
Abstract
Bariatric surgery has long been the most effective intervention for obesity, providing significant and durable weight loss, with procedures like sleeve gastrectomy and gastric bypass achieving 10-year total weight loss (TWL) rates of 23.4% and 26.9%, respectively. More complex procedures, such as duodenal switch, result in even greater TWL. Recently, glucagon-like peptide-1 receptor agonists (GLP-1 RA) have emerged as a promising pharmacological alternative, demonstrating up to 25.3% TWL with tirzepatide. However, GLP-1 RA efficacy remains inferior to bariatric surgery, with high discontinuation rates due to adverse effects, cost, and limited insurance coverage. While surgery offers superior long-term outcomes and cost-effectiveness, it is underutilized, with less than 1% of eligible patients undergoing surgical intervention annually. GLP-1 RA can expand access to obesity treatment, particularly for patients hesitant or ineligible for surgery, and may serve as a bridge to surgery or an adjunct for postoperative weight regain. Despite their benefits, GLP-1 RAs require sustained adherence, and weight regain is common upon discontinuation. A multidisciplinary approach integrating surgical, pharmacological, and lifestyle interventions is essential for optimizing obesity management. Future research should focus on long-term GLP-1 RA efficacy, combination therapy strategies, and improving access to both surgical and medical obesity treatments.
Key Takeaway
Bariatric surgery continues to provide the highest durable weight loss for obese patients. GLP-1 RA can expand access to obesity treatment, particularly for patients hesitant or ineligible for surgery, and may serve as a bridge to surgery or an adjunct for post-operative weight regain.
Introduction
The prevalence of obesity worldwide has doubled in the last 30 years, and in the United States (US) as of 2020. The CDC reports that approximately 41.9% of adults in US have obesity, equating to more than 100 million people.1,2 Obesity is associated with the development of many other chronic health conditions like diabetes mellitus (DM), cardiovascular disease (CVD), hypertension (HTN), obstructive sleep apnea, and certain cancers.1,3 Obesity and obesity related diseases pose a significant health burden, and treatment can be challenging.1,2 Bariatric surgery has been established as a highly effective tool for treating obesity, and compared to medical weight loss alone, surgery can lead to meaningful long-term weight loss and greater resolution of some obesity related comorbidities.4,5 However, medical weight loss strategies were generally limited to diet and exercise programs with medication adjuncts to treat comorbidities. 6 The emergence of glucagon-like peptide-1 receptor agonists (GLP-1 RA) has introduced a promising pharmacological option for significant weight loss, leading some to consider them a viable alternative to surgery. 7 This shift towards medical management of obesity offers quicker access to care and has the potential to expand the reach of obesity treatment on a public health magnitude. While GLP-1 RA demonstrate encouraging results, their weight loss efficacy still does not match that of bariatric surgery, even under the controlled conditions of randomized clinical trials. This manuscript reviews the reported outcomes, benefits, side effects, cost-effectiveness, and limitations of bariatric surgery and GLP-1 RAs in obesity management.
Advantages of Bariatric Surgery in the Treatment of Obesity
Efficacy and Durability
Surgery Versus GLP-1 Agonists on Total Weight Loss.
