperative changes in BMI, total FSFI scores and proportion of FSD.
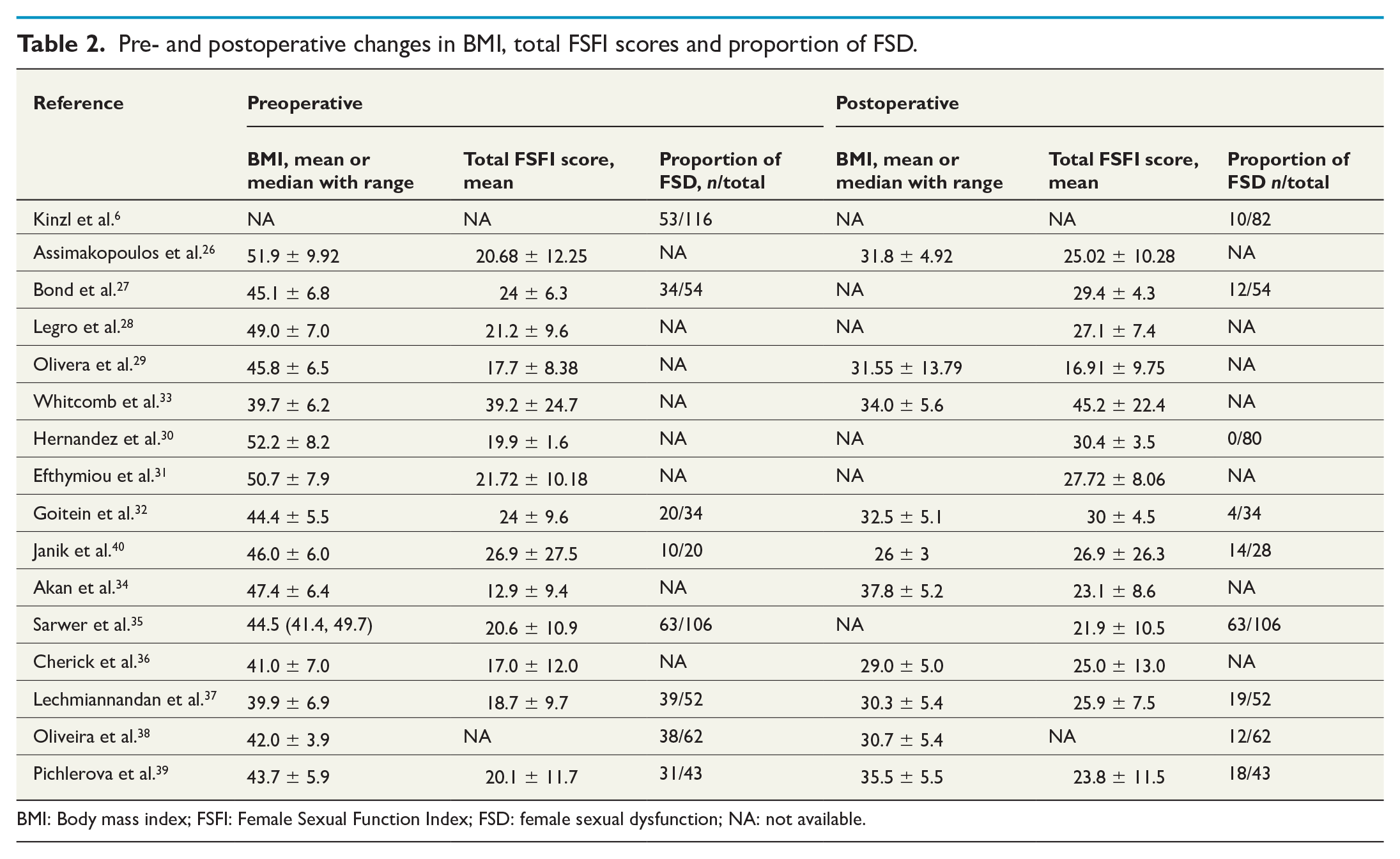
BMI: Body mass index; FSFI: Female Sexual Function Index; FSD: female sexual dysfunction; NA: not available.
The mean age of the subjects was 39.4 ± 3.2 years. There was a significant reduction of preoperative BMI of 45.4 kg/m2 ± 4.0 (range 39.7 kg/m2–50.7 kg/m2) to 31.9 kg/m2 ± 3.0 (range 26.0 kg/m2–37.8kgm 2 ) postoperatively (p < 0.0001). Approximately two-third (63.57%) of the cohort was married.
