
Abstract
Background:
The trend in liver trauma management has progressively become increasingly conservative. However, a vast majority of literature focuses heavily on the management of blunt trauma. This study reviews the management of hepatic trauma at a major trauma center in a developing world setting, in order to compare blunt and penetrating liver trauma and to define current management algorithms and protocols.
Methods:
All patients who sustained liver trauma between 2012 to 2018 were identified in the Hybrid Electronic Medical Registry and extracted for further analysis.
Results:
A total of 808 patients with hepatic trauma were managed by our trauma center. There were 658 males and 150 females. The mean age was 30 years (standard deviation 13.3). A total of 68 patients died (8.2%) and a total of 290 (35%) patients required intensive care unit admission. The mean presenting shock index was 0.806 (standard deviation 0.67–1.0), the median Injury Severity Score was 18 (interquartile range 10–25) and the mean Revised Trauma Score was 12 (standard deviation 11–12). There were 367 penetrating and 441 blunt liver injuries. The age distribution was similar in both groups. There were significantly less females in the penetrating group. The shock index and the Injury Severity Score on presentation were significantly worse in the blunt group, respectively: 0.891 (standard deviation 0.31) versus 0.845 (standard deviation 0.69) (p < 0.001) and score 21 (interquartile range 13–27) versus 16 (interquartile range 9–20) (p < 0.01). The opposite applied to the Revised Trauma Score of 11.75 (standard deviation 0.74) versus 11.19 (standard deviation 1.3) (p < 0.001). There were significantly more associated intra-abdominal injuries in the penetrating group than the blunt group, in particular that of hollow organs, and 84% of patients with a penetrating injury underwent a laparotomy while only 33% of the blunt injuries underwent a laparotomy. The mortality rate was comparable between both groups.
Conclusion:
Hepatic trauma is still associated with a high morbidity rate, although there have been dramatic improvements in mortality rates over the last three decades. The mortality rates for blunt and penetrating liver trauma are now similar. Non-operative management is feasible for over two-thirds of blunt injuries and for just under 20% of penetrating injuries.
Introduction
The trend in management of liver trauma over the last 50 years has progressively been toward a more conservative approach. Most authorities advocate a selective non-operative approach, and if operation is required, most suggest that a minimalistic strategy should be adopted (1). Usually, this implies that complex liver resections must be eschewed in favor of non-resection-based techniques to control hemorrhage. These techniques are well within the skill set of most general surgeons and usually involve liver packing or suturing (2). However, a vast majority of the literature on hepatic trauma focuses heavily on the management of blunt trauma. In this setting, the focus is mostly on resuscitation and early imaging with computed tomography (CT). If the patient can be stabilized, then most authors suggest that most blunt liver injuries can be treated expectantly (1–3). The liver is also vulnerable to penetrating injuries, and this mechanism presents a different spectrum of challenges to patients with blunt hepatic trauma. The liver injury itself may not be the primary concern and other intra-abdominal injuries may mandate operative exploration (4, 5). Previously, blunt hepatic trauma was associated with a much higher mortality rate than penetrating liver trauma. Since those early reports, there has been widespread adoption of damage control approaches. This study reviews our cumulative experience with the management of hepatic trauma at a major trauma center in a developing world setting. We aimed to compare blunt and penetrating liver trauma in order to define our management algorithms and protocols and to see if the widespread adoption of damage control approaches had impacted on the outcome of blunt and penetrating liver trauma.
