
Abstract
Background and Aims:
Emergency laparotomy is associated with a great risk of mortality in the elderly. The hyperadrenergic state induced by surgical trauma may play an important role in the pathophysiology of this increased risk. Studies have shown that beta-blocker exposure may be associated with decreased morbidity and mortality in the perioperative period. We aimed to study the effect of beta-blocker on mortality in geriatric patients undergoing emergency laparotomy.
Material and Methods:
This is a retrospective study of patients who underwent emergency laparotomy between 1 January 2015 and 31 December 2016 at a single institution. The outcomes of interest were the association between post-operative complications and in-hospital and 1-year mortality in patients on beta-blocker therapy (BB(+)) and those who were not (BB(−)). The Poisson regression analysis was used to evaluate the association.
Results:
A total of 192 patients were included of whom 62 (32.2%) had pre-operative beta-blocker therapy with continued exposure during their hospital stay. The in-hospital mortality was 17.7% in the BB(+) and 23.8% in the BB(−) cohorts (p = 0.441). One-year mortality was significantly lower in the BB(+) group compared to the BB(−) group (30.6% versus 47.7%; p = 0.038). After adjusting for confounders, the incidence of deaths during 1 year post-operatively decreased by 35% in the BB(+) group (incidence rate ratio = 0.65, p = 0.004). No significant differences in the incidence of post-operative complications between the two groups could be measured.
Conclusion:
Beta-blocker therapy may be associated with reduced 1-year mortality following emergency laparotomy in geriatric patients.
Introduction
Improvements in health care have resulted in an increasing geriatric population (1). This has resulted in a rising need for emergency laparotomy in an increasingly older patient population (1, 2). Emergency surgery is associated with a higher risk of morbidity and mortality than an elective operation, and this risk is further augmented in the geriatric population (2, 3). In addition, elderly patients demonstrate not only an increased mortality risk after surgery, but this risk remains for a longer period of time in comparison to the younger population (4).
The stress response to surgery encompasses a cascade of endocrinologic, neurologic, and immunologic responses (5). The activation of the sympathetic nervous system, as part of this stress response, results in an increased secretion and circulation of catecholamines (5). However, sustained and excessive adrenergic activity is associated with increased mortality (6). Immunosuppression, catabolism, coagulopathy, and cardiac dysfunction, with subsequent multisystem organ failure, have been implicated as the cause of this increased risk of death (7).
The use of beta-blockade in a subgroup of patients undergoing non-cardiac surgery results in a reduced risk of in-hospital mortality, possibly by blunting the hyperadrenergic state (8, 9). Studies of the effect of beta-blocker use in geriatric populations undergoing emergency abdominal surgery are lacking. We hypothesize that utilizing pre-operative beta-blockade in this patient cohort reduces mortality and post-operative complications.
Material and Methods
After obtaining Regional Review Board approval (Uppsala County Dnr 2018/455), all geriatric patients (age ⩾65 years) who underwent an emergency laparotomy between 1 January 2015 and 31 December 2016 at the Orebro University Hospital, Sweden, were identified. Patients who died within 24 h of surgery were excluded. Emergency laparotomy was defined as unplanned, same index admission surgery.
Data were retrospectively retrieved from electronic medical records. The obtained data for patient characteristics were the most recent values before any surgical interventions. Age, gender, Charlson Comorbidity Index (CCI) score, body mass index (BMI), American Society of Anesthesiologists (ASA) score, pre-operative heart rate, systolic blood pressure (SBP), hemoglobin (g/L), C-reactive protein (CRP), creatinine, packed red blood cell (PRBC) transfusion, indication for surgery, surgical procedure performed, and number of operations were abstracted for analysis. Outcome variables of interest were post-operative complications and in-hospital and 1-year mortality. Post-operative complications of interest were any type of infection needing antibiotic treatment, heart failure, dysrhythmia, myocardial infarction (MI), and new-onset dialysis–dependent kidney failure. These complications have been associated with inflammatory and immunological responses due to the hyperadrenergic state derived by the surgical trauma (5, 10).
