
Abstract
Background and Aims:
It has become clear that vein resection and reconstruction for pancreatic ductal adenocarcinoma (PDAC) is the standard of care as supported by multiple guidelines. However, resection of large peri-pancreatic arteries remains debatable.
Materials and Methods:
This review examines the current state of vascular resection with curative intent for PDAC in the last 5 years. Herein, we consider venous (superior mesenteric vein, portal vein), as well as arterial (superior mesenteric artery, celiac trunk, hepatic artery) resection or both with or without reconstruction.
Results:
Improvement of multidrug chemotherapy has revolutionized care for PDAC that should shift traditional surgical thinking from an anatomical classification of resectability to a prognostic and biological classification.
Conclusion:
The present review gives an overview on the results of pancreatectomy associated with vascular resection, with consideration of new perspectives offered by the availability of better systemic therapies.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is currently the fourth cause of cancer-related deaths in the Western countries and it is estimated to become the second leading cause of cancer-related death by 2030 (1). Approximately 20% of patients are considered as surgical candidates at the time of diagnosis, with 50% having a metastatic disease and 30% having locally advanced (2).
Fifty years ago, Joseph Fortner first described a series of patients treated with pancreatectomy associated with major peri-pancreatic vascular resection and reconstruction (regional pancreatectomy) in order to extend the surgical indications for patients with locally advanced disease and no evidence of visible metastases (3). From that moment, pancreatic surgeons worldwide started to debate this innovative technique and there continues to be significant division between supporters and opponents of Dr Fortner’s work. One common criticism of Dr Fortner’s approach is the high peri-operative morbidity and mortality rates associated with vascular resection. In 1977, Fortner reported a series of 18 patients who underwent “regional pancreatectomies” with a postoperative mortality rate of 16.6% (4). However, in the same period, the postoperative mortality rate was 15% to 20%, after “conventional pancreatic resections” as reported in the literature of the time (5–7). Another criticism against “regional pancreatectomy” was poor long-term survival results. In Dr Fortner’s report, the 1-year survival rate of patients who underwent regional pancreatectomy was 62%. However, in the same period of time, the median survival after pancreaticoduodenectomy for PDAC was 10 months and no difference in survival between palliative bypass and resection was reported at that time (8). Thus, even without strong evidence from the literature and future guidelines were influenced by the strong criticism against the “regional pancreatectomy.”
This review examines operative procedures involving venous resections (superior mesenteric vein, portal vein), arterial resections (superior mesenteric artery, celiac trunk, hepatic artery), or both vein and artery with reconstruction. Until the end of the 90s, and despite limited evidence, the majority of pancreatic surgeons did not perform any type of pancreatectomy associated with vascular resection and reconstruction. More recently, reports have shown equivalence in terms of morbidity, mortality, and survival of pancreatectomy with versus without vein resection and reconstruction (9–11). For this reason, vein resection and reconstruction to achieve curative resection are considered the standard of care in patients with the portal/superior mesenteric vein (PV/SMV) involvement (12). In contrast, the resections of peri-pancreatic arteries remain debatable as the literature until recently has not been felt to show encouraging results in terms of long-term survival of patients who underwent pancreatectomy with combined arterial resection(s). Despite this opinion, the literature has consistently demonstrated survival advantages in patients undergoing arterial resection compared to palliative procedures (13). More interestingly, it has been demonstrated that arterial resection alone may be associated with the better long-term outcome than combined artery–vein resection. These data that tumor dimension and biology, rather than the type of vessel involved, play a prognostic role and should be taken into consideration in determining respectability (9).
The development of markedly more effective systemic therapies has called surgical dogma regarding arterial resection into question. The introduction of more effective multidrug regimens has raised the median survival of primary resectable PDAC patients treated with adjuvant therapy, from 35 to 54 months (14). At the same time, these changes have also contributed to an increase the long-term survival of patients who underwent pancreatectomy associated with arterial resection to nearly the same level of patients with primarily resectable PDAC (2, 15).
