
Abstract
Objectives:
To compare the standard percutaneous nephrolithotomy and mini-percutaneous nephrolithotomy in order to determine the optimal tract size for patients with renal stones.
Methods:
A systematic search of Web of Science, EMBASE, Cochrane Library, and PubMed databases was conducted for articles published through 20 August 2019, reporting on a comparison of the standard percutaneous nephrolithotomy and mini-percutaneous nephrolithotomy using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results:
Of 763 studies, 14 were considered for the evidence synthesis. A total of 1980 cases were included. Of these patients, 897 cases underwent standard percutaneous nephrolithotomy, and 1083 cases underwent mini-percutaneous nephrolithotomy. Stone-free rates were 87.6% (786 of 897 patients) for standard percutaneous nephrolithotomy and 87.8% (951 of 1083 patients) for mini-percutaneous nephrolithotomy (p = 0.57). Tract sizes of 30F and 22–26F in standard percutaneous nephrolithotomy group shorten operation time compared with mini-percutaneous nephrolithotomy (p = 0.02; p = 0.004; respectively). Leakage (p = 0.04), bleeding (p = 0.01), blood transfusion (p < 0.00001), and renal pelvis perforation (p = 0.02) were more common in standard percutaneous nephrolithotomy group than in mini-percutaneous nephrolithotomy group. Subgroup analysis showed only blood transfusion for 30F and 22–26F standard percutaneous nephrolithotomy group was more common than mini-percutaneous nephrolithotomy (p < 0.0001, p = 0.005, respectively).
Conclusions:
Standard percutaneous nephrolithotomy was associated with higher leakage, bleeding, blood transfusion, and renal pelvis perforation, but had a shorter operation time. Tract size of 30F improved the stone-free rate compared with mini-percutaneous nephrolithotomy, but led to more complications. Tract size of 22–26F was no better than 30F or mini-percutaneous nephrolithotomy.
Keywords
Introduction
Mini-percutaneous nephrolithotomy is considered minimally invasive than standard percutaneous nephrolithotomy (PCNL). Several meta-analyses have compared the stone-free rate (SFR), operative time, and complications between mini-PCNL and standard PCNL 1,2. These meta-analyses consistently indicated that mini-PCNL was a safe and effective procedure with an SFR comparable with that of standard PCNL. Mini-PCNL also resulted in less complications, less pain, and shorter hospitalization. Standard PCNL was superior in terms of shorter operating duration 1,2. Limitations were noted in these meta-analyses. Most of the studies were nonrandomized comparisons and heterogeneity among studies was found to be high for several parameters
2
. The use of different tract sizes (14
There were many high-quality researches focusing on the issue since last meta-analysis 10 –16. Most of these were randomized trials 10,12 –16. Therefore, we performed the meta-analysis to update the outcomes of comparison between standard and mini-PCNL. Subgroup analyses were performed according to study design, stone size, stone number, and especially tract size. Subgroup analyses for variable complications were also performed.
Materials and Methods
Search Strategy
The meta-analysis and systemic review were performed by searching the Web of Science, PubMed, Cochrane Library, and EMBASE databases for studies published through 20 August 2019. Additional records were identified through searchers of other sources (by screening the reference in the identified studies). Search details were “‘standard’[All Fields] OR ‘mini’[All Fields] OR ‘micro’[All Fields] AND ‘Percutaneous Nephrolithotomy’[All Fields] OR ‘PCNL’[All Fields] AND ‘renal stone’[All Fields] OR ‘ureter stone’[All Fields].” Searches were restricted to publications in English. In addition, we also manually searched the identified articles and references in the system review to find more references.
Inclusion and Exclusion Criteria
Two investigators (J.D. and L.W.W.) independently extracted the data, and an agreement was reached by discussion. Studies that met the following criteria were included: (a) compared standard PCNL and mini-PCNL and (b) sufficient data that were reported or could be calculated (including the study design, population characteristics, surgical instruments, surgical techniques, SFR, operation time, and complications). Major exclusion criteria were (a) incomplete data for the analysis; (b) conference abstracts, reviews, letters to editors/commentaries/editorials, and articles cannot be translated into English; (c) pediatric patients under 18 years old; (d) ultra-mini-PCNL (<12F); and (e) duplicate data.
Data Extraction
The primary outcomes were the operation time and SFR. The secondary outcomes were bleeding, renal pelvis (RP) perforation, and other complications. Authors’ names, publication year, study design, patient number, stone size, tract size, operation time, complications, and SFR of each comparison were collected from the included publication. Complications included leakage (conservative), bleeding, blood transfusion, fever and urinary tract infection (UTI), RP perforation, calcular obstruction (ureteroscope, URS), leakage (JJ insertion), pneumothorax, and hematoma (embolization).
Assessment of Study Quality
The level of evidence (LE) was rated for each included study according to the criteria provided by the Oxford Centre for Evidence-Based Medicine 17 . The methodological quality of the studies was assessed using the Newcastle–Ottawa Scale (NOS) for non–randomized controlled trials (RCTs) 18 and the Jadad scale for RCTs 19 . Two reviewers reviewed the full texts of the included studies. Preoperative demographic characteristics as well as perioperative and postoperative outcomes between the two procedures were compared.
Statistical Analysis
The heterogeneity of the studies was evaluated using I 2 statistics 20 . We pooled the information with a random or fixed-effect model according to the p value. The fixed-effects model method was used when p > 0.1, indicating a lack of heterogeneity among studies. When heterogeneity was observed, the random-effects model was applied 21 . Publication bias was evaluated using Begg’s and Egger’s tests. A sensitivity analysis was performed to assess the stability of the results. Funnel plots were drawn to estimate publication bias, and the symmetry of the funnel plot was assessed using Egger’s test 22,23. When using Egger’s test to assess the publication bias, p < 0.05 indicated statistically significant publication bias. The statistical analysis was performed using STATA 12.0 software (StataCorp., College Station, TX, USA).
Results
Study Selection and Characteristics
A total of 756 potentially relevant studies were identified through the literature search. Seven other studies were added through searches of other sources (by screening the references of the identified studies). Four hundred sixty three records were screened after removing duplicates. After excluding 390 unrelated articles, 73 articles were further assessed. Finally, 14 studies met the inclusion criteria and were included in our meta-analysis 3 –16 (Fig. 1). A total of 893 patients with 897 renal units received standard PCNL, and 1080 patients with 1083 renal units undergoing mini-PCNL. Nine RCTs (LE:2b) 4,5,8,10,12 –16 and five non-RCTs (LE:3b) 3,6,7,9,11 were included in the study. The methodological quality of included studies was relatively high for two of the non-randomized studies (NOS: 6 of 9 points) 6,11 and medium for three (NOS: 5 of 9 points, 5 of 9 points, and 4 of 9 points) 3,7,9, whereas the nine RCTs were medium quality (Jadad scale: 3 of 5 points) 4,5,8,10,12 –16. Some studies compared the outcome of mini-PCNL versus standard PCNL for stone size >2 cm 5,9,16, some for stone size <2 cm 3,4,10,13,14. Characteristics for included studies are shown in Table 1. Surgical technique for PCNL varied in terms of image guidance, access, use of flexible nephroscopy, and type of lithotripsy (Table 2).
