
Abstract
Introduction:
Few reports encompass the treatment of first metatarsophalangeal joint (MTPJ) arthritis complicating hallux valgus. Indeed, in the literature, there is a lack of guidance concerning the management of patients affected by mild to moderate first MTPJ arthritis complicating hallux valgus. The aim of this study is to present the mid-term results of an original joint-preserving surgical technique.
Materials and Methods:
A group of 50 patients (60 feet) affected by mild to moderate first MTPJ arthritis complicating hallux valgus who underwent modified Giannini’s SERI (simple, effective, rapid, inexpensive) surgical procedure were prospectively reviewed. They were clinically and radiographically evaluated preoperatively and after surgery and were also assessed using the American Orthopedic Foot and Ankle Society (AOFAS) score and Coughlin and Shurnas classification. The average follow-up was 38 months. A multivariate analysis was performed to evaluate the existing relationship between postoperative AOFAS results and radiological preoperative measured angles and sesamoid grade of dislocation.
Results:
The average AOFAS score significantly improved at last follow-up to an average of 90.5 ± 14.5, while preoperatively it was 45.6 ± 15.3 (p < 0.001). On multivariate analysis, a statistically significant correlation resulted among all the radiographic preoperative registered parameters and clinical postoperative results. However, it was shown that any radiological parameter alone could not predict a better clinical recovery.
Conclusions:
The surgical technique proposed here could extend the indications of the SERI procedure to those patients affected by mild to moderate hallux valgus combined with mild to moderate osteoarthritis.
Introduction
Over the years, many studies have described various techniques for hallux valgus correction, involving distal or proximal first metatarsal osteotomy and soft tissue procedures. 1 –3 Each technique is characterized by a different surgical approach, osteotomy design, and fixation device. Most surgical techniques are associated with good outcomes in above 80% of cases, but no technique is considered to be entirely satisfactory or superior to the others. 1
Distal metatarsal osteotomies are preferred to correct mild to moderate hallux valgus deformities. 3 In 1998, a new technique to treat hallux valgus was described by Giannini et al. 3,4 They defined this approach as: “simple,” “effective,” “rapid,” and “inexpensive” (SERI). Following Giannini’s inclusion and exclusion criteria, this technique is performed in our institution. Although the SERI technique is a valid surgical approach, it is not recommended for all hallux valgus deformities. Indeed, Giannini et al. report specific exclusion criteria which include, among others, arthritis of the first metatarsophalangeal joint (MTPJ) up to grade 2 according to the Regnaud classification. 5,6 In addition, the presence of osteoarthritis has been mentioned as a contraindication to joint-preserving surgical procedures for the correction of hallux valgus. 7
Arthritis of the first MTPJ associated with hallux valgus is a well-known disease, although its pathogenesis is not completely understood. 8 –10 It arises from a preexisting hallux valgus deformity and increasing incongruity of the first MTPJ. 9 Symptoms range from mild to disabling. However, few reports encompass the treatment of arthritis of the first MTPJ complicating hallux valgus. 11,12 Primarily, the literature includes three kinds of nonjoint-preserving surgical procedures, implant arthroplasties, resection arthroplasties, and arthrodesis of the first MTPJ, regardless the stage of joint degeneration. 11,12 In fact, in the literature, there is a lack of guidance concerning the management of patients affected by arthritis of the first MTPJ at grade 1–2 of the Coughlin–Shurnas scale 13 complicating hallux valgus. In the population analyzed in the current study, a group of selected patients are identified in which mild to moderate arthritis (grade 1–2) of the first MTPJ complicates a condition of chronic hallux valgus.
The aim of this study is to present the mid-term results of an original joint-preserving surgical technique to correct the deformity and reduce pain in these patients.
