
Abstract
Background and Aims:
Selective nonoperative management of abdominal stab wound is well established, but its application in the setting of isolated omental evisceration remains controversial. The aim of the study is to establish the role of selective nonoperative management in the setting of isolated omental evisceration.
Materials and Methods:
A retrospective study was conducted over an 8-year period from January 2010 to December 2017 at a major trauma center in South Africa to determine the outcome of selective nonoperative management.
Results:
A total of 405 consecutive cases were reviewed (91% male, mean age: 27 years), of which 224 (55%) cases required immediate laparotomy. The remaining 181 cases were observed clinically, of which 20 (11%) cases eventually required a delayed laparotomy. The mean time from injury to decision for laparotomy was <3 h in 92% (224/244), 3–6 h in 6% (14/244), 6–12 h 2% (4/244), and 12–18 h in 1% (2/244). There was no significant difference between the immediate laparotomy and the delayed laparotomy group in terms of length of stay, morbidity, or mortality. Ninety-eight percent (238/244) of laparotomies were positive and 96% of the positive laparotomies (229/238) were considered therapeutic.
Conclusion:
Selective nonoperative management for abdominal stab wound in the setting of isolated omental evisceration is safe and does not result in increased morbidity or mortality. Clinical assessment remains valid and accurate in determining the need for laparotomy but must be performed by experienced surgeons in a controlled environment.
Introduction
Selective nonoperative management (SNOM) of penetrating abdominal trauma has been widely accepted as a safe approach and is the standard of care for most high-volume trauma centers worldwide (1). However, the management of the subgroup of patients with abdominal stab wounds (SWs) and associated omental evisceration remains highly controversial (2, 3). Mandatory laparotomy is still regarded as the standard of care by many surgeons, especially in low-volume centers (2–5). The rationale behind this is the perceived high incidence of significant intra-abdominal injuries, the necessity to repair the abdominal wall defect, and the potential for sepsis if contaminated content is replaced back into the abdominal cavity (3, 4). Although omental evisceration implies established peritoneal breach, this observation per se does not automatically imply the presence of significant intra-abdominal injury (2–5). In principle, the same indications for mandatory laparotomy as those without omental evisceration remain valid and provided that the patient does not have any concerning clinical evidence of significant intra-abdominal injury, there is little reason why SNOM cannot be applied (2, 6). SNOM is widely practiced in South Africa due to resource constrains in face of a huge burden of penetrating trauma. The landmark paper by Huizinga et al. (2) in the 1980s from our parent institution at King Edward VIII Hospital in Durban demonstrated that SNOM in the setting of abdominal SW with isolated omental evisceration is safe. We have continued to manage this injury by SNOM over the past four decades, but the contemporary outcome of patients managed under this policy has never been subjected to any formal review. The objective of this study was to review our contemporary experience and the clinical outcome of a policy SNOM of patients with abdominal SWs with associated isolated omental evisceration managed by a major trauma center in South Africa.
Materials and Methods
Clinical Setting
This was a retrospective, observational study that focused on a specific predefined population of patients who sustained abdominal SW with isolated omental evisceration. The study was based at the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa. The PMTS provides definitive trauma to the city of Pietermaritzburg, the capital of KwaZulu Natal (KZN) province. PMTS is the largest academic trauma center in western KZN and is the tertiary trauma referral center covering a total catchment population of over three million people. Each year, approximately 5000 trauma cases are admitted to the PMTS with over half of these due to penetrating trauma. This is directly related to the high incidence of interpersonal violence, gang-related activities, and serious crime throughout the province. The proportion of penetrating trauma is relatively high in comparison to many centers in Western Europe and the volume managed is comparable to similar sized centers in the United States (7, 8). The PMTS maintains a formal regional trauma registry. All patients who present to our trauma center are prospectively entered into the database, and the information entered includes details regarding injury mechanism, operative intervention, patient progress, and clinical outcomes. Ethics approval for the maintenance of this registry for both clinical care and research has been formally endorsed by the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu Natal (UKZN). Where applicable, formal consent from patients for the use of clinical photographs pertaining to this study has been obtained.