FSFI scoring
Fourteen studies compared preoperative (range 12.88–39.20 ± 1.60–24.70) and postoperative total FSFI scores (16.91–45.20 ± 3.50–22.40).26 –40 Only two showed nonsignificant change of the scores postoperatively.29,40
Nine studies reported FSFI domain scores.26,29,31,32,34,35,37,39,40 For sexual desire, three studies showed a nonsignificant change in the score postoperatively.29,32,35 Two studies showed no significant difference in sexual arousal and lubrication domains post-surgery.29,35 No significant change was observed in sexual orgasm in four studies.26,29,35,40 Similarly, three studies showed no improvement in sexual satisfaction postoperatively.29,35,40 There was no obvious change in sexual pain after surgery in four studies.29,34,35,40
Proportion of FSD
Eight studies compared the proportion of FSD before and after bariatric surgery.6,27,32,35,37 –40 All but two studies reported a reduction in proportion of FSD after surgery.35,40
Meta-analysis
Bariatric surgery led to significant improvement in all sexual domains, that is, desire (3.14 ± 1.41 vs 3.77 ± 1.29, p < 0.0001) (Supp Figure A), arousal (3.27 ± 1.99 vs 3.94 ± 1.85, p < 0.0001) (Supp Figure B), lubrication (3.53 ± 2.13 vs 4.14 ± 1.74, p = 0.0013) (Supp Figure C), orgasm (3.40 ± 2.14 vs 4.02 ± 1.84, p = 0.0004) (Supp Figure D), satisfaction (3.73 ± 2.06 vs 4.47 ± 1.69, p < 0.0001) (Supp Figure E), but not pain (3.30 ± 2.29 vs 4.04 ± 1.89, p = 0.0544) (Supp Figure F). The total FSFI scores improved postoperatively (21.19 ± 8.59 vs 26.05 ± 7.62, p = 0.0005) (Fig. 2).
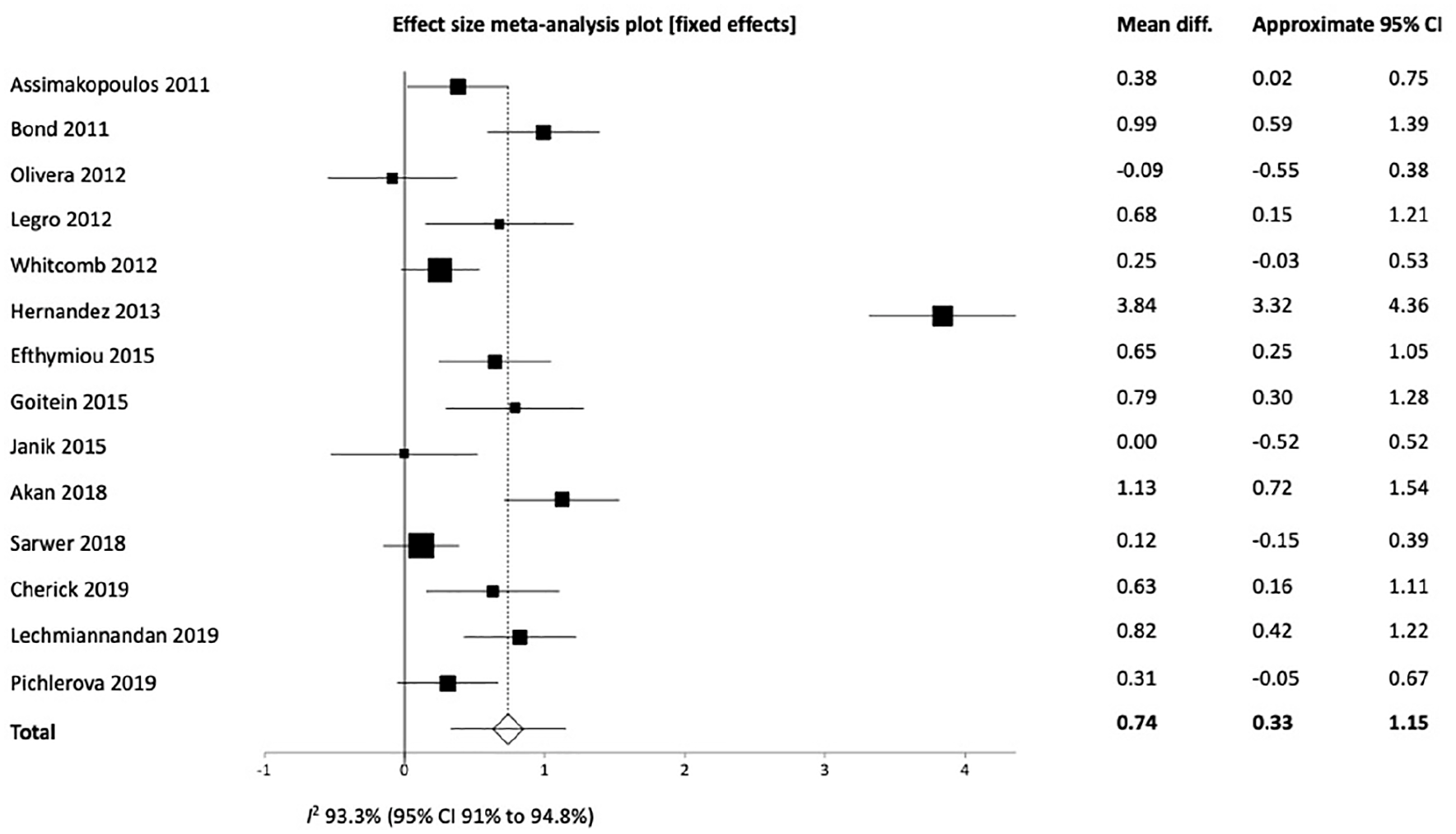
