
Abstract
Background and Aims:
Although thymoma is inextricably linked to autoimmune disease, its best treatment method remains unclear. In this study, we sought to evaluate therapeutic effect of surgical resection of thymoma on non-myasthenia gravis autoimmune diseases.
Materials and Methods:
This was a retrospective study covering 32 patients with thymoma accompanied with non-myasthenia gravis autoimmune disease. The relationships between surgical treatment, thymoma pathological type, and prognosis of autoimmune diseases were analyzed from postoperative follow-up data.
Results:
In total, 32 patients in this study underwent surgical treatment. The mean age of the patients was 51.7 years. By the last follow-up, 2 patients had died, while the other 30 patients showed no sign of tumor recurrence and metastasis. According to the postoperative follow-up data, 22 patients (68.75%) showed improvement or even complete recovery of autoimmune disease symptoms, 9 patients (28.13%) showed no significant change, and only 1 patient’s (3.12%) postoperative symptom was aggravated. Female patients and patients aged 50 and older were more likely to combine with non-organ-specific autoimmune diseases (p = 0.036, p = 0.017).
Conclusions:
In conclusion, this study presents that surgical treatment achieves a satisfactory prognosis for thymoma combined with non-myasthenia gravis autoimmune disease.
Introduction
Thymoma is the most common tumor in the anterior superior mediastinum originating from thymic epithelial cells. Thymoma is often associated with many autoimmune diseases, such as myasthenia gravis (MG), pure red cell aplasia (PRCA), and Good’s syndrome (GS). Since the first report of thymoma with MG by Simpson 1 , a number of studies investigating the association between autoimmune disease and thymoma have ensued. However, due to low incidence, most of them are case reports. We have not found that the systematic analysis of the relationship between the thymoma and autoimmune diseases exists in literature yet. In this study, we included patients who had received surgical treatment for thymoma combined with non-MG autoimmune diseases at Peking Union Medical College Hospital (PUMCH) in the past 12 years. We then analyzed their clinical data to explore the therapeutic effect of surgical resection of thymoma on non-MG autoimmune disease.
Materials And Methods
We reviewed 327 patients who had received surgical treatment in PUMCH from 2007 to 2019 for thymoma complicated with autoimmune disease. After exclusion of MG patients, 32 patients were included in the study. Based on the type of autoimmune disease, the patients were divided into organ-specific and non-organ-specific autoimmune disease (OSAD and NOSAD) groups. We define OSAD as the autoimmune that pathological damage and dysfunction of tissues and organs are limited to one organ, and NOSAD is defined as autoimmune that involves multiple organs and tissues throughout the body. The patients were followed up by telephone or during outpatient visits. Data collected from follow-up included the treatment of thymoma before and after operation, the recurrence and metastasis of tumor after operation, and the prognosis of autoimmune disease. The improvement of autoimmune disease was reflected by the continuous decrease of immune-related indices, improved clinical symptoms, recovery of laboratory test indices related to autoimmune diseases, and the decrease or withdrawal of drug dosage needed to alleviate the respective symptoms. After the follow-up, sex, age, operation mode, postoperative pathology, and prognosis of autoimmune diseases data were analyzed and recorded.
SPSS 25.0 software was used to perform rank correlation analysis, Pearson’s correlation, Mann–Whitney test, and Kruskal–Wallis test. Clinical significance was set at p < 0.05.
Results
Distribution Of Admitted Patients
Of the 32 patients, 12 were male and 20 were female. The average age of the patients in the study was 51.7 years (Table 1); 26 patients placed into the OSAD subgroup, with a male to female ratio of 12:14, and had an average age of 53.0 years. The remaining six patients (all female, with an average age of 45.7 years) were designated into the systemic autoimmune disease group. The median follow-up time was 53.5 months (9–143 months).
General conditions of included patients and prognosis of autoimmune diseases.