Current Management Protocol
Any patient who sustains an abdominal SW with omental evisceration is assessed immediately upon arrival our trauma center. Initial assessment is based on the Advanced Trauma Life Support (ATLS©) principles. Further comprehensive assessment is then conducted that includes an appropriate history, physical examination, routine laboratory tests (full blood count, urea and electrolytes), and urinalysis. Those who present with frank peritonitis and/or hemodynamic instability are considered as absolute indications for laparotomy and are expedited to the operating room immediately. Those in whom abdominal examination is regarded as unreliable (e.g. concurrent severe head trauma or severe intoxication) are also subjected to laparotomy. In all cases who required immediate surgery, the eviscerated omentum is covered with a clear dressing and the patient is transferred to the operating room. Fig. 1 illustrates a typical example of a young male patient who sustained an abdominal SW with isolated omental evisceration.

Abdominal SW with isolated omental evisceration.
Those who do not have any indication for immediate laparotomy (IL) are managed as follows: First, protruding omentum is ligated (e.g. 3/0 polydioxanone sutures (PDS)) and amputated. The ligated proximal portion is then reduced back into the abdominal cavity. The fascial defect can be extended sufficiently to allow reduction of the ligated portion. The wound is thoroughly irrigated with antiseptics and the fascial defect is closed under direct vision with nonabsorbable sutures (e.g. 2/0 Prolene). The skin is lightly opposed with several interrupted non-absorbable sutures (e.g. 2/0 Prolene). This is performed under local anesthetics in the resuscitation room. Fig. 2 illustrates the technique for ligation, amputation, and reduction.

Ligation and amputation of the eviscerated omentum.
Tetanus toxoid is given where appropriate but prophylactic antibiotics are not given routinely. The patients are then admitted to the general trauma ward for active clinical observation. These patients are kept strictly nil by mouth, with intravenous fluid, and specifically, two hourly vital signs are recorded (including temperature, heart rate, and blood pressure). Regular repeated physical examination, preferably by the same duty trauma surgeon (or the senior registrar), is performed to determine any change to patient’s clinical status. Those who exhibit (or subsequently develop) signs of sepsis (new-onset pyrexia, trending rise of leukocytosis, persistent tachycardia, increasing tenderness away from site of injury (despite maximal analgesia)), peritonitis, gastrointestinal intolerance (on feed resumption), or any unexplained clinical deterioration, at the discretion of the duty trauma surgeon, will proceed to laparotomy. All patients are actively observed for up to a period of 48 h. At present, most literature on SNOM of abdominal SWs suggested minimal benefit for observation beyond 48 h (9). Thereafter, if the patient’s clinical status remains unchanged throughout the observation period, they are discharged home from the general trauma ward with advice to return if they deteriorate after discharge. We do not perform computed tomography (CT) for abdominal SWs. The management protocol is summarized in Fig. 3.