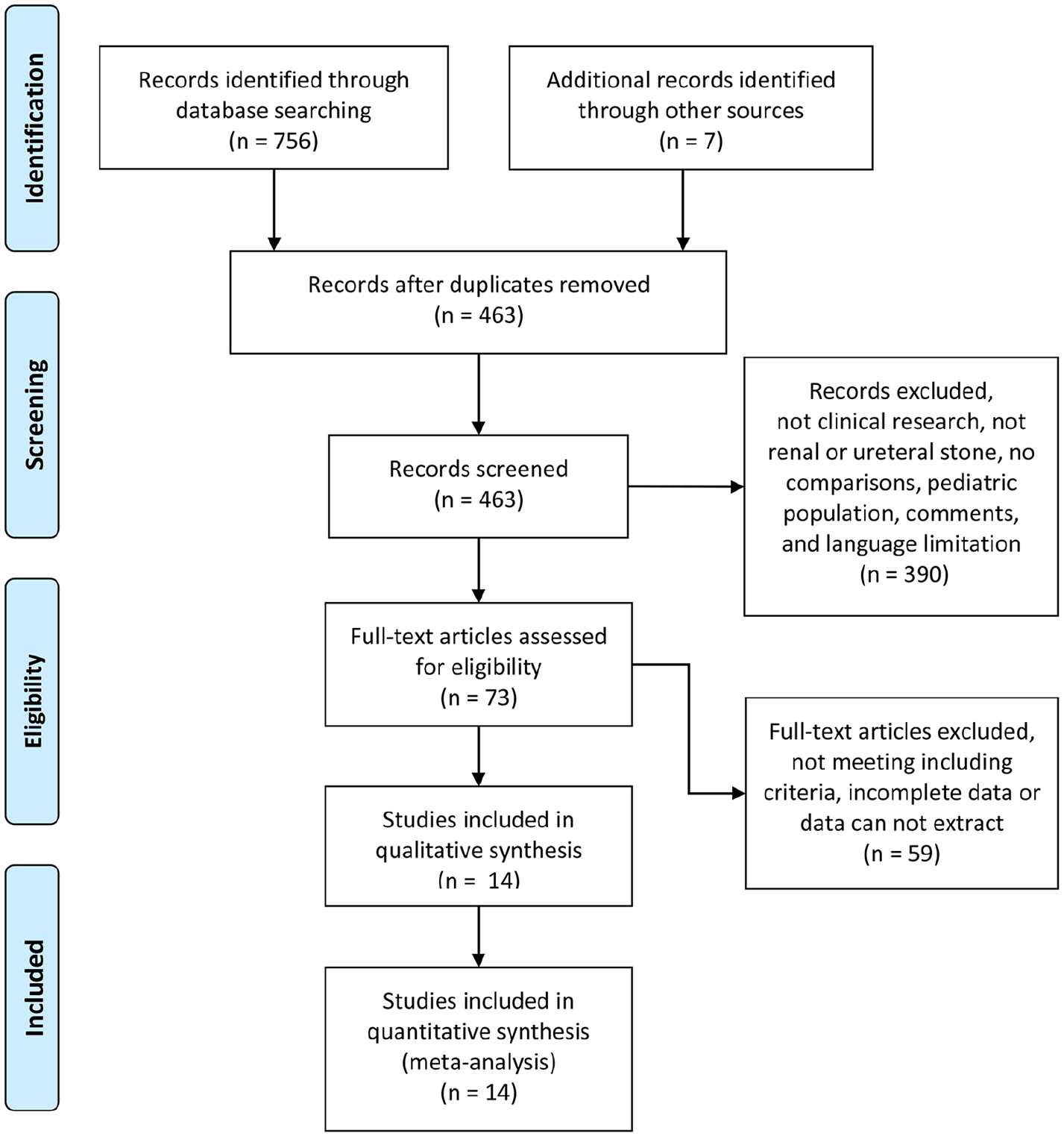
Flow diagram of the details of the study.
Characteristic for included studies.
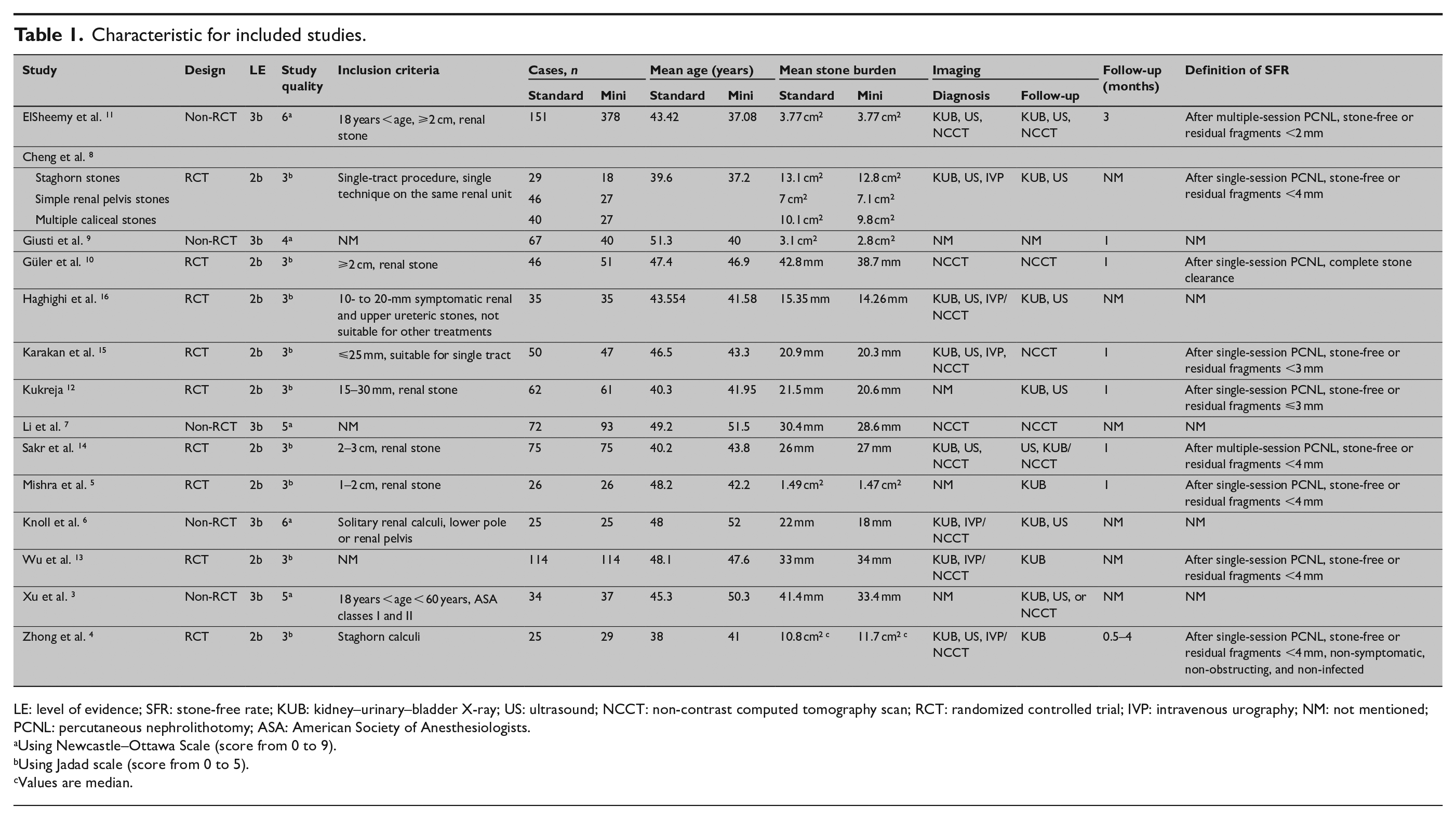
LE: level of evidence; SFR: stone-free rate; KUB: kidney–urinary–bladder X-ray; US: ultrasound; NCCT: non-contrast computed tomography scan; RCT: randomized controlled trial; IVP: intravenous urography; NM: not mentioned; PCNL: percutaneous nephrolithotomy; ASA: American Society of Anesthesiologists.