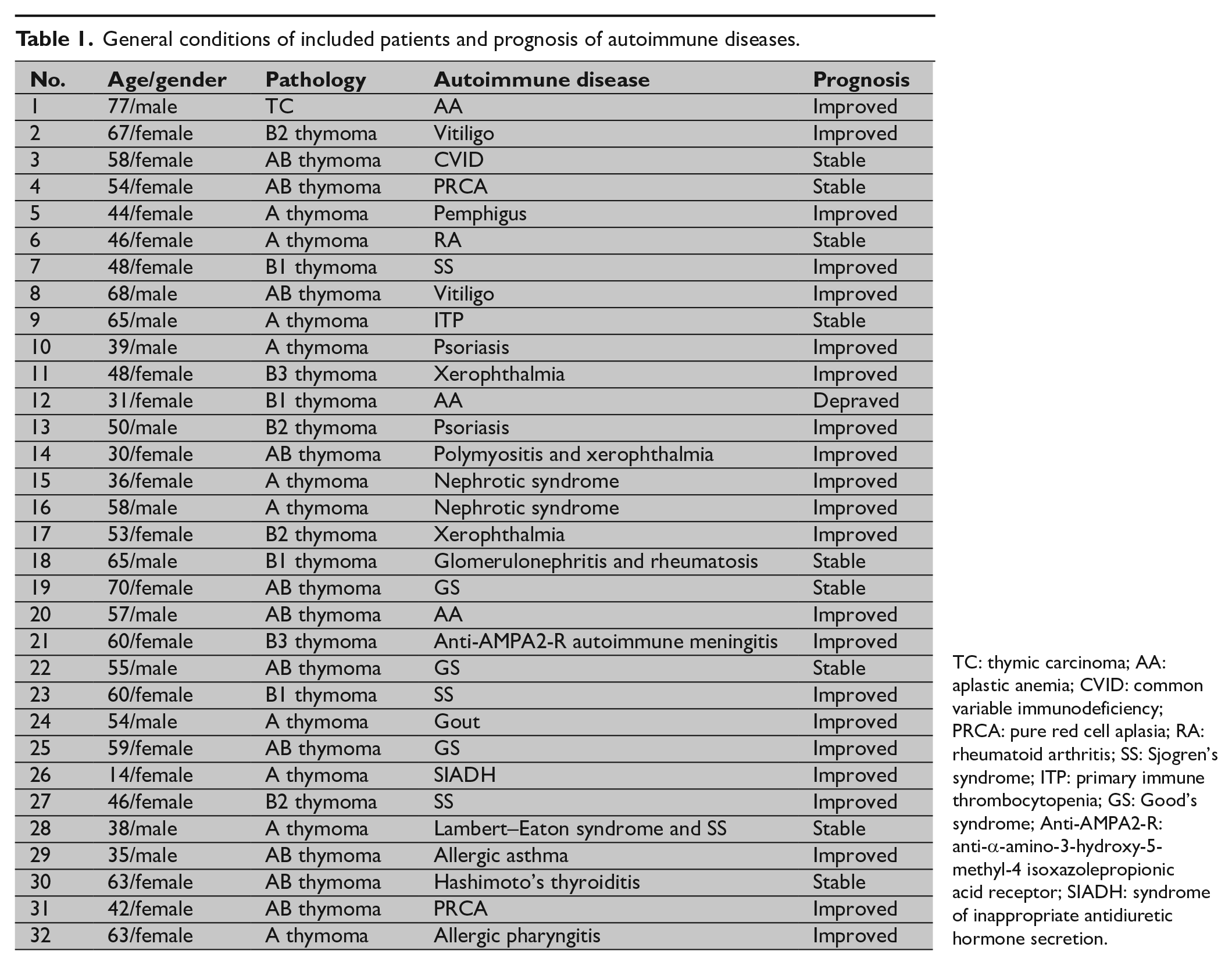
TC: thymic carcinoma; AA: aplastic anemia; CVID: common variable immunodeficiency; PRCA: pure red cell aplasia; RA: rheumatoid arthritis; SS: Sjogren’s syndrome; ITP: primary immune thrombocytopenia; GS: Good’s syndrome; Anti-AMPA2-R: anti-α-amino-3-hydroxy-5-methyl-4 isoxazolepropionic acid receptor; SIADH: syndrome of inappropriate antidiuretic hormone secretion.