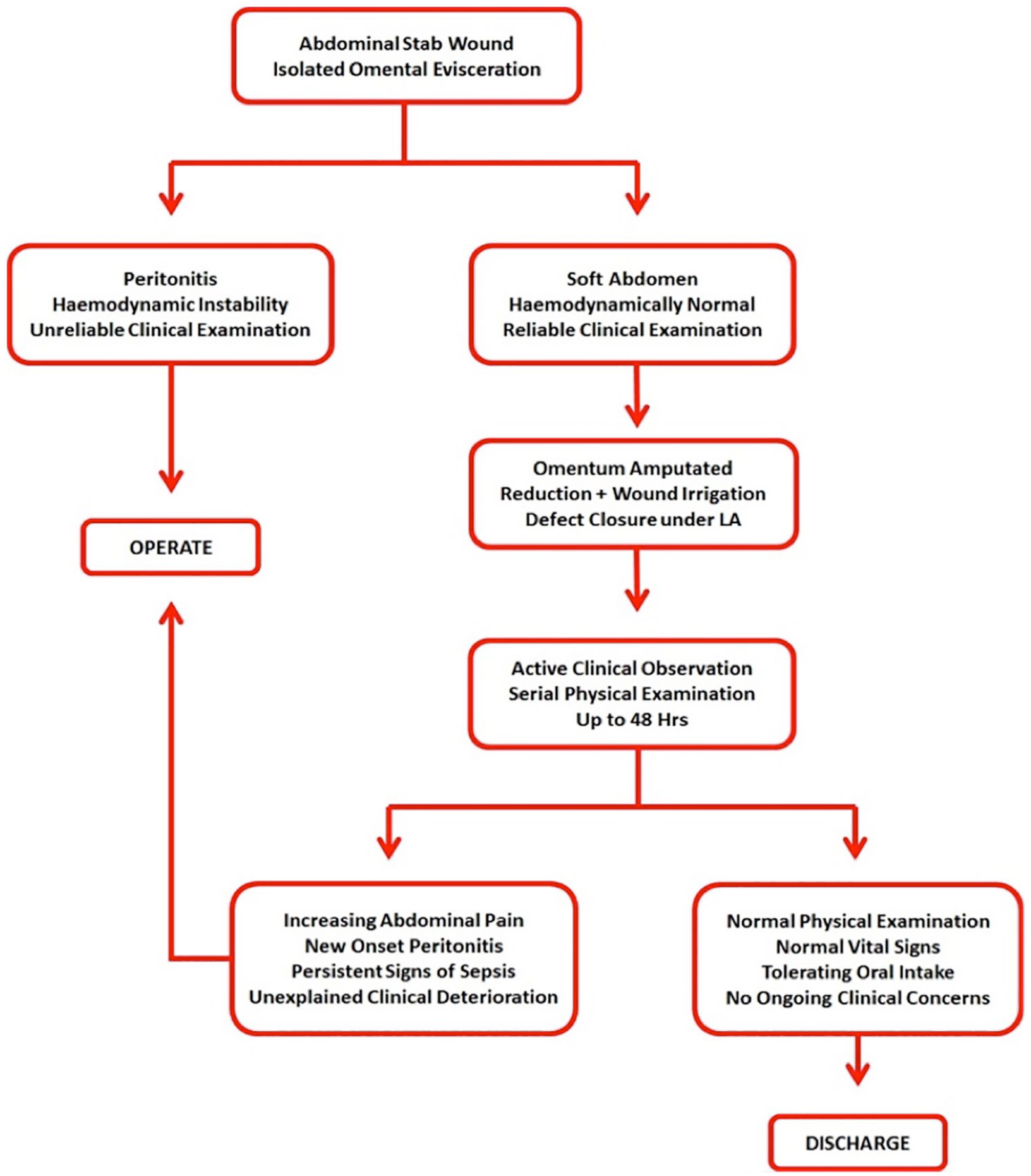
Management protocol for abdominal SW with isolated omental evisceration.
The Study
A retrospective review was conducted on all patients who presented with abdominal SW and isolated omental evisceration over the 8-year period from January 2010 to January 2018. For the purpose of this study, only SWs to the anterior abdomen were considered. The boundary of the anterior abdomen was defined by the costal margin superiorly, the inguinal ligaments and pubic symphysis inferiorly, and the anterior axillary line laterally. All patients who presented with organ evisceration (e.g. small bowel), with or without omental evisceration, underwent mandatory laparotomy and were excluded from this study. All patients with concurrent injuries to the chest, head and neck, and limbs were also excluded.
The spectrum of injury and clinical outcome of all patients with an abdominal SW and isolated omental evisceration managed under our current SNOM policy were reviewed. Basic demographic data were reviewed. Other data reviewed included time period of clinical observation and time from injury to operation. The clinical outcome was described in terms of in-hospital morbidity (e.g. wound sepsis, pneumonia), intensive care admission, length of hospital stay, and mortality. A subgroup analysis was performed on those who underwent laparotomy. Those patients who presented with established indications for laparotomy (the “immediate laparotomy” group) and those who subsequently developed indications for laparotomy during the observation period were reviewed. The latter group was called the “delayed laparotomy” (DL) group. The time from initial assessment to establishing the need for laparotomy was further classified according to the following time scale: <3 h, 6 h, 12 h, 18 h, and 24 h. Patients with an immediate indication for laparotomy were classed under time period <3 h. Operative findings were classified as either positive or negative. A positive laparotomy denotes any organ injury found intra-operatively as a direct result of the SW. A negative laparotomy was one where there were no injuries identified. Positive laparotomies were further subdivided into therapeutic or nontherapeutic. A positive therapeutic laparotomy was defined as identifying significant organ injuries which required operative repair. Failure to repair these injuries will result in an adverse outcome. A positive nontherapeutic laparotomy was identifying findings of an injury which did not require operative repair and which, if undetected, would have been unlikely to result in significant morbidity. These include minor splenic or liver lacerations, non-bleeding small serosal, or mesenteric injuries.