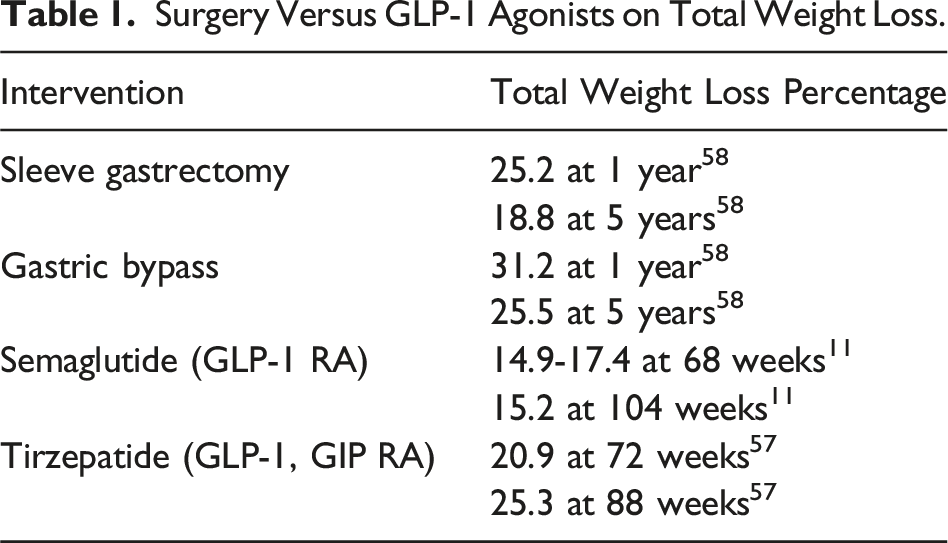
Several studies have also evaluated effects of bariatric surgery and GLP-1 RAs on reducing other obesity-related conditions such as DM, CVD, HTN, kidney disease, and stroke. Diabetes remission rates for GLP-1 RAs are comparable to results of a sleeve gastrectomy, though are variable (32.5-92%) depending on the specific GLP-1 RA being studied. 14 Treatment with semaglutide resulted in a 20% reduction in nonfatal MI, nonfatal stroke, and cardiovascular related death. 15 A large retrospective cohort study by Dicker et al 16 compared patients who had undergone bariatric surgery to those treated with a GLP-1 RA and found no statistically significant difference in all-cause mortality or major adverse cardiac events for patients with obesity and a diagnosis of diabetes for greater than 10 years. 16
These medications are very effective but limited due to patient compliance and side effects. Although symptoms are usually transient and mild to moderate in severity, common adverse effects of semaglutide and tirzepatide include nausea (35% and 46%), diarrhea (21% and 23.5%), constipation (20% and 22%), and vomiting (16% and 15.5%), with 81-84% of patients reporting adverse events overall.12,17-19 The high adverse event rates experienced by patients on GLP-1 RAs may affect patient compliance and explain the elevated discontinuation rates of up to 50% at 1 year. 18 Patients are at a greater risk of experiencing adverse events with higher doses or during periods of dose escalation. There is some suggestion that adverse events are occurring less frequently with newer generation GLP-1 RAs; nonetheless, severe complications such as pancreatitis, cholecystitis, and medullary thyroid cancer (observed in mice) have also been reported but lack strong clinical correlation in large trials.12,14,15,20 Despite their effectiveness, the long-term success of GLP-1 RAs is often limited by tolerability concerns, dose-dependent adverse effects, and the potential for rare but serious complications, highlighting the need for careful patient selection, monitoring, and continued research into improving their safety and adherence.
Compliance and Limitations of Medications
Adherence to GLP-1 receptor agonists is critical for sustained weight loss but is often challenging due to side effects, high costs, manufacturer availability, and limited insurance coverage. The discontinuation rates for GLP-1 RAs are high, with real-world studies showing that less than 50% of patients remain on these medications at one year, leading to weight regain. 18 The STEP and SURMOUNT-4 trials demonstrated that upon discontinuation, patients regained approximately two-thirds of their lost weight, with cardiometabolic benefits disappearing.17,20,21 Whether due to an unaffordable cost or due to side effects, discontinuation typically leads to weight regain. While still not fully understood, we know that weight regain after GLP-1 RA cessation is in part due to a surge of ghrelin, which stimulates the patient’s appetite and contributes to weight regain. Weight regain also occurs even in patients who continue lifestyle interventions like dietary changes and regular exercise. 3 Interestingly, patients being treated for obesity alone had higher rates of medication discontinuation compared to patients with obesity and DM (50.3% compared to 43.2%). 22 Rather than discontinuation due to adverse side effects, this may be due to limited insurance coverage of GLP-1 RAs for obesity during the study period, therefore incurring a higher out of pocket cost to the patient, and increased likelihood of discontinuation. 22
Cost-Effectiveness
Bariatric surgery offers superior cost-effectiveness over time compared to GLP-1 RAs. Studies by Docimo et al highlight that the cost of GLP-1 RAs (eg, Wegovy or Mounjaro) exceeds the cost of sleeve gastrectomy or gastric bypass within 8.3-14.72 months, depending on the medication and procedure. 23 Compared to traditional medical management of obesity, surgery is still more cost effective at five years post operatively, and cost-effectiveness continues to improve over a longer time period. 24 The weekly cost of semaglutide and tirzepatide can exceed $1,000, making these medications inaccessible for many patients. In contrast to weight loss medications, bariatric surgery does not rely on continuous compliance for effectiveness and provides more durable results with fewer long-term relapses. A cost-effectiveness analysis by Cunningham et al determined that patients treated with bariatric surgery have fewer long-term expenditures compared to currently available medical therapy options. 25 The Institute for Clinical and Economic Review’s 2022 report concluded that the cost of semaglutide or liraglutide exceeds commonly accepted thresholds for cost-effectiveness, requiring a price reduction of 44-57% to achieve value benchmarks. 26
Advantages of GLP-1 RAs in the Treatment of Obesity