Thymoma and surgical status
All the patients in this study underwent surgical treatment, and different operative approaches were used based on the tumor location, size, and relationship with the surrounding tissue. These included neck incision, median thoracotomy, and thoracoscopic surgery (Table 2). The median diameter of the tumor was 4.5 cm (1.5–15 cm). Except for three patients with pleura or phrenic nerve invasion, no significant tumor invasion was found in the other patients. All the 32 patients included in this study had no severe perioperative complications, like phrenic nerve invasion and temporary or permanent diaphragm paralysis. Postoperative pathology showed that the pathology of thymoma was distributed from type A thymoma to thymic carcinoma, and all the cases’ tumor margin were free. Non-MG autoimmune diseases were more common in patients with type AB and A thymoma (34.37%, 31.25%). However, there was no significant difference in the distribution of autoimmune diseases in different types of thymoma (p = 0.906; Fig. 1). We performed Tumor, Node, Metastasis (TNM) staging and Masaoka staging, and established that the two staging systems yielded consistent results (p = 0.001). None of the patients included received neoadjuvant therapy before operation, while four patients received adjuvant radiotherapy after operation. The four patients were suspected tumor invasion during operation, and postoperative adjuvant radiotherapy was used to reduce the possibility of recurrence. The follow-up examination was carried out every 6 months and consisted of computed tomography (CT) scans for chest and abdomen to monitor tumor recurrence or metastasis. By the last follow-up, 32 patients showed no sign of tumor recurrence and metastasis (Table 2).
General conditions and prognosis of thymoma.
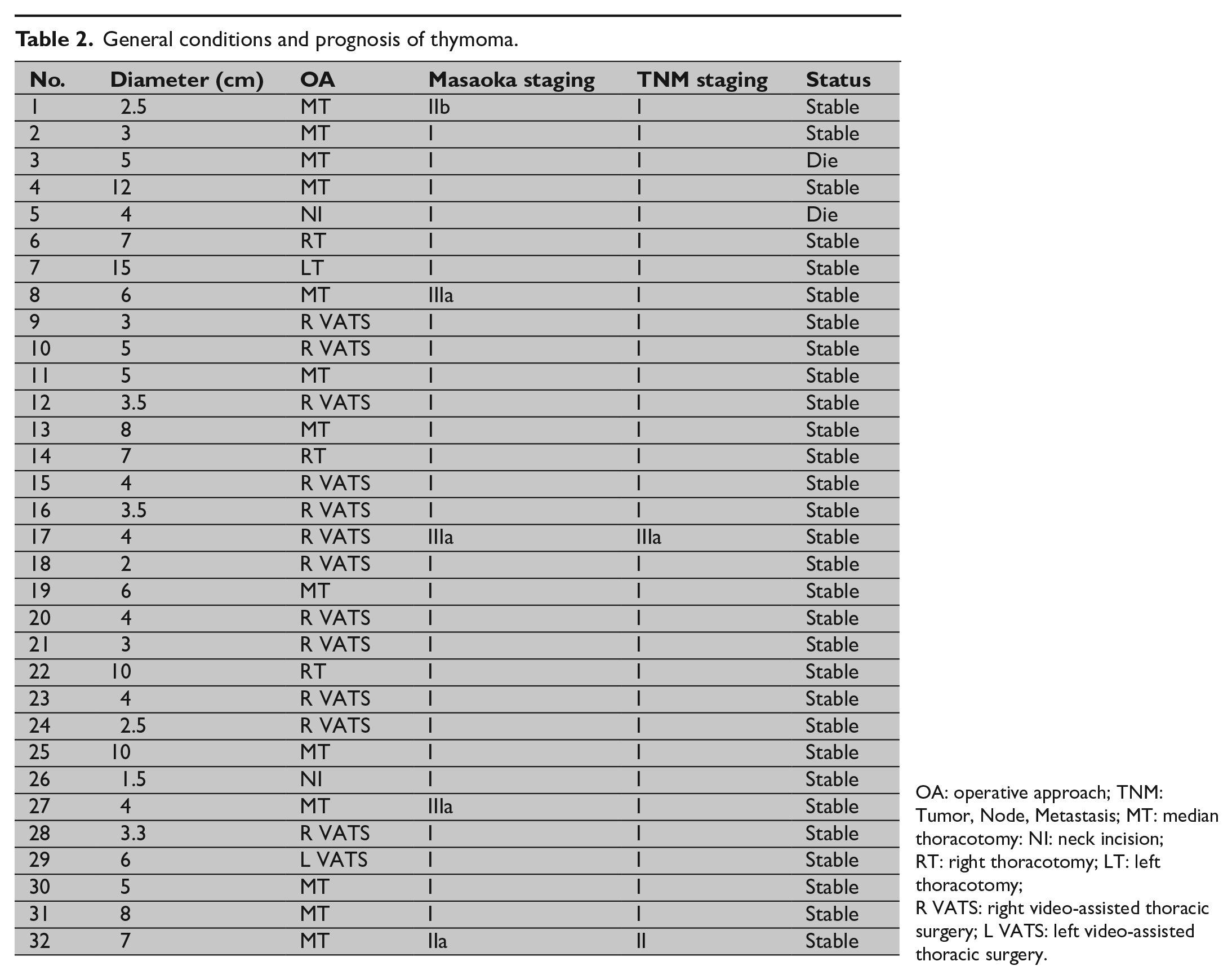
OA: operative approach; TNM: Tumor, Node, Metastasis; MT: median thoracotomy: NI: neck incision; RT: right thoracotomy; LT: left thoracotomy; R VATS: right video-assisted thoracic surgery; L VATS: left video-assisted thoracic surgery.
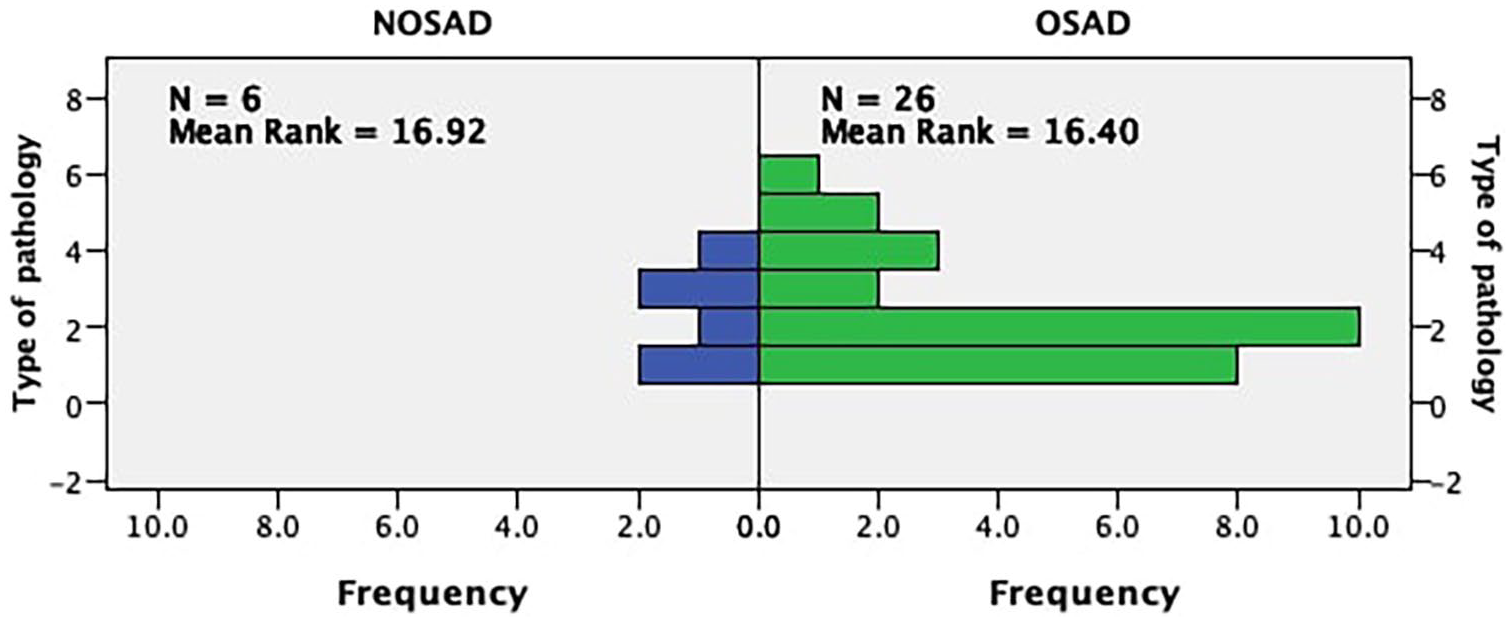
Distribution of different autoimmune diseases in different types of thymoma.