Statistical Analysis
All relevant data were extracted and initially summarized onto an EXCEL© spread sheet for review. Nonparametric (asymmetrical) data were descriptively described. All statistical analysis was performed using SPSS version 19 (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp.). Chi-square tests were used to examine differences in morbidity and mortality between those who had IL and those in whom laparotomy was indicated during the period of clinical observation (DL). A two-tailed t-test assessed whether there was a difference in total length of stay between the two groups.
Results
Demographics
A total of 405 patients over the 8-year study period were included. All of these had presented with an SW to the anterior abdomen with omental evisceration, as per the inclusion criteria. Ninety-one percent (368/405) were male and the mean age was 27 years.
Clinical Management
Two hundred twenty-four patients (55%) required IL. The remaining 181 patients did not have indications for IL and were observed clinically. Of these, 20 (11%) eventually required a laparotomy (DL). Of the total 244 who underwent laparotomy, the time from injury to decision for laparotomy was <3 h in 92% (224/244), 3–6 h in 6% (14/244), 6–12 h in 2% (4/244), and 12–18 h in 1% (2/244). This is summarized in Fig. 4.
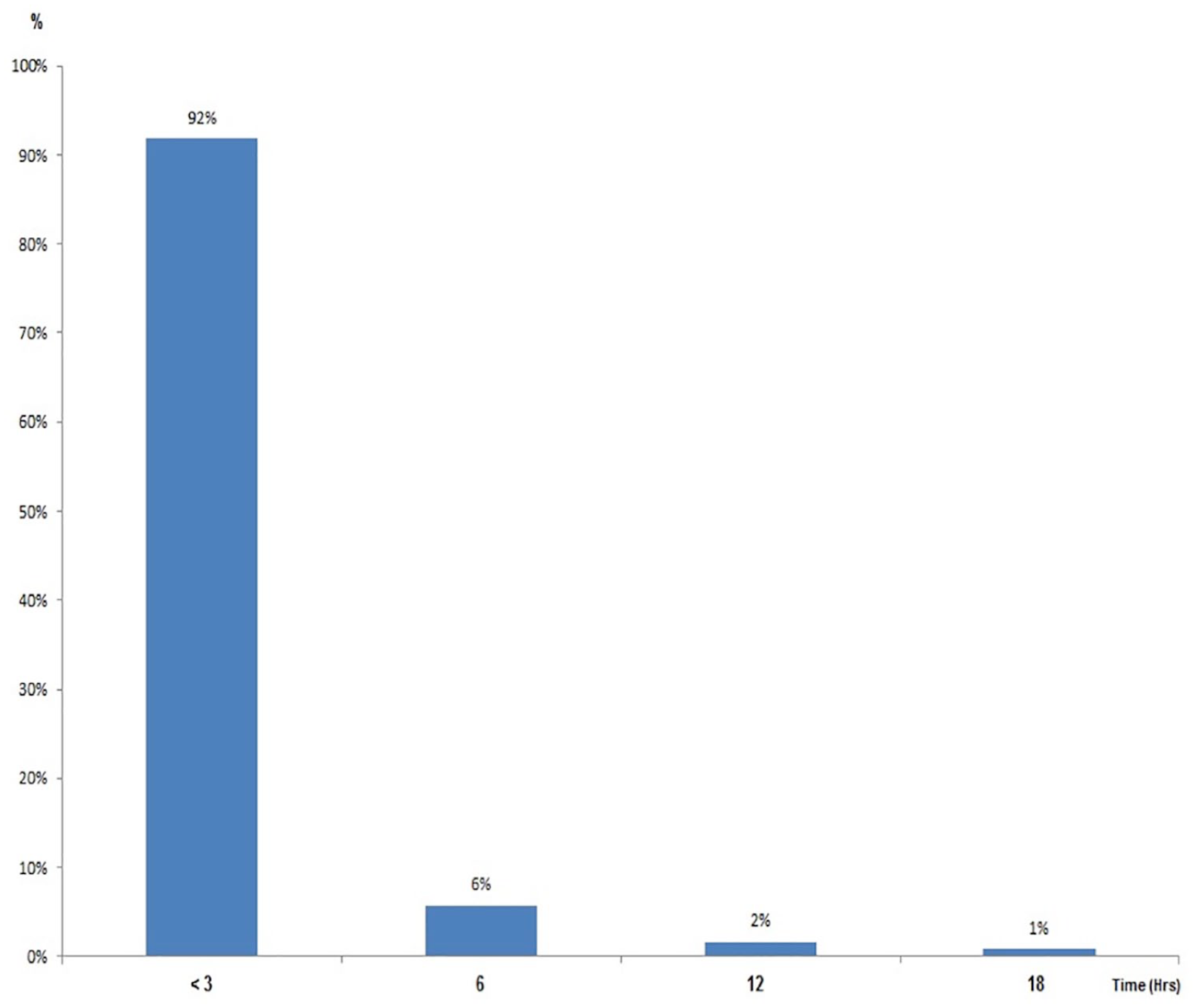
Time from injury to decision for laparotomy.