Methods
Inclusion criteria and patient population
A group of 50 consecutive patients (60 ft) who underwent modified Giannini’s SERI surgical procedure was prospectively reviewed. The study was authorized by the ethical committee of the institution. All these procedures were performed by the senior author between January 2008 and April 2011. The inclusion criteria were (1) mild or moderate hallux valgus with hallux valgus angle (HVA) <40° 14 and an intermetatarsal angle (IMA) ≤20°, 14 (2) arthritis of the first MTPJ of grade 1–2 of the Coughlin–Shurnas classification (29% grade 1, 71% grade 2). 13 The exclusion criteria were (1) history of rheumatoid arthritis or other inflammatory diseases, (2) diabetes mellitus, (3) neurological disorders, (4) prior hallux surgery, (5) hypermobility of the first MTPJ or first cuneometatarsal joint (in patients affected by generalized ligamentous laxity), (6) arthritis of the first MTPJ above grade 2 on the Coughlin–Shurnas scale, and (7) clinically irreducible deformity of the first MTFJ. The patients were 46 women and 4 men. Mean age was 59.2 years (standard deviation: 12.4 years), minimum 51 and maximum 75. All the patients but two were evaluated at final follow-up (total feet: 58).
Surgical technique
Planning of the operation was performed by the senior author in terms of the obliquities of the bone cut, the extent of the medial-lateral or dorsal-plantar dislocation of the metatarsal head and the correction of the distal metatarsal articular angle (DMAA), as reported by Giannini. 3 –6
Surgery was performed using a tourniquet and under regional anesthesia, with patients in the supine position. The average surgical time was 12 min (ranging between 10 and 18 min). In 28 cases, surgery of the lesser toes was also performed.
The approach was medial, above the medial eminence, between the plantar and dorsal skin, to avoid injury of the digital nerve. The incision was full-thickness, involving skin, subcutaneous tissue, and the capsular layer (Figure 1). The medial eminence was freed, respecting the entry points of blood vessels at the first metatarsal neck level. The proximal medial aspect of the first phalanx was also freed, thereby exposing the metatarso-sesamoid joint. A periosteal elevator was used in order to release the “glued” sesamoids and the labrum (plantar release; Figure 1). By penetrating with this instrument, the first intermetatarsal space was reached. Transection of the lateral metatarso-sesamoid suspensory ligament and release of the lateral capsule (usually retracted) were performed, using a small curved periosteal elevator, passing under the metatarsal head and reaching the first intermetatarsal web space. Using an oscillating saw, the medial prominence was removed, taking care to spare the sulcus in order not to destabilize the first phalanx. Any dorsal osteophytes were excised. A portion of the medial capsular tissue was dissected from both sides of the previous capsular cut. The residual medial capsule was then tightened to the correct tension and the hallux maintained in the corrected position using two crossed stitches in long-lasting reabsorbable suture (Vycril™ No. 1; Figure 2). Then the neck of the first metatarsal bone was freed and exposed, proximally to the entry points of blood vessels, at the level of the next bone cut. All the above-mentioned steps are the modifications to the SERI technique. The following surgical steps overlap Giannini’s SERI technique as described 6 (Figure 3). A dressing was then applied.

The approach is strictly medial. A periosteal elevator is used to release the “glued” sesamoids and the labrum.

The residual medial capsule is tightened to the correct tension and the hallux is maintained in the corrected position using two crossed stitches.

The neck of the first metatarsal bone is freed and exposed and the osteotomy is performed using a pneumatic saw.
All patients were discharged the same day or that following surgery, depending on their pain. Ambulation was allowed immediately using postoperative Talus shoes. Foot elevation was advised for when the patient is at rest, as prophylaxis against venous thromboembolism. After 30 days, the dressing, the suture, and the Kirschner wire were removed. Progressive rehabilitation through passive and active exercises, cycling, and swimming was advised. Comfortable shoes were prescribed and gradual recovery of normal walking was encouraged, depending on the swelling.
