
Abstract
Background and Aims:
Decreased range of motion of the elbow and forearm and decreased grip strength are potential findings following a childhood upper extremity fracture. Clinical follow-up is essential because spontaneous improvement is seen several months after the injury. Freehand measuring with a goniometer and hydraulic dynamometer is used to evaluate clinical result. The new methods are justified in avoiding human typewriting errors, thus improving patient safety. Nevertheless, their feasibility in child patients is unknown. This study aimed to evaluate congruence between the computer-assisted and the free-hand measuring methods.
Materials and Methods:
A total of 59 children with a previous supracondylar humerus fracture were clinically examined by means of free-hand (transparent goniometer and hydraulic dynamometer; Jamar, Lafayette Ltd.) and computer-assisted (E-Link System Packages, Biometrics Ltd.) methods. The range of motion and grip strength were measured separately using both methods. Agreement between the measurements was evaluated using the Bland–Altman method.
Results:
The results between the two methods were incongruent and the differences between measurements increased along with the mean of measurements in all categories except elbow extension. Rotational range of motions were smaller and grip strength was weaker while measuring with the computer-assisted method. The mean discrepancy was 0.97° (95% confidence interval = −2.46 to 0.53) for elbow extension and 7.97° (95% confidence interval = 6.60–9.33) for elbow flexion.
Conclusions:
Grip strength is used to evaluate impairment of hand function. The study method showed slightly lower results in grip strength. Range of motion is essential when evaluating the outcome of supracondylar humerus fracture, while >10° of change in elbow range of motion associate with impaired function. As compared with the gold-standard goniometer, the methods were not congruent. However, all differences were under 10° and probably beyond clinical importance. Because of its advantages in recording the outcomes to electronical charts, the computer-assisted method is recommended option in performing the follow-up of complicated pediatric supracondylar humerus fractures.
Introduction
Supracondylar humerus fractures are most usual distal humerus fractures in children, and it is a fracture type that mostly requires surgical (operative) treatment in children. Despite good natural history of bone fractures among children in general, the patients with impaired recovery after supracondylar humerus fracture are not rare in pediatric orthopedic units (1–3). Impaired joint movements in the elbow and/or forearm and weakened grip strength are possible findings in these patients (1, 4).
The long-term outcome of supracondylar humerus fracture is usually assessed clinically by using Flynn’s criteria, which define unsatisfactory results as >15° asymmetry in elbow range of motion (ROM) and/or carrying angle. According to Flynn’s criteria, 11°–15° of loss in ROM refers to fair, 6°–10° to good, and 0°–5° to excellent outcomes. Tuomilehto et al. (2) investigated 65 children with a former supracondylar humerus fractures, and 7.7% (N = 5) had inferior ROM in mean 9 years after injury. In short-term, 19% (N = 6/32) of the patients with supracondylar humerus fracture complained restricted elbow motion (5). More than 10° of loss in ROM associate with lower functional outcomes (2). In another long-term study, good/excellent ROM was achieved in 67% of the patients (6).
Despite decreased ROM of the elbow primarily after injury, the natural history is good: ROM values reach 72% of the corresponding contralateral elbow motion by 6 weeks postoperatively, 86% by 12 weeks, 94% by 26 weeks, and 98% by 52 weeks (7). This high-spontaneous recovery of limited ROM emphasizes the need of satisfactory long clinical follow-up in means of repeated measurements, instead of needless and too early surgical treatment.
Another clinically relevant index in assessing impairment in upper extremity function is grip strength (8). Overall, grip strength reflects well how much upper extremity can be used (9). Therefore, occupational therapists include grip power in their evaluation of hand function (10). Supracondylar humerus fractures, especially displaced fractures, have shown to be associated with decreased grip strength (1). In addition, there are several other factors affecting on it, such as sex, age, diseases, and handiness. A minimal clinical difference in grip strength has shown to be 6.5 kg (11).
Full ROM of the elbow and forearm and satisfactory grip strength are the key treatment goals after supracondylar humerus fractures (4, 12). Therefore, these functional outcomes must be reasonably determined within outpatient clinics. In current clinical practice, functional measurements are usually made by a physician with a free-hand transparent goniometer and hydraulic dynamometer (Jamar, Lafayette Ltd.) (13) due to their ease of use and sufficient availability (14). Intrarater reliability of the transparent goniometer is satisfactory when measuring ROM (14, 15). The hydraulic dynamometer is considered a valid instrument for maximal muscle strength assessment (14–18).
