
Abstract
Background and objective:
Posterolateral hemivertebrectomy with monosegmental instrumentation at an early age is an established method to correct congenital scoliosis but is associated with a relatively high risk of instrumentation failure and health-related quality of life outcomes are not available. We aimed to investigate the effects hemivertebrectomy with postoperative hip spica cast on complications and health-related quality of life in small children with congenital scoliosis.
Methods:
A follow-up study of 30 children (at mean age = 3.4 years, range = 1.0–8.5 years) undergoing posterolateral hemivertebrectomy and short pedicle instrumentation. Children were immobilized postoperative with hip spica cast for 6 weeks and immobilization for 4 months using a rigid thoracolumbosacral orthosis. The Caregivers filled out Scoliosis Research Society 24 outcome questionnaire preoperatively, at 6 months, and at final follow-up visit on behalf of their child. Standing radiographs were obtained preoperatively, postoperatively in the cast, and standing at final follow-up.
Results:
Mean major curve was 41° (range = 26°–87°) preoperatively and was corrected to 14° (4.0°–35°) at final follow-up. Eight (27%) children had postoperative complications, including three (10%) deep surgical site infections. The Scoliosis Research Society 24 back domain showed an improvement from a mean of 3.8 preoperatively to 4.4 at final follow-up (p < 0.001). Function from back condition domain showed a significant deterioration from 4.2 preoperatively to 3.7 at 6 months (p = 0.020) but improved back to baseline at final follow-up (4.2, p = 0.0022 6 months vs final follow-up).
Conclusions:
Hemivertebrectomy with short instrumentation resulted into 64% correction of scoliosis and improved health-related quality of life in back pain and function domains.
Keywords
Introduction
Congenital scoliosis can be caused by malformations of the vertebrae like hemivertebra, unilateral bar, or a combination of these two.1,2 The treatment of congenital vertebral anomaly focuses on early diagnosis and appropriate surgical management before the development of large curves.3,4,5,6
Hemivertebra is the most frequent case of congenital scoliosis. The fully segmented hemivertebra has a unilateral growth potential creating a wedge-shaped deformity that typically progresses during growth. 7 Posterolateral (PL) hemivertebrectomy with monosegmental instrumentation at an early age is an established method to correct congenital scoliosis and to prevent compensatory curves but is associated with a relatively high risk of pedicle fracture and instrumentation failure.8,9,10,11,12 Supplementation of pedicle screws with a third rod with laminar hooks in young children protects against the most common mode of implant failure in these patients. 11 The senior author has, however, noted that a third rod is often very prominent in small children, and therefore, an advanced postoperative immobilization instead using a hip spica cast has been applied to prevent instrumentation failure.
Quality of life (QoL) is commonly conceptualized as health-related quality of life (HRQoL) in health care research, which includes the perceived impact of a disease and its treatment on physical, psychological, and social well-being.13,14,15,16,17 The effects of PL hemivertebrectomy at an early age on HRQoL remain unknown.
The aims of this study were to evaluate the effects of hemivertebrectomy with postoperative hip spica casting on the surgical outcomes and complications as well as HRQoL in small children with congenital scoliosis. We hypothesized that early hemivertebrectomy would improve radiographic parameters and HRQoL, and second, that postoperative hip spica cast would effectively prevent spinal instrumentation failure in these children.
Materials and methods
Patients
Thirty consecutive children, who had undergone a single-staged PL hemivertebra excision and monosegmental spinal fusion and instrumentation for congenital scoliosis before the age of 10 years between 2009 and 2018, were prospectively followed up at Helsinki and Turku University Hospitals in Finland (Table 1).