Total female sexual function index score among obese women before and after bariatric surgery.
Using fixed-effects model, bariatric surgery reduced the odds of having FSD by 76% compared with those who did not undergo operation (OR 0.24, 95% CI = 0.17, 0.33, p < 0.0001) (Fig. 3). Univariate meta-regression showed that BMI was not a significant covariate for improvement of FSFI scores (β= 0.395, p = 0.100, 95% CI = 0.884, 0.095).
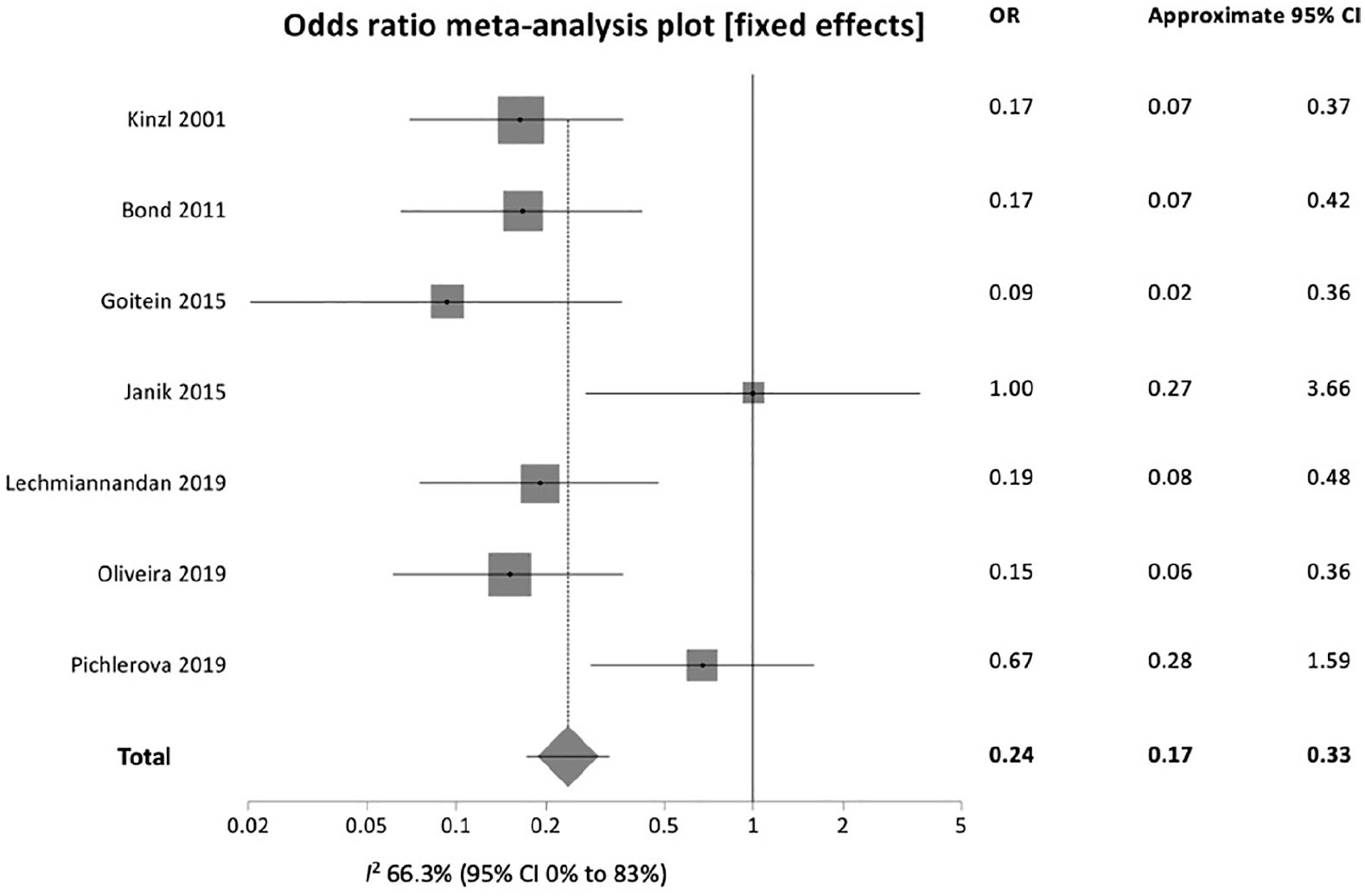
Proportion of female sexual dysfunction among obese women before and after bariatric surgery.
When the total FSFI scores were sub-analyzed, with study-level data, using age as the variable with 40 years as the cutoff, the improvement after bariatric surgery remained significant for patients <40 years of age (n = 375, 19.45 ± 3.65 vs 26.27 ± 2.24, p < 0.001) (Supp Figure G), but not significant for patients aged ⩾40 years (n = 462, 24.06 ± 7.33 vs 27.36 ± 8.39, p = 0.056) (Supp Figure H). The changes seen in the total FSFI scores remained significant during follow-up, within 12 months after surgery (n = 580, 23.04 ± 6.02 vs 28.77 ± 5.86, p = 0.0011) (Supp Figure I). All the FSFI domains improved significantly postoperatively for patients <40 years of age and for those with repeat scores within 12 months after surgery. However, most of the domains did not show significant improvement for patients aged ⩾40 years, except for desire (p = 0.0034).