Statistical Analyses
Patients were divided into two groups: those who were on pre-existing beta-blocker treatment (BB(+)) and those who were not (BB(−)). Demographics, clinical information, and outcomes are presented using descriptive statistical methods and compared between the two groups. Continuous data are summarized as mean with standard deviation (SD) or median with corresponding interquartile range (IQR) where suitable and categorical and ordinal data are presented as percentages. The chi-square test was used to compare categorical variables unless the sample size was small, in which case Fisher’s exact test was used. Student’s t test was utilized to analyze continuous data with normal distribution, and the Mann–Whitney U test was used to compare for non-parametric continuous variables.
Associations between in-hospital and 1-year mortality and beta-blocker use were evaluated using a Poisson regression model with robust standard errors. Potential confounding was adjusted for by including the following covariates in the model: age, gender, CCI score, BMI, ASA score, pre-operative heart rate, SBP, hemoglobin (g/L), log-transformed CRP, log-transformed creatinine, surgery indication, surgical procedure, number of operations, and PRBC transfusion.
In Poisson regression analysis, missing data were multiply imputed by using the iterative Markov chain Monte Carlo method (11). Five imputed datasets were generated. The estimates from the five datasets were then combined according to Rubin’s rules (12). Results are reported as incidence rate ratios (IRRs) with corresponding 95% confidence intervals (CIs). A two-sided p value of less than 0.05 was considered statistically significant. All analyses were carried out in Stata 15.1 (StataCorp, College Station, Texas, USA).
Results
Patient Characteristics
A total of 192 patients met inclusion criteria during the 2-year study period. The mean (SD) age of patients was 76 (7) years with 97 (50.5%) patients being male. Sixty-two patients (32.3%) had pre-operative beta-blocker therapy that was continued throughout the hospital length of stay. The majority of patients on beta-blockers received metoprolol (56.5%), followed by bisoprolol (30.6%), atenolol (8.1%), and other types of beta-blockers (4.8%). The median ASA and CCI scores were 3 (IQR 2–3) and 6 (IQR 4–6), respectively.