Clinical characteristics and perioperative data of the study groups. a
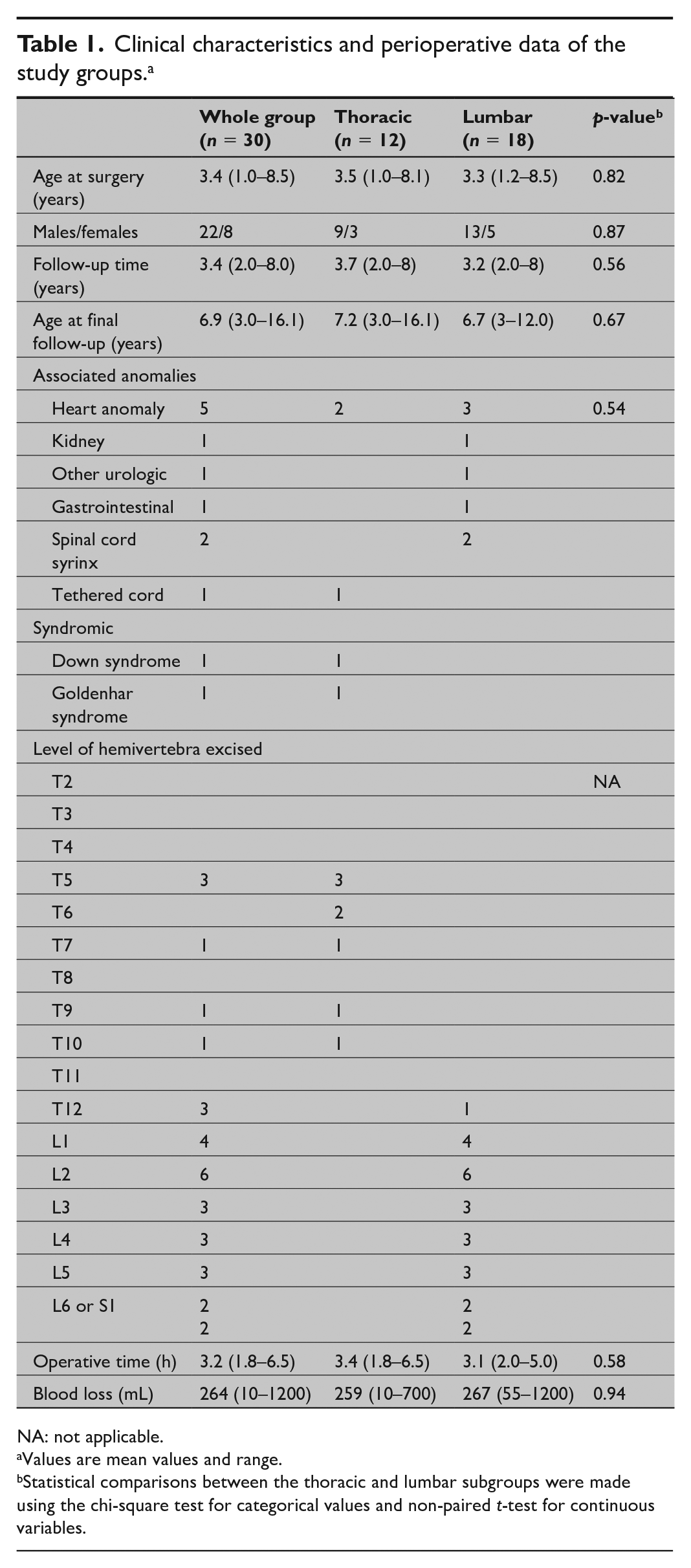
NA: not applicable.
Values are mean values and range.
Statistical comparisons between the thoracic and lumbar subgroups were made using the chi-square test for categorical values and non-paired t-test for continuous variables.
All children were immobilized postoperatively with hip spica cast (both legs) for 6 weeks and immobilization was continued for an additional 4 months with a rigid thoracolumbosacral orthosis. The hip spica cast was extended to above ankle on the operated side and above the knee joint on the other side and to under arm in the upper part to provide adequate immobilization.
Study design
The study design was a retrospective analysis of prospectively collected data, single surgeon case series of 30 children at mean age 3.4 years (range = 1.0–8.5 years) undergoing PL hemivertebrectomy with monosegmental pedicle screw fixation (one pair of pedicle screws above and below the hemivertebrectomy site; Vertex Max and CD 4.5, Medtronic) (Fig. 1). All children had a minimum 2-year radiographic follow-up.
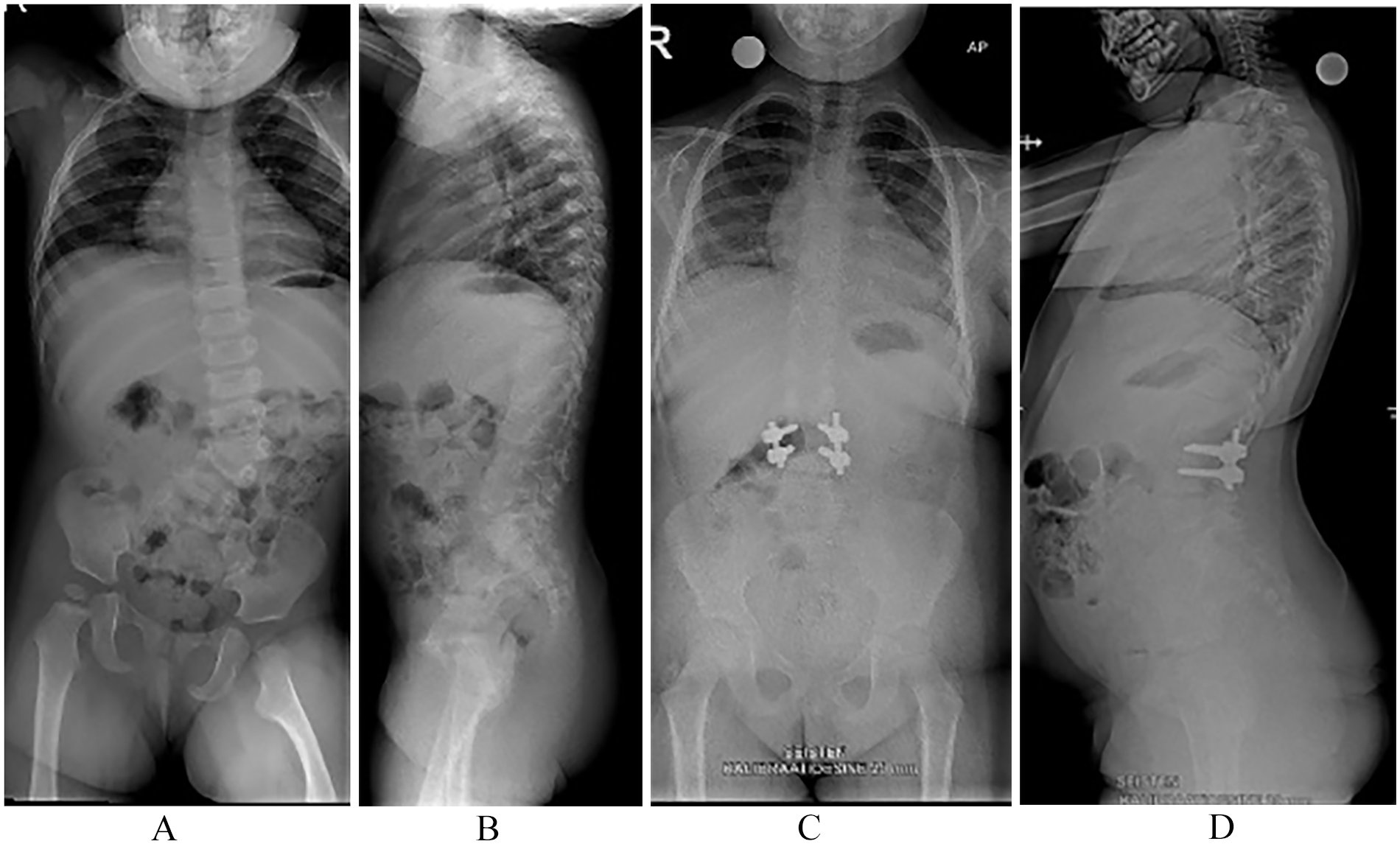
Standing posteroanterior (A) and lateral spinal radiograph (B) on an 18-month-old girl shows an isolated lumbar fully segmented hemivertebra with congenital scoliosis. Standing posteroanterior (C) and lateral spinal radiographs (D) 4 years after posterolateral hemivertebrectomy and one pair of pedicle screws above and below the osteotomy site. Radiographs demonstrate good correction of scoliosis and spinal imbalance with solid intercorporeal spinal fusion.
SRS-24 outcome questionnaire
The parents or other caregivers filled out SRS-24 preoperatively, at 6 months, and at final follow-up visit. The SRS-24 is an original disease-specific HRQoL questionnaire by the Scoliosis Research Society (SRS)18,19,20 used to assess the current state of patients with adolescent idiopathic scoliosis and the effects of scoliosis surgery. The questionnaire consists of 24 questions with a minimum score of 1.0 and maximum score of 5.0, indicating a highly satisfied and asymptomatic patient. The SRS-24 questionnaire has seven domains: pain, general