Using Newcastle–Ottawa Scale (score from 0 to 9).
Using Jadad scale (score from 0 to 5).
Values are median.
Variations in standard and mini-PCNL techniques, as stated in the “Methods” section: an overview.
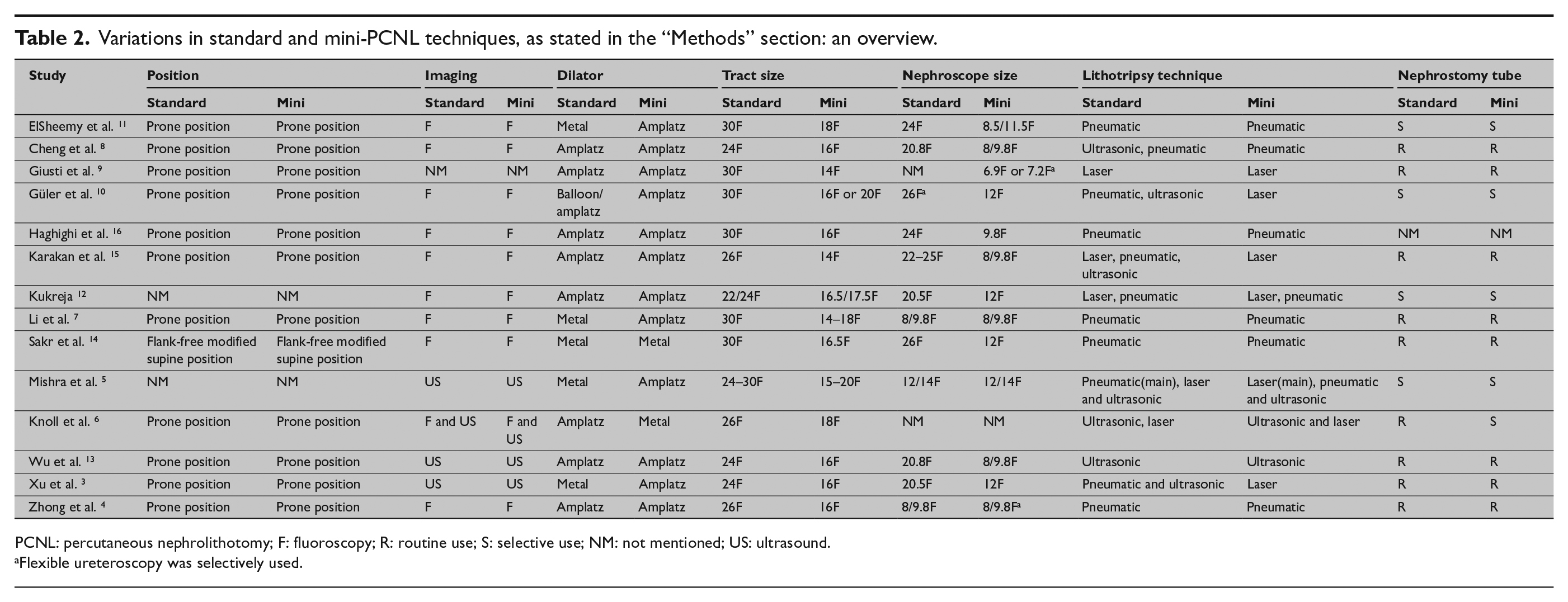
PCNL: percutaneous nephrolithotomy; F: fluoroscopy; R: routine use; S: selective use; NM: not mentioned; US: ultrasound.
Flexible ureteroscopy was selectively used.
Sfr and Subgroup Analysis
SFR was 87.6% (786 of 897 patients) for standard PCNL and 87.8% (951 of 1083 patients) for mini-PCNL (odds ratio (OR) = 1.08, 95% confidence interval (CI): 0.82–1.44, p = 0.57; Fig. 2). For RCT studies, SFR was 84.9% (465 of 548 patients) for standard PCNL and 88.0% (449 of 510 patients) for mini-PCNL (OR = 0.76, 95% CI: 0.53–1.10, p = 0.15; Fig. 2). For non-RCT studies 3,6,7,9,11, SFR was 92.0% (321 of 349 patients) for standard PCNL and 87.6% (502 of 573 patients) for mini-PCNL (OR = 1.91, 95% CI: 1.18–3.08, p = 0.008; Fig. 2). When stratified according to stone type, SFR was not statistically different between standard and mini-PCNL for single (OR = 1.63, 95% CI: 0.66–4.05, p = 0.29), multiple (OR = 1.13, 95% CI: 0.35–3.67, p = 0.83), or staghorn stones (OR = 0.92, 95% CI: 0.40–2.13, p = 0.84; Supplemental Fig. 1). When stratified according to stone size, stone ⩽2 cm in standard PCNL was associated with a better SFR than mini-PCNL (OR = 2.79, 95% CI: 1.12–6.98, p = 0.03), whereas stone >2 cm did not (OR = 0.96, 95% CI: 0.53–1.74, p = 0.89; Supplemental Fig. 2). The tract size of the same group was not the same. The tract size of the standard PCNL ranges from 22F to 30F, and the mini-PCNL varies from 14F to 20F. We divided the tract size of standard PCNL into 24F group, 26F group, and 30F group. The results showed that 30F group of standard PCNL was associated with higher SFR than mini-PCNL group (OR = 1.73, 95% CI: 1.12–2.68, p = 0.01), while there was no statistically significant difference between 24F and 26F groups and mini-PCNL (OR = 0.50, 95% CI: 0.21–1.18, p = 0.11; OR = 0.78, 95% CI: 0.49–1.25, p = 0.30; respectively; Fig. 3).