In univariate analysis, there were no significant differences in age, gender, BMI, CCI score, ASA score, and pre-operative laboratory values between the BB(+) versus BB(−) cohorts (Table 1).
Patient characteristics and outcomes according to beta-blocker administration.
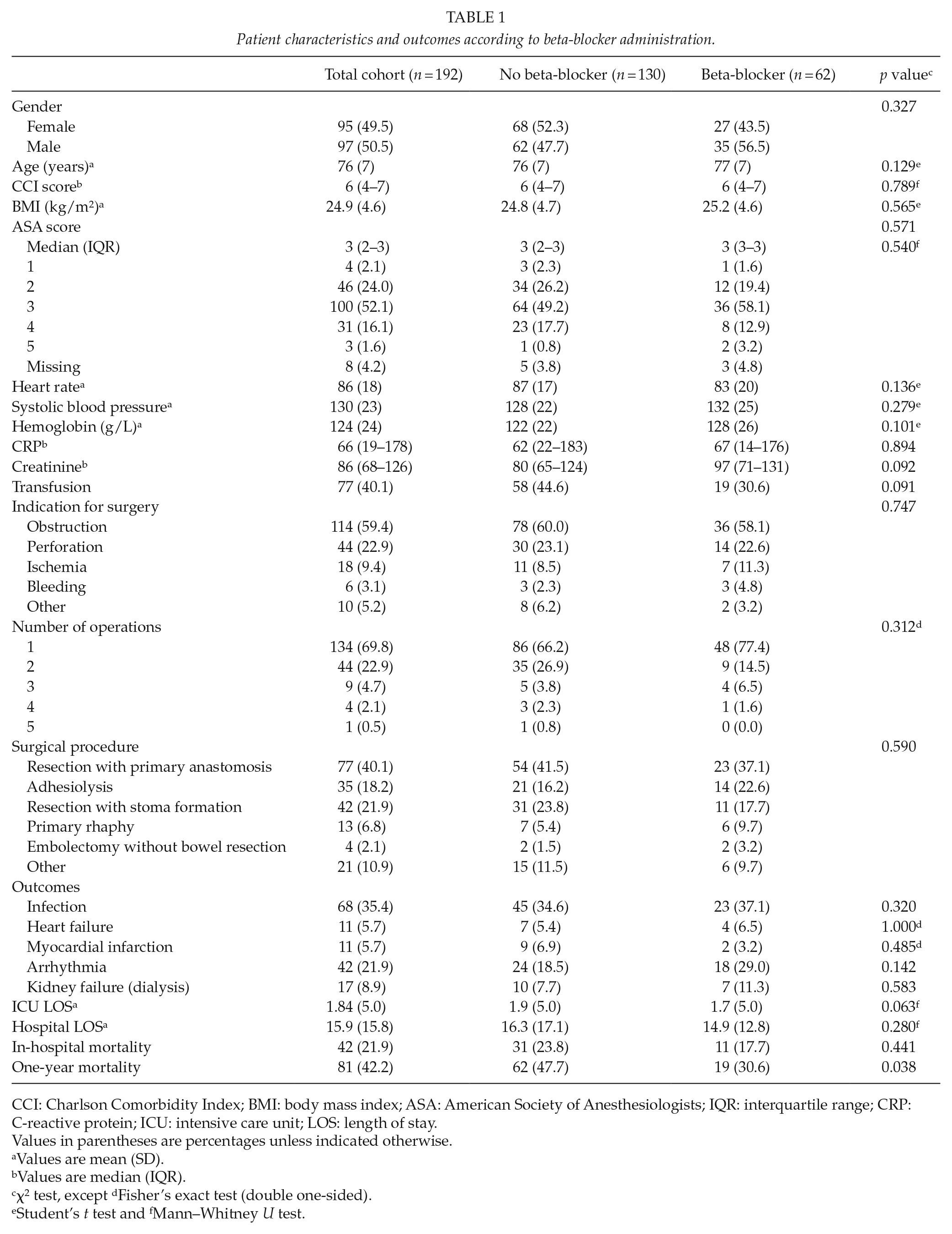
CCI: Charlson Comorbidity Index; BMI: body mass index; ASA: American Society of Anesthesiologists; IQR: interquartile range; CRP: C-reactive protein; ICU: intensive care unit; LOS: length of stay.
Values in parentheses are percentages unless indicated otherwise.
Values are mean (SD).
Values are median (IQR).
χ2 test, except dFisher’s exact test (double one-sided).
Student’s t test and fMann–Whitney U test.
Operative Characteristics
The most common indication for emergency laparotomy was bowel obstruction (59.4%). The majority of patients (92.7%) had no more than two operations during their hospital admission. Bowel resection with primary anastomosis was performed in 77 patients (40.1%), and 42 patients (21.9%) underwent bowel resection with the formation of a stoma. There was no significant difference in indication for surgery, surgical procedure performed, and number of operations between the BB(+) and BB(−) groups (Table 1).
Outcomes of Interest
There were 31 in-hospital deaths (23.8%) in the BB(−) group compared to 11 deaths (17.7%) in the BB(+) group (p = 0.441). The mortality rate was significantly higher after 1 year in the beta-blocker negative group (47.7% versus 30.6%; p = 0.038) (Table 1).
Although a lower risk (multivariate adjusted IRR = 0.66) was observed for the incidence of in-hospital mortality in the beta-blocker exposed patients, the result was not statistically significant (95% CI of IRR = 0.33, 1.32; p = 0.24) (Table 2). After adjusting for potential confounders, the risk of 1-year mortality was reduced by 35% in the beta-blocker group (IRR = 0.65, 95% CI = 0.44, 0.98; p = 0.04) (Table 3).