self-image, function from back condition, general level of activity, postoperative self-image, postoperative function, and satisfaction. Each domain score ranges from one to five with higher scores indicating better patient outcomes.18,19,20 The translation of the SRS-24 was performed according to accepted guidelines and this questionnaire has been widely used in our country for HRQoL, but it has not been officially validated in the Finnish cultural setting.19,21 EOSQ-24 would have been the optimal HRQoL questionnaire in this patient group, but it has been launched recently 18 , which prevented us using it as this study was started on 2009. The SRS-24 questionnaire has not been used previously in this patient group, but SRS-22, the modification of this original questionnaire, has recently shown a good correlation with the EOSQ-24 questionnaire in this patient population. 22
Radiographic measurements
Standard standing or sitting posteroanterior and lateral radiographs were taken of the entire spine preoperatively and at follow-up visits. The main thoracic, and thoracolumbar/lumbar curves were measured from the posteroanterior radiographs using the Cobb method. 23 Thoracic kyphosis (T5–T12) and lumbar lordosis (T12–S1) were measured from the lateral radiographs by the Cobb technique by an independent observer experienced in the radiographic measurement techniques (H.M.O. and T.J.).
Statistical methods
Mean values and ranges are given. Mean values and standard deviation (SD) are given for the results of the SRS-24. Statistical comparisons were made using the χ2 test for categorical values and non-paired t-test for continuous variables. Wilcoxon signed-rank sum test was used to evaluate whether significant changes occurred in the SRS-24 domains from preoperative to final follow-up. In postoperative domains (postoperative self-image, postoperative function, and satisfaction), the comparison was between 6-month and the final follow-up. p-values 0.05 or below were considered statistically significant.
Ethical considerations
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments. Ethical committee approval (reference no: ETMK 162/13/03/03/2008 and T216/2018) was obtained from the University Hospital.
