
Abstract
Background and Aims:
The interpositional arthroplasty was developed to retain foot function and to relieve pain due to the arthritis of the first metatarsophalangeal joint. The bioabsorbable poly-L-D-lactic acid RegJoint® interpositional implant provides temporary support to the joint, and the implant is subsequently replaced by the patient’s own tissue. In this study, we retrospectively examined the results of the poly-L-D-lactic acid interpositional arthroplasty in a 9-year follow-up study among patients with hallux valgus with end-stage arthrosis or hallux rigidus.
Material and Methods:
Eighteen patients and 21 joints underwent interpositional arthroplasty using the poly-L-D-lactic acid implant between February 1997 and October 2002 at Tampere University Hospital. Of these, 15 (83.3%) (21 joints) patients were compliant with clinical examination and radiographic examination in long-term (average 9.4 years) follow-up. The mean age of the patients was 48.3 (from 28 to 67) years at the time of the operation. Six patients underwent the operation due to arthritic hallux valgus and nine patients due to hallux rigidus.
Results:
The mean Ankle Society Hallux Metatarsophalangeal–Interphalangeal Scale and visual analogue scale (VAS) for pain scores improved after the operation in all patients. The decrease of pain (visual analogue scale) after the operation was statistically significant (77.5 vs 10.0; p < 0.001). Postoperative complications were observed in 3 (14.3%) joints of two hallux rigidus patients. For these patients, surgery had only temporarily relieved the pain, and they underwent reoperation with arthrodesis.
Conclusion:
In conclusion, interpositional arthroplasty using a poly-L-D-lactic acid implant yielded good results. This study indicates that the poly-L-D-lactic acid interpositional implant may be a good alternative for arthrodesis for treatment of end-stage degeneration of the first metatarsophalangeal joint.
Keywords
Background and Aims
Hallux valgus (HV) is a common chronic foot complaint, and hallux rigidus (HR) is the most common degenerative arthropathy of the foot (1, 2). The term HV describes the situation wherein the first metatarsophalangeal (MTP-1) joint is in malposition. The malposition forms when the first metatarsal rotates to valgus and turns to abduction, and this malposition can lead to MTP-1 degeneration. HR of the MTP-1 joint is a common arthritic condition that affects the big toe leading to a restricted and painful motion at the MTP-1 joint (1). Since the etiology is not the same, it is challenging to select the appropriate surgical method to correct arthritic HV and HR and to avoid the shortening of the first ray (1, 3).
A variety of surgical techniques for the treatment of arthritic HV and HR are described in the literature (2, 4). Keller performed the first resection interpositional arthroplasty, and Brandes performed the first resection in the proximal phalanx and inserted a part of the medial joint capsule into the joint to serve as a pillow (5). However, it is well known nowadays that resection arthroplasty carries a high risk of postoperative metatarsalgia due to the instability and poor function of the MTP-1 joint. Therefore, there is a need to research new techniques that will retain the mobility of the MTP-1 joint after HV or HR surgery (6).
Interpositional arthroplasty was first developed to retain foot function and to eliminate pain (7, 8). The purpose of the technique is to maintain MTP-1 mobility while at the same time stabilizing the varus–valgus movement of the joint and retaining the length of the toe. Several modifications have been used for interpositional arthroplasty, including the MTP-1 joint capsule, the extensor hallucis brevis (EHB), the flexor hallucis longus, the plantaris and the gracilis tendons, and the bioresorbable implant. To date, however, there is no clear evidence or studies to compare different techniques, so there are no golden standard for interpositional arthroplasty (9).
A bioabsorbable poly-L-D-lactic acid (PLDLA) RegJoint® interposition implant has been developed at Tampere University of Technology (10). The porous implant provides temporary support for the joint, and it is designed to be replaced later by the patient’s soft tissue ingrowth to allow a gradual optimized replacement of the implant with fibrous tissue, providing a flexible, but durable, pseudojoint (10). The support provided by the implant is preserved for more than 2 months, and it takes between 2 to 3 years before the implant is fully replaced by own tissue (11). In this retrospective study, we examined the results of the PLDLA interpositional arthroplasty in a 9-year follow-up study among patients with HV with end-stage arthritis of the MTP-1 or HR.