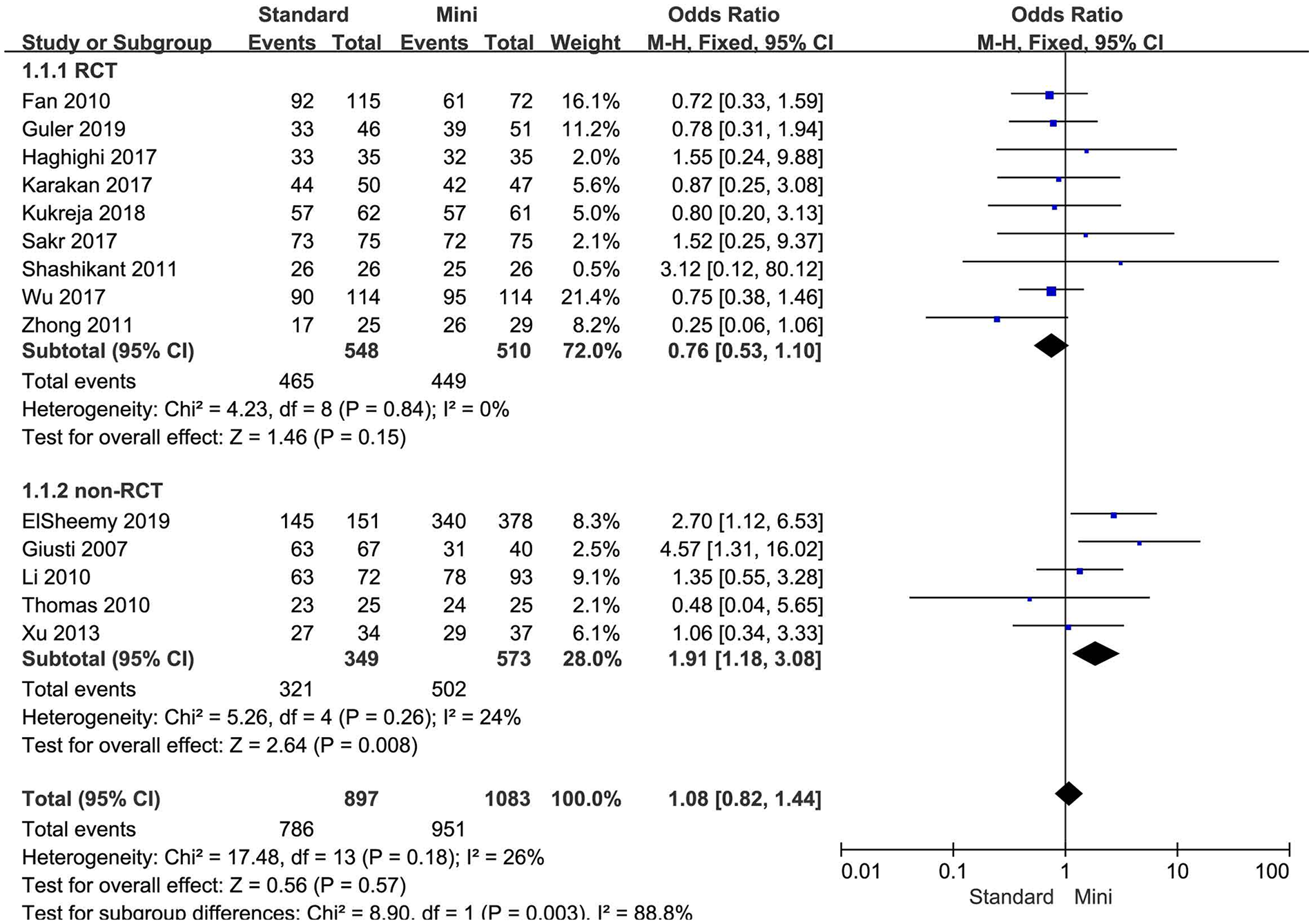
Forest plot for SFR according to trial design.
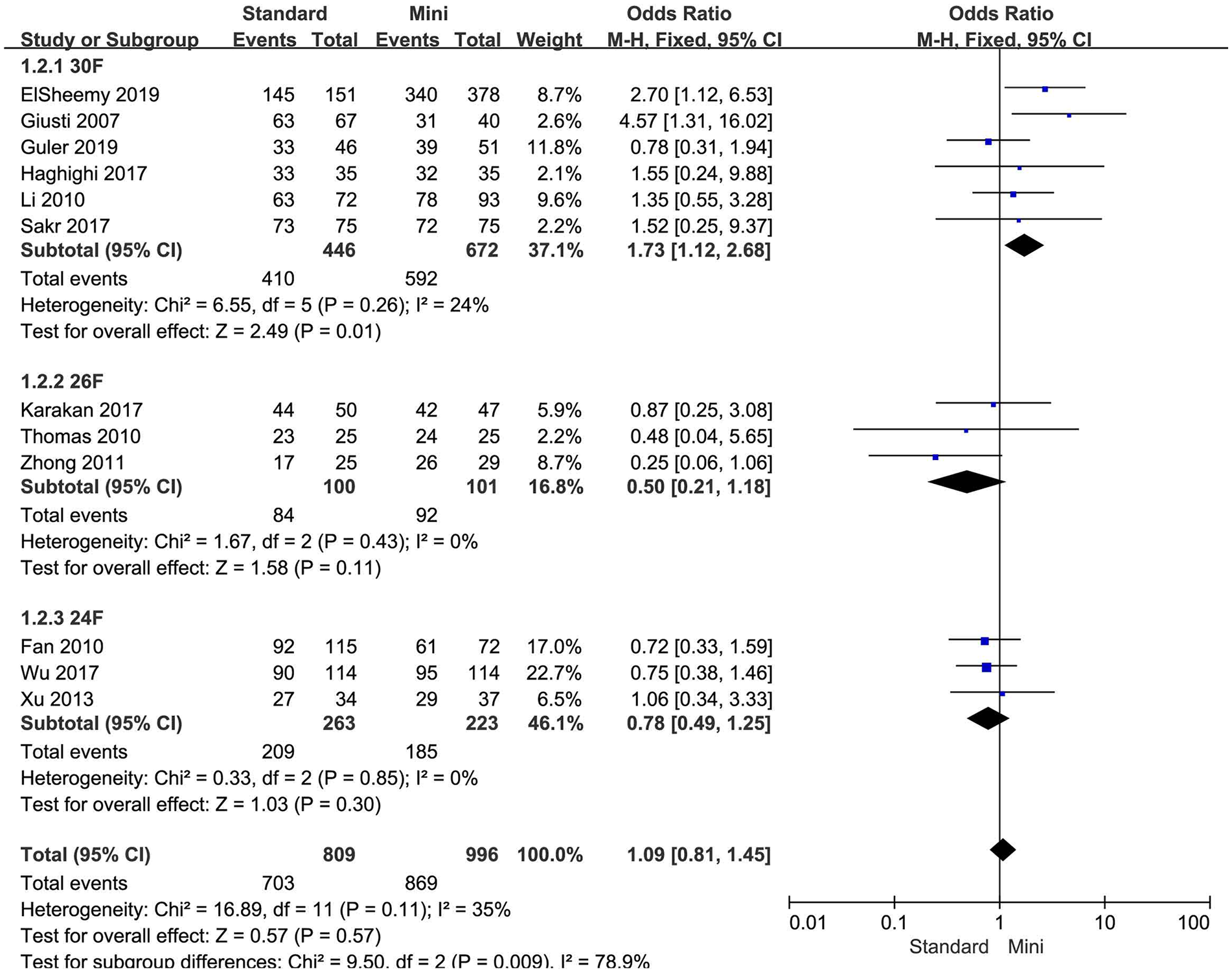
Forest plot for SFR according to tract size.