Materials and Methods
Clinical Setting
The Pietermaritzburg Metropolitan Trauma Service (PMTS), a division within the Department of Surgery at Grey’s Hospital, is based in the city of Pietermaritzburg, South Africa. It provides definitive trauma care to the city of Pietermaritzburg and the surrounding catchment area with a total population of over 4 million. Annual admission to our trauma center exceeds 4000 cases and over 50% are penetrating trauma. The PMTS is the largest academic trauma service in western Kwa Zulu-Natal (KZN) Province and is a major teaching hospital of the University of KwaZulu-Natal. It is responsible for undergraduate, postgraduate, and subspecialist fellowship training for trauma surgery for both local and international doctors. Over 5 years from December 2012–December 2017, the PMTS admitted 5027 patients following blunt trauma and 3334 patients with penetrating injuries. There were 2201 stab wounds (SWs) and 1028 gunshot wounds (GSWs). We performed a total of 1075 laparotomies for abdominal trauma. This is an average of 215 trauma laparotomies annually. The PMTS maintains a regional electronic trauma database called the Hybrid Electronic Medical Registry (HEMR), which captures data on all admissions to our trauma center. Ethics approval for the maintenance of our registry and for this study was formally approved by the Biomedical Research Ethics Committee of the University of Kwa Zulu-Natal (reference number: BCA 207/09 and BCA 221/13).
The Study
The HEMR was reviewed for the time period December 2012 and December 2018, and all patients with a hepatic injury were identified for review. Basic demographic data were documented along with the mechanism and the severity of the injury. Once the entire cohort had been classified and analyzed, the total group was broken down into blunt and penetrating mechanisms for comparison. All injuries were graded according to the American Association for the Surgery of Trauma (AAST) grading system using either operative data or CT scan image or both.
Statistical Analysis
Statistical analysis was performed using the chi-square test for categorical variables and two-sided Fisher’s exact for expected cell count less than five. Independent t-test and Mann–Whitney U-test were used for continuous variables. The association between AAST and grouping variables, was assessed by means of logistic regression. AAST 1 was chosen as reference category. For normally distributed data the mean and standard deviation (SD) were calculated. For not normally distributed data, the median and interquartile range (IQR) were reported. A value of p < 0.05 was considered to be statistically significant. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS®, Version 24, IBM Corporation, Armonk, New York, USA).
Results
Demographics
For the 6-year period under review, a total of 808 patients with hepatic trauma were managed by our trauma center. There were 658 males and 140 females. The mean age was 30 years (SD 13.3).
Spectrum of Injury
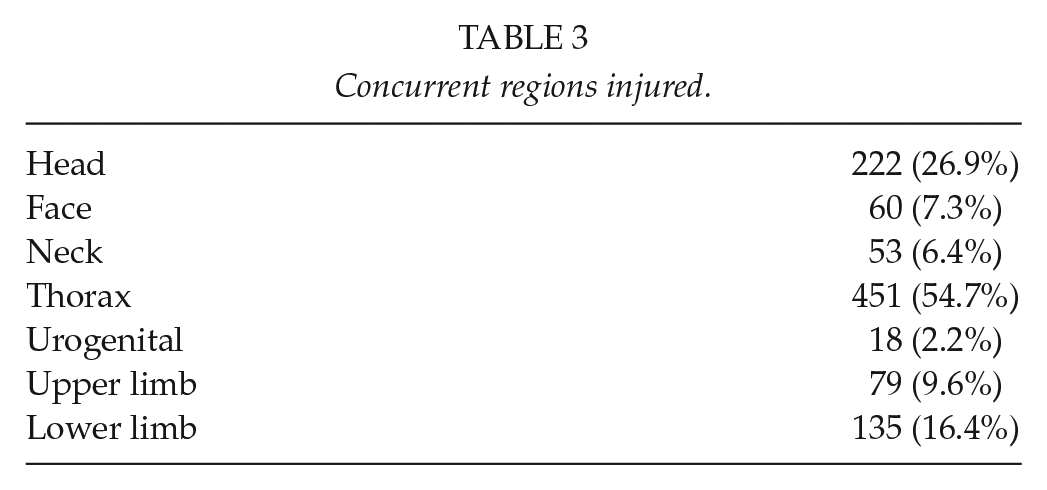
There were 367 patients with penetrating injuries and 441 with blunt injuries. The mean shock index on presentation was 0.806 (SD 0.67–1.0) and the median Injury Severity Score (ISS) on presentation was 18 (IQR 10–25) (Table 1). The mean Revised Trauma Score (RTS) was 12 (11–12). Of the penetrating injuries, 168 were GSWs and 196 SWs. Of the blunt injuries, there were 209 motor vehicle accidents (MVAs) and 148 pedestrian vehicle accidents (PVAs). There were also 51 assaults, 21 falls from a height, 10 heavy objects falling on a patient, and 2 animal-related injuries. The imaging modalities used are shown in Table 2. There were 222 concurrent head injuries, 60 facial injuries, 53 neck injuries, 451 thoracic injuries, 18 urogenital injuries 79 upper limb injuries, and 135 lower limb injuries (see Table 3). In 661 patients, accurate grading of the liver injury was possible. The spectrum of the grade of liver injury is shown in Table 4 and Graph 1.
