
Abstract
Background and objective:
Deep sternal wound infection is a feared complication of open-heart surgery. Negative pressure wound therapy has gained an important role in the treatment of deep sternal wound infection. Incisional negative pressure wound therapy has been introduced as a method to prevent wound complications after sternotomy, and lately, after flap reconstructions in the treatment of deep sternal wound infection. We aimed to study if incisional negative pressure wound therapy with PICO™ had similar beneficial effect described earlier with competing commercial devices.
Methods:
This study included 82 patients treated with pectoralis major muscle flap for deep sternal wound infection during the years 2006–2020. PICO group consisted of 24 patients treated with preoperative negative pressure wound therapy and postoperative incisional negative pressure wound therapy (PICO™). Two control groups included 48 patients with conventional treatment and 10 patients with preoperative negative pressure wound therapy only.
Results:
In the PICO group, the complication rate declined from 50.0% to 33.30%, major complication rate from 29.2% to 12.5%, and need for an additional flap from 14.6.% to 4.2% when compared to conventional treatment. The length of hospital stay decreased as well. Preoperative negative pressure wound therapy alone was associated with moderate decline in the complication rates. In addition, we described the use of split pectoralis major muscle flap reconstruction in 57 patients. To our knowledge, this is the largest published patient series describing this method in the treatment of deep sternal wound infection.
Conclusions:
Incisional negative pressure wound therapy with PICO™ seems beneficial after flap reconstruction. Split pectoralis major muscle flap is a versatile reconstruction option suitable to be used as a workhorse in the treatment of deep sternal wound infection.
Introduction
Deep sternal wound infection (DSWI) is a rare but devastating complication of open-heart surgery. The incidence has varied between different publications but has been estimated at approximately 1% in the recent reports.1–3 DSWI has been associated with increased mortality, prolonged hospitalization, morbidity, numerous re-operations, complications, and high costs.2,4
The treatment comprises of a well-performed debridement of devitalized tissue, removal of sternal wires, and administration of culture-specific antibiotics. The closure of the wound can be achieved in several ways using negative pressure wound therapy (NPWT), re-fixation of the sternum, and reconstruction with a variety of flap options. 5 A number of flap options, including muscle, musculocutaneous, and fasciocutaneous flaps as well as omentum, have been proposed.5,6 However, in many centers, pectoralis major muscle flap has remained as a workhorse, because of the proximity to the wound, a constant vascular supply, and straight-forward operation technique without any additional skin incisions.7,8 All of the flap options, including the pectoralis major muscle flap, have been associated with a relatively large number of complications augmented by the multimorbidity of this patient group.7–10 There has been a wide variation in reporting of the complications; nonetheless, the total complication rate in various flap reconstructions has been described around 40%. 3
Split pectoralis major muscle flap has been previously described but has remained less common reconstructive option when compared to the standard turnover or advancement techniques.9,11,12 The split technique has been used to attain better reach for the most caudal part of the sternum. The complication rates of the split pectoralis major muscle flap have not been directly compared to other types of flaps.
NPWT has rapidly gained popularity in the treatment of DSWI either as a single treatment modality or as a bridge to reconstruction. Its disputed benefits include declined mortality rate and shorter hospital stay,13,14 for example, although some recent studies have reported the opposite findings when comparing NPWT to early reconstruction.15,16 In addition, incisional negative pressure wound therapy (iNPWT) has been used to prevent infections after open-heart surgery with mostly promising results.17–20 Recently, there have been a few reports of using iNPWT after pectoralis major muscle flap reconstruction in the treatment of DSWI to prevent flap-related surgical complications.10,21,22 Most of the studies concerning the use of NPWT and iNPWT have been relatively small retrospective studies with heterogeneity, possibility for publication bias, and the matter of manufacturer involvement to discuss.23,24
There are two leading commercially available NPWT systems for incisional wounds. Prevena™ (KCI, San Antonio, TX, USA) is a foam-based system with a canister and a continues pressure of −125 mm Hg. PICO™ (Smith & Nephew Ltd, Hull, UK) is a canister-free device with the pressure of −80 mm Hg. Prior studies have reported promising preliminary results using iNPWT after sternal flap reconstruction. In a study with 30 patients in the intervention group treated with Prevena™, the complication rate declined from 37.5% to 13.0%, and the major complication rate from 15.0% to 3.0%. 22 In a study with 19 patients treated with Prevena™, the rate of major complications declined from 32.1% to 5.3%. 10 A small study with 10 patients using Vivano System™ presented a decrease in the hospitalization length. 21 The superiority of one iNPWT system over another has not been defined. There is a meta-analysis that aimed to compare the two most used systems and favored Prevena™, but the study had significant clinical heterogeneity and was sponsored by the manufacturer of the Prevena™. 25
In this study, we had two separate goals. Our first aim was to investigate if using PICO™ after pectoralis major muscle flap reconstruction would lead to similar decline in the complication rates that has earlier been described with competing iNPWT devices. Our second aim was to report our experience with split pectoralis muscle flap reconstruction as a workhorse in the sternal reconstructions after DSWI.