Operation Time and Subgroup Analysis
We divided the tract sizes of standard PCNL into 22–26F group and 30F group to analyze the operation time. One of the studies included 22F and 24F tract sizes in the standard PCNL 12 was assigned to the 22–26F group. Compared with the mini-PCNL, the 30F group of the standard PCNL was associated with shorter operation time (mean deviation (MD): –18.41, 95% CI: –33.79 to –3.03, p = 0.02; Fig. 4), and the 22–26F group showed similar results (MD: –7.94, 95% CI: –13.39 to –2.49, p = 0.004; Fig. 4).
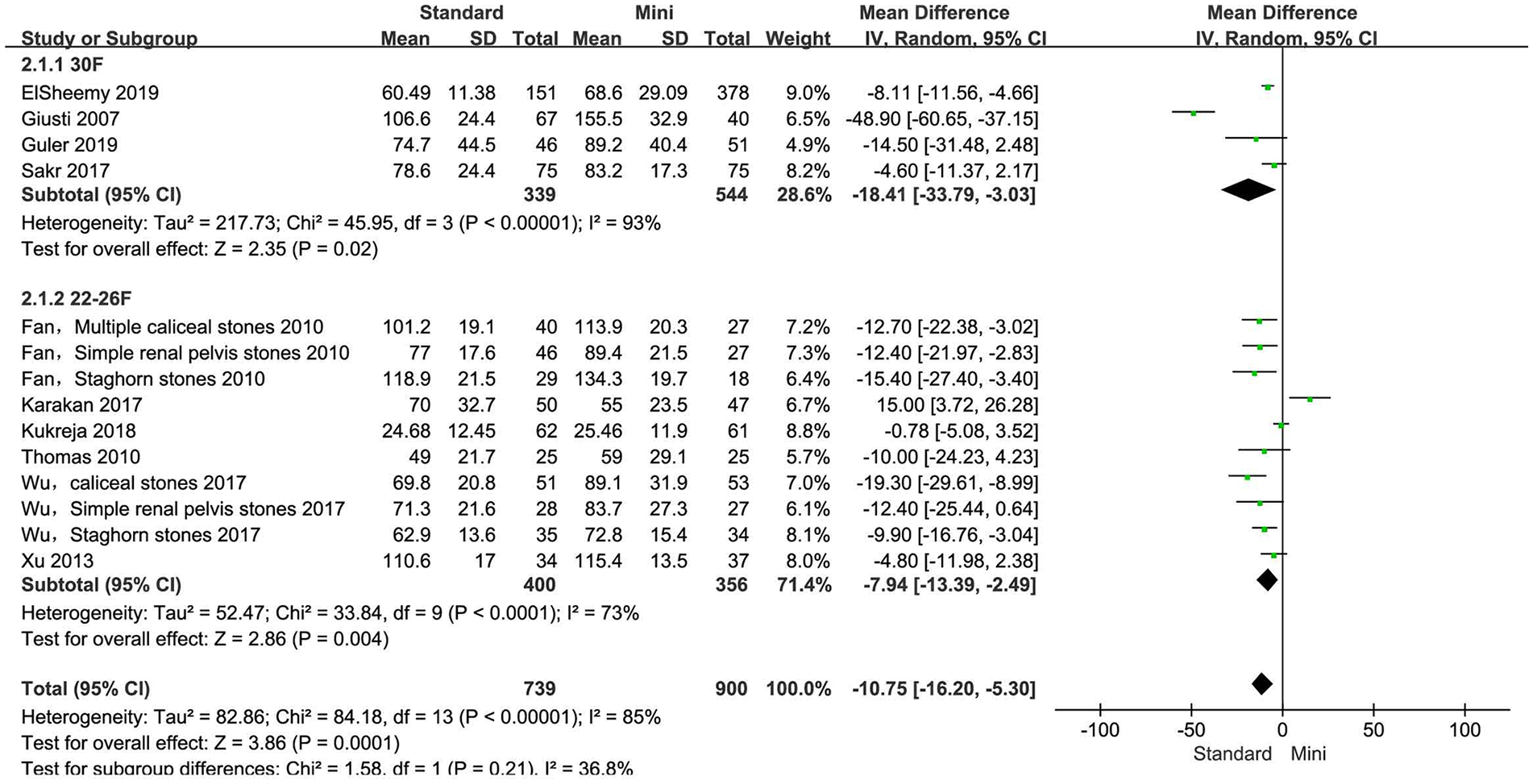
Forest plot for operation time according to tract size.