Demographics and trauma scores.
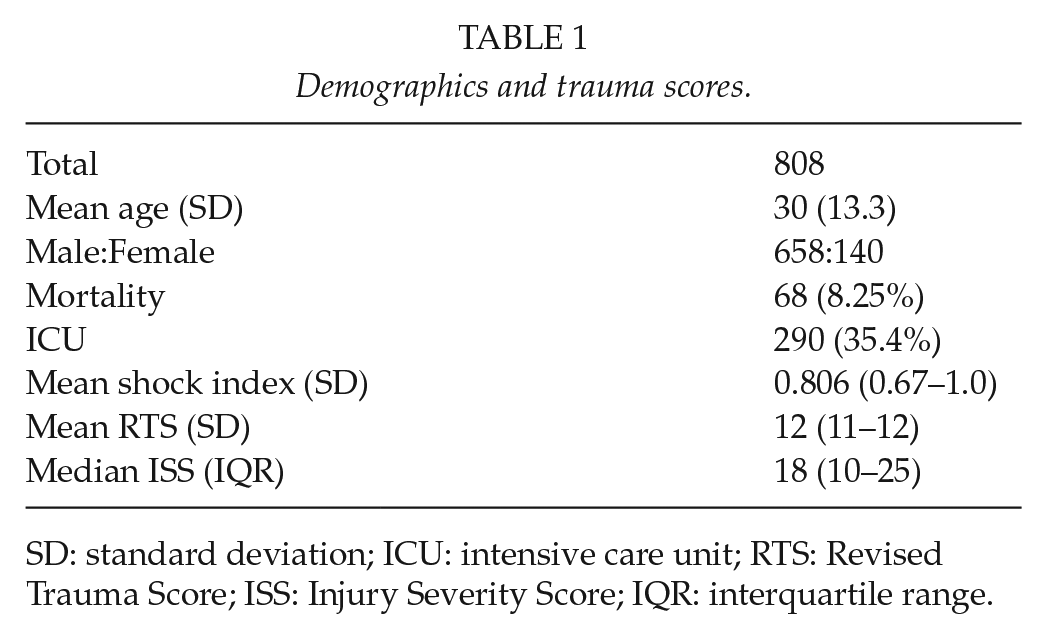
SD: standard deviation; ICU: intensive care unit; RTS: Revised Trauma Score; ISS: Injury Severity Score; IQR: interquartile range.
Imaging modalities.