Materials and methods
Patients treated with pectoralis major muscle flap reconstruction were identified from the operating room records and information was manually collected from the patient records. Retrospective analysis was conducted. Institutional review board approval was not required for this non-interventional study according to national laws.
Between the years 2012 and 2020, there were 87 patients treated for DSWI with pectoralis major muscle flap in a single university hospital. To form comparable study groups, we excluded two patients because instant skin grafts were used in combination with the muscle flap. In addition, three patients with pectoralis major muscle flap and iNPWT with Prevena™ were excluded. Subsequently, all remaining 82 patients with the pectoralis major muscle flap were included and divided into three groups as follows: PICO group consisted of 24 patients treated with preoperative NPWT, pectoralis major muscle flap reconstruction, and postoperative iNPWT between the years 2012 and 2020; control group 1 consisted of 48 patients treated between 2006 and 2012 with pectoralis major muscle flap without any forms of NPWT; and control group 2 consisted of 10 patients treated between 2012 and 2017 with preoperative NPWT and pectoralis major muscle flap (Fig. 1).
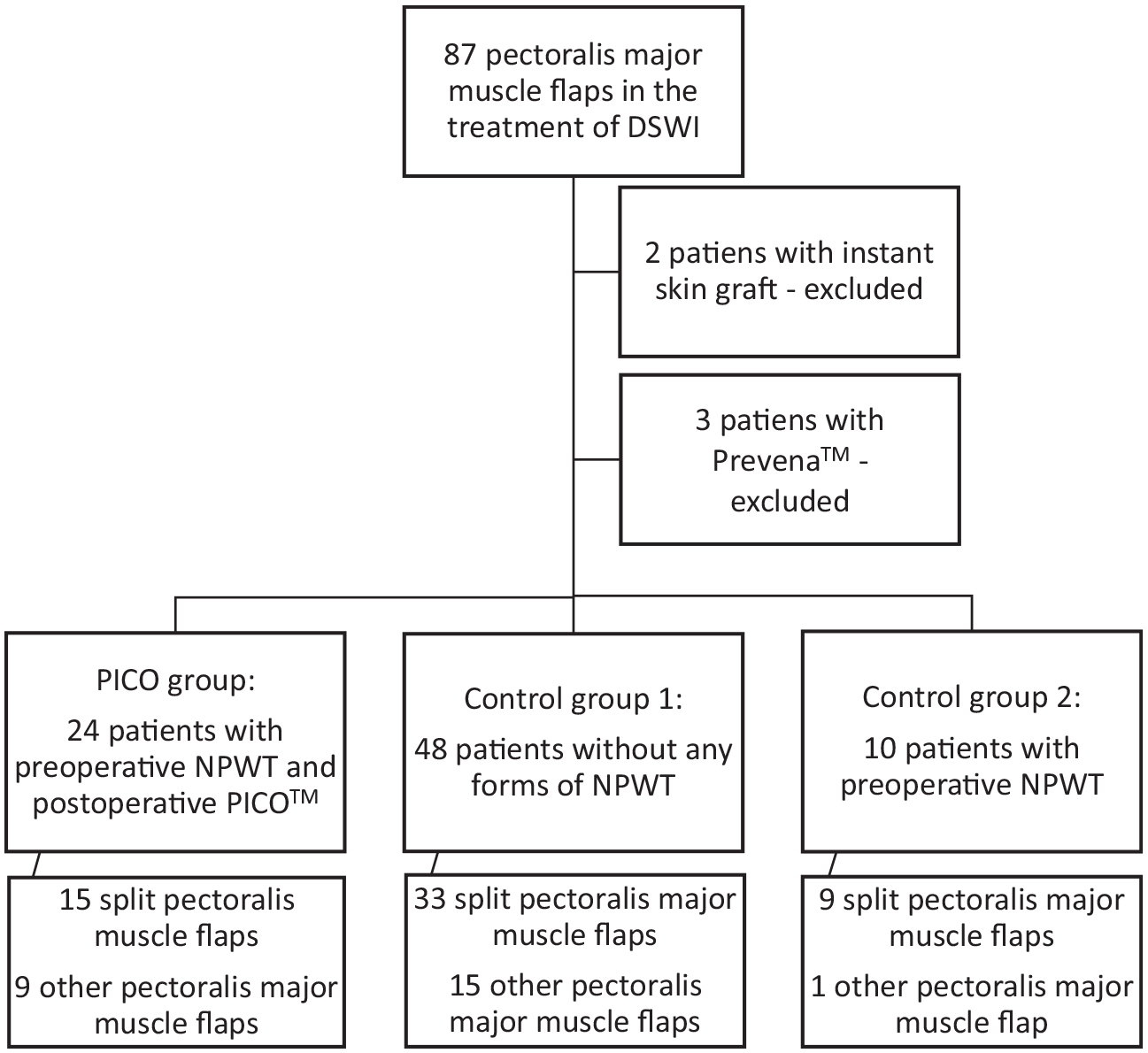
The study design.