Clinical and radiological evaluation
At preoperative assessment, all the patients complained of pain, stiffness, and limitations in wearing shoes. They were clinically and radiographically evaluated preoperatively, 1, 3, and 6 months after surgery, yearly and at final follow-up, by two researchers not involved in the surgeries. The average follow-up was 38 months, with a range from 24 to 60 months. The clinical evaluation included an assessment of the severity of the prominent medial eminence and the reducibility of the deformity. The latter was tested by pushing laterally on the head of the first metatarsal bone and simultaneously pulling the first toe medially. Soft tissue conditions such as bursitis were also assessed. At the same time, all the deformities affecting the lesser toes and the stability of the other MTPJs were evaluated. For each patient, the Hallux-Metatarsophalangeal-Interphalangeal Scale proposed by the American Orthopedic Foot and Ankle Society (AOFAS; see Table 1) was used. 15,16 Through radiographic examination (including dorsoplantar and lateral view standing radiographs of the forefoot), the congruency of the first MTPJ, the other MTPJs, the HVA, the IMA, and the DMAA were assessed for each patient, according to the guidelines of the AOFAS ad hoc Committee on Angular Measurements 17 (Table 1).
Clinical and radiological data of all the cases.

PRE A: preoperative AOFAS (…/100); POST A: postoperative AOFAS (…/100); PRE H: preoperative HVA (radiological angle); POST H: postoperative HVA (radiological angle); PRE D: preoperative DMAA (radiological angle); POST D: postoperative DMAA (radiological angle); PRE I: preoperative IMA (radiological angle); POST I: postoperative IMA (radiological angle); PRE S: preoperative sesamoids evaluation; POST S: postoperative sesamoids evaluation; AOFAS: American Orthopedic Foot and Ankle Society; HVA: hallux valgus angle; DMAA: distal metatarsal articular angle; IMA: intermetatarsal angle.
Moreover, in the dorsoplantar view, the grade of dislocation of the sesamoids was identified using the methods recommended by the AOFAS committee 18 (Table 1).
For all the above-mentioned parameters, a standard deviation was calculated (Table 1).
In accordance with the Coughlin and Shurnas classification, 13 for each patient, the preoperative range of dorsiflexion was stated and recorded, thereby distinguishing the grade of pain and stiffness, and the radiographic grade of degenerative arthritis of the first MTPJ. All these preoperative scores were compared with data collected at final follow-up.
Following a 3-month period after surgery, each radiographic feature and the healing status of the osteotomies was assessed by two independent observers not involved with either surgery or postoperative care, and when opinion differed among the two observers, a combined assessment was performed and agreement was reached. Intraoperative, early and late postoperative complications were also recorded for each patient. During the follow-up, an accurate radiographic analysis was performed in order to check possible cases of nonunion, delayed union, and malunion of the osteotomy or osteonecrosis of the metatarsal head. HVA ≥20° was considered an under-correction. HVA ≤0° was considered an iatrogenic hallux varus. 11
Statistical analysis
A statistical analysis was performed using Statistical Package for the Social Sciences (IBM SPSS 20.0). All continuous data (HVA, IMA, and DMAA) are expressed in terms of the mean and standard deviation.
The univariate analysis Mann–Whitney U test was used to verify correlation between postoperative AOFAS and each radiological preoperative characteristic (preoperative measured angles and preoperative grade of osteoarthritis).
Moreover, a first multivariate analysis was performed including all preoperative radiological angles to test the predictive power for a worst clinical outcome (AOFAS).
Finally, a second multivariate analysis was completed to investigate the relation between preoperative and postoperative grade of arthritis and preoperative and postoperative radiological measured angles. For all tests, p < 0.05 was considered significant.
Results
The average AOFAS score significantly improved at last follow-up to an average of 90.5 ± 14.5 (minimum 48 and maximum 100), while preoperatively it was 45.6 ± 15.3 (minimum 17 and maximum 68) (p < 0.001). The mean HVA value decreased from 33.5° ± 4.4° (minimum 14° and maximum 38°) preoperatively to 12.7° ± 6.9° (minimum 3° and maximum 31°) at final follow-up (p < 0.001) with a mean correction of 22.9°. The mean IMA value decreased from 14.6° ± 2.5° (minimum 9° and maximum 20°) preoperatively to 6.9° ± 2.1° (minimum 3° and maximum 14°) at final follow-up (p < 0.001). The mean DMAA value decreased from 34.3° ± 9.6° (minimum 20° and maximum 58°) preoperatively to 9.6° ± 6.7° (minimum 4° and maximum 26°) at final follow-up (p < 0.001). The median sesamoids position was graded as 0.5 ± 0.6 at final follow-up, while preoperatively it was graded as 2.6 ± 0.5 (p < 0.001).