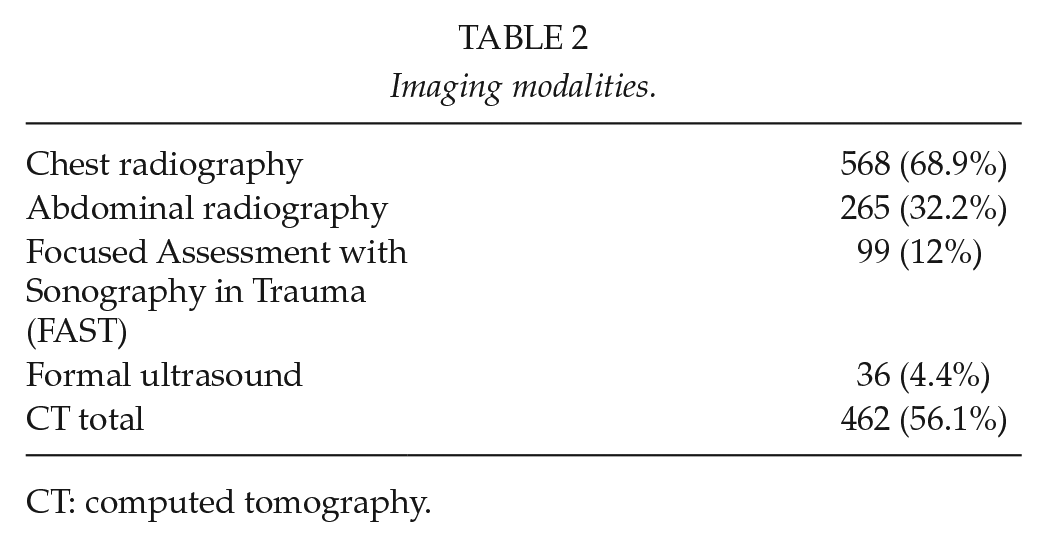
CT: computed tomography.
Concurrent regions injured.
AAST classification versus need for ICU and mortality.
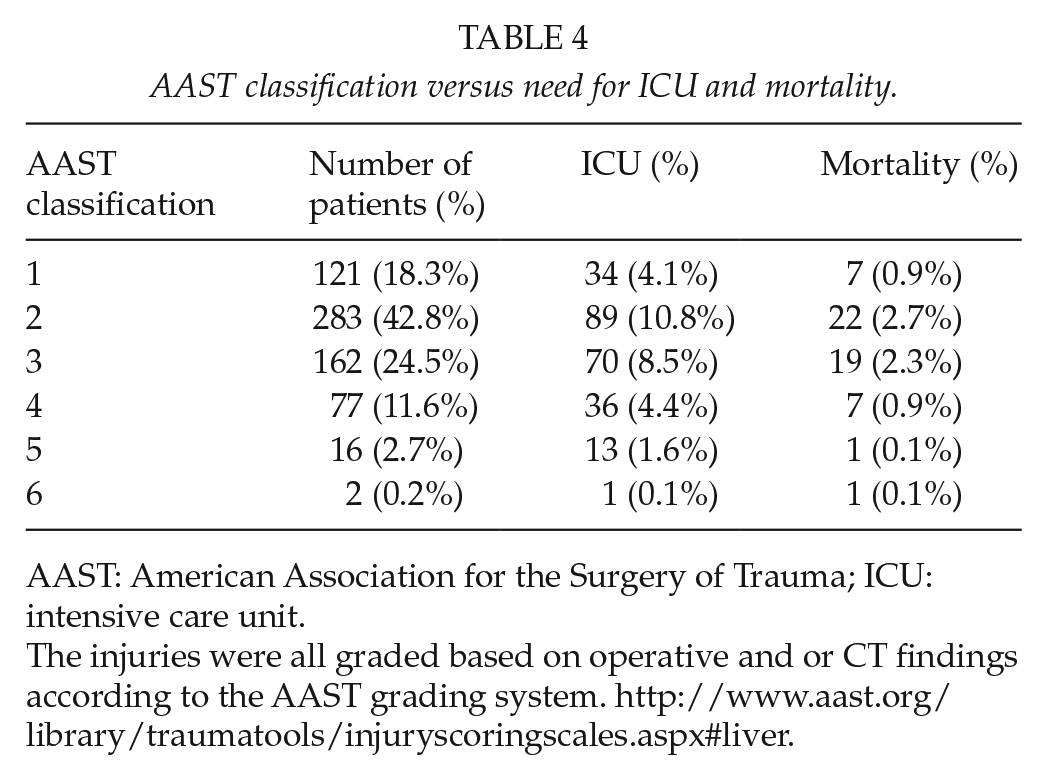
AAST: American Association for the Surgery of Trauma; ICU: intensive care unit.