Results
Thirty children operated at mean age of 3.4 years (range = 1.0–8.5 years) were identified, and they had a mean postoperative follow-up time of 3.4 years (range = 2.0–8.0 years) (Table 1). Of them, 27 had a single hemivertebra and 3 patients had two hemivertebrae. Fifteen hemivertebrae were in the thoracic and twenty in the lumbar region (Table 2). One child had two hemivertebrectomies at the same level and two children had two hemivertebrectomies at distant levels during the same surgery.
Clinical characteristics of the patients and outcomes of hemivertebrectomy.
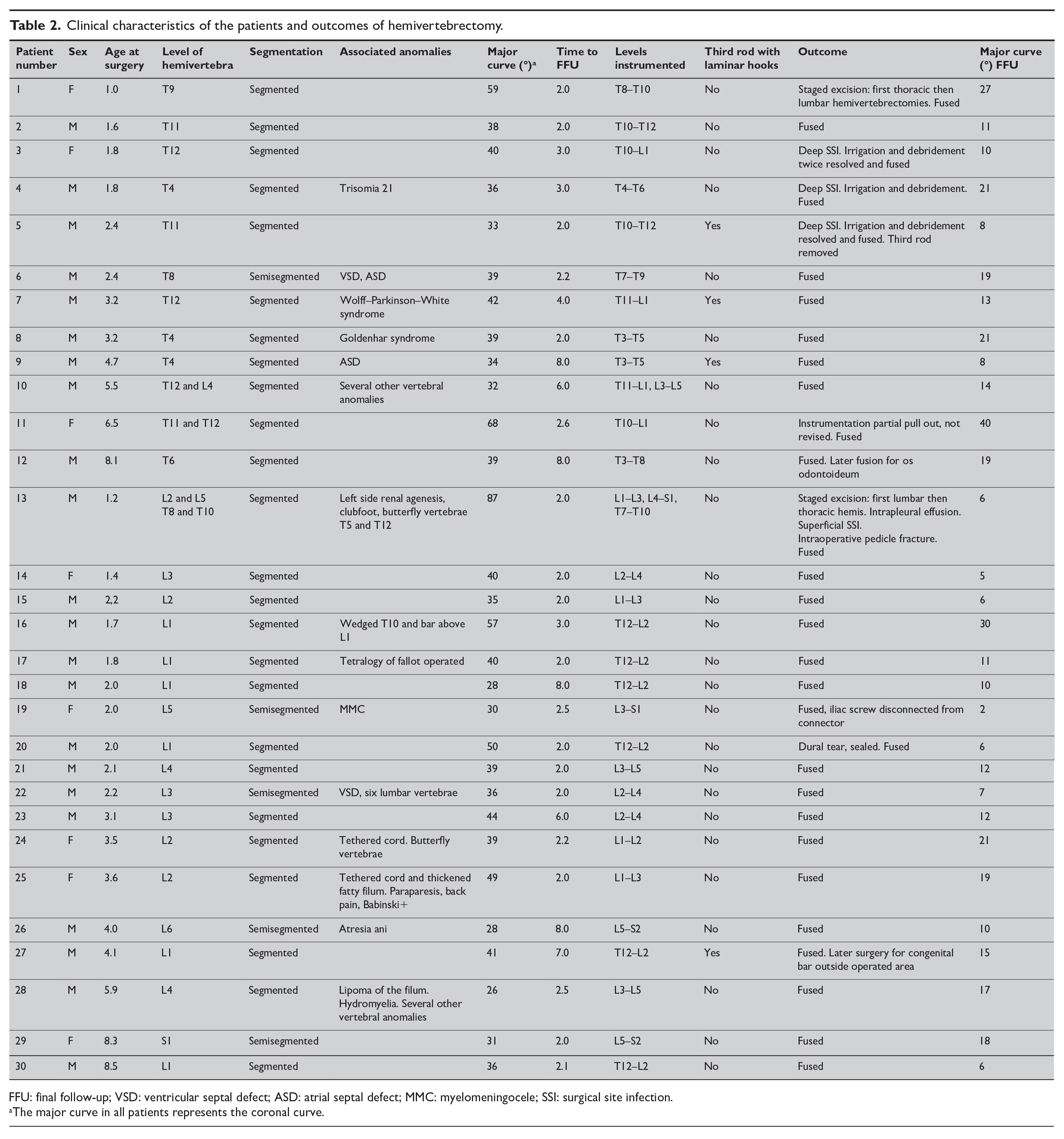
FFU: final follow-up; VSD: ventricular septal defect; ASD: atrial septal defect; MMC: myelomeningocele; SSI: surgical site infection.
The major curve in all patients represents the coronal curve.
