
Abstract
Background:
A contralateral occult inguinal hernia is frequently observed in patients planned for a unilateral laparoscopic inguinal hernia repair. Surgical strategy for contralateral groin management in patients scheduled for an endo-laparoscopic unilateral inguinal hernia repair is controversial and based on questionable evidence. This study aimed to gather international opinion concerning the surgical strategy for the contralateral asymptomatic side when no hernia or lipoma is clinically evident at the preoperative examination or anamnesis.
Methods:
An international Internet-based questionnaire was sent to all the members of the European Hernia Society, the Americas Hernia Society, and the Asia Pacific Hernia Society. The clinical scenario for responders was a patient with a unilateral symptomatic inguinal hernia planned for endo-laparoscopic repair with no preoperative symptoms/lump on the contralateral side.
Results:
A total of 640 surgeons replied (response rate = 26%), of whom 506 were included for analysis. Most surgeons had performed > 300 repairs. The preferred surgical technique was evenly distributed between laparoscopic total extraperitoneal repair and laparoscopic transabdominal preperitoneal repair. In total, 54% preferred to implant a prophylactic mesh on the contralateral side when an occult hernia was found, 47% when a lipoma was found, and 6% when no occult hernia/lipoma was identified.
Conclusions:
Mesh implementation was preferred by half of the endo-laparoscopic hernia surgeons for a contralateral occult hernia and/or lipoma. Although not supported by strong evidence, mesh implantation on the asymptomatic contralateral side might be cost-effective and perhaps beneficial in the long term but could be offset by increased risk of chronic pain and sexual dysfunction.
Keywords
Introduction
An occult hernia can be defined as “an asymptomatic hernia not detectable by clinical examination” 1 . The incidence of contralateral occult inguinal hernias reported during total extraperitoneal repair (TEP) or laparoscopic transabdominal preperitoneal repair (TAPP) varies from 5% to 58% and 13% to 22% after TEP and TAPP, respectively1 –5. The incidence of contralateral lipoma is unknown.
Mesh repair of contralateral occult inguinal hernia or a contralateral lipoma (after retraction) is controversial. Bilateral repair may be cost-effective and even clinically beneficial in the long term. However, this practice may be offset by an increased risk of chronic pain and sexual dysfunction/ejaculatory pain.
During a TAPP repair, an assessment of the contralateral groin may be performed under direct visualization without dissection, although some lipomas of the cord may be overlooked 1 . During a TEP repair, a contralateral exploration or a transperitoneal laparoscopy is necessary to identify the presence of occult contralateral hernias and lipomas2,6,7. Currently, no strong evidence supports contralateral exploration during TEP in patients with overt unilateral inguinal hernias although some authors advocate for the opposite 6 .
The decision to implant a “prophylactic” mesh is controversial and, from a critical point of view, not based on solid evidence 1 . However, surgeons’ strategy on this issue is not known. Due to the lack of evidence, more studies within this specific area are required. The primary objective of this study was therefore to analyze surgeons’ preference to implant a contralateral prophylactic mesh for an occult inguinal hernia or contralateral lipoma (after retraction), and the secondary objective was to analyze the strategy in cases of no hernia or after no lipoma retraction defect at all.
Materials and Methods
Settings
The survey was endorsed by the European Hernia Society (EHS), Americas Hernia Society (AHS), and Asia Pacific Hernia Society (APHS) and used the cloud-based platform SurveyMonkey®. To minimize survey response bias, an automatic question logistic was incorporated into the questionnaire setup. Members from the three hernia societies were emailed with a link to the survey platform (see Supplemental Appendix). The EHS surgeons received an email invitation to participate during July 2016, the AHS surgeons during March 2017, and the APHS during December 2017 (thus, the long inclusion period from July 2016–December 2017 reflected differentiated inclusion periods from the three societies). Non-responders were sent a reminder twice with 14-day intervals. If surgeons were members of more than one society (meaning two surveys were sent), only data from the first questionnaire received were included in the analysis. The risk of duplicate responses was minimized by allowing only one answer per email address and IP address. Due to software restrictions and limitations (national firewall), the survey questionnaire did not reach most members from the Peoples Republic of China.