The injuries were all graded based on operative and or CT findings according to the AAST grading system. http://www.aast.org/library/traumatools/injuryscoringscales.aspx#liver.
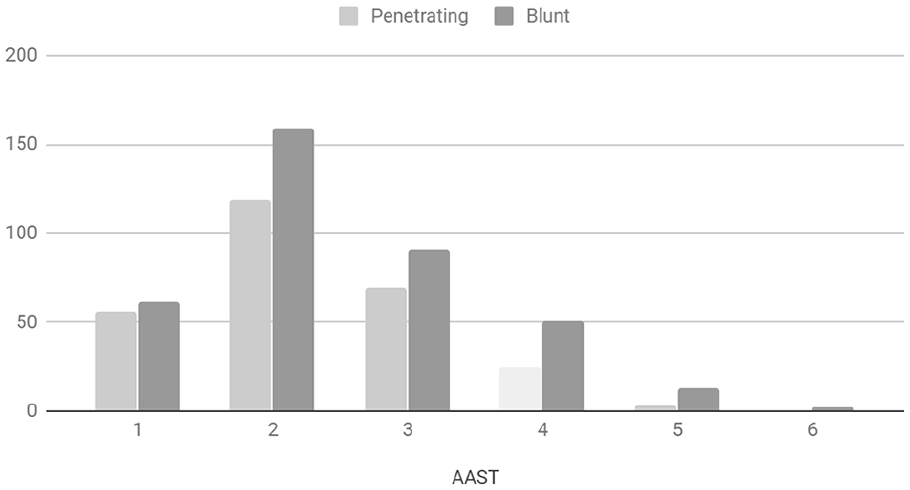
Number of patients per AAST classification.
Management and Outcome
A total of 422 patients underwent an index laparotomy, of which 86 required one or more repeat laparotomies. A total of 386 patients were treated initially conservatively of which 23 (5%) ultimately required an operation. Of these delayed operations, 17 were laparoscopies and 6 laparotomies. A total of 283 (35%) patients required intensive care unit (ICU) admission. The overall rate for non-operative management was 44% (363/808). The need for ICU admission increased dramatically as AAST grade increased (Table 4). Morbidities were recorded in 454 (55%) of patients. However, there was no significant difference in mortality rate between the different AAST grades. A total of 68 patients died (8.25%). Of the operative cohort, the mortality rate was 10% (46/445) and of the initial non-operative group the mortality rate was 5% (22/402).
Blunt Versus Penetrating Trauma
A detailed comparison of blunt liver injuries and penetrating liver injuries was undertaken (Table 5). There were 367 penetrating and 441 blunt liver injuries. The age distribution was similar in both groups; however, the blunt group had significantly more females than the penetrating group. The shock index on presentation and the ISS were significantly worse in the blunt group. The opposite applied to the RTS. There were 66/441 (14%) high-grade liver injuries defined as AAST Grade 3 or greater, in the blunt cohort compared to 25/367 (7%) in the penetrating group. There were significantly more associated intra-abdominal injuries in the penetrating group than in the blunt group. In particular, the diaphragm was most often injured in the penetrating group (n = 106 vs n = 12). The stomach, the large and small bowel as well as the duodenum were also statistically more frequently injured in the penetrating than in the blunt group. The structures most often injured in the blunt group were the kidney and the spleen. Of the patients with a penetrating injury, 84% underwent a laparotomy while only 33% of the patients with blunt injuries underwent surgery. The operative procedures included packing, suturing, resection, and drainage. In 30 patients, the abdomen could not undergo primary closure. These procedures were comparable in both groups except packing which was significantly higher in the blunt group. The intensive care admission rate was higher in the blunt group 38% versus 31%. The mortality and morbidity rates were comparable in both cohorts.
Comparison of penetrating and blunt liver trauma.