Nevertheless, there are limitations in traditional measuring methods, for example, the results must be manually tabulated into clinical charts. Furthermore, the descriptive (range) and mathematical (e.g. mean) results of the repeated measurements must be manually calculated. There is a risk of human typewriting error at every extra stage. Thus, new devices have been developed to make the measurement process as accurate, fast, and safe as possible (13, 17, 19). For example, computer-assisted and photography-based goniometers (14, 20, 21), fluid goniometers (13), and cell phone application tools (22, 23) have been suggested to directly capture the quantitative results. Furthermore, experts other than medical doctors and surgeons, for example, occupational therapists, would be incorporated to follow up the patients at out-hospital visits. Improved job sharing between physicians and occupational therapists would impose economic benefits upon healthcare units, despite the higher purchase costs of high-technology measuring methods. However, the congruence of the traditional and computer-based measuring methods has not been widely studied, and it is rather unclear whether or not the tools may be used interchangeably (20) during follow-up visits. Furthermore, it is unclear whether these methods are even feasible with children and adolescent patients because their cooperation may not be optimal.
Therefore, keeping the high clinical importance of the ROM and grip strength in children patients with former upper limb fracture in mind, this study was aimed to evaluate the congruence of two different measuring methods: a computer-assisted method versus free-hand goniometer and hydraulic dynamometer methods.
Materials and Methods
Study Design
This was a prospective, observational study performed in Oulu University Hospital in Oulu, Finland. Patients with a former supracondylar humerus fracture were clinically examined during out-of-hospital follow-up visits at an average of 10 years after the initial injury at an average age of 17 years (10–24 years). All but one of the intended 60 cases participated (23 males and 36 females), and each patient’s injured extremity was examined using both study method (E-Link System Packages, Biometrics Ltd.) and the standard method (plastic goniometer; Baselane® and hydraulic dynamometer; Jamar, Lafayette Ltd.) The primary outcome was the ROM in elbow flexion–extension and forearm pronation and supination, while grip strength was the secondary outcome. Finally, the congruence between the study method and the free-hand reference method was evaluated.
Measuring Arrangements
The studied measurements were independently performed during the same out-of-hospital visits by two thoroughly educated investigators (A.H. and J-J.S.) who were previously instructed about measurement details and the use of measurement devices. The patients’ sitting position was coordinated, and the accuracy of data recording was decided as entire units (Nm) in regard to strength and one decimal (of degrees) in regard to motion.
The universal goniometer used in this study consists of stationary and moving arms and was constructed from clear, flexible plastic with a scale of degrees in the central protractor and referring lines for determining the angles in both arms (14, 24). A computer-assisted tool was constructed from two arms with clear plastic and colored borders; however, the tool does not have a visible scale, but rather the result is only readable on the computer screen when the measurement is ongoing (Fig. 1). The hydraulic and computer-assisted dynamometers look similar apart from the cable that connects the computer-assisted dynamometer to its central unit. The purchase price of the study method equipment in the study country is approximately 6200€, including goniometer and grip strength measure, according to the importer in Finland (Villa Manus ltd, Vantaa, Finland). The equipment is connected to any external computer, which is not included in this price. The reference goniometer costs about 25€ and hydraulic dynamometer approx. 620€ and needs yearly calibration with 105€–330€.

Elbow flexion measured with the universal goniometer (Jamar, Lafayette Ltd.) made from clear plastic as well as the computer-assisted goniometer (E-Link System Packages, Biometrics Ltd.), both of which possess two movable arms. The mechanical center point of the hinge is not visible in the computer-assisted goniometer, which may have affected the correct positioning of the goniometer.
Elbow
To measure elbow flexion and extension, each patient sat up straight in his or her chair and the goniometer was lined in a laterally parallel position to his or her upper arm and forearm (Fig. 2). The flexion was measured from 0° (full extension) to 180°, and hyperextension was marked as angles below 0.