Clinical Outcome
A total of 52 patients (13%) experienced one or more complication. Six percent (25/244) of all patients had pneumonia, 6% (24/244) had wound sepsis, and 6% (24/244) required intensive care unit (ICU) admission. Two percent (9/244) had renal failure and the 1% (6/244) developed complications classified as miscellaneous (e.g. delirium). The mean length of hospital stay for all patients was 6 days. There were five mortalities: Two patients had multiple SWs with major injury to the inferior vena cava, both exsanguinated on the operating table prior to vascular control was obtained. Two patients died from acute respiratory distress syndrome (ARDS) with multiple organ failure. One patient died from pulmonary embolism. The overall mortality rate was 2%.
Immediate Laparotomy Versus Delayed Laparotomy
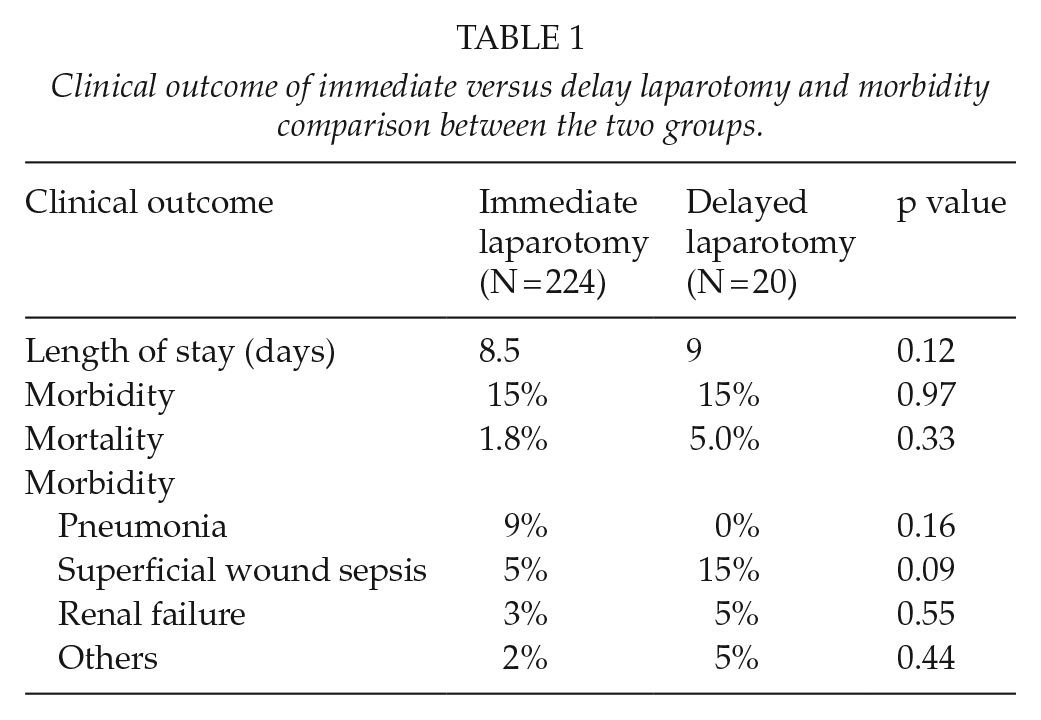
Direct comparison was made between the 224 patients who underwent IL and the 20 patients who underwent a DL after a period of clinical observation after the indication for laparotomy became apparent found no differences in terms of length of hospital stay, morbidity, or mortality. This is summarized in Table 1. The type of morbidities was further compared between those who underwent IL and those who underwent a DL, which is also summarized in Table 1.
Clinical outcome of immediate versus delay laparotomy and morbidity comparison between the two groups.