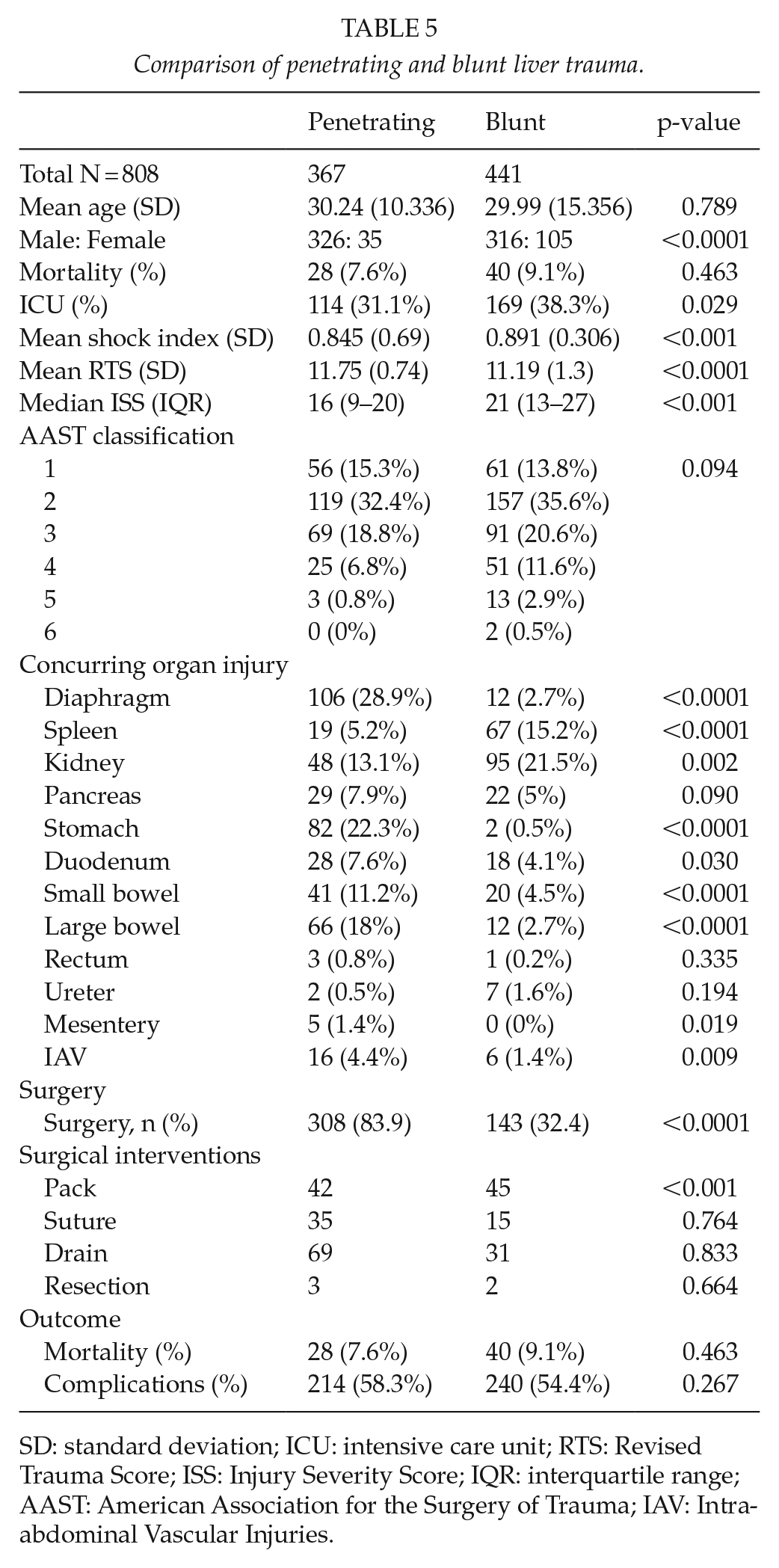
SD: standard deviation; ICU: intensive care unit; RTS: Revised Trauma Score; ISS: Injury Severity Score; IQR: interquartile range; AAST: American Association for the Surgery of Trauma; IAV: Intra-abdominal Vascular Injuries.