In this review, we will focus our attention on the results of pancreatectomy with associated vascular resection in the last 5 years, with attention directed toward improved outcomes from markedly improved systemic therapies (14, 16).
Pancreatectomies Associated with Vein Resections and Reconstructions
After many years of debate regarding the role of vein resection during pancreatic surgery for PDAC, there is general agreement that invasion of the PV/SMV is not a contraindication for resection and reconstruction as long as technically feasible (12). The literature has demonstrated similar postoperative morbidity and mortality rates and long-term survival compared to “conventional” pancreatectomy for some time (9, 10). Specifically analyzing the published results from the last 5 years, there are no survival differences when vein resection and reconstruction are needed for curative intent. Furthermore, the morbidity and mortality rate is not different from that reported for “conventional pancreatectomies.” Interestingly, 13 out of 43 papers published in the past 5 years report a mortality rate below 1% (Table 1). Survival data were available in a limited number of studies; however, even there, the 5-year survival rate varies from 0% to 39%, which is not different from studies published for pancreatectomy without vein resection (17–59). The overall picture as demonstrated in Table 1 shows that vein resections are commonly done in experienced centers, and that short- and long-term results are comparable with these of “conventional” pancreatic surgery.
Results of Pancreatectomies associated with vein resection.
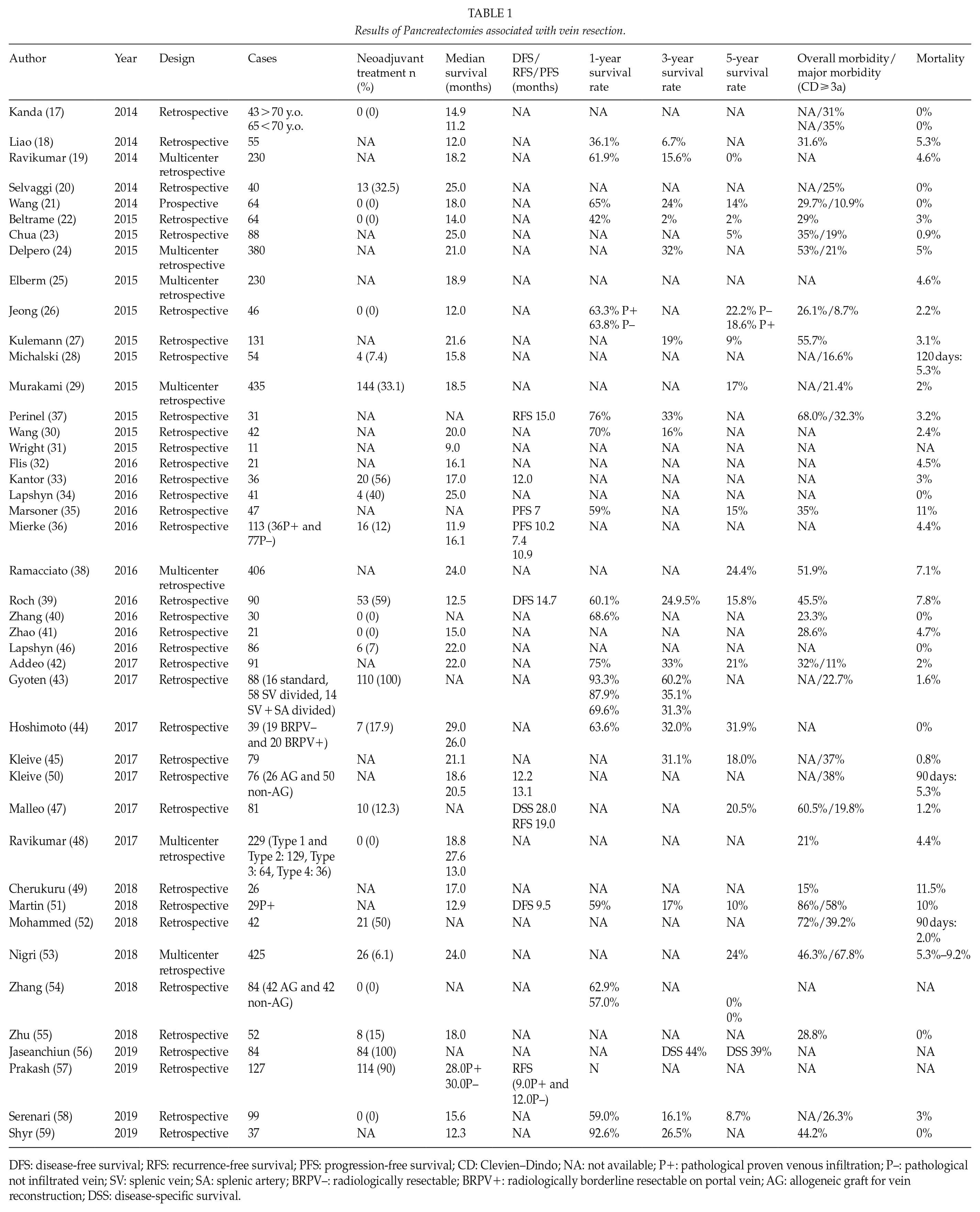
DFS: disease-free survival; RFS: recurrence-free survival; PFS: progression-free survival; CD: Clevien–Dindo; NA: not available; P+: pathological proven venous infiltration; P–: pathological not infiltrated vein; SV: splenic vein; SA: splenic artery; BRPV–: radiologically resectable; BRPV+: radiologically borderline resectable on portal vein; AG: allogeneic graft for vein reconstruction; DSS: disease-specific survival.