Radiographic outcomes
Mean major curve was 41° (range = 26°–87°) preoperatively and was corrected to 14° (4.0°–35°) at final follow-up (FFU) (mean correction 64%) (p < 0.001) (Tables 2 and 3; Fig. 1). In the subgroups, the major curves averaged preoperatively 42° (range = 32°–64°) in the thoracic group and 41° (range = 26°–87°) in the lumbar group (Tables 2 and 3). These were corrected to 16° (range = 4.0°–35°) in the thoracic group and 12° (range = 6.0°–21°) in the lumbar group at final follow-up (p < 0.001 preoperative vs final follow-up). This represented a 62% correction of the thoracic and 71% in the lumbar group (not significant (NS)).
Radiographic outcomes. a
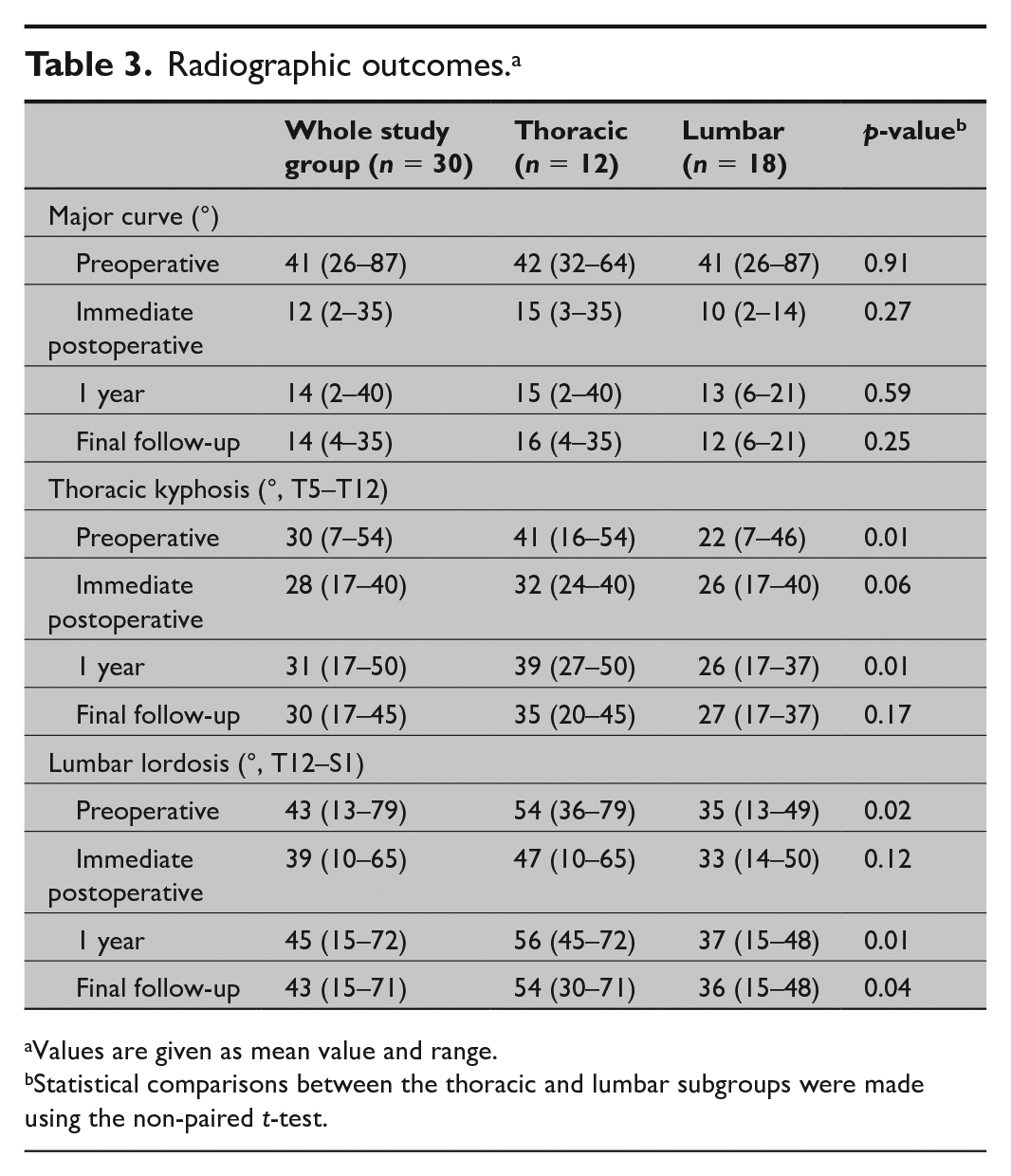
Values are given as mean value and range.
Statistical comparisons between the thoracic and lumbar subgroups were made using the non-paired t-test.
In the whole group, the mean thoracic kyphosis (T5–T12) and lumbar lordosis (T12–S1) remained unchanged from preoperative to final follow-up (mean thoracic kyphosis 30° and lordosis 43° preoperatively and at final follow-up, NS) (Table 3). In the subgroup analysis, thoracic kyphosis (T5–T12) averaged preoperatively 41° in the thoracic group and 22° in the lumbar group (p = 0.010) and were 35° in the thoracic group and 27° in the lumbar group at final follow-up FU (p = 0.17). Similarly, lumbar lordosis (T12–S1) averaged preoperatively 54° in the thoracic group and 35° in the lumbar group (p = 0.020) and were 54° in the thoracic group and 36° in the lumbar group at final FU (p = 0.040).