Preoperative NPWT was not standardized, and multiple different commercial devices designed for open wounds were utilized. The length of preoperative NPWT varied from 3 to 174 days. Dressings were changed predominantly twice a week.
In the PICO group, single-use battery-powered iNPWT system (PICO™) was placed over closed wound in the operating room under sterile conditions. iNPWT was recommended to continue 7 days with a possible dressing change after 3 days. Multiple different sizes of PICO™ dressings were used, including 10 cm × 30 cm, 10 cm × 40 cm, and 25 cm × 25 cm, according to individual requirements.
The reconstructions with the split pectoralis major muscle flap or other modifications of the pectoralis major muscle flap were carried out by several senior cardiothoracic and plastic surgeons. The split pectoralis major muscle flap was raised by splitting of the muscle into two or three parts based on the internal mammary artery perforators and handled as independent turnover flaps (Fig. 2). The technique has been described in more detail by Li et al. 11 in 2004.
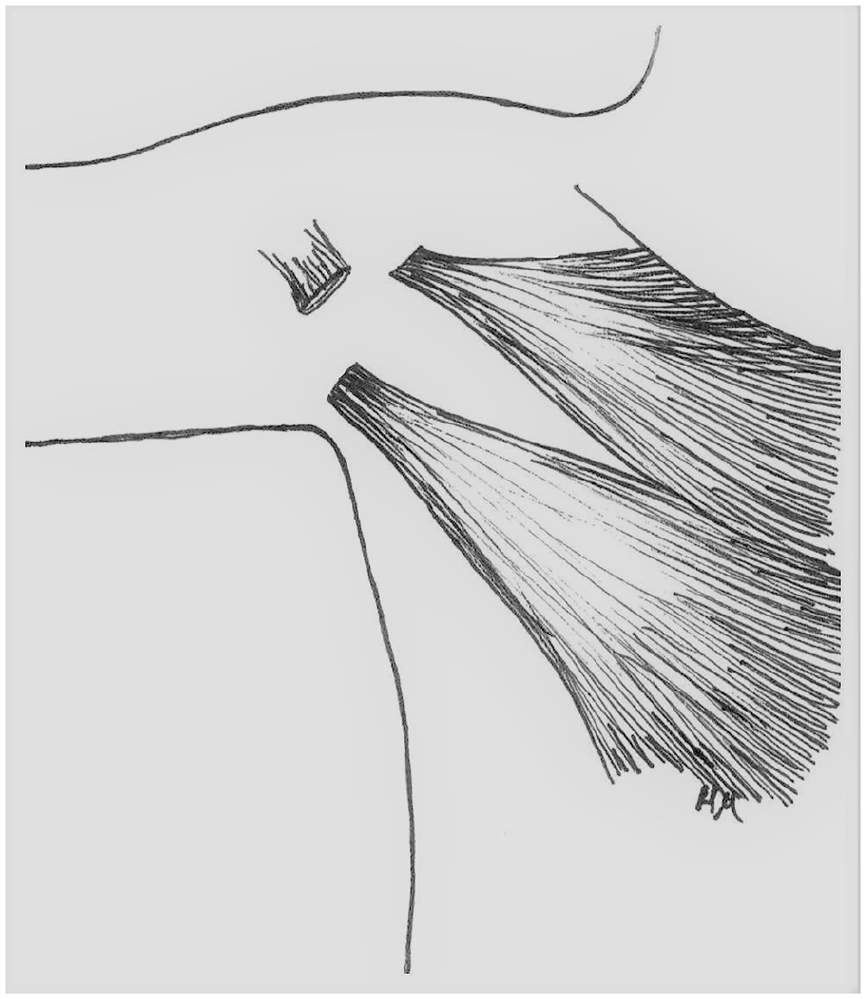
Schematic drawing of splitting of the muscle.