Incidence rate ratio for all-cause in-hospital mortality for the total cohort (192 patients).
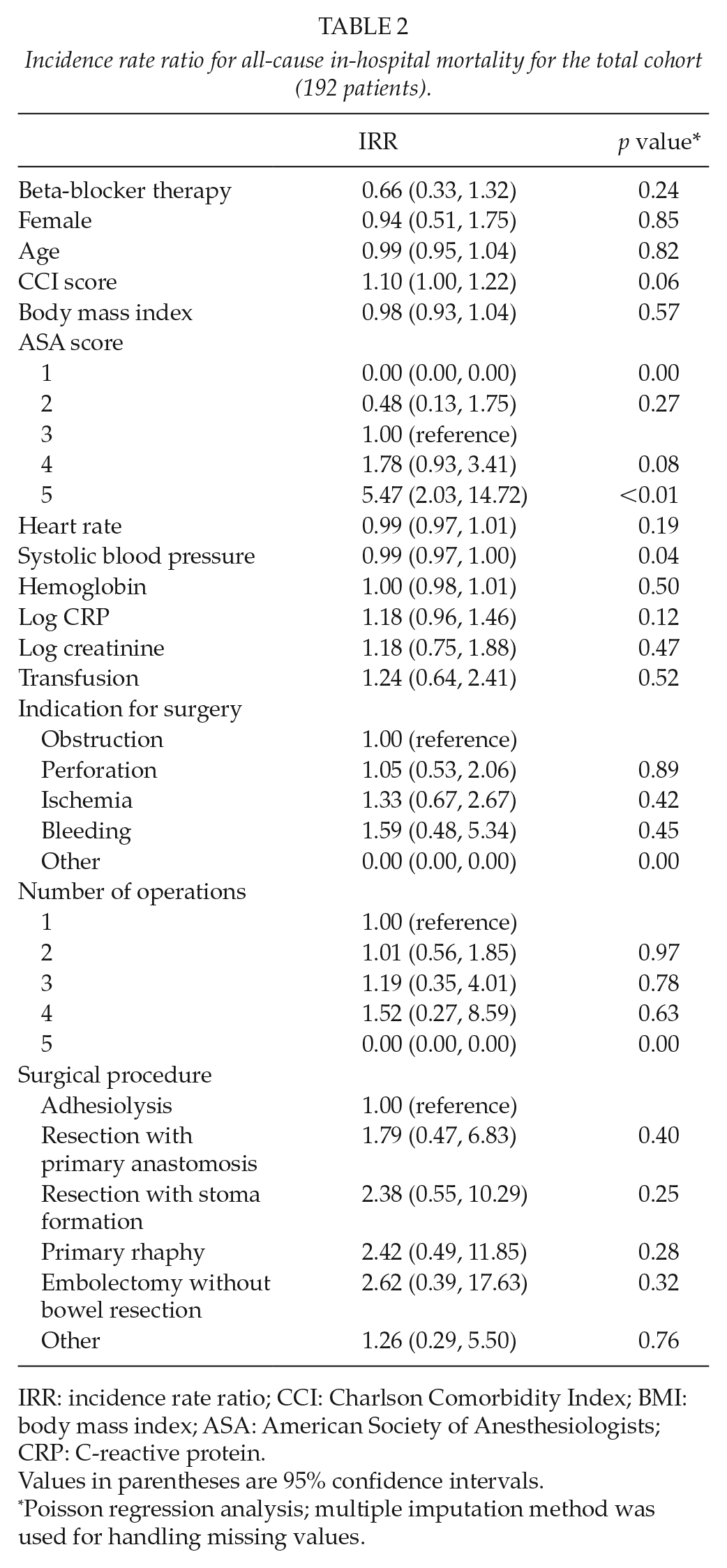
IRR: incidence rate ratio; CCI: Charlson Comorbidity Index; BMI: body mass index; ASA: American Society of Anesthesiologists; CRP: C-reactive protein.
Values in parentheses are 95% confidence intervals.