Complications
Eight (27%) children had complications, including one intraoperative pedicle fracture, one cerebrospinal fluid leak, one superficial surgical site infection (SSI), three deep SSIs, one distal femoral fracture, and one with pleural effusion requiring chest tube (Supplemental Material). There was no spinal cord or permanent nerve root associated complications. Eight children required additional surgery: three for deep wound infection (irrigation and debridement) and one for laminar hook removal. The indication for a hook removal was a prominent implant not a complication. Two children underwent additional hemivertebrectomy at another level. There were two postoperative partial instrumentation failures during follow-up which did not change the course of treatment (one unilateral iliac screw and connector disconnection; one partial unilateral pedicle screw pull out). One child had later surgery for congenital bar at distant level and one atlantoaxial arthrodesis for os odontoideum with cervical instability.
HRQoL
In the whole group, the mean (SD) SRS-24 total scores were preoperatively 4.52 (0.42), 3.83 (0.37) at 6 months, and 4.10 (0.41) at final follow-up (p < 0.001 preoperative vs 6 months and preoperative vs final follow-up) (Table 4). The SRS-24 back pain domain showed an improvement from a mean (SD) of 3.85 (0.50) preoperatively to 4.17 (0.57) at 6 months (p = 0.064) and further to 4.38 (0.72) at final follow-up (p < 0.001). The function from back condition domain showed a significant deterioration from 4.23 (0.47) preoperatively to 3.70 (0.63) at 6 months (p = 0.020) but improved back to baseline at final follow-up (4.22 (0.18), p = 0.0022 6 months vs final follow-up). The satisfaction domain was on high level being 4.52 (0.64) at 6 months and 4.41 (0.48) at final follow-up (NS). There were no significant differences in the SRS-24 total score or the domains between the thoracic and lumbar hemivertebra subgroups preoperatively, at 6 months, or at final follow-up. As the questionnaire SRS-24 was not constructed for small children, we also present results of those individual questions that are applicable for this age group (Table 5). These scores show a similar tendency with a postoperative decrease and return to preoperative level as the domain scores.
Changes in the Scoliosis Research Society (SRS-24) domain scores. a
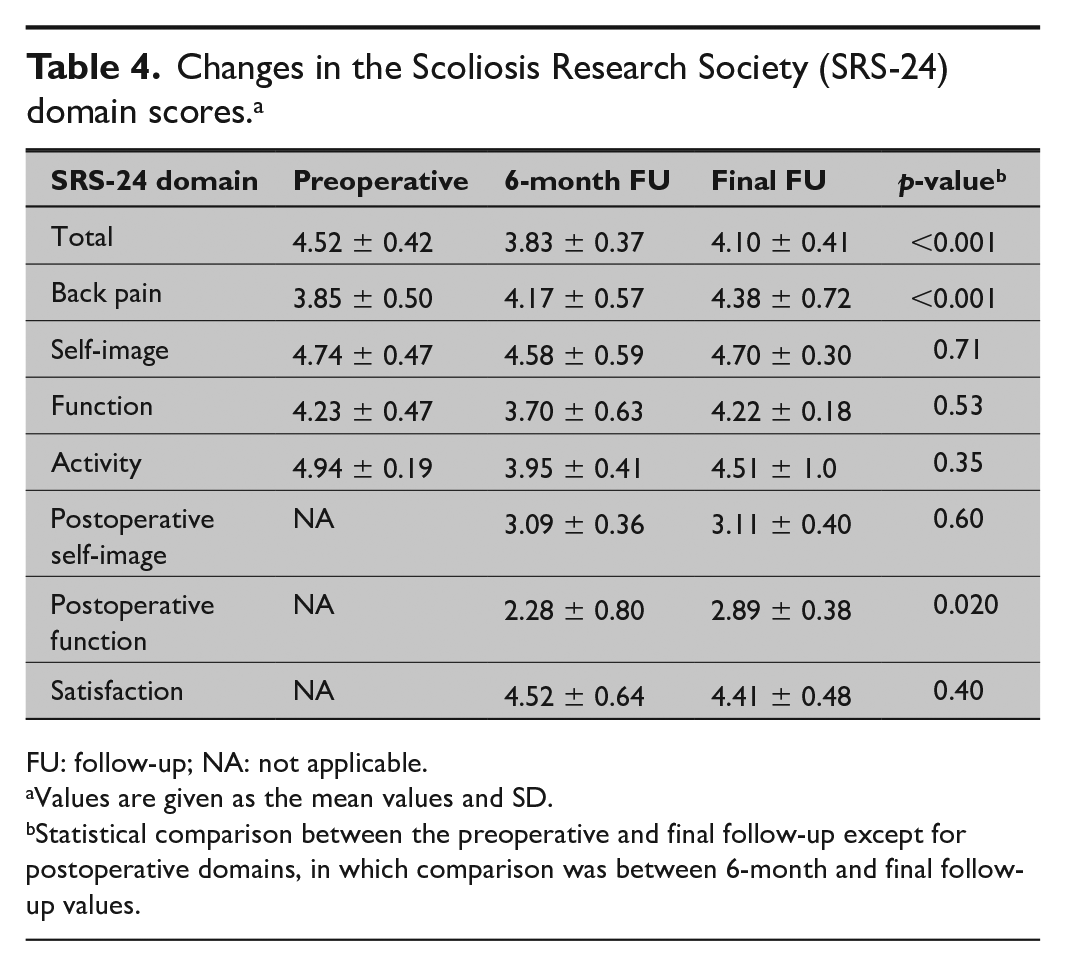
FU: follow-up; NA: not applicable.