Material and Methods
Eighteen patients underwent interpositional arthroplasty using the PLDLA implant (16, 18, or 20 mm) between February 1997 and October 2002 at Tampere University Hospital by five experienced foot and ankle surgeons. Of these 18 patients, 15 (83.3%) were compliant with clinical examination and radiologic assessment in long-term (average 9.4 years) follow-up. Six patients underwent bilateral operation; hence, the study comprised 21 joints. Twelve of the patients were female, and three were male. The mean age of the patients was 48.3 (from 28 to 67) years at the time of the operation. Six patients underwent surgery due to arthritic HV and nine patients due to HR.
Patients were controlled at a follow-up visit 9 years after the operation. Physical function was evaluated using the American Orthopedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal scale (AOFAS). Preoperative AOFAS scores were collected from patients’ medical histories. Pain was evaluated using the visual analogue scale (VAS) from 0 to 10, where a higher number indicates higher pain and vice versa. The pain VAS was obtained before surgery and at the time of the follow-up visit. Furthermore, the palpation of the joint was clinically estimated, and any tenderness and swelling were recorded. The symptoms and findings were classified into four groups: no symptoms, slight symptoms, moderate symptoms, and substantial symptoms.
Plain radiographs were obtained from every patient, and the images were analyzed (anteroposterior, oblique, and lateral views) by a radiologist. The radiologist estimated the state of the joint, as no radiological classification exists for operations involving the bioabsorbable PLDLA interpositional implant.
Clinical and sosiodemographic data are presented as means with ranges or as counts with percentages. Means of the paired continuous variables were compared with Wilcox test. Confidence interval was determined at 95%, and therefore p values of <0.05 were considered to be statistically significant. Statistical analysis was performed using IBM© (Armonk, New York, U.S.) SPSS Statistics, version 22 software.
HV Technique
Six patients with seven joints were operated due to end-stage arthritic HV. The operations were performed through a dorsal or dorsomedial longitudinal incision. The capsule was then released and opened. The osteophytes were removed if needed. The bone resection was performed to base of proximal phalanx in four cases and to first metatarsal head in two cases, and in one case, the both sides were resected. The PLDLA implant was fixed in three joints with absorbable sutures through holes in the bone. In four joints, implants were inserted in the joint space without fixation. Bunionectomy was done in three and adductor tenotomy in four cases. Additional procedure of the second toe was performed in two cases.
HR Technique
Nine patients and 13 joints were operated due to HR. The approach and the opening of the capsule were the same as used in the HV technique. To create an adequate space for interposition implant, bone resections were made for all patients. Resection of the base of proximal phalanx was performed in 10 cases; first metatarsal head in five cases, and in one case, the both sides were resected. Bunionectomy was done in seven joints.
The average postoperative immobilization time was (range) 23.7 (from 2 to 42) days. Postoperative regimen varied considerably; most patients used orthosis or postoperative shoe for 2–6 (average 3) weeks.
Results
The mean AOFAS score and pain VAS improved after the operation in all patients (Table 1). The improvements were most notable in the Pain and Function subscales. All examined patients reported that the joint felt better than before the operation. The decrease of pain (VAS) after the operation was statistically significant (10.0 vs 77.5, p < 0.001).
Direct comparison between the preoperative and postoperative AOFAS score and its subscales together with pain VAS.