Similarly, the proportion of FSD reduced significantly after bariatric surgery for patients <40 years of age (n = 264), from 59.7% preoperatively to 19.8% postoperatively, with OR of 0.158 (95% CI = 0.099, 0.247, p < 0.001), translating to a reduction of 15.8% of odds of FSD with surgery (Supp Figure J). However, the improvement was nonsignificant for patients aged ⩾40 years (n = 194, p = 0.993). The change in the proportion of FSD was significant for subjects seen within 12 months postoperatively (n = 406), from 55.5% before surgery to 26.6% after surgery, with OR of 0.264 (95% CI = 0.133, 0.526, p < 0.001) (Supp Figure K).
Discussion
In the present meta-analysis, we have shown that bariatric surgery leads to significant improvement in FSD among women with obesity, concurring with past meta-analyses.17,18 Our findings give credence to the benefits of bariatric surgery in improving FSD, for younger women, and at least for the first year postoperatively. Our results can be generalized to a number of populations as our pooled cohort were from diverse study populations. The results of the present meta-analysis add to two previous meta-analyses, which did not provide additional analyses looking at effect of age and duration after surgery on the outcome.17,18 The findings from this meta-analysis demonstrate a reduction of FSD with bariatric surgery by 76% compared with their counterparts who did not undergo operation. The positive effect of bariatric surgery on female sexual function was especially seen within the first 12 months post-surgery, and for women <40 years of age. Besides, the findings from this research suggest new evidence that the improvement of FSD seen among women with obesity after bariatric surgery could be contributed by reasons beyond weight reduction, as BMI was not found to be associated with improvement of FSFI scores.