There are still limitations in the data available regarding pancreatectomies associated with vein resection. First of all, the data available come from different institutions with different levels of experience in this kind of procedure. Data regarding the indication for vein resection are not available in many publications. Clearly knowing the intent of surgery preoperatively is important in manuscript interpretation. In the authors’ opinion, a planned to vein resection to guarantee a local radicality is quite different from needing to perform a resection by necessity when the involvement of the vein is detected after irreversible surgical maneuvers.
Also, the absence of prospective studies makes the quality of data available debatable. Finally, no data at all are available regarding the timing of chemotherapy for these patients. In most of the classifications of resectability, vein involvement is considered as a sign of borderline resectable disease. Some centers prefer to use neoadjuvant treatment (NAT) in these cases and some others prefer to proceed with surgery first. However, no prospective randomized trials are available to offer an answer to this question.
Pancreatectomies Associated with Artery Resections without Reconstructions
This category commonly included patients with a tumor located in the body of the pancreas who undergo distal pancreatectomy associated with celiac trunk resection without reconstruction. This operation is often referred to as an Appleby procedure or distal pancreatectomy with celiac axis resection (DP-CAR). DP-CAR is a rare procedure and indicated in a very small number of patients (60). The advantages of this operation are that the redundancy of the blood supply to the liver and stomach through the gastroduodenal artery obviates the need for arterial reconstruction. Common complications are positive pancreatic margin and insufficient post-resection blood supply to the liver, and more often the stomach.
Data from the last 5 years show that DP-CAR operations can be performed safely and with an encouraging median survival (Table 2) (61–73). Only recently, a large multicenter retrospective study, collecting 174 DP-CAR, created concerning regarding the safety of this operation, reporting a postoperative mortality rate of 9.5% (73). However, this study contains patients coming from different centers that may reflect inexperience of some centers included.
Pancreatectomies associated with arterial resections without reconstruction (Appleby procedure/(distal pancreatectomy + celiac axis resection (DP-CAR).