Poisson regression analysis; multiple imputation method was used for handling missing values.
Incidence rate ratio for all-cause 1-year mortality for the total cohort (192 patients).
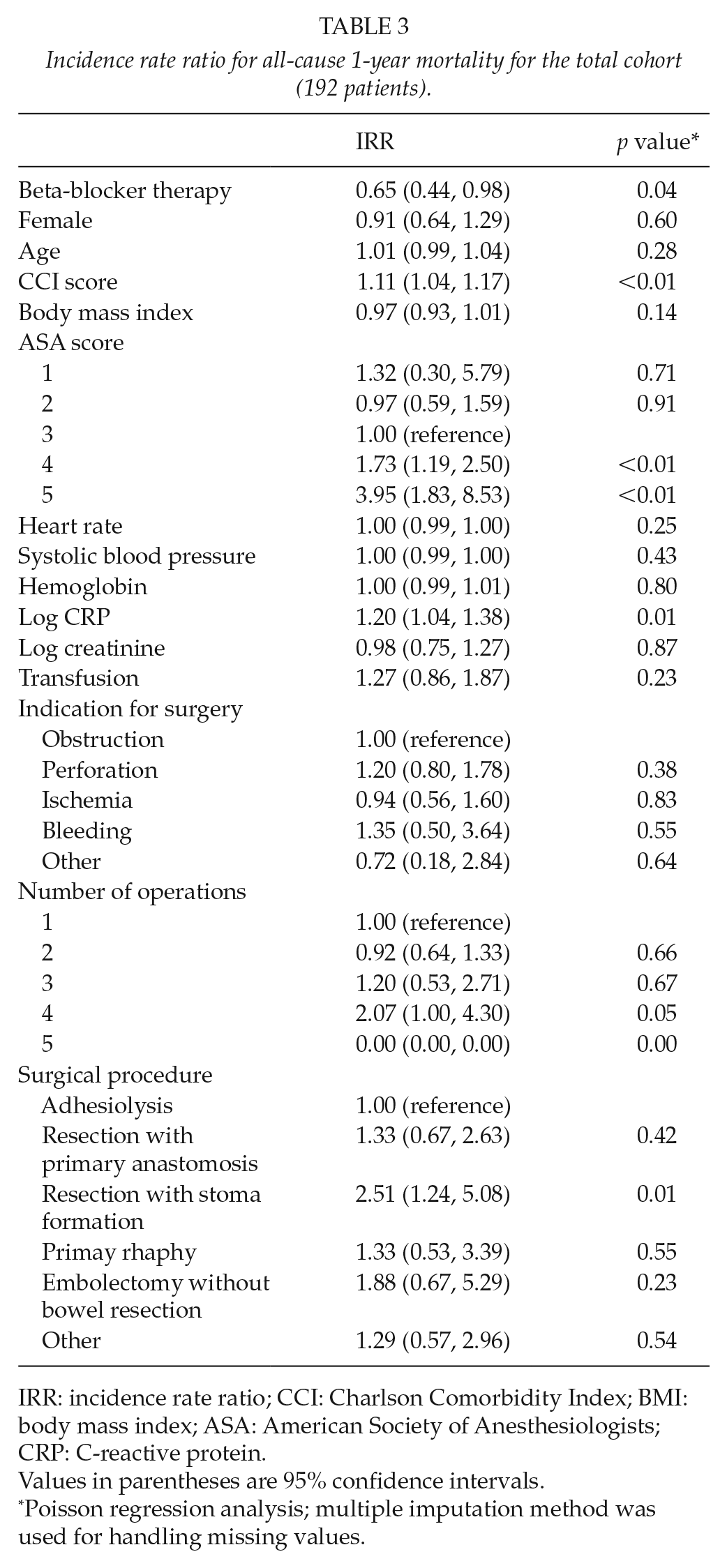
IRR: incidence rate ratio; CCI: Charlson Comorbidity Index; BMI: body mass index; ASA: American Society of Anesthesiologists; CRP: C-reactive protein.