Complications and Subgroup Analysis
Complications analyzed in this meta-analysis included leakage, bleeding, blood transfusion, fever and UTI, RP perforation, calcular obstruction, leakage (JJ insertion), pneumothorax, and hematoma (embolization). Leakage (OR = 6.31, 95% CI: 1.06–37.53, p = 0.04), bleeding (OR = 2.27, 95% CI: 1.22–4.24, p = 0.01), blood transfusion (OR = 3.53, 95% CI: 2.02–6.17, p < 0.00001), and RP perforation (OR = 2.55, 95% CI: 1.15–5.64, p = 0.02) were more common in standard PCNL group than in mini-PCNL group (Supplemental Fig. 3). Fever and UTI (OR = 1.22, 95% CI: 0.70–2.14, p = 0.48), calcular obstruction (OR = 1.78, 95% CI: 0.18–18.07, p = 0.63), leakage (JJ insertion) (OR = 2.58, 95% CI: 0.84–7.93, p = 0.10), pneumothorax (OR = 0.28, 95% CI: 0.03–2.71, p = 0.27), and hematoma (embolization) (OR = 1.82, 95% CI: 0.30–11.18, p = 0.52) were not statistically different between standard PCNL and mini-PCNL (Supplemental Fig. 3). The subgroup analyses were carried out according to the size of tract. Bleeding risk for 30F or 22–26F standard PCNL group was similar to mini-PCNL (OR = 1.95, 95% CI: 0.90–4.23, p = 0.09; OR = 2.70, 95% CI: 0.83–8.81, p = 0.10; respectively; Fig. 5). However, blood transfusion for 30F and 22–26F standard PCNL group was more common than in mini-PCNL (OR = 3.52, 95% CI: 1.95–6.33, p < 0.0001; OR = 6.93, 95% CI: 1.78–27.02, p = 0.005; respectively; Fig. 6). In terms of RP perforation, the risk was similar between 30F or 22–26F standard PCNL and mini-PCNL (OR = 2.26, 95% CI: 0.18–28.07, p = 0.53; OR = 1.53, 95% CI: 0.44–5.34, p = 0.50; respectively; Fig. 7).
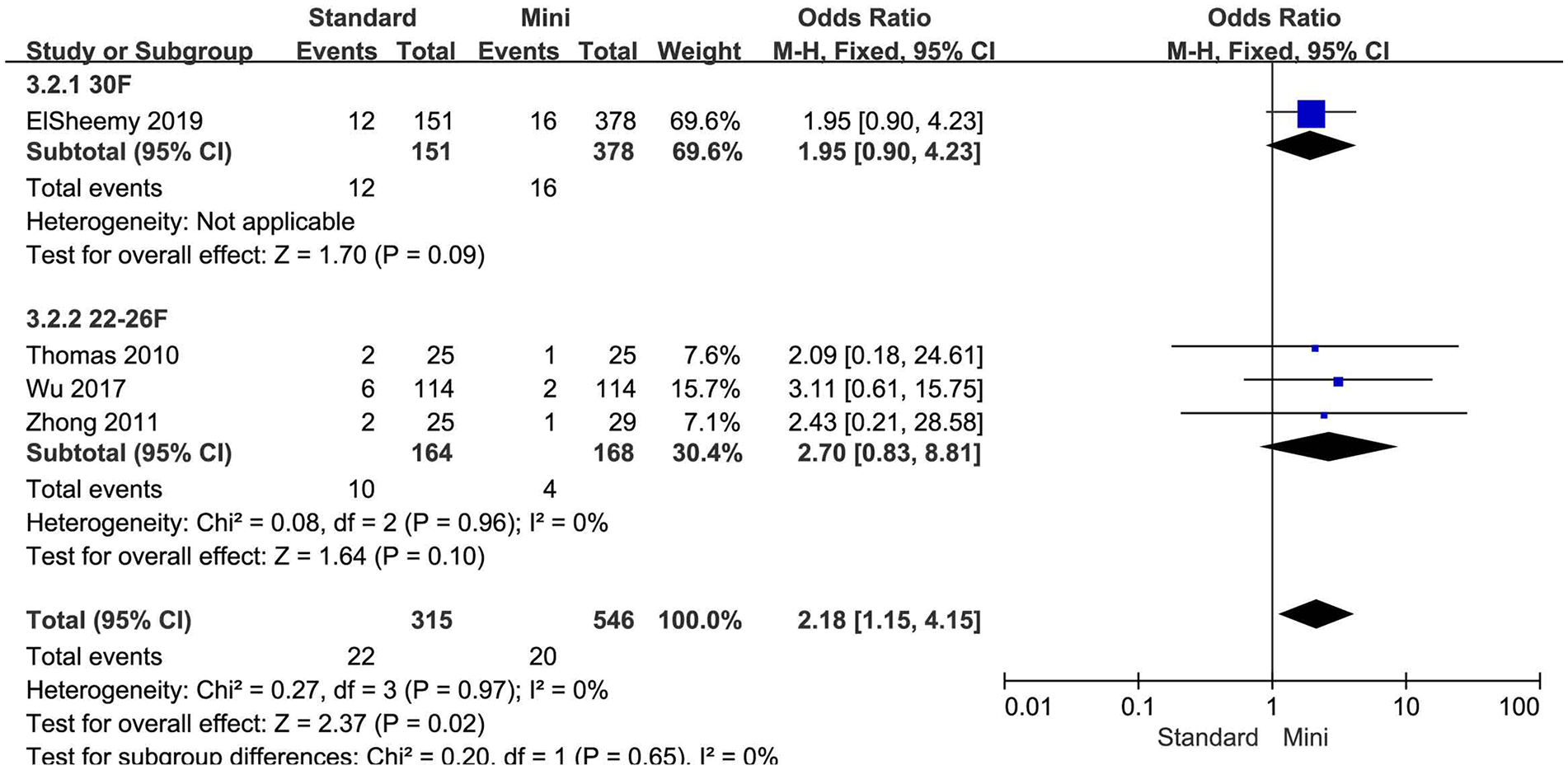
Forest plot for bleeding according to tract size.