Questionnaire
The accompanying responder-introduction to the questionnaire is shown in Supplemental Appendix. The clinical scenario of a patient with symptomatic overt unilateral inguinal hernia planned for an elective unilateral laparoscopic inguinal hernia repair with no symptoms or bulge on the contralateral side was included in the email to participants. Surgeons who preferred TEP repair were asked if they would perform a contralateral groin exploration during planned unilateral repair (see Supplemental Appendix). The responders were informed not to address an emergency, femoral, or obturator hernia situation. Questions comprised of demographics, surgical experience, and preferences regarding the use of a prophylactic mesh implantation for a contralateral occult hernia and/or a contralateral lipoma without the presence of a hernia, or even systematically in the absence of a hernia or lipoma (see Supplemental Appendix). A contralateral occult hernia was not defined according to the EHS classification and according to retracting of the peritoneum. Respondents were not asked to justify the latter strategy. The survey included questions on preoperative conditions (gender, patient’s smoking, type of work and leisure, sport, and heavy lifting) with potential influence on the surgical decision-making (not shown in Supplemental Appendix).
Statistics
The study was explorative and a pre-study power calculation for sample size was not possible. Data were presented as frequencies, percentage, median and range, and percentage and 95% confidence intervals (95% CI) if not stated otherwise. A chi-square test was used when appropriate.
Results
In total, 2444 (EHS = 957, AHS = 893, and APHS = 594) surveys were mailed and 640 responders (from 55 different countries) returned with answers (response rate = 26%). Thirteen responses were incomplete (missing data), and 121 surgeons did not routinely perform laparoscopic inguinal hernia repair (instead of open repair). The present analysis was therefore based on replies from 506 laparoscopic hernia surgeons.
EHS members contributed with 44% of the responders (95% CI, 40%–49%) (Fig. 1), of which 54% were from Germany (other EHS countries, 1%–7%). From the AHS, the United States contributed 87% of responders (other AHS countries, 1%–3%). From the APHS, India contributed 47% (other APHS countries with 1%–12%). Most of the responders had performed > 300 laparoscopic inguinal hernia repairs and were mainly affiliated to a public healthcare institution. The number of surgeons preferring TEP or TAPP was equally distributed (Fig. 1). Thirty-two percent of the TEP surgeons (26%–37%) would perform a contralateral exploration despite no contralateral bulge or symptoms.
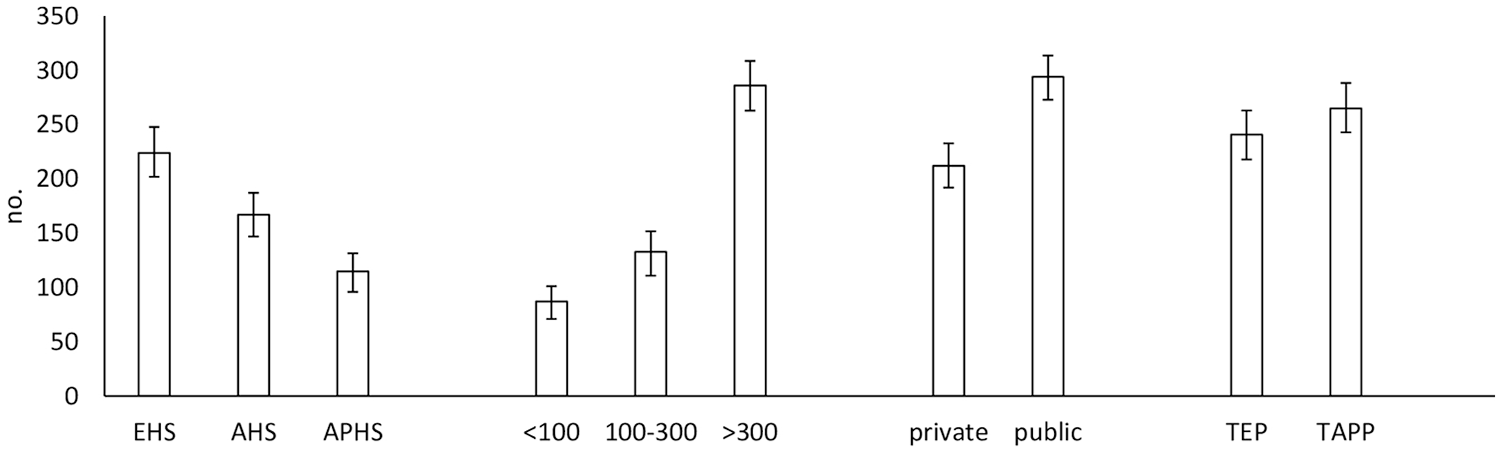
Surgeons’ professional background. Number of respondents according to (1) hernia society (European Hernia Society (EHS), the Americas Hernia Society (AHS), and Asia Pacific Hernia Society (APHS)), (2) total number of laparoscopic inguinal hernia repairs performed by each surgeon (<100 repairs, 100–300 repairs or >300 repairs), (3) responders’ primary affiliation, private or public healthcare institution, and (4) preferred technique for laparoscopic inguinal hernia (total extraperitoneal repair (TEP) or transabdominal preperitoneal repair (TAPP)). Data are indicated by numbers of surgeons and 95% confidence intervals.