Values in parentheses are 95% confidence intervals.
Poisson regression analysis; multiple imputation method was used for handling missing values.
There was no statistically significant difference between the two groups in the incidence of post-operative complications such as infection rates, heart failure, MI, dysrhythmia, or kidney failure needing dialysis (Table 1). This result did not change between the two cohorts after adjustments for potential confounding factors (Table 4).
Incidence rate ratio of beta-blocker therapy for post-operative complications.
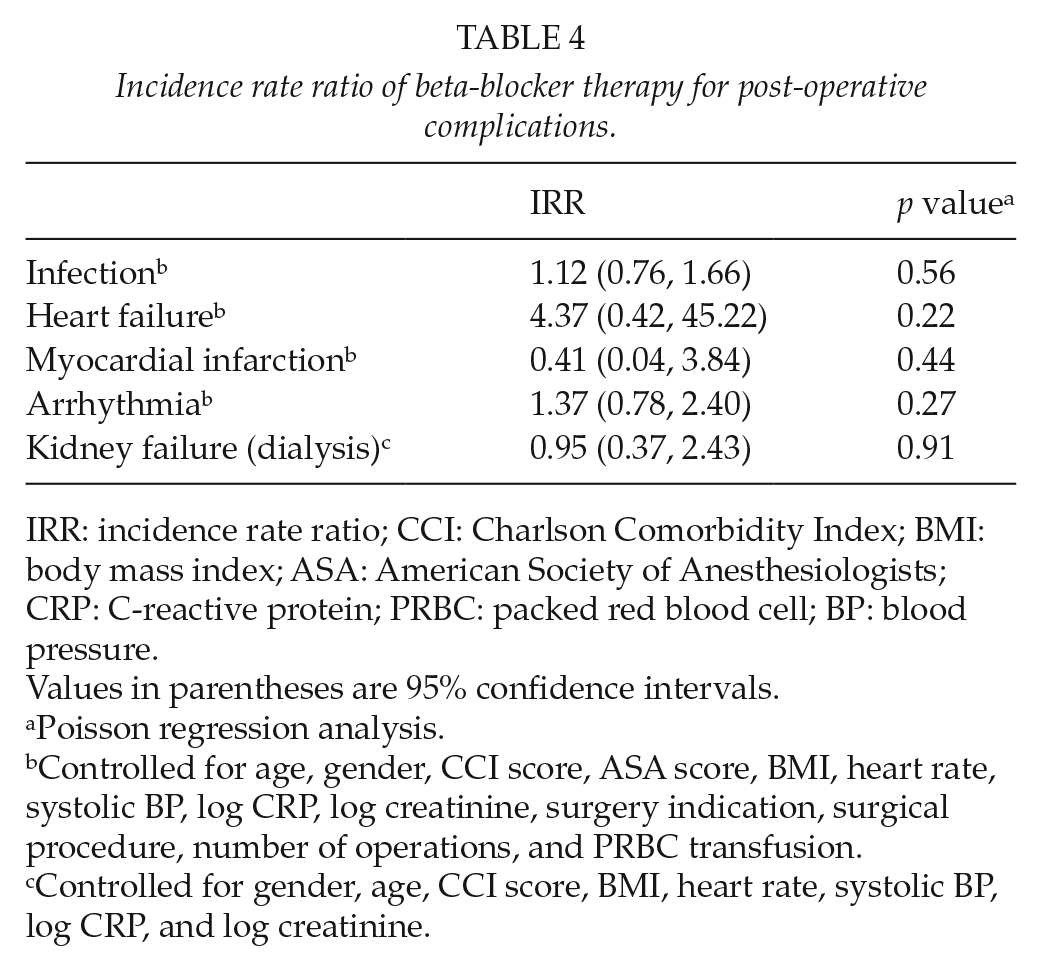
IRR: incidence rate ratio; CCI: Charlson Comorbidity Index; BMI: body mass index; ASA: American Society of Anesthesiologists; CRP: C-reactive protein; PRBC: packed red blood cell; BP: blood pressure.