Laparotomy Findings
Of the total of 244 patients who underwent laparotomy, 98% (238/244) were positive and the remaining 2% (6/244) were negative. Of the 224 positive laparotomies, 96% (229/238) were considered therapeutic and the remaining 4% (9/238) were nontherapeutic. This is summarized in Fig. 5.
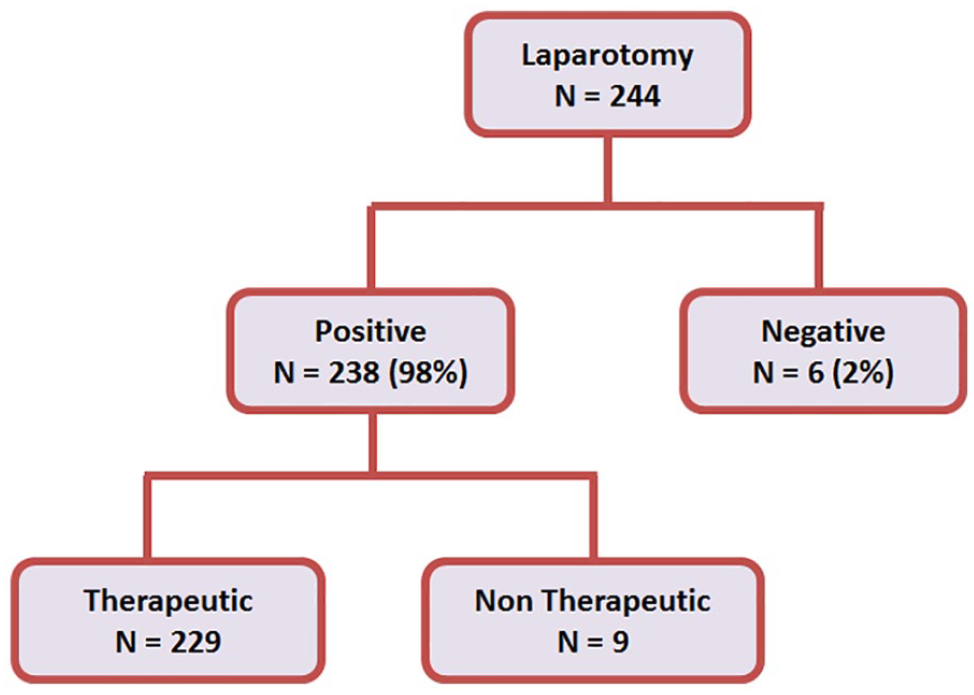
Flowchart of key results.
Of the IL group (224), the total number of associated visceral injuries was 238 (98%). As a proportion of the IL group, of the associated visceral injuries, 81 (36%) were isolated visceral injuries, and the remaining 143 (64%) of cases had injury to more than one visceral structure. Of the DL group (20), the total number of associated visceral injuries was 20 (100%). As a proportion of the DL group, of the associated visceral injuries, 14 (70%) were isolated visceral injuries, and the remaining 6 (30%) of cases had injury to more than one visceral structure.
Discussion
The selective management of penetrating abdominal trauma has been widely accepted as a safe approach and is the standard of care for most high-volume trauma centers worldwide (1). Although most trauma surgeons practicing in high-volume trauma centers are comfortable with such an approach for abdominal SWs, the management of the subgroup of patients with concurrent isolated evisceration of the omentum has remained highly controversial (2). In 2010, the Eastern Association for the Surgery of Trauma (EAST) Practice Management Guideline group was unable to find sufficient evidence to provide any formal recommendations on how to manage this specific subgroup of patients (2). For many surgeons, especially in centers which do not commonly manage penetrating torso trauma, mandatory laparotomy is still widely practiced, as the perceived risk of missing a significant intra-abdominal injury is thought to outweigh that of a negative or non therapeutic laparotomy. Further arguments in support of such an approach include the need to repair the abdominal wall defect, and the potential for sepsis if contaminated omentum is reduced into the abdominal cavity.