Most of the TEP and TAPP surgeons stated that the decision to perform a bilateral mesh implantation, despite a planned unilateral hernia repair, was based on patients’ request and informed consent.
In total, 54% (50%–58%) of the surgeons preferred to implant a contralateral prophylactic mesh for an occult inguinal hernia (27% of TEP and 85% of TAPP surgeons, see Table 1). Only 2% of the responders reported that surgical decision-making was influenced by specific preoperative conditions in male patients and 0.2% (one surgeon) in female patients (physical work, sport, etc., for simplicity conditions, are not shown in the Supplemental Appendix). In patients with coincidental contralateral finding of a lipoma (irrespective of the size), 47% (43%–51%) preferred to implant a prophylactic mesh after lipoma reduction (TEP 29% and TAPP 79%). A comparison of individual hernia societies (EHS vs AHS vs APHS) showed no significant difference in the surgical strategy or between primary affiliation to private or with public healthcare institutions (p = 0.705). Six percent of responders (4%–8%) preferred on a routine basis to implant a prophylactic contralateral mesh even if no contralateral occult hernia or lipoma was evident (Table 1).
Surgical strategy.
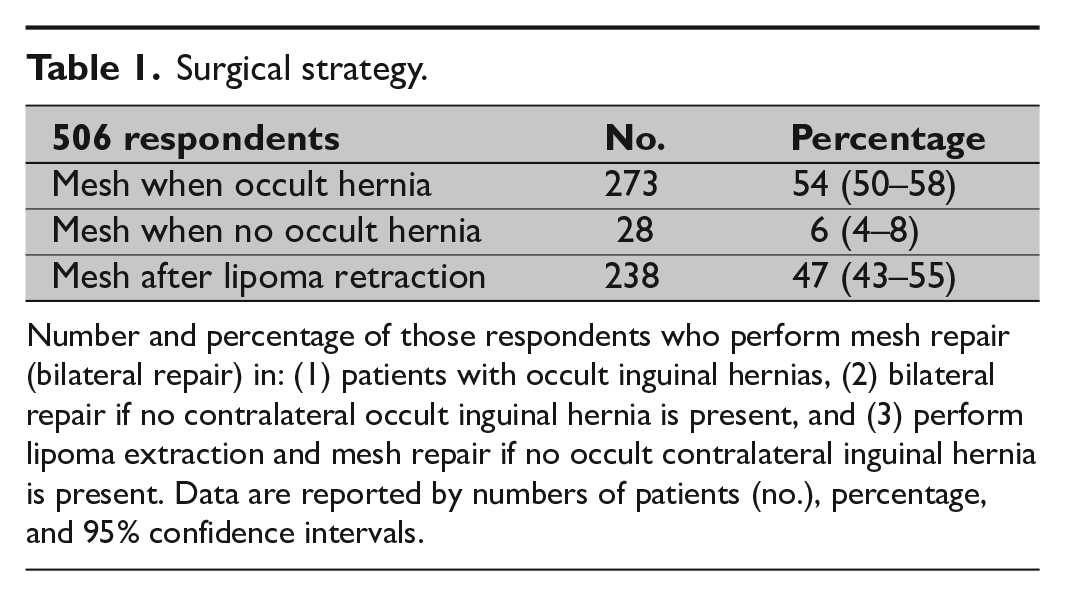
Number and percentage of those respondents who perform mesh repair (bilateral repair) in: (1) patients with occult inguinal hernias, (2) bilateral repair if no contralateral occult inguinal hernia is present, and (3) perform lipoma extraction and mesh repair if no occult contralateral inguinal hernia is present. Data are reported by numbers of patients (no.), percentage, and 95% confidence intervals.
Discussion
The present survey reports on the surgical strategy among international laparoscopic hernia surgeons. Despite limited evidence, half of the responders used on a routine basis prophylactic exploration and mesh implantation in the contralateral groin to repair an occult hernia or following a retraction of an incidental lipoma. Six percent would routinely implant a contralateral prophylactic mesh despite no contralateral inguinal hernia or lipoma.
There are three small studies3 –5 describing planned unilateral TAPP and a strategy to repair an occult hernia on the contralateral side. Unfortunately, the quality of studies was low with no uniform assessment described, poor definition of an occult hernia, and short follow-up. The authors concluded that repair of an occult inguinal hernia seems to be associated with a low rate of morbidity and a contralateral repair was recommended3 –5. In one of these studies 5 , only large defects (hernias which allowed protrusion) on the contralateral side were repaired. A follow-up was undertaken in all patients with small (incipient) hernias. Of the 61 patients with remaining small hernias, 13 became symptomatic during follow-up (9 years). Due to the small number of patients included and imprecise definition of the contralateral inguinal hernia, a recommendation to perform a primary repair of an occult contralateral inguinal hernia at the time of laparoscopic inguinal hernia repair is not possible.