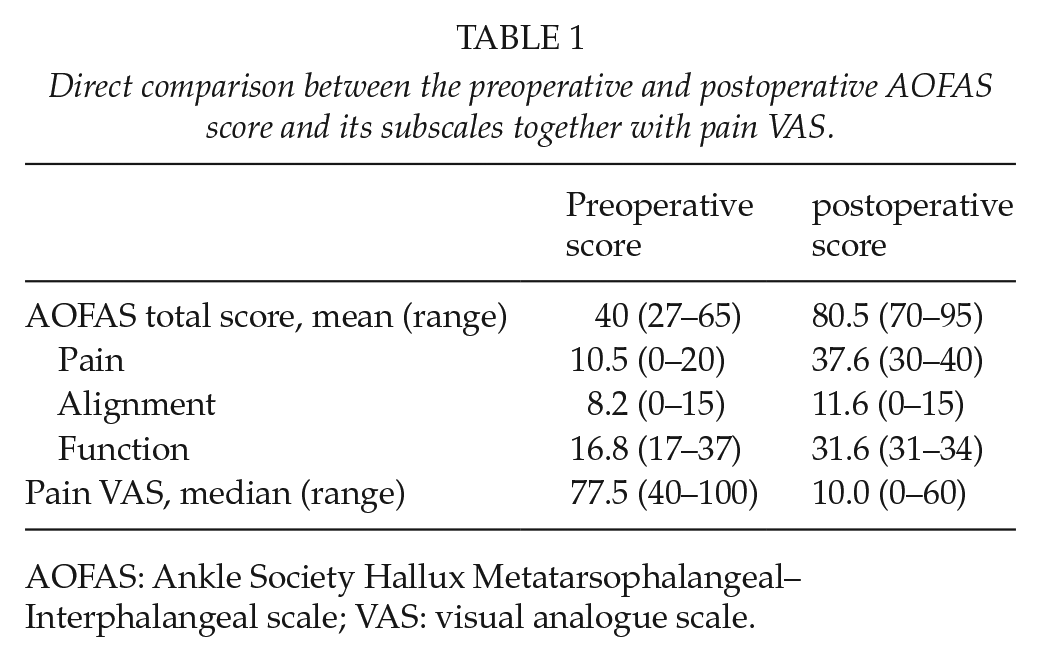
AOFAS: Ankle Society Hallux Metatarsophalangeal–Interphalangeal scale; VAS: visual analogue scale.
The radiological findings are shown in Table 2. The radiological findings were contradictory, since the radiographs contained multiple pathological features, yet most of the patients were painless. Osteophytes and articular space narrowing were detected in all joints. Two joints included intra-articular loose bodies and none of the patients had congruence.
Radiological findings of patients with PLDLA implant.
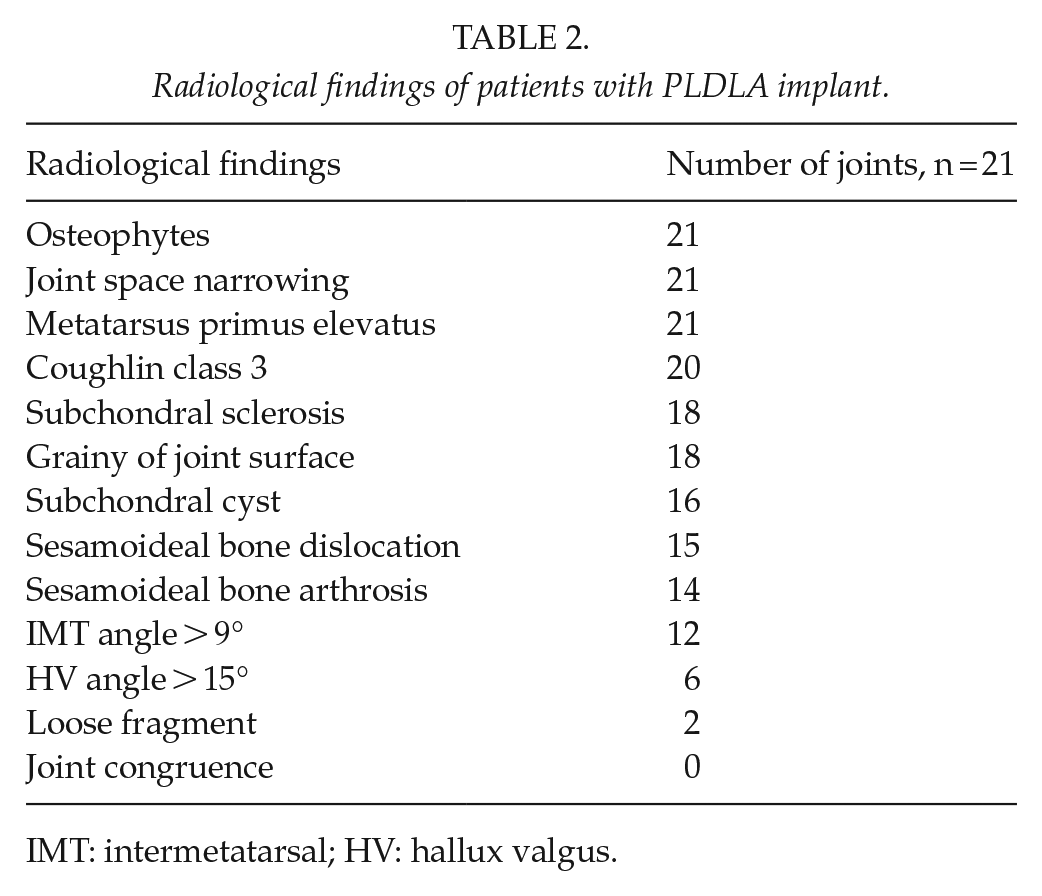
IMT: intermetatarsal; HV: hallux valgus.
The patients were evaluated at an outpatient clinic, and the symptoms and findings were classified into four classes: (1) no symptoms, (2) slight symptoms, (3) moderate symptoms, and (4) substantial symptoms. In total, 18 joints were considered to be Class 1 and 3 joints to be Class 2. None of the joints were considered to be Class 3 or 4. Swelling was not observed in 18 joints, swelling was moderate in 2 joints, and swelling was substantial in 1 joint.
Postoperative complications occurred in 3 (14.3%) joints of two HR patients. For these two patients, surgery had only temporarily relieved the pain, and they underwent reoperation with arthrodesis of the MTP-1 joint.
Discussion
To the best of our knowledge, this study is the first clinical evaluation of long-term results (average 9.4 years) of MTP arthroplasty using a PLDLA interpositional implant. Results show that the operations reduced pain and that patients were satisfied with the improved range of motion (ROM) of the MTP-1 joint in long-term follow-up.
Tiihonen et al. (12) reported 1-year results after PLDLA implant for lesser MTP joint interpositional arthroplasty for rheumatoid forefoot deformities. They reported no significant differences when conventional metatarsal head resection (MHR) and PLDLA implant were compared (12). Moreover, a recent study by Horita et al. (13) also reported good results after MHR and joint-preserving technique. However, it is currently known that distal metatarsal resection can cause metatarsalgia and lead to postoperative deformities. Still, studies have shown no significant differences between these two techniques (14, 15). Furthermore, multiple previous studies have concluded that the interpositional technique may lead to postoperative metatarsalgia (16–19). The PLDLA implant was initially developed to retain joint movement and to avoid postoperative deformities caused by the formation of loose connective tissue inside the joint (20). Tiihonen et al. (12) did not report any deformities or metatarsalgia in 1-year follow-up. Our 9-year case series did not show similar problems as those seen in the Brandes–Keller procedure in long-term follow-up (6). In this study, the bone resections were performed in both sides of phalangeal and metatarsal bones or only metatarsal, depending on the arthritis of the bones. According to our results, we cannot compare our technique with the Brandes–Keller procedure, yet it seems that there might not be similar problems with postoperative metatarsalgia or deformities with PLDLA implant.