Preoperative evaluation of the arthritis component of the hallux valgus, performed using the Coughlin-Shurnas scale, 13 showed a grade 1 in 17 ft and a grade 2 in 41 ft, while final follow-up scores were grade 0 in 13 ft, grade 1 in 40 ft, and grade 2 in 5 ft (p < 0.001).
On univariate analysis, no relation was found between preoperative grade of osteoarthritis and the AOFAS results (p = 0.258). Instead, the other univariate analysis demonstrated that the cases with the worst preoperative measured radiological angles showed a higher frequency of the worst postoperative clinical results (postoperative AOFAS). In fact, a statistically significant correlation resulted among all the radiographic preoperative registered parameters (HVA, IMA, DMAA, and grade of dislocation of sesamoids) and the clinical postoperative results. However, on multivariate analysis, it was shown that any radiological parameter alone could not predict a better clinical recovery (Table 2). In fact, in this study, all investigated radiological parameters resulted in a significant correlation with the postoperative AOFAS. Therefore, it is important to stress that a surgeon should not focus attention on only one parameter in isolation, but that all radiological angles require the same attention. The other multivariate analysis demonstrated no relation between the preoperative and postoperative grade of arthritis and preoperative/postoperative radiological angles, showing that there is no relationship between arthritis grade and HVAs in the preoperative and postoperative period.
Multivariate analysis: Correlates radiological data with postoperative clinical results.
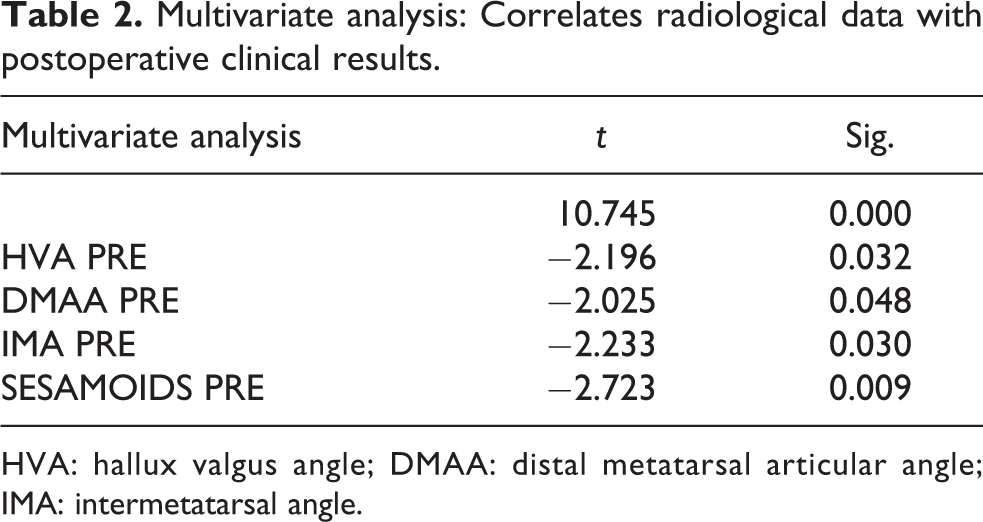
HVA: hallux valgus angle; DMAA: distal metatarsal articular angle; IMA: intermetatarsal angle.
Complications
Radiographic control at follow-up showed complete healing of the osteotomy with bone remodeling at the metatarsal bone. All but one osteotomy healed within 4 months postsurgery (Figure 4). In one case, there was an asymptomatic delayed union. At final follow-up (36 months), it had healed (Figure 5). No cases of nonunion occurred. No radiographic evidence of avascular necrosis of the metatarsal was observed. In two cases, there was an under-correction (see Table 1). In two cases, an inflammatory reaction at the cutaneous exit point of the K-wire was documented. In both cases, this clinical situation resolved a few days after K-wire removal. One patient was treated for the onset of deep vein thrombosis.