Values are given as the mean values and SD.
Statistical comparison between the preoperative and final follow-up except for postoperative domains, in which comparison was between 6-month and final follow-up values.
Individual question scores on the SRS-24 outcome questionnaire.
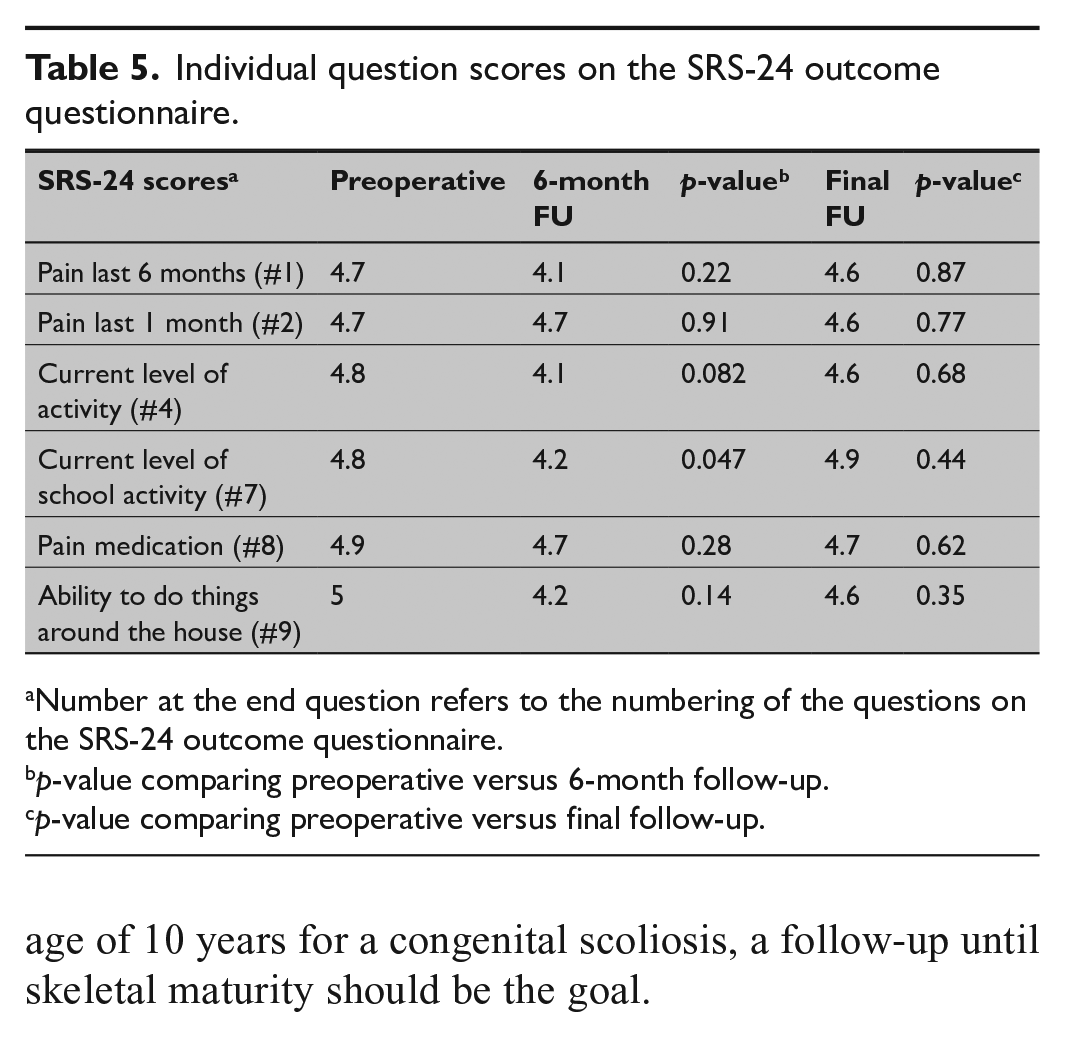
Number at the end question refers to the numbering of the questions on the SRS-24 outcome questionnaire.
p-value comparing preoperative versus 6-month follow-up.
p-value comparing preoperative versus final follow-up.