Discussion
Blunt hepatic trauma is the prototypical example of both selective non-operative management (SNOM) of blunt abdominal trauma and of damage control surgery (DCS) (1, 6). The widespread availability of accurate CT assessment and grading of liver injuries following blunt abdominal trauma have facilitated a selective non-operative strategy. Almost all patients with blunt liver trauma in our series underwent a CT scan. This allowed for accurate staging of the liver injury and facilitated clinical decision-making. Only one-third of all patients with a blunt injury to the liver in our series required surgery. If surgery is necessary for blunt hepatic trauma, then the most common operative approach is to pack the liver. This is reflected in our series as the most common operative technique used in blunt liver trauma was peri-hepatic packing (9). Of note is the emerging role of laparoscopy for patients who fail non-operative management. Laparoscopy allows the liver injury to be directly visualized and allows for collections of bile and blood to be aspirated.
With penetrating abdominal trauma, the potential for injuries remote from the liver may necessitate laparotomy (4, 5, 7). This is the case in our data where the number of associated injuries was far greater in the penetrating group than in the blunt cohort. The fact that the need for liver packing was much higher in the blunt operative group suggests that the reason for laparotomy in the blunt group was mostly the liver injury in its own right. In the penetrating group, frequently remote injuries mandated the operation and hence the need for liver packing was much lower. The decision to operate on patients with penetrating abdominal SWs is generally made without recourse to imaging. This means that it is difficult to provide a true value for how many SWs of the liver are treated non-operatively. In many cases, patients with an abdominal SW are observed and not imaged or operated on. In these cases, it is impossible diagnose or to classify and grade a possible liver injury. There is a role for non-operative management of penetrating liver trauma, and this was first described by Muckart et al. (8) and was taken forward by Demetriades who showed that in isolated GSW of the liver non-operative management was safe and effective. A contrast-enhanced abdominal CT scan is mandatory to exclude any associated injury which would mandate operation (9-14). We managed to treat penetrating liver trauma non-operatively in just under 17% of patients. The operative management of penetrating liver trauma follows the same principles as that for blunt trauma and minimalistic approaches are advocated (1,2). These include packing the liver and suturing of visible bleeding. The rate of resection was low in both the penetrating and the blunt cohorts.
We have successfully applied the lessons of the last two decades in our setting with an overall rate of non-operative management (NOM) of 43% and a rate of failed NOM of 6% (23) failed. Of note, when NOM failed, most of the patients were managed by laparoscopy (17). Laparoscopy can directly visualize the liver injury, and be used to aspirate the collection of bile and/or blood which has accumulated from the injury. Selective embolization is a useful adjunct, and we made use of this in three patients to deal with ongoing liver bleeding. CT scan will identify extravasation of contrast, and if this is shown, then we proceed to formal angiography and selective arterial embolization as required.
We appear to have improved outcomes for liver trauma. In a large series of 446 patients from Krige et al. (2) over two decades ago, the mortality rate for blunt liver trauma was much higher than for penetrating liver trauma (blunt 27% vs penetrating 5%). The authors pointed out that centers with a preponderance of blunt hepatic trauma over penetrating trauma, at the time, all reported significantly higher mortality rates. The increased application of and familiarity with non-operative management of liver trauma over the last 20 years seems to have impacted on this, and a more recent publication from Cape Town states a mortality rate for blunt liver injury of 5%. In our study, the mortality rate was similar in the blunt and penetrating groups (blunt 9.1% vs penetrating 7.6%), and this is much lower than that reported 20 years ago. Fig. 1 attempts to provide an overview of our approach to hepatic trauma in Pietermaritzburg.