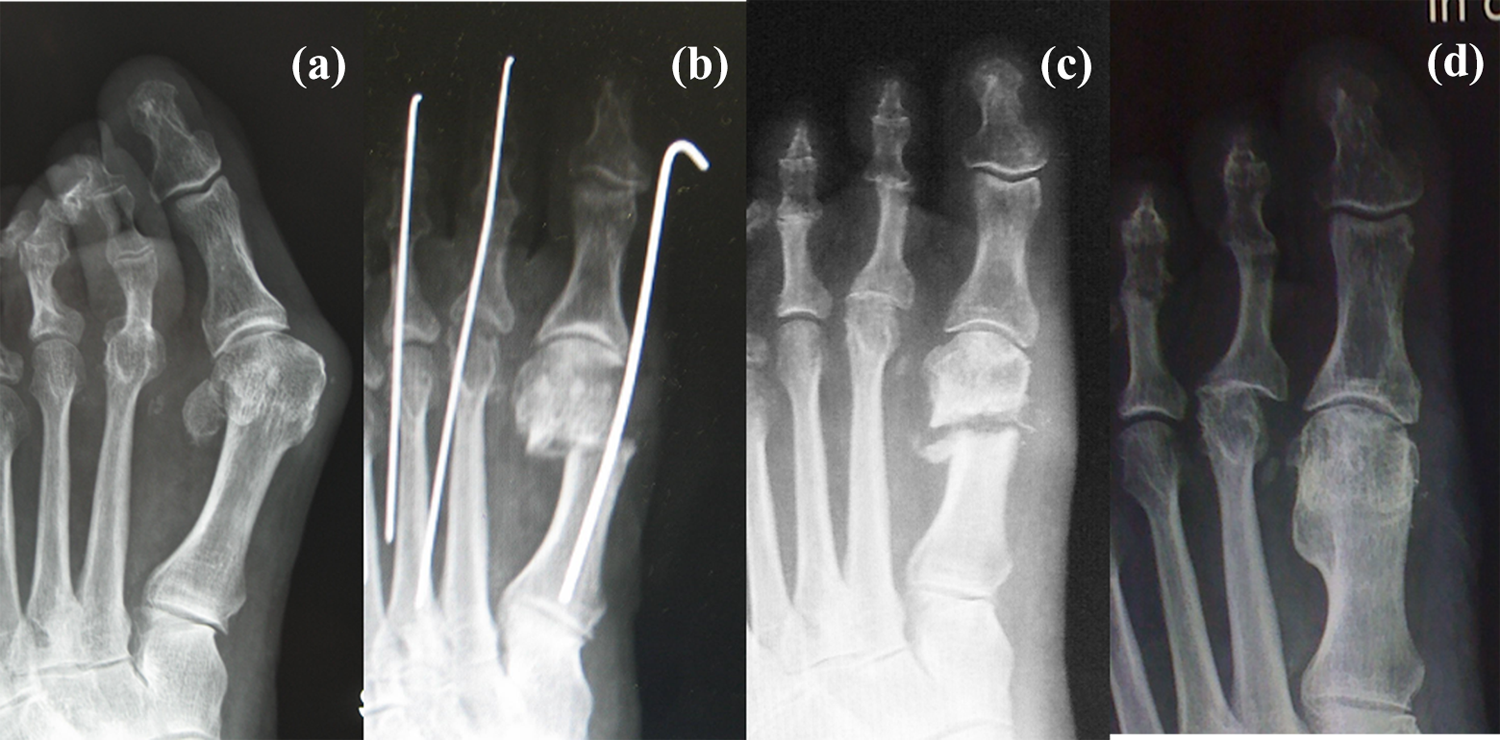
(a) and (b) Preoperative X-ray and clinical picture, showing hallux valgus combined with moderate arthritis of the first MTPJ. (c) Postoperative X-ray. (d) and (e) X-ray and clinical picture at final follow-up. MTPJ: metatarsophalangeal joint.