Discussion
Strengths and limitations
The study design was a prospective data collection with a radiographic follow-up rate of 100%. Validated patient outcome tool, SRS-24, was used for the HRQoL evaluation. All the surgical procedures were carried out by the same orthopedic spine surgeon. The surgical technique was standardized, that is, PL hemivertebrectomy with monosegmental pedicle screw fixation and all were immobilized postoperative with both leg hip spica cast and rigid thoracolumbar orthosis. HRQoL evaluation included preoperative, 6 months, and 2-year follow-up.
It should be noted that because of the young age, the patients themselves were not able to fill out the questionnaires and required help from their parents. The SRS-24 has been designed to be used in the evaluation of treatment outcomes in adolescent idiopathic scoliosis. 19 However, there was no other validated scoliosis-specific health-related quality of questionnaire available, when this follow-up study was planned and initiated in 2009. In addition, the SRS-22 questionnaire, which is a modification of the original SRS-24, has been shown to provide similar results as the early onset scoliosis questionnaire 24 (EOSQ-24) in congenital scoliosis with the strongest relationship between the age group between 0 and 5 years. 22 The domains of the SRS questionnaire used in this questionnaire such daily activities outside the home may reflect more the QoL in teenagers and not in smaller children. The HRQoL assessment did not take into account the normal development during childhood, for example, starting to walk around the age of one. However, 29 out of 30 children had started to walk before the hemivertebrectomy.
The reliability to let caregivers answer instead of the patient has been evaluated previously and seems a reliable method.24,25,26 It is possible that not the same caregiver answered the questionnaire pre- and post-operatively. Although many of the children with congenital scoliosis presented with other associated anomalies, for example, cardiac or renal, none of these children had mental developmental problems, which could have affected the HRQoL assessment. Other limitations of this study include a relatively small patient group. Follow-up period was minimum 2 years, but as these children were operated all before the age of 10 years for a congenital scoliosis, a follow-up until skeletal maturity should be the goal.
Comparison with previous data
Ruf and Harms were the first to describe a PL hemivertebrectomy with monosegmental pedicle screw technique. 10 Pedicle fracture or pedicle screw pull out has been an issue with this otherwise effective technique for congenital scoliosis.11,12,13 Therefore, Hedequist et al. 11 introduced a three-rod instrumentation using bilateral pedicle screws and a hook construct between these two rods. In our practice, the third rod has been very prominent in younger children (less than 5 years). To reduce the forces acting on the pedicle screws, we have employed a technique of a temporary third rod using the hooks as an additional corrective maneuver and this third rod has been removed at the end of surgery. In addition, all patients have been casted into a both leg hip spica cast. These maneuvers seem to be useful, as we did not see any patient with postoperative pedicle fracture in this case series (Fig. 1).
A few studies have investigated the effects of hemivertebrectomy on the HRQoL in young children. 10 The effect of immobilization at an early age on HRQoL has remained unknown. The difficulties encountered in this evaluation include their young age, and therefore, we asked their parents to fulfill these questionnaires. 22 In accordance with our hypothesis, the long immobilization (cast 6 weeks and brace 3 months) decreased their QoL at 6 months, although the function domain of the SRS-24 improved further to final follow-up. Future research needs to address ways to decrease the incidence of skin-related complications.
Conclusion
Hemivertebrectomy at a mean age of 3.4 years provided 64% correction of scoliosis. Postoperative high hip spica cast prevented postoperative instrumentation failure in all 30 consecutive children, but three children (10%) developed deep SSI. The HRQoL as assessed using SRS-24 questionnaire filled out by caregivers suggested improvement in pain domain and high satisfaction.
Supplemental Material
sj-pdf-1-sjs-10.1177_14574969211020640 – Supplemental material for Outcomes of early hemivertebrectomy in children with congenital scoliosis: A prospective follow-up study
Supplemental material, sj-pdf-1-sjs-10.1177_14574969211020640 for Outcomes of early hemivertebrectomy in children with congenital scoliosis: A prospective follow-up study by Hanna M. Oksanen, Tuomas Jalanko and Ilkka J. Helenius in Scandinavian Journal of Surgery
Footnotes
Author contributions
H.M.O. collected the data, analyzed the data, and wrote the manuscript. T.J. collected the data, analyzed the data, and edited the manuscript. I.J.H. performed the surgeries, and wrote the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.M.O. and T.J. declare no conflict of interest. I.J.H. is a consultant for Medtronic International, and received grants and research funding from Medtronic International and Baxter International.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical committee approval was obtained from the University Hospital (reference. no. ETMK 162/13/03/03/2008 and T08/035/19). As no patients were contacted, no informed consent was requested by the ethical committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The grants to the institution were received from Medtronic International and K2M via Innosurge.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.