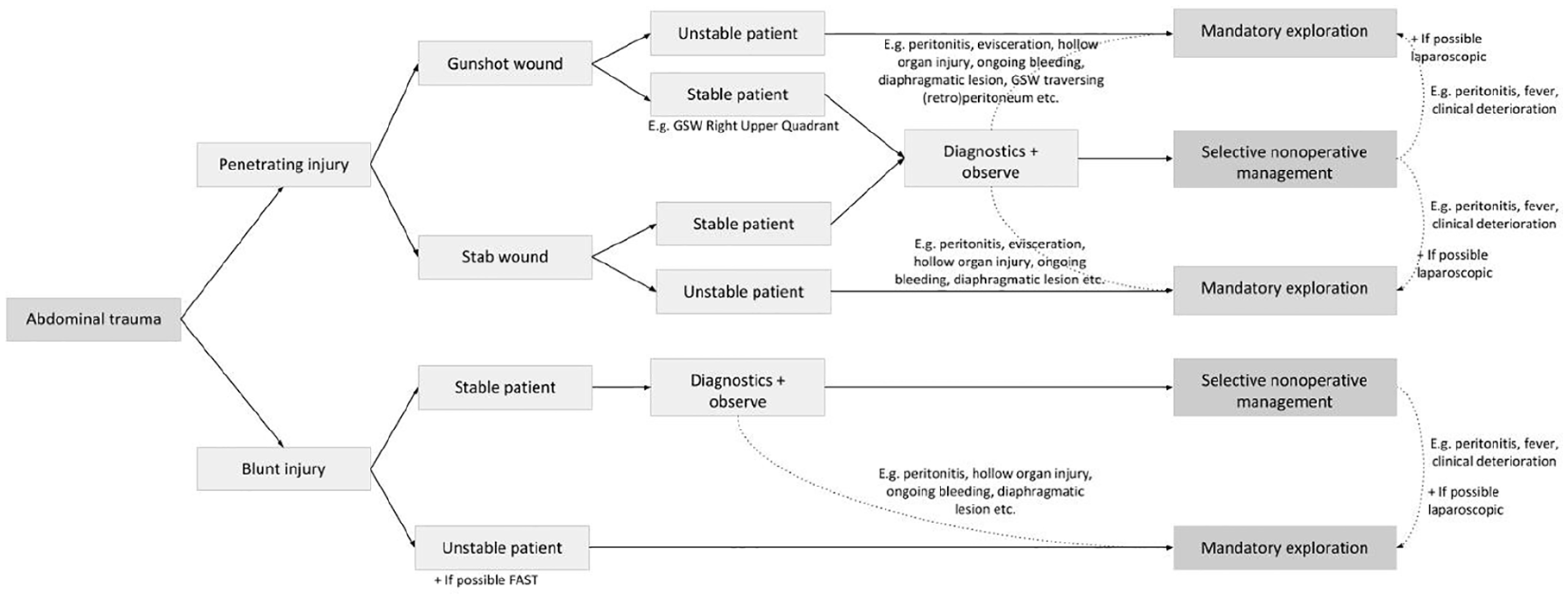
The PMB approach to liver trauma.
This article has a number of limitations despite the use of an electronic prospective data capture system. Missing data are always a problem in such systems, and retrospective review means that it is difficult to extract key data around the actual clinical decision-making. One also needs to bear in mind the fact that many patients may have been operated on for concurrent injuries to which the liver injury itself was incidental. This is especially the case with penetrating trauma. In addition, patients with relatively mild liver injuries may have required ICU or died as a result of other major remote thoracic and neurological injuries.
Conclusion
Hepatic trauma is still associated with a high morbidity rate, although there have been dramatic improvements in mortality rates over the last three decades. The mortality rates for blunt and penetrating liver trauma are similar. NOM is feasible for over two-thirds of blunt injuries and for just under 20% of penetrating injuries.
Footnotes
Author’s Note
R.Hoencamp is also affiliated with Trauma Research Unit, Department of Trauma Surgery, University Medical Center Rotterdam, Erasmus, MC, Rotterdam, the Netherlands
Declaration of Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.