Values in parentheses are 95% confidence intervals.
Poisson regression analysis.
Controlled for age, gender, CCI score, ASA score, BMI, heart rate, systolic BP, log CRP, log creatinine, surgery indication, surgical procedure, number of operations, and PRBC transfusion.
Controlled for gender, age, CCI score, BMI, heart rate, systolic BP, log CRP, and log creatinine.
Discussion
This retrospective study found that beta-blocker therapy in geriatric patients undergoing emergency laparotomy is associated with a significant reduction in 1-year mortality.
Emergency surgery is inherently associated with increased risk of morbidity and mortality (3). This risk is amplified in the geriatric population because of comorbidities and overall increase in frailty (2). Previous studies have reported up to 20% of 30-day mortality in patients undergoing emergency laparotomy with an increase to 38% in patients over 80 years (2, 3). A review of the American College of Surgeons National Surgical Quality Improvement Program database showed an incidence of 14% of 30-day mortality after emergency laparotomy. In the multivariate analysis, the adjusted risk (odds ratio) was increasing with age from 1.69, 2.33, 3.50, and 5.91 in the age brackets 40–59, 60–69, 70–79, and 80–89 years, respectively (13). However, none of these studies reported long-term mortality. The results in the current study with respect to the incidence of in-hospital deaths of 21% for the age range of the studied population are in line with these previous data reported. The stress response to surgery activates multiple physiological processes which induce derangements in inflammatory and hormonal activities (5). The duration and magnitude of surgery-induced stress response vary according to the severity of the surgical injury and the development of complications. In addition, data suggest that older patients tend to have a higher and more sustained response (5, 10). This can be the result of multiple comorbidities leading to poorer perioperative performance status, higher risk of post-operative complications, and more frequent requirement for emergency surgeries when compared to younger patients. Elevation of inflammatory cytokines (interleukin-1, tumor necrosis factor-α, and interleukin-6) and stress hormones, such as cortisol, glucagon, and catecholamines, exacerbates the stress response to surgery (5, 10). Persistent elevation of cytokines and stress hormones can induce a hypercatabolic state, which can result in muscle wasting, immune system dysfunction, and eventual multi-organ failure and death (10). In particular, the maintained hyperadrenergic state can be detrimental to patient survival due to a constant increase in myocardial oxygen demand, hypertension, and tachycardia. It is evident from multiple studies that beta-blocker exposure ameliorates the hyperdynamic and hypercatabolic response in a subgroup of patients after an elective or emergency non-cardiac surgery with resultant decrease in mortality (8, 9). This beneficial effect is also seen in critically ill patients with traumatic injuries (14). In addition, many patients undergoing emergency surgery are in a septic state due to perforation of hollow viscus or bacterial translocation. Beta-blockade has also been associated with improved outcomes in severe sepsis (15).
The effect of pre-operative beta-blocker therapy on geriatric patients undergoing emergency abdominal surgery has not been investigated previously. The current study found reduced 1-year all-cause mortality in geriatric patients receiving regular pre- and post-operative beta-blocker treatment. The risk of mortality was reduced by 35% after adjusting for confounders. Not surprisingly, the regression analysis in this study identified high ASA classification as an independent risk factor for both in-hospital and 1-year mortality. In addition, the increasing CCI score, elevated CRP levels, and bowel resection with stoma formation were identified as independent risk factors for increased 1-year all-cause mortality. Analysis also showed that having a lower SBP on admission is correlated with a protective factor for in-hospital all-cause mortality, which may also be partly due to treatment with a beta-blocker.