(a) Preoperative X-ray, (b) postoperative X-ray, (c) delayed union at 3 months postoperative, and (d) healing at final follow-up (36 months).
Discussion
Osteoarthritis combined with hallux valgus has been mentioned as a contraindication 7 to joint-preserving surgical procedures, although Sung et al. still report the preservation of the joint as paramount whenever arthritis is not advanced. 12 The options for management in patients affected by osteoarthritis combined with hallux valgus include implant arthroplasties, 19 resection arthroplasties such as Keller’s procedure, 10 Heuter–Mayo’s procedure, 20 or Regnauld’s procedure 21 and arthrodesis of the first MTPJ. 11,12 Implant arthroplasties have not been shown to produce better results than simple resection arthroplasty. 20 The reported satisfaction rate after an arthrodesis ranges from 85% to 95%. 11 Both resection arthroplasties and arthrodesis of the first MTPJ are not joint preservation procedures. They should be used in cases with hallux valgus associated with moderate to severe osteoarthrosis. 10,12
There is a lack of guidance in the literature concerning the management of patients affected by mild to moderate first MTPJ arthritis complicating mild–moderate hallux valgus. Kristen et al. described a correlation between a higher preoperative HVA and the postoperative AOFAS score. 15 The higher the preoperative HVA, the lower the postoperative score. The researchers could not provide any explanation for this trend. 22 Moreover, Giannini et al., observing the long-term outcomes of 896 ft treated using SERI, highlighted a significant correlation between the presence of preoperative degenerative arthritis and poorer clinical results at final follow-up, with worsening of stiffness. 6 An explanation could be that the worsening clinical outcome caused by the arthritic component in patients treated with “simple standard joint preservation correction procedures” is often considered as not significant, or unavoidable, or it is underestimated. Our surgical modifications to the SERI technique were directed at patients with mild to moderate arthritis complicating mild to moderate hallux valgus. The goal of the treatment was to relieve pain, to obtain a satisfactory correction of the deformity and to maintain or improve the first MTPJ range of motion (ROM). To correct the valgus component, we adopted the SERI technique that, as other kinds of distal metatarsal osteotomies, has been indicated in cases of mild or moderate deformity with an IMA up to 15°–20° and also in order to correct deformities characterized by deviation of the DMAA. 1,3,4
As regards the treatment of the arthritic component, we agree with Bock, Schneider, and Shereff’s considerations. 9,23,24 Although osteoarthritis of the first MTPJ is usually related to hallux rigidus, many cases of osteoarthritis actually result from articular incongruence. 9 With worsening of hallux valgus, clinical and radiological signs of osteoarthritis develop because of the increasing incongruity of the joint surfaces. 8 Shereff et al. 24 showed that kinematics are changed within all compartments in hallux valgus deformity. They stated that the MTPJs displayed irregularities in kinematic pattern compared with normal joints. The grade of joint degeneration within both the metatarsophalangeal and metatarso-sesamoid compartments was positively correlated with an increase of the HVA. Moreover, Bock et al. demonstrated that there are more early arthritic lesions within the metatarso-sesamoid compartment than within the metatarsophalangeal compartment. Their findings indicate that changes in the load pattern within the first MTPJ initially affect the metatarso-sesamoid compartment, both laterally and medially, and then the metatarsophalangeal compartment. They confirmed that the degree and extent of joint degeneration are clearly correlated with the degree of HVA. 9 As the sesamoids remain in place, the distal aspect of the first metatarsal shifts medially, losing its position and guidance on top of the medial and lateral sesamoids. 23 This leads to elongation of the medial ligamentous and capsular structures and consequently to shortening of the lateral soft tissue structures. This imbalance between medial and lateral soft tissue structures can be seen on plain dorsoplantar radiographs. It is caused by the development of an incongruous joint with shortening of the distance corresponding to the lateral collateral ligament and respective lengthening of the medial collateral ligament. 23 The shortening of the lateral suspensory ligament corresponds to the “sesamoid luxation” seen on plain dorsoplantar radiographs together with an elongation of the medial metatarso-sesamoid ligament. 23 All the above-mentioned studies suggest that incongruity of the first MTPJ is powered by soft tissue imbalance.