However, two patients succumbed to death: one patient combined with pemphigus had positive progress after operation, but died of multiple organ failure, 2 years after operation; another patient died 6 years after operation of systemic multiple organ failure triggered by liver failure, and her combined autoimmune disease, common variable immunodeficiency, was not significantly improved after surgery.
Outcome Of Autoimmune Disease
Among the included patients, there were 22 types of autoimmune diseases, including GS, Sjogren’s syndrome, and Lambert–Eaton syndrome (Table 1). In 29 patients, thymoma was combined with single autoimmune disease, while in 3 patients, the combination involved multiple autoimmune diseases. These included polymyositis and xerophthalmia, glomerulonephritis and rheumatosis, and Lambert–Eaton syndrome and Sjogren’s syndrome, separately. We observed gender and age differences in the occurrence of different types of autoimmune diseases, with female patients prone to suffer from NOSADs (p = 0.036), and patients aged 50 and above are more likely to have a combination of NOSADs (p = 0.017). Among the 32 patients in the study, 22 patients (68.75%) showed improvement or even complete recovery of autoimmune diseases by the last follow-up, after operation. However, nine patients (28.13%) had no significant improvement in treatment symptoms and laboratory indices of autoimmune diseases compared with before operation, and only one patient (3.12%) had an exacerbation of autoimmune disease symptoms. There was no significant difference in the prognosis of different types of autoimmune diseases (p = 0.494; Fig. 2) and in the prognosis of autoimmune diseases among different pathological types of thymoma (p = 0.561). In addition, although there were some differences in TNM stage and Masaoka stage between the two staging methods, there was no significant difference in disease outcome between them (p = 0.653, p = 0.788).
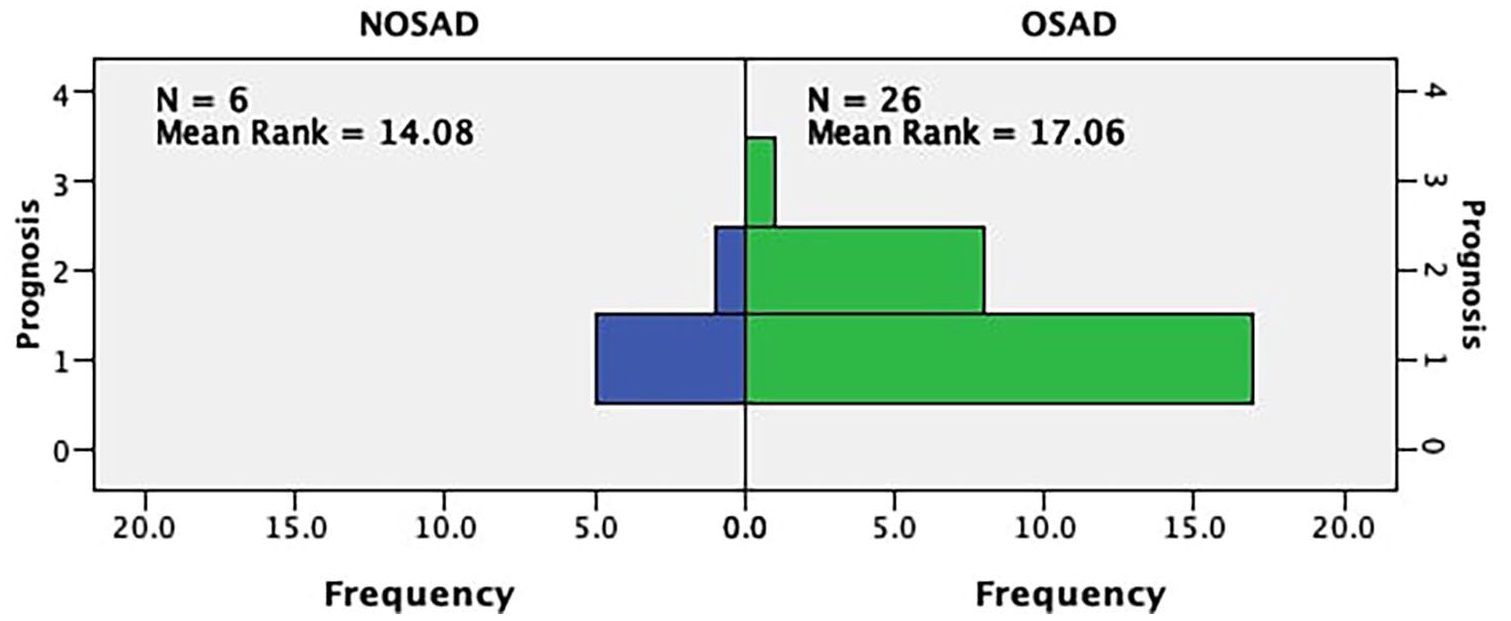
Prognosis of different types of autoimmune diseases.
The following were the specific situations of 22 patients that had improved outcome of autoimmune diseases:
One patient with GS was treated with gamma globulin to correct immune deficiency. The prescriptions before and after the operation were 20 g/day for 5 days and 10 g/day for 3 days. The frequency of gamma globulin administration was further reduced from once a month before operation, to once in every 3 months.
The frequency of symptom attack in two patients with vitiligo reduced after the operation; symptoms also alleviated.
One patient with polymyositis combined with xerophthalmia was treated with prednisone 10 tablets (50 mg) per day before operation and was relieved of the systemic muscle pains after operation. In addition, xerophthalmia symptoms disappeared completely in two patients after operation.
One patient with aplastic anemia had a hemoglobin concentration of 98 g/L, which was restored to 135 g/L after operation. Normal hemoglobin concentration was also restored in two patients that had PRCA within 3 months after operation.
One patient with anti-α-amino-3-hydroxy-5-methyl-4 isoxazolepropionic acid receptor encephalitis (anti-AMPA2-R autoimmune meningitis) exhibited decreased memory and cognitive ability symptoms before operation. However, the anti-AMPA2-R antibody decreased from 1:100 to 1:32 after operation, and the memory and cognitive ability of the patients also recovered. Besides, the initial treatment of eight prednisone tablets (40 mg) per day was withdrawn after operation.
Before operation, one patient with abnormal antidiuretic hormone secretion syndrome was treated with tolvaptan 0.5 tablets (15 mg) per day, and salt capsule 3 g qid, to control blood sodium. After operation, blood sodium improved to 140 mmol/L, and sodium supplementation drugs were withdrawn.
There were two patients with nephrotic syndrome. In one case, preoperative blood pressure of 200/120 mm Hg dropped to 110/60 mm Hg after operation, and preoperative urinary protein quantity reduced from 15 to 0.8 mg/d postoperation. The prednisone dosage was also reduced from 14 tablets (70 mg) per day before operation to 0.5 tablets (2.5 mg) per day. In the second case, urinary protein reduced from 17,939.5 to 0.13 mg/d, and dosage of methylprednisolone from 14 tablets (70 mg) per day before operation to 2 tablets (10 mg) per day plus cyclosporine 6 tablets per day.