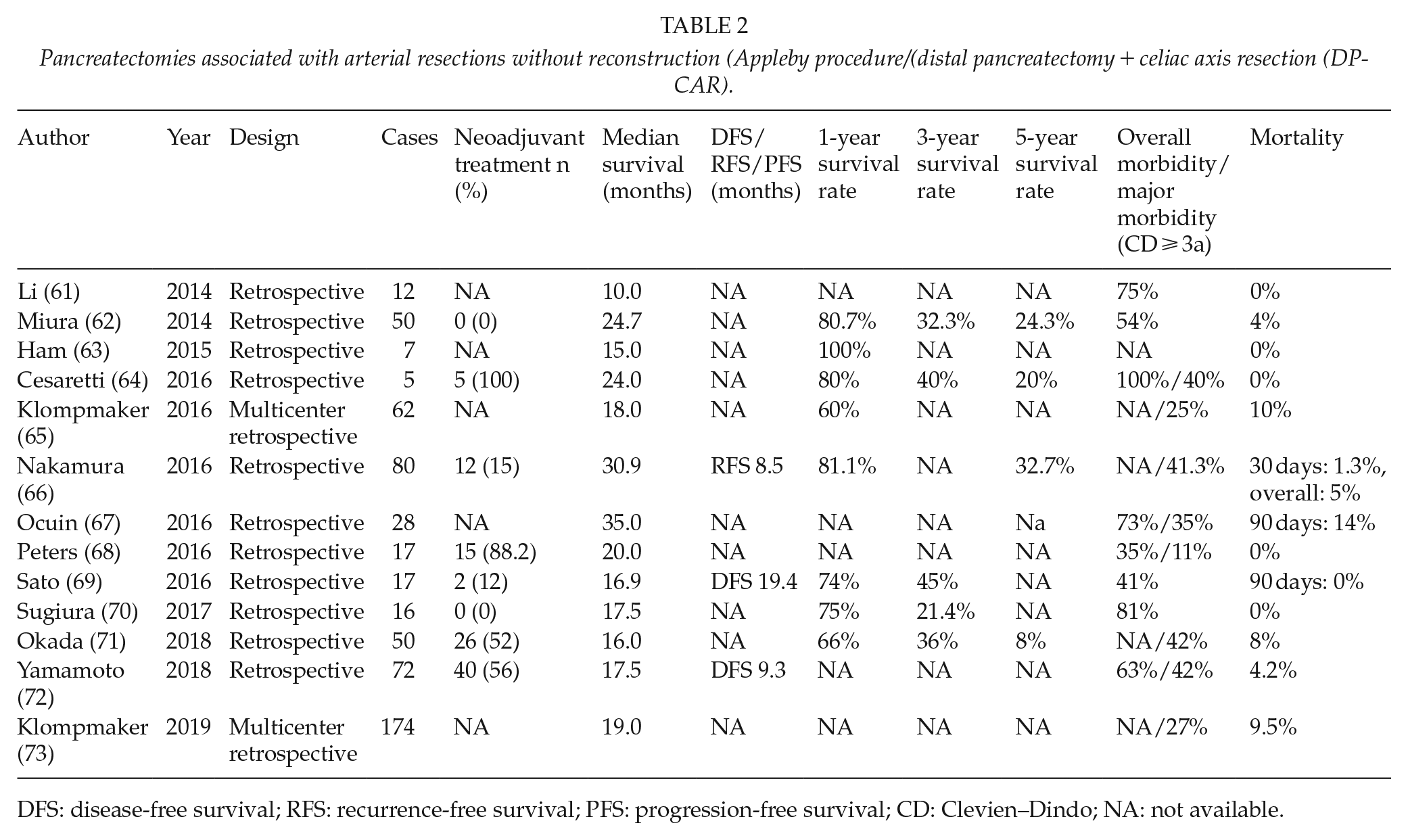
DFS: disease-free survival; RFS: recurrence-free survival; PFS: progression-free survival; CD: Clevien–Dindo; NA: not available.