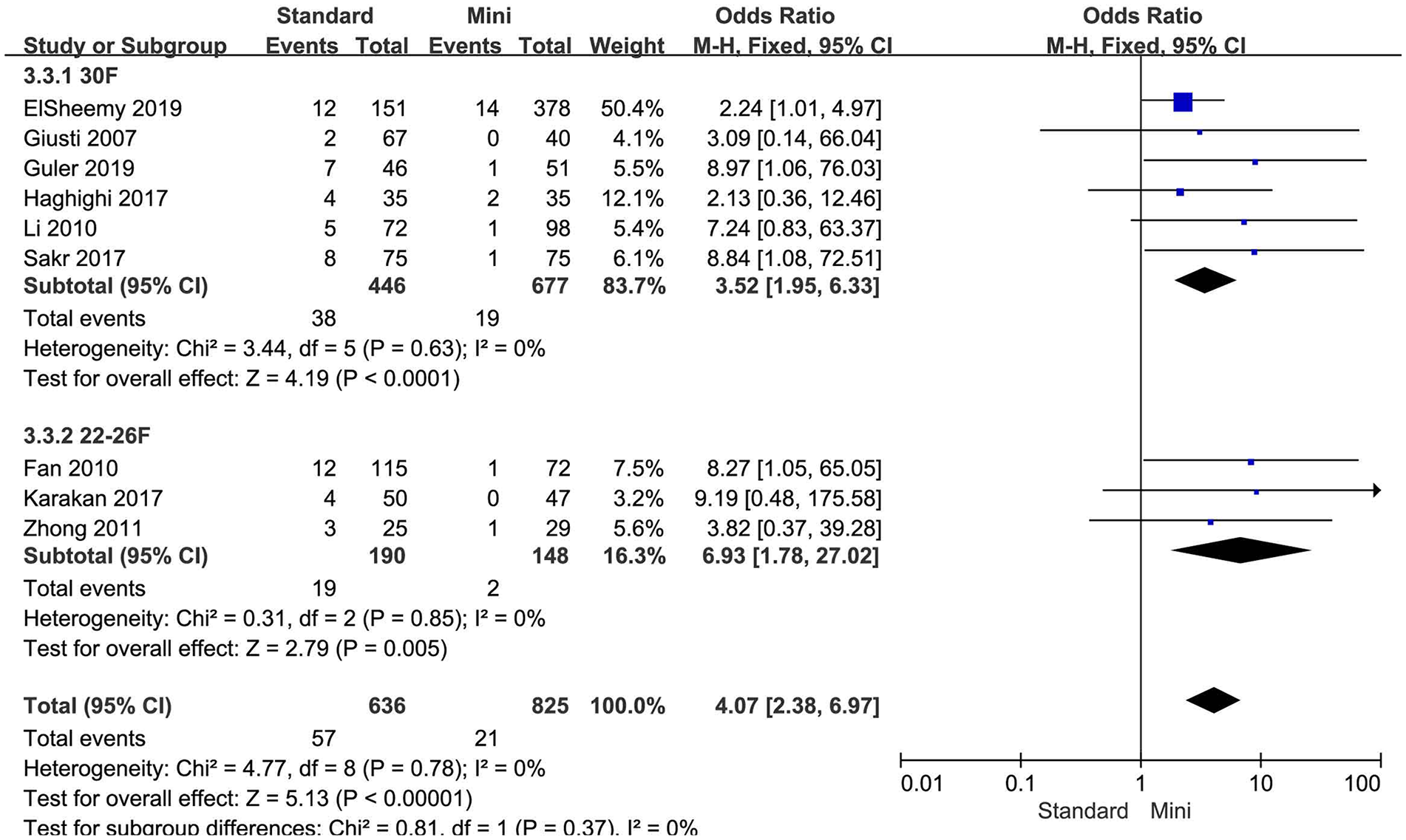
Forest plot for blood transfusion according to tract size.
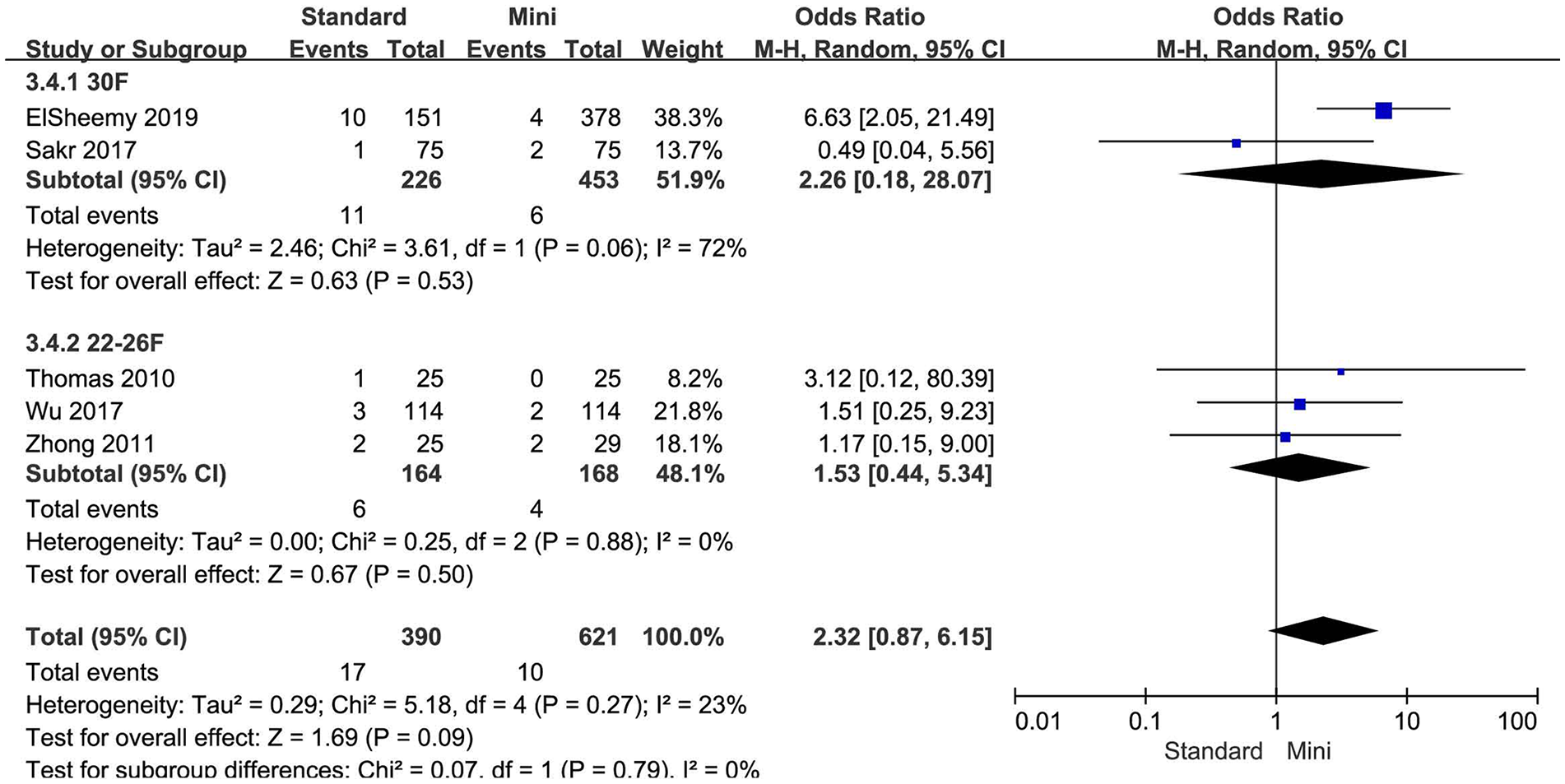
Forest plot for RP perforation according to tract size.
Publication Bias
Egger’s test and Begg’s funnel plots were used to assess the publication bias in this meta-analysis. The results of Egger’s funnel plot test were as follows: SFR (p = 0.871), operation time (p = 0.119), leakage (p = 0.798), bleeding (p = 0.204), blood transfusion (p = 0.093), fever and UTI (p = 0.782), RP perforation (p = 0.097), calcular obstruction (p = 0.317), leakage (JJ insertion) (p = 0.346), and hematoma (embolization) (p = 0.317). It verified that publication bias did not exist among the included studies. Berg test (p = 0.903; Supplemental Fig. 4) also supports this conclusion.