In two patients with psoriasis, the frequency of onset of symptoms (distributed in scalp and lower extremity) decreased after operation, therefore decreasing the disease severity.
One patient with pemphigus was treated with prednisone tablets: eight tablets (40 mg) per day before operation and six tablets (30 mg) per day after operation.
Interestingly, all of the three patients who only combined with Sjogren’s syndrome had different degrees of remission or total disappearance of symptoms after operation.
One patient with gout had an improvement of degree and frequency of symptoms onset after operation.
One patient had allergic pharyngitis before operation, and the cough symptoms disappeared completely after operation; the frequency and degree of postoperative asthma attacks were improved in another patient with allergic asthma.
Discussion
The thymus, as an immune organ of the human body, is involved in a variety of immunological functions, including T-cell maturation and autoimmune tolerance 2 . Thymic epithelial tumors are components of a poly-autoimmune syndrome 3 and are commonly associated with many autoimmune diseases, with autoantibody-mediated MG occurring in about 40% of patients 4 . In 30% of thymoma patients, autoimmune diseases are usually diagnosed either in a comorbid state or at post-thymectomy, whereas up to 50% of patients are diagnosed concomitantly with two autoimmune diseases5,6. In this study, we conducted a review of 32 thymoma cases with non-MG autoimmune diseases. We established that the incidence of thymoma combined with non-MG autoimmune diseases was about 9.79%, of which 9.38% was the incidence of multiple autoimmune diseases. After follow-up, we found that the surgical removal of thymoma could effectively control the development of autoimmune diseases, leading to a better prognosis. In addition, we observed that in female patients, the combination of thymoma with NOSADs was more common, and NOSADs were more common in patients older than 50.
In an attempt to explain the relationship between thymoma and autoimmune disease, three theories have been put forward. According to immature T-cell theory, epithelial components and lymphocytes of thymoma closely mimic normal thymocytes. However, unlike normal thymocytes, thymoma-derived thymocytes may not be mature and lack the self-tolerance needed to maintain normal function. The thymoma-derived thymocytes mentioned above may shed into the peripheral blood circulation and escape the key steps of medullary selection and maturation, thus becoming autoreactive. In the theory of neoplastic–genetic theory, thymocytes acquire their antigen specificity in the thymic cortex, where the arrangement of T-cell receptor genes occurs. The high proliferation rate of thymocytes in the thymoma cortex is a high factor for genetic mutations 7 . In addition, it has been reported that thymocytes acquire self-reactivity in the hyperproliferative region of the thymic cortex 8 . Furthermore, neoplastic epithelial cells in thymoma have been reported to be genetically different from the normal thymus cells, due to the slight reduction observed in the expression of HLA-DR (human leukocyte antigen-DR) molecules in the former. Such impaired expression of HLA-DR in neoplastic epithelial cells may affect the positive selection and autoreactivity associated with HLA-A24 and HLA-B8, which are significant predictive factors for MG. Finally, in the combined cellular and humeral deregulation theory, a model consisting of two independent steps has been put forward 9 . The first step involves a large number of thymoma-derived CD8+ T cells exhibiting impaired tolerance, therefore initiating an autoimmune cascade. In the second step, the activation of CD4+ T cells that drives the transformation from cellular to humoral immunity occurs, which, in turn, activates B cells to produce auto-antibodies. The presence of aberrant autoimmune CD4+ T cells in thymoma-associated MG as well as association of thymoma support this mechanism with the presence of autoantibodies in other diseases. From the above theories, resection of thymoma can significantly control autoimmune diseases by restraining its progress. Combined with the postoperative pathological results, we suggest that performing an enlarged thymectomy to obtain complete thymoma resection and thymectomy is an important factor in achieving satisfactory surgical results.