Examining publications on DP-CAR, it appears that better long-term outcome is related to the use of preoperative chemo (radiation) therapy. Dr Nakamura and colleagues reported a 5-year survival rate of 78.8% after DP-CAR and NAT compared to 26.7% of patients who underwent upfront surgery (66). This difference in prognosis likely reflects improvements of modern chemotherapy as this helps stratify patient as NAT also identifies favorable biological behavior of some tumors (74).
Pancreatectomies Associated with Artery (±Vein) Resections and Reconstructions
Arterial resection/reconstruction remains a controversial topic in pancreatic surgery. Although data from the past did not clearly support the use of this aggressive approach to PDAC, newer data do suggest benefit of arterial resection in well-selected groups of patients (2, 9, 13, 15). Data from the last 5 years examining arterial resection for curative surgical intent for PDAC have changed compared to the past 20 years ago. Interestingly, many centers are reporting 5-year survival rates (around 20%) for patients who undergo arterial resection, which is improved compared to the previous results, reaching, in selected cases and after NAT, 53 months of median survival (Table 3) (2, 15, 24, 37, 75–86).
Outcome of pancreatectomies associated with artery (±vein) resection and reconstruction.
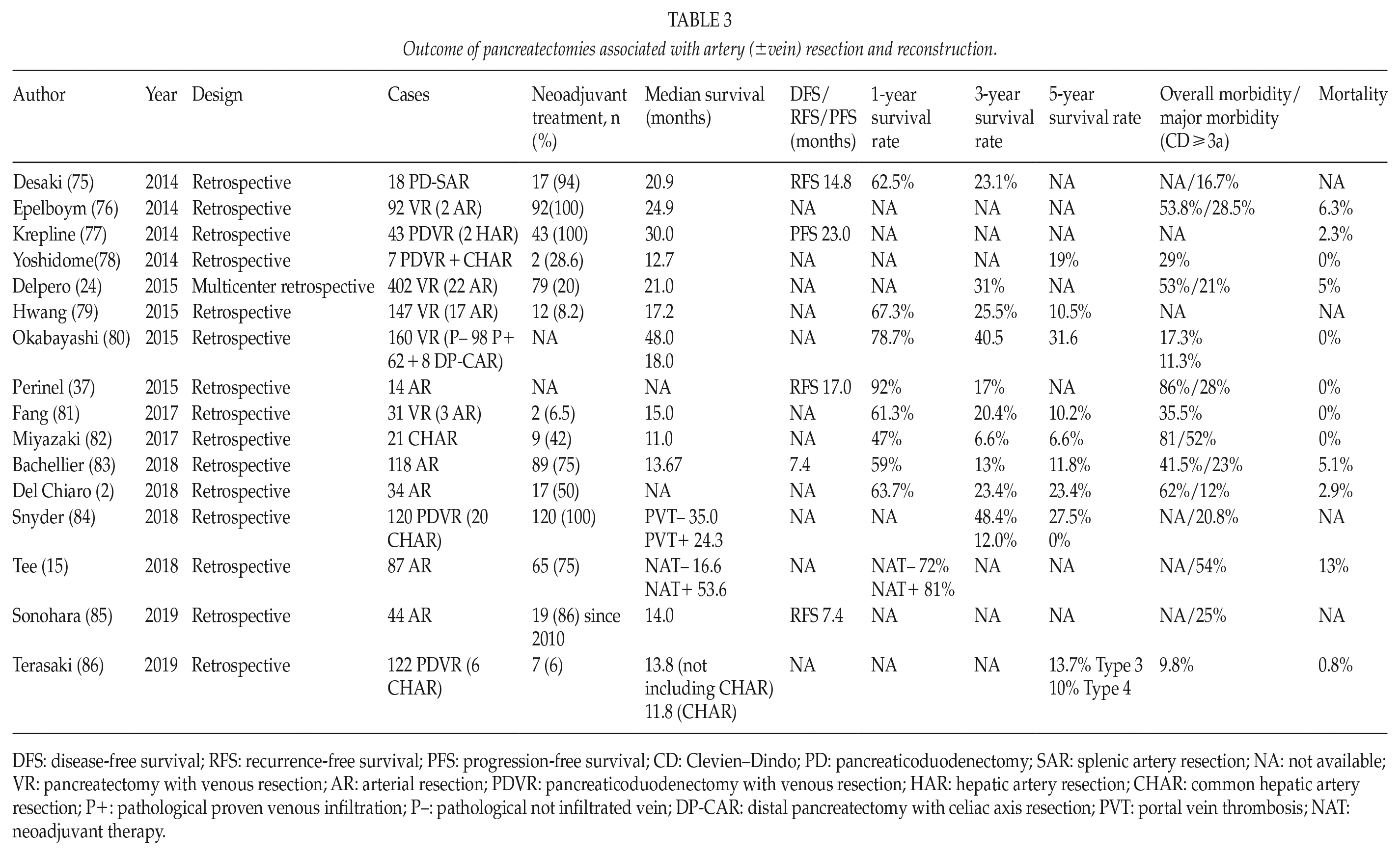
DFS: disease-free survival; RFS: recurrence-free survival; PFS: progression-free survival; CD: Clevien–Dindo; PD: pancreaticoduodenectomy; SAR: splenic artery resection; NA: not available; VR: pancreatectomy with venous resection; AR: arterial resection; PDVR: pancreaticoduodenectomy with venous resection; HAR: hepatic artery resection; CHAR: common hepatic artery resection; P+: pathological proven venous infiltration; P–: pathological not infiltrated vein; DP-CAR: distal pancreatectomy with celiac axis resection; PVT: portal vein thrombosis; NAT: neoadjuvant therapy.
Although survival rates for arterial resection are encouraging, certainly compared to systemic therapy alone, data regarding morbidity and mortality remain more controversial. Operative mortality rates reported in this group range from 0% to 13% and morbidity from 9.8% to 54% (Table 3). However, in 50% (6/12) of the studies, the postoperative mortality rate was below 1%. This variability of results likely represents different surgical techniques and approaches as well as reflecting aggressiveness in treating locally advanced disease (87). There does not appear to be any reason to believe that complex vascular reconstruction should significantly increase the peri-operative risk. In fact, looking at the results of transplant surgery where, at least two vessel reconstructions (artery and vein), are always performed, the vascular complications rates are very low (88). Marked improvements in systemic therapy have increased surgical indications for treating PDAC, even in cases that require artery, or combined artery and vein resection. However, it is also clear that these procedures should only be done in high-volume centers with specific experience in combined arterial–vein resection for PDAC.
Indications for Surgery After Nat
Improved systemic therapies have complicated preoperative determination of indications for surgical treatment of locally advanced PDAC. The rate of radiological response to the best current chemotherapy (FOLFIRINOX) for PDAC is approximately 25%. In the majority of patients (69%), the disease remains radiographically stable; approximately 6% have radiologic progression during chemotherapy (89). However, pathological response ranges from complete to moderate and can be observed in up to 77% of patients treated (90). These data clearly show that radiology after NAT can only assess progression of disease but not response to chemotherapy. In fact, in a recent observational study, Ferrone and colleagues showed that 92% of patients who underwent surgical exploration with an “unresectable” disease as determined by a post-therapy staging CT (receipt of FOLFIRINOX) are able, with to achieve an (R0)resection with an appropriate “radical” operation (91). These data suggest that after NAT, criteria formerly used to define resectability are inadequate, if not inaccurate. Even the technical criteria (i.e. a tumor that infiltrates the aorta by initial CT findings) should no longer be a complete contraindication to surgery as radiographic imaging cannot differentiate viable tumor from fibrous change post treatment. Consequently, the term “unresectable” tumor should no longer be used except for the presence of metastatic disease or rare technical conditions (i.e. presence of a complete thrombosis of the PV/SMV without margins for reconstruction). Post neoadjuvant radiologic staging, should strongly consider replacing the term—tumor with the more accurate description mass or abnormal tissue. Further radiologic technique cannot asses biologic stability, but only stability in the size of a mass.