The outcomes were measured by the complications requiring treatment in the university hospital. Complications requiring operative treatment were defined as major. Complications requiring active local wound care, antibiotics, prolonged hospitalization, and/or additional visits to the hospital were defined as minor. Follow-up time ranged from 14 years to 3 months.
We included only patients with prior DSWI, which was diagnosed based on the guidelines by the Centers for Disease Control and Prevention in the United States. The diagnosis of DSWI required at least one of the following:
An organism isolated from culture of mediastinal tissue or fluids.
Evidence of mediastinitis seen during the operation.
One of the following conditions: chest pain, sternal instability, or fever (>38 °C), in combination with either purulent discharge from the mediastinum or an organism isolated from the blood culture.
The statistical analyses were performed using IBM SPSS statistics 27.0 software for Windows (SPSS Inc., Chicago, IL, USA). Intention to treat analysis was conducted. Categorial variables were reported as frequencies and percentages. Continuous variables were reported as mean values and standard deviations. The Mann–Whitney U test was used as a non-parametric test to compare two unpaired groups. To compare categorial variables, Fisher’s exact test was used when there were <5 expected values in any of the cells of a contingency table. In other cases, the Pearson chi-square test was used.
Results
There were 87 patients treated with the pectoralis major muscle flap for DSWI in the Kuopio University Hospital between the years 2006 and 2020. Most of the patients (65.5%) were treated with the split pectoralis major muscle flap. This was the most common reconstructive option in all of the study groups, constituting 62.5% of the flaps in the PICO group, 68.8% of the flaps in the control group 1, and 90.0% of the flaps in the control group 2. However, other modifications—including monolateral and bilateral advancement flaps, monolateral and bilateral turnover flaps without splitting, split pectoralis major muscle flap with internal mammary artery perforator flap, turnover flap with skin graft, and turnover flap combined with contralateral advancement flap—were used when needed. Different techniques and their complications are listed in Table 1 to demonstrate the wide range of reconstructive options. In our material, the split pectoralis major muscle flap was associated with less complications compared to other forms of the pectoralis muscle flap reconstruction.
Pectoralis major muscle flap, various forms.
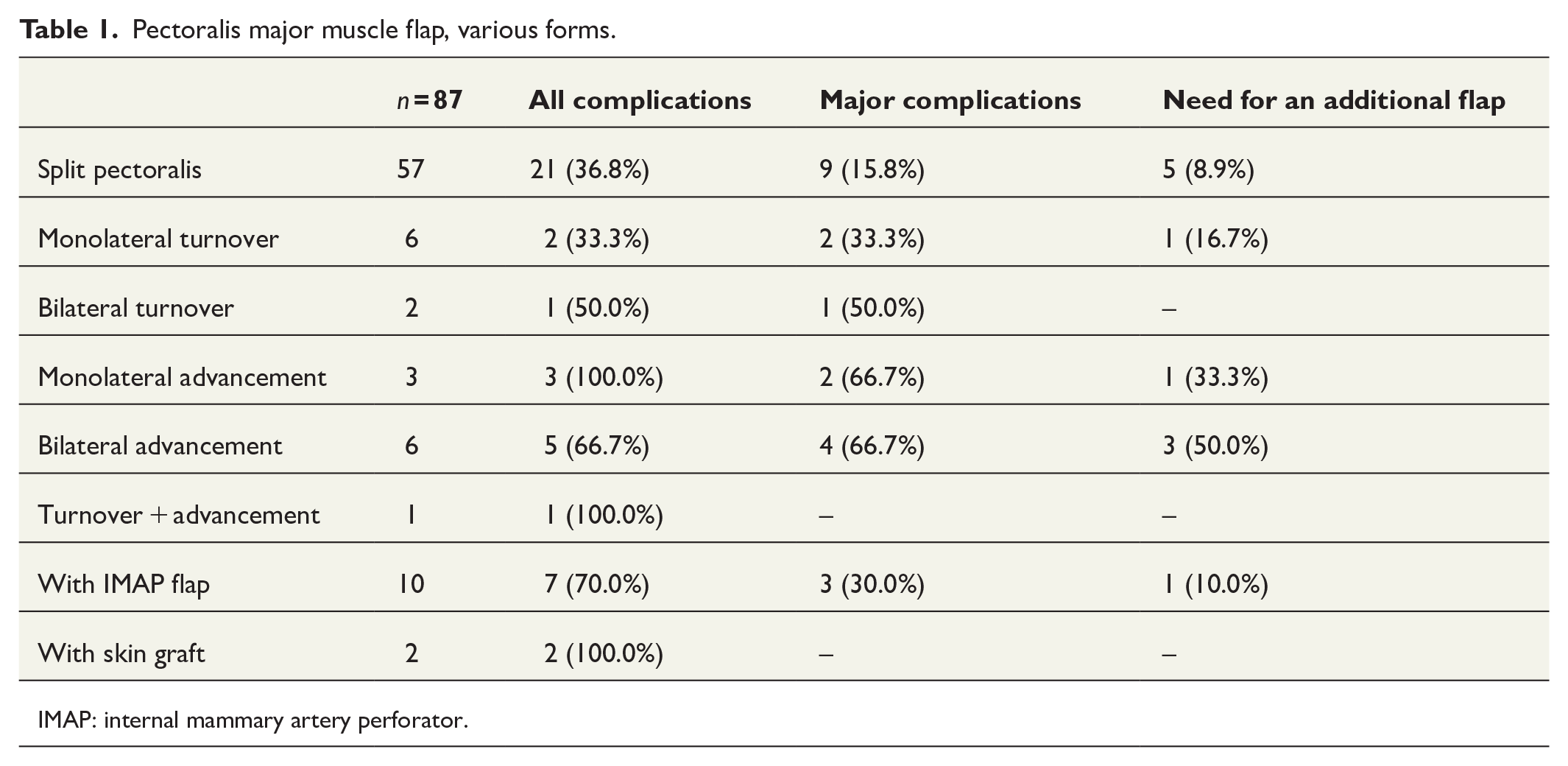
IMAP: internal mammary artery perforator.
The basic characteristics of the three patient groups are represented in Table 2. The distribution of age, obesity, and other co-morbidities, including diabetes, seemed relatively even between the groups. There were only slightly higher EuroSCORE II values in the PICO group. Smoking was more common in the control group 2.
Pre- and intraoperative data.
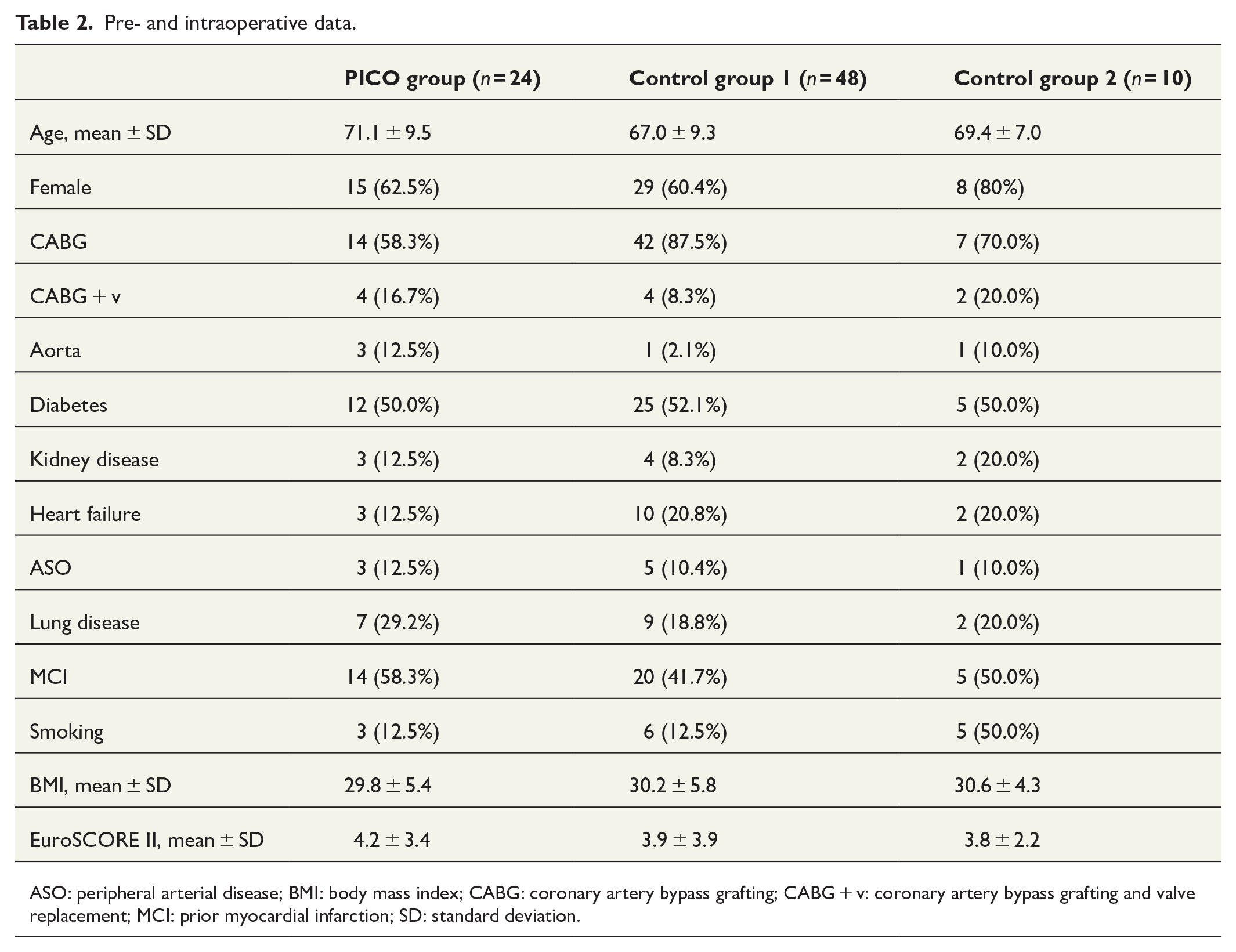
ASO: peripheral arterial disease; BMI: body mass index; CABG: coronary artery bypass grafting; CABG + v: coronary artery bypass grafting and valve replacement; MCI: prior myocardial infarction; SD: standard deviation.