In accordance with Schneider, 23 we believe that distal soft tissue procedures combined with the osteotomy performed in hallux valgus deformities associated with mild/moderate arthritis cannot be considered as merely supplementary surgeries but rather are indispensable procedures to restore the physiological function of the first MTPJ. Therefore, the additional procedures we have adopted for the treatment of the arthritic component are addressed at a morphological and functional rebalancing of the first MTPJ and the first ray. Moreover, these avoid the recurrence of deformity caused by the failed reduction of the metatarsal head on the sesamoids. Indeed, in these cases, a “simple osteotomy” could lead to normalization of the IMA but would not restore the functional balance of the first ray. The imbalance is caused by the sesamoid bones, which maintain a dislocated position with respect to the metatarsal head. The modifications we have described are necessary to correct this situation. Reduction of the sesamoid luxation is only possible when the lateral metatarso-sesamoid suspensory ligament is transected. 23,25 On the one hand, the ligament must be transected completely to guarantee the expected effect, on the other hand, the plantar and proximal attachment of the articular capsule must be preserved to avoid disturbances of vascular supply to the metatarsal head. 26 In mild–moderate hallux valgus with grade 1–2 of osteoarthritis both sesamoids are misaligned in X-ray dorsoplantar view and “glued” on X-ray lateral view. Restoration of their correct balance with respect to the first ray also allows better functioning of the flexor tendons. This contributes to decreasing the risk of recurrency, under-correction, and further worsening of osteoarthritis. Closing the structures on the medial side should be tightened, while reducing and rebalancing the metatarso-sesamoid joint complex. Bunionectomy is necessary to reduce the medial prominence of the distal metatarsal head, thereby relieving the pain caused by foot-shoe impingement, even if the HVA/IMA is corrected. Bunionectomy cannot be performed using a simple SERI technique. Furthermore, our additional modifications allow the removal of osteophytes. This procedure is necessary, not only to improve the ROM but also to primarily reduce impingement and therefore pain. Viladot 27 also described soft tissue procedures combined with distal metatarsal osteotomy and a stabilization similar to the Kramer technique or SERI for correction of mild to moderate hallux valgus deformity, regardless of the coexistence of arthritis. In his surgical technique, he performed the correction of the hallux valgus before the soft tissue procedure. Conversely, we prefer to perform the soft tissue procedures first, because we believe that this sequence guarantees a better hold of stabilization. From our analysis, we documented a statistically significant difference between all pre and postoperative clinical and radiological parameters. However, with multivariate analysis, we showed that there are no radiological parameters which could alone predict a better clinical recovery.
We are aware of the limitations of this study. The first is the absence of a control group. The second relates to the small number of case reports. Both these limitations do not allow definitive conclusions. The third relates to the average final follow-up of 38 months. Although it is not a long-term follow-up, we affirm that the correction we have obtained should in any case be considered as stabilized. Indeed, we believe (and it is a common experience) that if a recurrence occurs, it is already present within 6 months after surgery and should rather be considered a failed correction or an under-correction. Our average final follow-up does not allow us to provide definitive data on the progression of the arthritic component. In fact, although our outcomes are excellent, and good in terms of no worsening of symptoms related to the arthritic component, we cannot affirm that our treatment is long lasting. We are aware that arthritic patterns are likely to worsen over the years. Nevertheless, by correcting not only the valgus deformity of the first MTPJ but also the balance of the metatarso-sesamoid joint complex (confirmed by a statistically significant improvement of the median sesamoid positions), we trust this worsening could be asymptomatic for a longer interval or, in any case, less disabling.
Conclusions
The surgical technique we have proposed could extend the indications of the SERI procedure to those patients affected by mild to moderate hallux valgus combined with mild to moderate osteoarthritis. However, we deem further studies to be necessary, to analyze this issue in detail and confirm or refute our hypothesis.
Footnotes
Author contributions
All authors contributed to all aspects of the study design, data collection, and write-up.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.