Expanding Access to Care
Currently in the US, less than 1% of eligible patients undergo bariatric surgery annually for the treatment of obesity. 27 There are many reasons contributing to this, but one of the major barriers to undergoing bariatric surgery is related to concerns from both patients and primary care physicians (PCP) regarding complications from surgery. 28 This in turn affects PCP referral patterns. 29 Focus groups conducted with PCPs in Wisconsin demonstrated that decision making often over-emphasizes risk of bariatric surgery, while under-prioritizing treatment for obesity. 30 This negative perception of bariatric surgery is also shared by patients. Multiple studies interviewing patients suffering from obesity highlighted that patients had concerns over the legitimacy of bariatric surgery for the treatment of obesity or viewed surgery as a last resort.31,32
The fear of bariatric surgery is largely unfounded, as its safety is well-established, yet it still limits access to obesity care. 33 The hope is that GLP-1 RAs will help expand access to care as these medications are perceived as safe and have been prescribed for many years by PCPs for the management of diabetes. A recent study demonstrated that unlike bariatric surgery, the perceived side effects of these medications by PCPs was actually lower than those reported in clinical trials. 34 PCPs are also more familiar with these medications. A survey of over 750 health care professionals showed that 65% of providers were very or extremely familiar with GLP-1 RA. 35 Until we can dispel the current stigma regarding bariatric surgery, GLP-1 RAs provides an easier avenue for access to obesity care.
GLP-1 RA may also improve access to effective obesity treatment for patients who are not surgical candidates. A cohort study published by Ilanga, et al evaluated patients with a BMI >50 who were deemed too high risk to undergo bariatric surgery, and individuals treated with GLP-1 RAs were able to lower their BMI by an average of 5.5 points, therefore successfully bridging them to bariatric surgery. 36 For patients with obesity who are in need of other elective surgeries like hernia repair or orthopedic surgery, utilizing GLP-1 RAs for weight loss and comorbidity management can be a successful alternative to bariatric surgery.37,38 Patients with obesity in need of elective hernia repair who were treated with GLP-1 RAs preoperatively had an average BMI reduction by 6 points, and had a shorter time to surgery compared to controls. 37
Shorter Time to Treatment
Another hypothesis for the low prevalence of bariatric surgery for the treatment of obesity is due to surgical resource limitations and restricted access to surgery based on insurance qualifications or insurance payer type.39-41 Alvarez et al found that patients with Medicaid insurance were significantly more likely to have long wait times to surgery compared to those with private insurance (OR 3.02). 41 Other studies have also identified public insurance to be associated with long-wait times. 39 These delays are a huge deterrent to receiving care, and up to 49.1% of patients cited long wait times as the primary reason they did not follow through with bariatric surgery after surgical consultation. 42 In the US, several studies have evaluated regional wait times. Alvarez et al utilized a state-wide database in Michigan and identified median wait times ranging from <67 days (lowest quartile) to >204 days (highest quartile). 41 Similar variability in time from initial consultation to surgery was seen in published data from Stanford (mean 150 days, range 7-1813 days), and the University of Chicago (mean wait time 11.2 months, range 3-38 months).39,43
In some of those studies, wait times were also found to be increasing over the study period, despite data demonstrating that there is no health benefit to this delay to surgical treatment and no difference or improvement in surgical outcomes.40,41,43,44 For these reasons, GLP-1 RAs offer an opportunity to improve timely access to obesity treatment, and patients could potentially start treatment after their first contact with the health care system. Over the last four years the US has seen a 2-fold increase in use of GLP-1 RAs for treatment of obesity, rather than a primary treatment for DM. 45 FDA approvals in 2024 mirrored this trend, and approved indications for use of GLP-1 RAs to include treating obesity alone (BMI >30), being overweight (BMI >27) with one weight-related comorbidity, and even for obese patients with obstructive sleep apnea. 46 With increasing access to and availability of GLP-1 RAs it is not surprising that from 2022 to 2023 privately insured patients experienced a two times increased use of GLP-1 RAs for the treatment of obesity, and a 25.6% decrease in patients undergoing bariatric surgery during that same time period. 7
Easier Lifestyle Adjustment