Patients with isolated omental evisceration following abdominal SW represent a specific entity in which mandatory laparotomy has been considered to be the accepted approach by most surgeons. The reported rate of intra-abdominal injuries found on laparotomy in the setting of omental evisceration varies widely between studies (2–5, 10). In 1983, Granson and Donovan (10) from Los Angeles County Medical Center (LAC-USC) reported a series of 100 consecutive cases who underwent mandatory laparotomy and found that major intra-peritoneal injuries were present in 69% of cases. In a subsequent study by Burnweit and Thal (5) from Dallas, Texas, of 115 cases, the rate of significant intra-abdominal injuries was 75%. Nagy et al. (3) at Cook County Hospital, Chicago, reported a rate of 77% in their 81 cases. The highest reported rate was 83% reported by Medina et al. (4) from New York based on 75 cases. These authors, along with other groups from the United States, continue to recommend mandatory laparotomy (3–5, 10, 11). However, a more contemporary study by Benissa et al. (12) reported a 78% negative laparotomy rate in the 18 patients who had no peritonitis or hemodynamic compromise, while that of Arikan et al. (6) was 36%. Furthermore, McFarlane (13) reported that no complications occurred in the 14 patients who were managed nonoperatively. Table 2 summarizes the key findings of the literature published to date.
Literature to date (1983–2018).
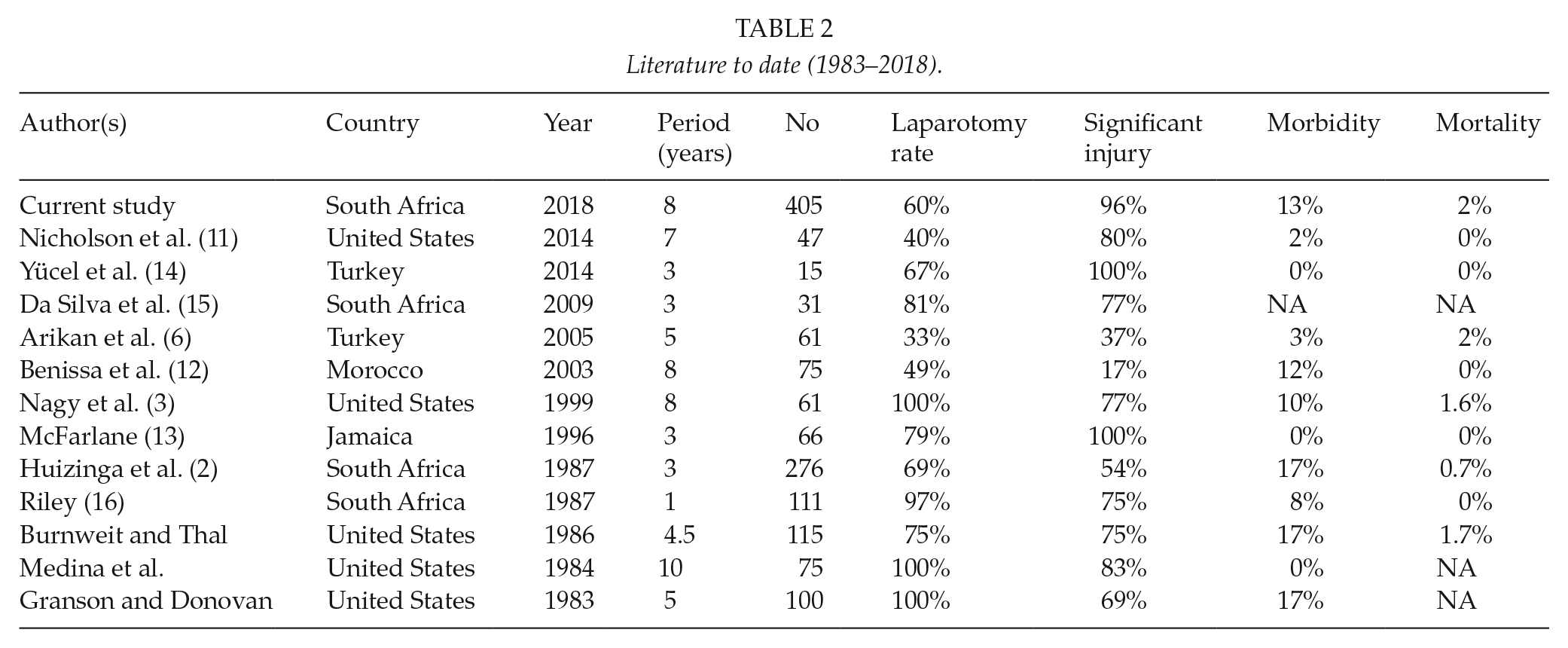
Riley (16) from our parent institution at King Edward VIII Hospital, Durban, published the first South African series of 111 patients who underwent mandatory exploration and found that 25% did not have significant intra-abdominal injury. Based on this initial experience, a policy of SNOM was then applied at the institution. Huizinga et al. (2) from the same institution then published the largest series of 276 cases managed by SNOM and documented significant intra-abdominal injuries in only 59% of cases. Furthermore, under the SNOM policy, of the subgroup of 86 patients who were observed primarily, only 10 (12%) eventually required a laparotomy (9 of which were positive) (2). The findings in our study were similar to that of Huizinga et al. (2) in that slightly over 10% of the primarily observed patients ultimately require a laparotomy. Even within the subgroup of the 26 cases managed by Demetriades et al. from Baragwanath Hospital in Johannesburg, it was noted that only one patient eventually required a laparotomy, which was negative (17).