Multiple graft techniques, including autogenous fascia lata, gracilis autograft, tendon allograft, amniotic membrane graft, collagenous tissue matrix, meniscal allograft, and synthetic hydrogel cartilage matrix, have all been described for MTP-1 interpositional arthroplasty with favorable outcomes (7, 21–23). Complications associated with the interpositional arthroplasty technique may include shortening of the first ray, lesser metatarsalgia, and weakness with hallux plantarflexion (24). In 2003, Coughlin and Shurnas (21) published a retrospective review, and they found that interpositional arthroplasty with gracilis tendon bundle in the MTP-1 joint increased the pressure under the second metatarsal head after 4 years average follow-up. The results of this study showed that there were no signs of problems affecting the lesser metatarsals. Lau and Daniels (25) retrospectively compared cheilectomy with a capsular interpositional arthroplasty technique involving the use of an EHB tendon graft. They reported complications that included asymptomatic callus (27.3%), postoperative weakness of the great toe (72.7%), and metatarsalgia (27.3%) (25).
Berlet et al. (7) reported good short-term results with a regenerative tissue matrix without wound healing problems, infections, inflammatory reactions, instabilities, malalignments, or loss of push-off strength at 12.7 months average follow-up. They also reported that the average postoperative AOFAS scores of the same cohort were 65.8 (range: 58–68) with notable pain relief and preserved foot function at 5 years follow-up (26). The preoperative AOFAS were 38 (range: 34–43). All patients reported that their surgery had been successful at a mean 5-year follow-up (26).
The MTP-1 joint arthrodesis is a common procedure for the treatment of arthritic HV and end-stage HR of the MTP-1 joint, and nowadays it is even considered to be the golden standard procedure. However, the procedure has several drawbacks, such as loss of ROM in the MTP-1, failure of fixation, nonunion, malunion, and transfer metatarsalgia (27). A recent prospective randomized multicenter trial did not report any differences between the interposition arthroplasty of a synthetic hydrogel cartilage matrix and the primary arthrodesis of the MTP-1 joint (28). The interpositional technique offers a ROM sparing alternative for the treatment of arthritic HV and end-stage HR of the MTP-1 joint. Interpositional arthroplasty also reserves the option for later arthrodesis (29).
The PLDLA implant has shown to induce osteolysis, which explains the findings in the follow-up radiographs (30). Nevertheless, these radiological changes are thought to be part of the process of hydrolysis (31). Honkanen et al. (30) showed in their study that osteolytic changes in PLDLA implant were minor. There is a controversial view that these osteolytic changes in bioabsorbable materials could lead to infection or nonunion (31, 32). The absorbable interposition implants, acting as joint spacers will be simultaneously replaced by ingrowing fibrous tissue. This process of absorbable implants could explain these radiological manifestations like grainy of joint surface and subchondral cysts (Figs 1 to 3). Mattila et al. recently reported high rate of adverse tissue reactions related to the degradation process of the PLDLA interposition implant for trapeziometacarpal osteoarthritis arthroplasty. Although, end of their 3 years follow-up when degradation process settle down, there were no signs of ongoing adverse tissue reactions (33). In our clinical study, we did not find any adverse tissue reactions which emerge out in clinical aspect.

Postoperative X-ray.

6 months after operation.

2 years after operation.
To date, there are no high-quality level-I studies comparing the outcomes of interpositional arthroplasty with other techniques to treat arthritic HV and HR. In this study, the sample size of 15 patients (21 metatarsophalangeal joints) was quite small. However, other studies have had comparable sample sizes (7, 12, 34). Another limitations of this study are retrospective design and the lack of preoperative evaluation with patient-reported outcome measures. The strength of this study, however, is a long follow-up time compared to other studies. The interpositional technique may be performed on young and active patient with advanced HR or HV with arthritis, to preserve the ROM of the MTP-1 joint. Interpositional arthroplasty using a bioabsorbable PLDLA implant should be studied in future in a prospective, randomized controlled study setting.
In conclusion, the results of this study on interpositional arthroplasty using a bioabsorbable PLDLA implant were generally good. Only two patients went to secondary surgery. This study indicates that the PLDLA interpositional implant is a good alternative for MTP-1 joint arthrodesis. The findings of this study show decreased pain and increased patient satisfaction after 9 years follow-up. The results of our study indicate that the interpositional arthroplasty using PLDLA implant is a safe technique to be evaluated in the future with randomized controlled study setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.