Although surgery has proven health benefits and overall success rates for weight loss, many patients will still experience issues with weight regain in the long-term, or experience symptoms related to complications from surgery.4,5 Recent studies indicate that roughly one-third of patients (35.4%) had experienced weight regain of >25% from their nadir weight at four years postoperatively. 47 At five years post operatively, 36% of patients who were initially satisfied after surgery were later unsatisfied with their results. Dissatisfied patients were individuals who experienced higher percent weight regain, had a lower percent total weight loss, and those who had discomfort from somatic symptoms at 5 years. 48
Complications from bariatric surgery are relatively rare and rates have been declining, but surgically altered anatomy puts the patient at risk for long-term complications like dumping syndrome, marginal ulcers, or nutritional deficiencies for the remainder of their lives.49-51 While most of these complications are managed with dietary or lifestyle changes, this requires patients to adhere to permanent lifestyle adjustments, which may be difficult to sustain over time.52,53 The psychosocial consequences of lifestyle changes after bariatric surgery may also play a role in patients’ ability to adhere to permanent lifestyle changes, including challenges with eating in social settings and patient reported feelings of isolation related to these limitations. 54
Although adverse events can also occur from GLP-1 RA use, most commonly these are reported as gastrointestinal in nature and include nausea, vomiting, and diarrhea or constipation. Multiple studies have documented that the vast majority of side effects are non-serious, mild to moderate in severity, and transient.12,19 Notably, in clinical trial data the most common consequence of experiencing adverse events are interruptions in doses (12%) or cessation of the medication (1.6-6%), and very few patients experience permanent or long-term effects from GLP-1 RAs use.12,19 Gorgojo et al published recommendations from a multidisciplinary expert panel on how to mitigate the intensity of adverse events from GLP-1 RAs, including improving patient education and slower dose adjustments. Overall, they concluded that in select patients GLP-1 RAs are considered easy to manage and have a good tolerability profile. 19 Patients are also generally satisfied with the ease of use of GLP-1 RAs available in pen injection devices, and more likely to adhere to medication use with weekly injections. 55
Conclusion
While bariatric surgery demonstrates superior efficacy and durability, obesity is a complex, chronic disease that requires a multifaceted approach. Ultimately, more studies are needed comparing GLP-1 RA use to surgery for the treatment of obesity. Combining surgical, pharmacological, and lifestyle interventions is essential for comprehensive care, analogous to the total comprehensive care seen in cancer treatment protocols. Current data suggests that GLP-1 RAs can serve as adjunctive treatments by improving preoperative weight loss (akin to neoadjuvant therapy) to prehabilitate patients with BMI >50. This not only enhances their surgical candidacy with a greater reduction in BMI pre-operatively, but also decreases their perioperative risk. 36 Additionally, GLP-1 RAs may play a role in treating post-surgical weight regain (adjuvant therapy), with promising results in weight loss maintenance. In patients who experienced weight regain after bariatric surgery and were treated with either liraglutide or semaglutide, the median patient lost 67.4% of the weight regained after the last bariatric procedure. 56
For those patients who do not wish to undergo surgery, new research is indicating that GLP-1 RAs may be a safe and less invasive option for weight loss and resolution of obesity-related comorbidities. However, while GLP-1 RAs offers a less invasive alternative for those unwilling or unable to undergo surgery, bariatric surgery still outperforms GLP-1 RAs in long-term weight loss, durability, and cost-effectiveness. Surgery does carry risks, but these are generally rare and manageable, and the benefits of sustained weight loss often outweigh the potential complications. Conversely, GLP-1 RAs face challenges related to compliance, cost, and long-term efficacy. Moving forward, a multidisciplinary team (including, but not limited to primary care providers, endocrinologists, gastroenterologists, psychologists, and surgeons) that integrates both surgical and pharmacological interventions may optimize obesity management. Advocacy for improved access, reduced costs, and comprehensive follow-up to both surgical procedures and pharmacological treatments is crucial to leveraging all available tools in the fight against obesity.
Footnotes
Author Contributions
All authors participated in manuscript writing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.