Our SNOM approach did not result in additional morbidity or mortality. Importantly, direct comparison between those who were subjected to IL and those in whom the decision for laparotomy was established during the period of clinical observation found no significant difference in terms of length of hospital stay, morbidity, or mortality.
It is important to note that our SNOM approach is based on serial physical examination performed by the same experienced clinician. It allowed accurate identification of those who required laparotomy, reflected by fact that 98% of all laparotomies in our study were positive. Furthermore, 96% of the positive laparotomies were therapeutic. This finding was also similar with that of Huizinga et al. (2) in which the accurate prediction was over 90% based on physical examination alone. Contrary to prevailing concerns over the potential high risk of intra-abdominal injury from the reduction of the omentum, our study has shown that this concern is unfounded (3, 4). Other than minor wound sepsis, to our knowledge, none of the patients who were managed nonoperatively suffered from intra-abdominal sepsis as a direct result of our management approach.
SNOM for penetrating abdominal trauma has been practiced in South Africa for over six decades (18). This was initially born out of necessity in response to the pressure of limited resources and an excessive burden of trauma. Over the ensuing decades, SNOM has continued to be refined and become the cornerstone of trauma management in South Africa. As the “malignant epidemic” of trauma in South Africa continues to be unabated, SNOM remains both a safe and a cost-effective approach. However, even in well-resourced centers in the developed world, the SNOM continues to be regarded as appropriate in minimizing the associated morbidity associated with unnecessary exploration (1). Though technological advances and the increased availability of sophisticated imaging, such as CT, have affected trauma care both in South Africa and globally, we still base our management of penetrating abdominal trauma on detailed and repeated clinical examination. Based on our extensive expierence with SNOM in penetrating abodminal trauma, we found this to be safe and cost effective. Other studies from our institution continue to support the validity of our management philosophy that extends to the setting of abdominal gunshot wounds (GSWs) (19). Nicholson et al. (11) from LAC-USC published the only study that examined the role of CT in the specific setting of omental evisceration and found that the diagnostic yield of CT was poor and had no impact on patient management.
Limitations
One of the major limitations of this study was the lack of long term follow-up data in regard to the incidence of wound site hernia. Due to socioeconomic factors, follow-up of patients in our setting is invariably poor. Other local studies have highlighted similar challenges (20). In our experience, patients who are successfully discharged and remained well often resume their normal daily activity and seldom perceive the necessity for further follow-up. Other sociological factors such as the perceived time lost in attending follow-up may lead to loss of earnings and fear of redundancy. We assume these patients did not have any further sequelae following discharge. Furthermore, in our resource-constraint developing world environment, routine follow-up for all these patients poses a significant challenge.
Another important limitation is the possible selection bias in the DL group. It appears to be the case that this group had less severe injuries in general, given less of this group had multiple visceral injuries. The number of DL patients is also relatively low and comparisons may not be entirely accurate.
In addition, the vast majority of patients treated at our trauma center tend to have a prolonged time from injury to presentation. Although the reason for this is likely complex and multifactorial, this does suggests a possible process of ‘self-selection’ taking place.
Conclusion
Abdominal SW with associated isolated omental evisceration can be managed safely with SNOM approach in our environment. This selective and clinically driven approach also allowed a high yield of significant injuries found on laparotomy. Active clinical observation coupled with frequent serial physical examination by experienced trauma surgeons allows appropriate selection of patients but must be performed in a strictly controlled environment.
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.