Sexual dysfunction has been recognized as an important part of health more recently. Despite gaining popularity among clinicians and researchers, FSD remains hidden from the limelight in comparison with male sexual dysfunction. 18 The sexual function model proposed by Masters, Johnson, and Kaplan has been well-accepted.41,42 The model describes sexual function in four linear stages: desire, arousal, orgasm, and resolution. However, Basson argued that female sexual stages are more circular with sexual response starting with arousal first, followed by desire. 43 In addition to the complexity of female sexual response, FSD among females with obesity is likely multifactorial, contributed by other potential mediating biological, comorbid, and psychological factors. 4
Among the biological factors involved include sex-hormone synthesis, androgen/estrogen ratios, decrease in nitric oxide, and adipose distribution, although the link between these factors and FSD in women with obesity is less clear compared with males. 4 Functionally, hormones that are involved in female sexual function include dihydroepiandrosterones and testosterone, where adequate levels are required for desire and libido, and adequate estrogen for lubrication.44,45 In women with obesity, sex-hormone binding globulin levels are reduced, resulting in compensatory hyperandrogenism. 46 Concentrations of testosterone in moderate amounts improve health parameters and sexual function, but not in low or high concentrations. 47 However, it is uncertain whether obesity has significant effects on estrogen and whether there is any evidence to link it with sexual impairment. 4 Despite reduction of sex hormone levels with bariatric surgery, FSD scores improved. 44
Obesity is also associated with multiple chronic conditions, such as diabetes mellitus and cardiovascular diseases, which may contribute to sexual dysfunction. 4 Furthermore, treatment of these conditions, such as some antihypertensive agents or antidepressants, can negatively impact sexual functioning. 46 Another possible reason is prolapse of pelvic organ secondary to increased intra-abdominal pressure from obesity contributing to pain. 48 Bariatric surgery results in substantial improvement in the comorbidities listed, as well as reduction in medication use, including antidiabetic, antipsychotics, antihypertensives, and lipid lowering agents.49 –52
The psychological components that may interfere with sexual function include anxiety and depression.44,53 Obesity can lead to various negative psychological effects, including low self-esteem, negative body image, and depression, with subsequent impact on sexual desire and functionality.4,44
Considering the discrepancies in hormonal factors before and after procedure, the improvement of FSD scores after bariatric surgery is possibly due to psychological factors linked to body image and weight loss itself. Weight reduction improved body image dissatisfaction, depressive symptoms, and several domains of romantic relationship functioning. 44 Anatomically speaking, even excessive skin hanging after massive weight loss did not obstruct sexual intercourse. 53
The unchanged pain score despite weight loss is possibly contributed by a few factors, including poor vaginal lubrication, vaginal atrophy, and childbirth. 54 In these instances, local factors such as dry vagina, atrophic vaginitis, and local infection should be investigated, before vaginismus can be diagnosed. 55 Moreover, among women with pelvic floor disorders, bariatric surgery did not improve their sexual function.18,56
The reasons as to why those >40 years old did not experience improvement in FSD scores, except for desire domain, remain unanswered. The proportion of menopausal women, being married and sexually active, could have influenced the FSD score. A study performed among Kurdish women demonstrated that those >40 years were more likely to have FSD. Other contributing factors included lower frequency of sexual intercourse, more children, older husbands, and longer marriages (>10 years). 21 All these factors may have a direct correlation with the older age group. Sexual functioning also typically declines with menopause, likely due to decline in estrogen production leading to vaginal atrophy, dryness, and pain during intercourse. 46 These possible correlations may explain why older patients tend to have persistent FSD. Differences in culture and educational background also influence the confidence and willingness to talk about sexuality and hence change how FSFI is scored.19,21
Our analysis showed that the improvement in FSFI and reduction in the proportion of patients with FSD remained significant up to 12 months post-surgery. However, there was inadequate data to suggest benefits beyond a year. As there were only two studies in this meta-analysis which reported proportion of FSD and total FSFI scores beyond 12 months post-surgery, no meaningful conclusion could be drawn. In one of the largest studies available, the authors found improved sexual functioning in more than half of the women who had undergone bariatric surgery at year 1 postoperation, compared with presurgical assessments, with a linear trend of decline from postoperative years 1–5. Although the sexual function assessment differed from the current meta-analysis, more than one-third of women in their research cohort reported improvements in frequency of sexual desire, sexual activity, and physical health limits sexual activity, but not in satisfaction with sexual life, during the follow-up period beyond 1 year after surgery. 16 Weight plateau or weight regain may explain the lack of improvement when assessed after 12 months. Most studies recorded long-term weight regain 2 or 3 years post-surgery.57,58 Women also experienced significant changes in their reproductive hormones, with the exception of estradiol, from postoperative years 2–4. 35 The initial reported improvements in sexual desire, arousal, and satisfaction, as well as romantic relationship quality and satisfaction, were not maintained through year 4 after surgery, when the women regained approximately 10% of the weight they had lost at year 2. In addition to that, we postulate that persistent or unresolved psychological and social factors surrounding these patients years after surgery contribute to this observation.