The complication rates were compared between the PICO group and the control group 1. The rate of all complications was 33.0% in the PICO group and 50.0% in the control group 1, with non-statistical difference (P = 0.180). The rates of major complications were 29.2% and 12.5%, respectively (P = 0.148). Only one additional flap was needed in the PICO group whereas seven additional flaps were needed in the control group 1 (P = 0.255). The complications are further described in Table 3. The greatest decline was seen with bleeding complications and partial flap necrosis, although the groups were too small to draw any definitive conclusions. The complication rates in the control group 2 laid in between the complication rates in the two other groups.
Complications.
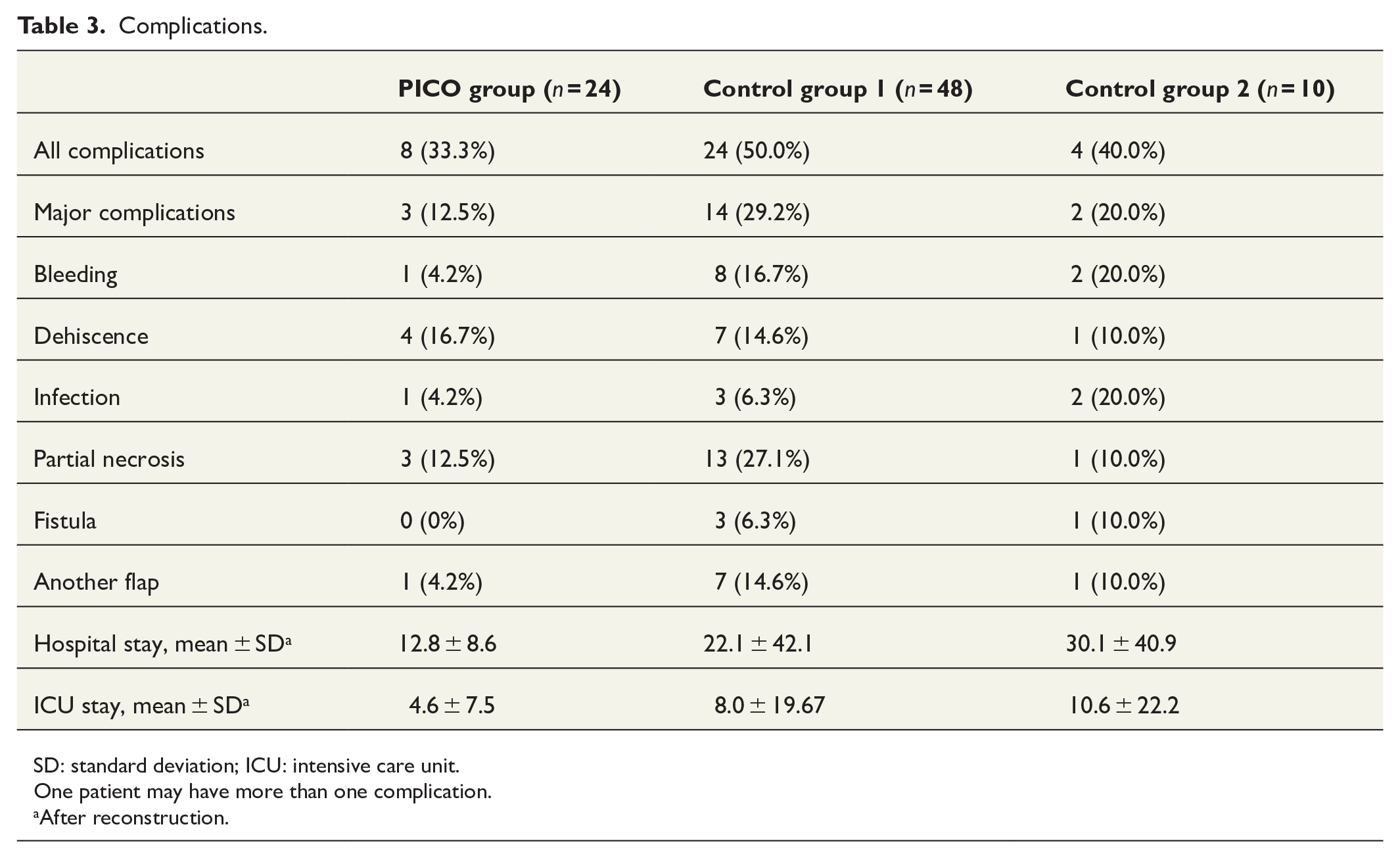
SD: standard deviation; ICU: intensive care unit.
One patient may have more than one complication.
After reconstruction.
Before the adaptation of NPWT and iNPWT into the treatment protocol, the flap-related complication rates showed no tendency to decline over time. The complication rate was 45.8% with the first 24 patients in the control group, operated between 2006 and 2009, and 54.2% with the second 24 patients, operated between 2009 and 2012.
The length of hospital stay after flap reconstruction as well as the length of stay at the intensive care unit after flap reconstruction were shorter in the PICO group when compared to the control group 1 (P = 0.914 and P = 0.096, respectively). The length of the hospital stay was even longer in the control group 2, but the small number of patients in this group must be considered when interpretating the results.
Discussion
Our results using PICO™, with the decrease in major complications from 29.2% to 12.5%, were in line with the previous studies.10,21,22 However, it seemed that some of the decline in the complication rates could be due to the preconditioning of the wound with NPWT. NPWT was adapted into clinical practice just before adapting iNPWT. This matter has not been discussed in the previous studies. The prevalence of NPWT was either not mentioned,10,22 or higher in the iNPWT group, as was the case in this study design as well. 21
In our hospital, PICO™ became a regularly used part of the treatment protocol after sternal flap reconstructions in 2012. The benefits of PICO™ include economical price and ease of use. However, with long or multiform skin incisions, Prevena™ has the benefit of allowing more individual tailoring and fitting of the wound dressing. Since all published results rely on small patient groups, the superiority of one system over another cannot be estimated. In the future, a randomized study concerning the subject would be highly interesting.
Interestingly, the length of hospital stay was shorter in the PICO group when compared to either of the control groups. Consequently, it seems that the shorter hospital stay was associated with postoperative iNPWT rather than preoperative wound conditioning. This may be due to faster wound healing and more confident early mobilization of the patients with iNPWT. Shorter hospitalization periods, if verified in future studies, would yield to certain cost-effectiveness of iNPWT.