This point is crucial for the treatment of PDAC in the new era of NAT. Considering that from 2001 to 2015 there were reported 254,200 new cases of PDAC in the United States and assuming that 30% of them were considered unresectable although there was no evidence of metastatic disease at the time of diagnosis, it may be that the problem of inaccurate re-staging is potentially applicable to 76,260 Americans patients in this interval of time (92). Assuming that all these patients got NAT, we know from the literature data that only 25% of them (in the best case scenario) would show a radiological response to the treatment. Even if one assumes that all patients with a radiological response (19,065 patients) are taken to surgery based on previous interpretations 52,619 patients would not have been explored to assess tumor viability (89). Knowing that with receipt of NAT, 77% of patients will have significant if not complete pathologic response (90). It is possible that more than 40,000 patients in that interval of time were denied a potentially curative surgery (Fig. 1).
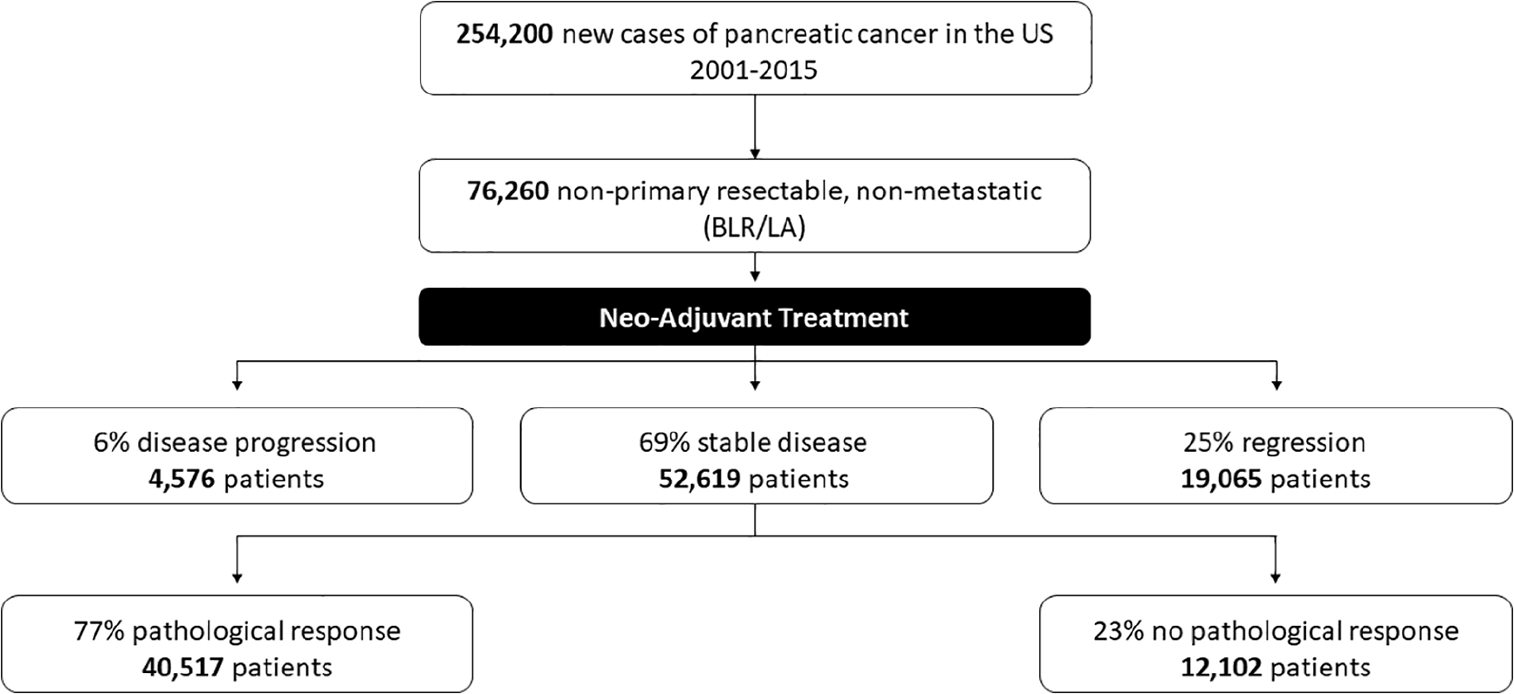
Were overstaged and therefore not considered surgical candidates.