Finally, our meta-regression analysis demonstrated that BMI was not associated with improvement of FSFI scores. Indeed, unlike improvement of sexual dysfunction seen among men with obesity who undergo nonsurgical weight loss, the results of weight loss using nonsurgical treatment among women with obesity are less robust. 4 Weight loss among these women showed improvement in only a few aspects of FSD.59 –61 Individual studies in this analysis which reported correlation between BMI and FSFI scores demonstrated inconclusive data.26,34,40 Hence, we postulate that the improvement in FSD seen among women with obesity after bariatric surgery could be attributed by other factors, such as alleviation of comorbidities and psychological benefits as described above.
Our study has several limitations. First, there was significant heterogeneity in the outcome analyses, probably contributed by different populations studied, different types of bariatric surgery used, as well as duration of follow-up and reassessment. Second, although the included studies covered a diverse study population, a majority of them were conducted in the West, hence we may need to interpret these findings with caution among other populations of different ethnic backgrounds. As FSD is a very much ethno- and culture-centric subject, scoring may differ between patients of different social backgrounds. A more conservative society may not be open to answering the questionnaire. Some cultures perceive sexual dysfunction as taboo and a matter not openly talked about, which leads to FSD often being underdiagnosed and ignored. 37 Third, we only analyzed studies using FSFI as the sexual function scale. Although a few other scoring systems were available, we could not make meaningful analysis due to the lack of adequate number of studies. Nevertheless, FSFI is a validated questionnaire shown to have good psychometric properties useful in assessing sexual dysfunction among women with diverse medical conditions. Moreover, patient-reported outcome is the most important and unbiased assessment of sexual function. Although FSFI has limitations especially in assessing sexual desire, it is one of the most widely used measures to assess various domains of sexual function.
We attempted to improve our meta-analysis quality by investigating the effect of bariatric surgery on the proportion of women with FSD, as well as the effect of age and duration of follow-up in this aspect. Finally, given the limited access to patient-level data, we were unable to evaluate the effects of some confounders, such as impact of psycho-social issues and sex hormone levels on the prevalence of FSD and FSFI scores. Nevertheless, our study has provided more insights and added on to current evidence that bariatric surgery improves both FSFI components and proportion of FSD. This is especially true for females <40 years of age, within the first year post-surgery.
Conclusion
Sexual health is an important part of health and quality of life, hence should be addressed appropriately among individuals with obesity. The present meta-analysis adds on to current evidence that bariatric surgery improves FSFI scores as well as prevalence of FSD among women with obesity, especially for those <40 years of age, at least for the first 12 months post-surgery. More high-quality studies are needed to verify the benefits of sexual function improvement beyond 12 months after bariatric surgery, and to verify our conclusion that BMI is not associated with the improvement of FSD.
Supplemental Material
sj-jpg-1-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-1-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-10-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-10-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-11-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-11-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-2-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-2-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-3-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-3-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-4-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-4-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-5-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-5-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-6-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-6-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-7-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-7-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-8-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-8-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-9-sjs-10.1177_14574969211072395 – Supplemental material for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis
Supplemental material, sj-jpg-9-sjs-10.1177_14574969211072395 for Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis by Huai H. Loh, Mohammad A. Shahar, Huai S. Loh and Anne Yee in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Dr Goh Siew Li for the additional statistical analysis.
Authors’ contributions
H.H.L. and A.Y. conceived and designed the work; H.H.L. and H.S.L. acquired data for the work; A.Y. analyzed and interpreted the data; H.H.L. and M.A.S. drafted the work and revised it critically for important intellectual content. All authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.