Previous reports on thymoma complicated with autoimmune disease mostly exist as case reports. Various autoimmune diseases, including aplastic anemia 10 , Sjogren’s syndrome 11 , and total encephalitis 12 , have been satisfactorily controlled through the removal of thymoma or thymectomy. This study encompassed a variety of autoimmune diseases, including pure erythrocyte aplastic anemia, GS, anti-AMPA2-R autoimmune meningitis, and nephrotic syndrome. Through postoperative follow-up and monitoring, most patients achieved stable or improved prognosis after operation (31/32). Like in previous case reports, patients with autoimmune diseases in this study underwent total thymectomy.
In 1954, three patients with thymoma and hypogammaglobulinemia were described by RA Good 13 , a condition currently designated as GS. GS is an adult-onset immunodeficiency disease that makes patients more susceptible to bacterial, fungal, and opportunistic infections, and its immunological features include hypogammaglobulinemia and reduced B cells in the peripheral blood 14 . According to the World Health Organization (WHO) system, thymoma A (37.8%) was reported as the most common type of thymoma. The frequencies of other types such as B (all subtypes), AB, and C were reported at 24.3%, 35.1%, and 2.7%, respectively, in 37 sampled patients combined with GS 14 . In this study, three AB thymoma patients had GS, of which one exhibited improved symptoms postoperatively and the total amount and frequency of gamma globulin input were lower than before operation as well. In addition, it is regrettable that the symptoms of the other two patients did not improve significantly.
In our study, one patient combined with anti-AMPA2-R autoimmune encephalitis that had decreased consciousness and memory before operation, and a high amount of glucocorticoid was administered to control the progress of the disease. After operation, the drug was gradually withdrawn, the antibody concentration decreased, and consciousness and memory were restored. In industrialized countries, autoimmune encephalitis is increasingly being recognized as an important and eminently treatable cause of subacute neurologic deterioration, with a prevalence that rivals infectious encephalitis15 –17. Antibodies against the GluA1 or GluA2 subunits of the alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR) have been associated with encephalitis 18 . Laurido-Soto et al reported disease-associated malignancy in 34 cases (62%), with lung carcinoma 19 and thymoma 20 patients dominating the cases.
In addition, three patients were complicated with multiple autoimmune diseases. One patient with polymyositis complicated with xerophthalmia and showed improvement in autoimmune diseases after operation. Besides the withdrawal of high-dose hormone therapy (prednisone 150 mg/day), the symptoms of systemic muscle pain and dry eye disappeared. Two other patients with two autoimmune diseases had no significant improvement in symptoms and laboratory indicators after operation, which also reflected the complexity and diversity of pathogenesis.
The limitations of this study included the following. First, we had a small sample size of 32 patients, which could have led to bias in the results. Second, the study was retrospective making it subject to bias, such as the choice of surgical methods and surgical approaches. However, conducting a prospective clinical study on thymoma is very challenging since these diseases rarely occur in the population. In future, we look forward to including more clinical medical centers in our research, to have a larger sample size that would enable us obtain more meaningful and persuasive results.
Conclusion
In conclusion, this study presents that surgical treatment achieves more satisfactory prognosis for thymoma combined with non-MG autoimmune disease (close to 70% remission rate). Therefore, surgical procedures should be prioritized in the treatment of such medical conditions. Although the number of cases in this study is small, the positive effect of surgery on the treatment of thymoma accompanied with non-MG autoimmune disease was found. Therefore, we propose that the findings of this study can be further validated by constructing a large sample size study of multicenter in the future, and expect its results to benefit more patients.
Footnotes
Acknowledgements
We would like to give our sincere thanks to Professor Hongsheng Liu, Yushang Cui, Naixin Liang, Zhijun Han, and Xiaoyun Zhou for their contributions to their clinical works.
Author Contributions
Shanqing Li contributed to research ideas and design; Lei Liu helped in paper writing and research coordination; Cheng Huang, Yeye Chen, and Chao Guo helped in modification and correction of articles; and Jiaqi Zhang and Guige Wang contributed to data collation, analysis, and postoperative follow-up.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.