The current absence of clear radiological criteria to define resectability in PDAC after NAT, underlines once more the great necessity to define new and more reliable clinical and biological criteria for surgical exploration of patients affected by borderline resectable and locally advanced PDAC. Although CA 19-9 has been proposed as a marker able to predict the response to chemotherapy, a significant percentage of population does not express this marker. Recently, it has been shown that despite the CA 19-9 level, surgical outcomes are superior to palliative care (93).
Conclusion
In the era of more effective NAT, many things need to be re-evaluated in the management of patients affected by PDAC. This is a systemic disease. In the past and currently, all the resectability criteria in non-metastatic PDAC are focused on local anatomical factors. However, what probably makes the difference in survival is systemic control of the disease. New data showing a significant improvement of long-term outcome of surgery in patients affected by locally advanced PDAC are not reflecting an improvement in surgical technique, but the development of new and more effective chemotherapies (2, 15, 94). Looking deeper data from the current literature, there is no evidence that the different local involvement of vessels reflects a different survival. Recently, Rangelova et al. (93) showed no difference in long-term survival between patients, treated with NAT, affected by borderline resectable or locally advanced PDAC. Van Roessel et al. (95) also showed that the T stage alone was not a prognostic factor in PDAC survival. Unfortunately, the limits of radiology in defining the “real responders” after chemotherapy in PDAC remain a significant problem in defining true candidates for surgical exploration. With limitations related to the theoretical calculations done using different studies, in Fig. 1, we offer a picture of the concrete risks of undertreating patients after NAT. The numbers in the figure are not “real,” but just an extrapolation done using available data regarding radiological and pathological response to chemotherapy. It is not an uncommon experience to have cases where radiology stated that PDAC is stable yet pathologic examination shows a significant response. Looking at these data, surgical exploration seems to be an appropriate option to be offered to every patient with a radiographically stable tumor after NAT and in good physical conditions. This approach will clearly expose some patients to unnecessary exploration or even overtreatment; however, it is our opinion that the morbidity of this approach can be managed and the alternative to non-surgical care is unfortunately tumor progression. At this point, CA 19-9 and positron emission tomography (PET) scan have been proposed as useful tools to re-stage patients after NAT; genetic differences in patients who do not produce CA 19-9 and technical issues with PET scanning will limit these options in appropriate surgical decision making (93, 96).
However, looking the outcome of PDAC surgery, the anatomical classification we are using today to define who should or should not receive surgery, seems to be misaligned with the biology of the disease. Even today, independent of the T stage, a significant number of patients affected by PDAC die within the first year from surgery (95). This occurs in primarily resectable cases, in borderline resectable and in locally advanced cases. We also have proof that the rate of local recurrence is similar in these groups of patients (9). Therefore, the problem is not the role of vascular resections in PDAC, but the role of surgery in PDAC.
In an era where the medical treatment has improved significantly, we believe that we should shift from anatomical classification of resectability to a more prognostic and biological classifications. There are probably primary resectable PDAC with bad biology that should never receive surgery and, in contrast, locally advanced cases, with good biology, that should be treated with aggressive surgical operations. In other words, we should invest in defining better prognostic, patients-related, and biological criteria more useful to select the best candidates for surgery, independent by the T stage of the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.