In our hospital, the split pectoralis major muscle flap reconstruction is the most common reconstructive method used in the treatment of DSWI. The technique is preferred because of the ability to tailor the muscle portions according to the individual requirements (Fig. 3). The reach into the most caudal part of the sternum is superior in comparison with advancement or standard turnover flap design. The split pectoralis muscle flap remains less widely used when compared to other modifications of the pectoralis major muscle flap. The technique is, although fast and straight-forward in experienced hands, slightly more technically demanding when compared to other forms of the pectoralis major muscle flap. As far as we are aware, this is the largest patient series published reporting the use of this flap option in the treatment of DSWI.
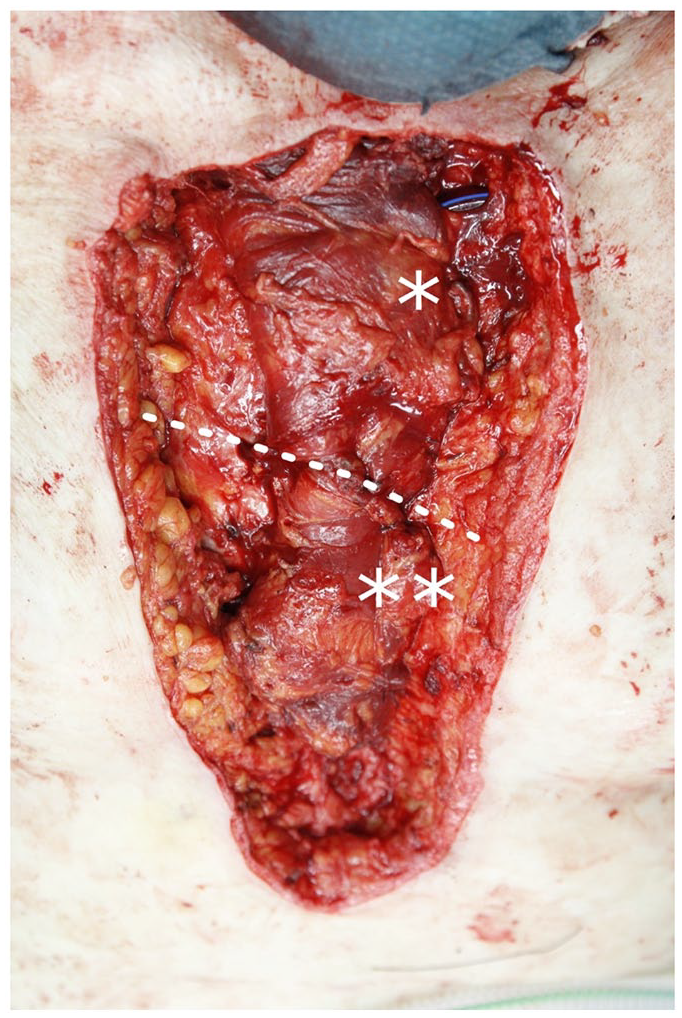
Split pectoralis major muscle flap with *cranial part and **caudal part combined is sufficient to cover the whole length of sternum.
We included, however, all forms of the pectoralis major muscle flap reconstruction in this study. Multiple different ways to use the pectoralis major muscle flap were used when needed. The complication rates with different forms of the flap were described, but potential selection bias prevented further analysis. It seemed, however, that complication rates with the split pectoralis major muscle flap were highly comparable. The size and location of the defect, the ability to reach direct skin closure, the existence of the intact internal mammary arteries, and the experience of the surgeon are some factors influencing the choice of flap.
The major limitation of this study is the retrospective study design and the limited number of patients in each group. However, considering the rarity of DSWI and the subsequent flap reconstructions, randomized study design remains challenging. All previous reports concerning the subject have been retrospective studies with relatively small study groups and historical control group, as was the case in this study as well. Thus, all results remain preliminary. Further studies with larger study groups or meta-analysis are warranted to draw any definite conclusions of the benefits of iNPWT after flap reconstruction.
Conclusion
NPWT seems to have beneficial effect on the rate of surgical complications related to flap reconstruction. Although preoperative preconditioning of the wound with NPWT seems to play its part, some additional benefit with iNPWT can be seen. iNPWT may also be useful to achieve shorter hospitalization periods. The split pectoralis major muscle flap is a versatile reconstruction option suited to be used as a workhorse in the treatment of DSWI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.