The repair of a primary unilateral inguinal hernia is significantly associated with a subsequent contralateral repair per se although the exact risk is not known 8 . To offer bilateral inguinal hernia repair despite no groin symptoms or lump in the contralateral groin is controversial. Following unilateral endo-laparoscopic repair the risk of disabling chronic pain and sexual dysfunction/ejaculatory pain is probably less than 2%–4%1, 9. Bilateral mesh implantation might be cost-effective and perhaps beneficial in the long term (one operation, one recovery), but there may be an increased risk of chronic pain (up to 15%) 10 . There are no data in the literature comparing chronic pain after unilateral versus bilateral endo-laparoscopic repair. One controlled register-based follow-up study comparing unilateral TAPP versus bilateral TAPP (n = 1172 patients) found no difference in risk of pain during sexual activity after unilateral compared with bilateral repair 9 .
During a TEP procedure, despite the lack of convincing data, recent international guidelines 1 do not recommend dissection (weak guideline recommendation) of the contralateral groin to allow inspection of a possible occult hernia or presence of an incidental lipoma. Nor does it recommend routine contralateral and mesh implantation in patients planned for overt unilateral inguinal hernia repair 1 . A recent study from the German HerniaMed Registry has shown a significantly lower rate of some early postoperative complications (postoperative ileus and risk of reoperation) after, respectively, unilateral compared with bilateral TAPP. The difference disappeared when comparing only high-volume expert centers. Other complications such as the risk of bleeding, intestinal lesion, seroma, infection, and impaired wound healing did not significantly differ 11 . Furthermore, it may be speculated that mobilization of a normal side or a small (incipient) occult hernia may be technically easier than when a clinical hernia is present, and thus associated with lower morbidity compared with bilateral procedures for clinically apparent, bilateral hernia.
The present survey has limitations. The low response rate of 26% may increase the risk of selection bias, reflecting that responses were dominated by an enthusiastic academic hernia and key opinion-leading surgeons rather than responses from everyday hernia-interested surgeons (external validity). However, the study was performed among international surgeons from three international hernia societies, which may strengthen the external validity of the study. Also, and hypothetically, the weak definition of an occult hernia (no EHS classification and whether the contralateral occult hernia was based on retracting the peritoneum or not) may have biased the results from the questionnaire answers.
A future randomized controlled trial comparing prophylactic mesh implantation to no mesh in patients having no hernia or an occult asymptomatic hernia or an incidental lipoma on the contralateral side at perioperative inspection would provide high-evidence data for surgical strategy guidance. A hypothesis on a clinically relevant outcome would need to be defined before a future study could be initiated, and a follow-up of at least 10 years may also be difficult to complete.
Conclusion
In conclusion, half of the dedicated laparoscopic hernia surgeons suggested using a mesh in patients scheduled for an endo-laparoscopic unilateral inguinal hernia repair with a contralateral occult inguinal hernia and/or following reduction of an incidental lipoma. Evidence for the optimal surgical strategy in this clinical scenario remains much to be desired.
Supplemental Material
sj-pdf-1-sjs-10.1177_1457496920938600 – Supplemental material for Surgical Strategy for Contralateral Groin Management in Patients Scheduled for Unilateral Inguinal Hernia Repair: An International Web-Based Surveymonkey® Questionnaire: Strategy for Contralateral Groin Management during Inguinal Hernia Repair
Supplemental material, sj-pdf-1-sjs-10.1177_1457496920938600 for Surgical Strategy for Contralateral Groin Management in Patients Scheduled for Unilateral Inguinal Hernia Repair: An International Web-Based Surveymonkey® Questionnaire: Strategy for Contralateral Groin Management during Inguinal Hernia Repair by Niels Johansen, Marc Miserez, Andrew de Beaux, Agneta Montgomery, Jose Macario Faylona, Alfredo Carbonell and Thue Bisgaard in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We thank the members of the EHS, AHS, and APHS for their time for answering the questionnaire and the societies for endorsement and technical support.
Author Contributions
N.J., M.M., A.d.B., A.M., J.M.F., A.C., and T.B. contributed to study conception and design. N.J. contributed to acquisition of data. N.J. and T.B. contributed to analysis and interpretation of data. N.J. and T.B. contributed to drafting of the manuscript. N.J., M.M., A.d.B., A.M., J.M.F., A.C., and T.B. contributed to critical revision of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.