Sensitivity Analysis
Studies were sequentially removed to investigate whether any study affected the pooled results. The pooled result did not exhibit alterations when an individual study was excluded (Supplemental Fig. 5).
Discussion
Mini-PCNL achieves fair stone-free status while minimizing morbidity and complications through a smaller tract size compared with standard PCNL. Debate always exists on the efficacy and safety 11 . Generally, standard PCNL leads to a better SFR but is associated with a significant treatment morbidity 24 . Previous meta-analysis demonstrated mini-PCNL was a safe and effective procedure with an SFR comparable to that of standard PCNL 1,2. As an issue focus on tract size, these researches did not perform subgroup analysis according to different tract size. In addition, randomized trials were limited. To our knowledge, this meta-analysis was the first to stratify tract sizes into 30F, 26F, and 24F groups. The aim of this study was to achieve more and accurate outcome of mini-PCNL versus standard PCNL for treatment of renal stones. Based on sufficient data of included studies, selection bias was reduced by subgroup analysis.
Several findings have not been reported before the present meta-analysis. First, SFR was different between standard PCNL and mini-PCNL for non-RCT trials, but not RCT trials (Fig. 2). Generally, RCT represented high-quality research, this meta-analysis provided high-level evidence suggested mini-PCNL reached similar SFR compared with standard PCNL. Second, 30F but not 24 or 26F tract size in standard PCNL was superior than mini-PCNL for SFR. Larger tract size (30F) had an advantage for SFR (91.9%) compared with mini tract size (14–20F; SFR = 88.1%). Third, standard PCNL had a shorter operation time than mini-PCNL; however, one study suggested duration of surgery was longer in standard PCNL group 15 . The reason may be that the tract was created by a single-shot 14F dilator in patients who underwent mini-PCNL. Fourth, complications such as leakage, bleeding, blood transfusion, and RP perforation were found more common in standard PCNL group than in mini-PCNL group, subgroup analysis only verified blood transfusion in 30F or 22–26F tract size group was more common than in mini-PCNL group, rather than bleeding, or RP perforation. On the whole, complications were similar between standard PCNL and mini-PCNL besides blood transfusion.
The comparison between standard PCNL and mini-PCNL is essential to find the optimal tract size used for PCNL. Usually, standard PCNL is referred to access sheaths no less than 22F, mini-PCNL covers sheath sizes between 11 and 20F for which a 7-F pediatric cystoscope or 9.5F flexible ureterorenoscope are commonly used 25 . Subgroup analysis for different tract size in standard PCNL was performed, 30F tract size for standard PCNL was superior than mini-PCNL according to SFR (91.9% vs 88.1%), but with more blood transfusion (8.5% vs 2.8%). Tract sizes of 22–26F had similar SFR when compared with mini-PCNL, blood transfusion was common (10% vs 1.4%). An advantage of 30F or 22–26F tract size was shortened operation time; it seems to be that the larger the tract size, the shorter the operative time (Fig. 4). It was noted that the fever and UTI incidence was not different between standard PCNL and mini-PCNL, controlled irrigation pressure, and intrarenal pressure maybe important 26 .
Present research indicated that mini-PCNL can reach similar SFR as standard PCNL, and mini-PCNL reduced the risk of blood transfusion. A disadvantage of mini-PCNL was longer operation time. Optimal tract size should be chosen by surgeon according to his experience. Mini-PCNL or 30F may be applied to achieve high SFR or low complication, while 22–26F tract size seemed to be having lower SFR and higher rates of blood transfusion.
Several improvements should be implemented in the future. First, some studies 3 –6,10,16 included a relatively small number of patients. Larger number of patients were needed to achieve sufficient power to obtain valid results. Second, few studies 8,11 focused on the effect of stone number on the comparison. Third, tract size in mini-PCNL group varies from 14 to 20F, the efficiency of distinct size in mini-PCNL group should be further assessed. Fourth, assessment of the SFR was performed by the use of either less sensitive standard radiology (kidney–ureter–bladder (KUB)) or significantly more sensitive computed tomography 1 . Despite these limitations, our meta-analysis updated previous data and provided high-quality evidence.
Conclusion
Standard PCNL was associated with higher leakage, bleeding, blood transfusion, and RP perforation, but had a shorter operation time. Tract size of 30F improved the SFR compared with mini-PCNL, but led to more complications. Tract size of 22–26F was no better than 30F or mini-PCNL. Optimal tract size may be chosen by surgeon according to experience.
Supplemental Material
sj-jpg-1-sjs-10.1177_1457496920920474 – Supplemental material for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis
Supplemental material, sj-jpg-1-sjs-10.1177_1457496920920474 for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis by Jun Deng, Jin Li, Longwang Wang, Yanyan Hong, Liangliang Zheng, Jieping Hu and Renrui Kuang in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-2-sjs-10.1177_1457496920920474 – Supplemental material for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis
Supplemental material, sj-jpg-2-sjs-10.1177_1457496920920474 for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis by Jun Deng, Jin Li, Longwang Wang, Yanyan Hong, Liangliang Zheng, Jieping Hu and Renrui Kuang in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-3-sjs-10.1177_1457496920920474 – Supplemental material for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis
Supplemental material, sj-jpg-3-sjs-10.1177_1457496920920474 for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis by Jun Deng, Jin Li, Longwang Wang, Yanyan Hong, Liangliang Zheng, Jieping Hu and Renrui Kuang in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-4-sjs-10.1177_1457496920920474 – Supplemental material for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis
Supplemental material, sj-jpg-4-sjs-10.1177_1457496920920474 for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis by Jun Deng, Jin Li, Longwang Wang, Yanyan Hong, Liangliang Zheng, Jieping Hu and Renrui Kuang in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-5-sjs-10.1177_1457496920920474 – Supplemental material for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis
Supplemental material, sj-jpg-5-sjs-10.1177_1457496920920474 for Standard versus mini-percutaneous nephrolithotomy for renal stones: a meta-analysis by Jun Deng, Jin Li, Longwang Wang, Yanyan Hong, Liangliang Zheng, Jieping Hu and Renrui Kuang in Scandinavian Journal of Surgery
Footnotes
Author contributions
J.H. developed the project; J.D., Y.H., L.W., and J.L. performed data collection and management; J.D., L.W., J.L., and L.Z. analyzed and interpreted the data; J.H., J.D., and J.L. wrote the manuscript; Y.H. and R.K. edited the manuscript; and R.K supervised the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in the included studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committees and with the 1964 Declaration of Helsinki and its subsequent amendments or comparable ethical standards. This article does not contain any studies with human participants performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Project of the Education Department of Jiangxi Province (GJJ160036, GJJ180007, and GJJ180031).
Informed consent
Informed consent was obtained from all individual participants in the included studies. For this study, formal consent was not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.