There was no significant difference in the in-hospital all-cause mortality between the two groups. This result correlates with some of the other previously published studies and meta-analyses (16, 17). In a meta-analysis of six randomized trials, Stevens et al. (18) reported that beta-blockers were associated with a 75% reduction in the risk of death from cardiac causes. On the other hand, there are studies that have shown increased 30-day all-cause mortality as well as increased risk of stroke in surgical patients receiving perioperative beta-blocker therapy for elective surgical procedures (19, 20). These studies have also demonstrated increased IRR of bradycardia and hypotension in the beta-blocker therapy group requiring treatment for these potential adverse effects. Hence, the post-operative favorable effects of beta-blocker therapy are not consistent among the different studies. This may be attributed to the different patient characteristics, inclusion and exclusion criteria, and the wide range of surgeries included in these studies comprising orthopedic, vascular, and abdominal procedures. Therefore, it is difficult to reach a meaningful conclusion when comparing distinct groups of patients.
Our study demonstrates that perioperative use of beta-blocker can reduce long-term risk of mortality. A similar result was obtained by Mangano et al. (21) in a randomized, double-blind, placebo-controlled trial that investigated the effect of perioperative atenolol use on overall survival and cardiovascular morbidity in patients undergoing non-cardiac surgery. Patients in this study had a reduced 2-year overall mortality after hospital discharge (21). The association between perioperative myocardial ischemia and adverse outcomes after discharge from the hospital is well established (22, 23). Beta-blockers improve this post-operative outcome by extending coronary diastolic filling time, inhibiting fatal ventricular arrhythmias, and impeding the rupture of atheromatous plaque in the presence of high sympathetic nervous system tone (24). However, it should be noted that pre-operative risk factors such as cardiovascular morbidities are unlikely to be the sole determinants of patient survival and outcome. In fact, multiple studies have shown that post-operative complications may be more important than pre-operative patient risk factors in determining the survival after a major surgery (25, 26). In a prospective multicenter study, Khuri et al. (25) demonstrated that post-operative complications, independent of a patient’s pre-operative risk, were associated with a 69% reduced median patient survival. Accordingly, any comprehensive initiative for quality improvement of surgical care should take into account both pre-operative risk factors and post-operative complications of a patient to reduce long-term risk of mortality.
Beta-blockers have shown protective effect with decreased 30-day mortality in emergency laparotomy for colon cancer (27). However, we also investigated the 1-year mortality rate in our study. Surgical mortality results are increasingly being reported at 90 days and 1 year after the index surgery in order to have a more meaningful measurement of post-operative mortality risk (28, 29). In particular, colorectal surgery carries a significant risk of complication or death (30), and considerable mortality beyond 30 days has prompted most centers to report 90-day mortality to better demonstrate the outcomes (28, 29). These long-term outcomes are often used to develop and validate quality measures and have the potential to improve surgical risk calculations (28, 29).
Several inherent limitations of this study should be noted. No distinction could be made as to the dose and type of beta-blocker prescribed and the associated degree of heart rate control achieved in each patient. However, the vast majority of patients (95%) received a selective beta-1 receptor antagonist. Furthermore, the study design precluded our ability to determine the indication for beta-blocker prescription. Another limitation is the inability to determine whether the apparent survival benefit of beta-blocker treatment is explained by the pre-operative administration of beta-blocker therapy or if the effect comes from continued administration throughout the post-operative period. In addition, patients on beta-blockers might be on other medications that could alter inflammatory responses and have a synergic effect on long-term survival; however, this was out of the scope of the current study and not investigated. The underlying diagnosis mandating an emergency surgery could potentially influence long-term outcomes too. The incidence of some adverse events associated with beta-blocker therapy, such as bradycardia and hypotension, could not be determined. The non-statistically significant findings might be due to the small sample size in the current study, and further confirmative studies with larger sample size are needed in the future. Finally, the exact cause of death and distinction between patients who had withdrawal of care and those who did not could not be made.
In conclusion, our results suggest that beta-blocker therapy in geriatric patients undergoing emergency surgery is associated with significantly lower 1-year mortality. The ideal timing of initiation, type of medication, dose, and safety profile remain important issues that require further study.
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Regional Review Board of Orebro University Hospital, Sweden (Uppsala County Dnr 2018/455).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.