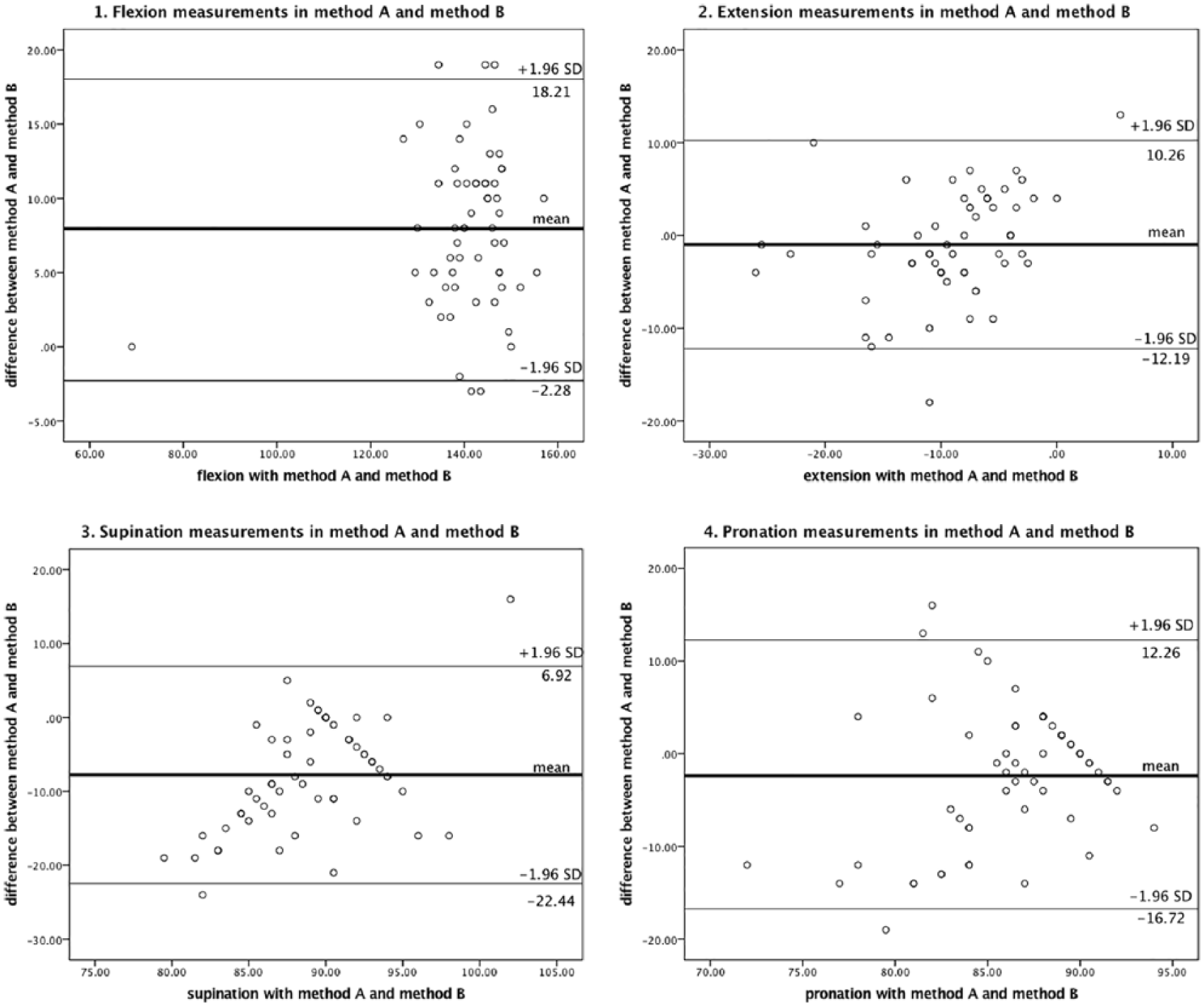
The representation of the level of agreement between measurements A (traditional free-hand method) and B (computer-assisted method) by Bland–Altman’s plot. Vertical lines (Y-axis) represent the mean difference and the standard deviation of the difference between the measurements. Horizontal lines (X-axis) represent the true value of each quantitative measurement result (plots). Each graph demonstrates each measured range of motion.
Forearm
To measure pronation and supination, the elbow was flexed at a 90° angle and positioned against the torso to eliminate compensation of potentially limited forearm pronation by shoulder abduction. The rotation measurements were taken from the distal forearm at the level of radius metaphysis (Fig. 3) rather than the thenar area to eliminate additional motion of the hand.
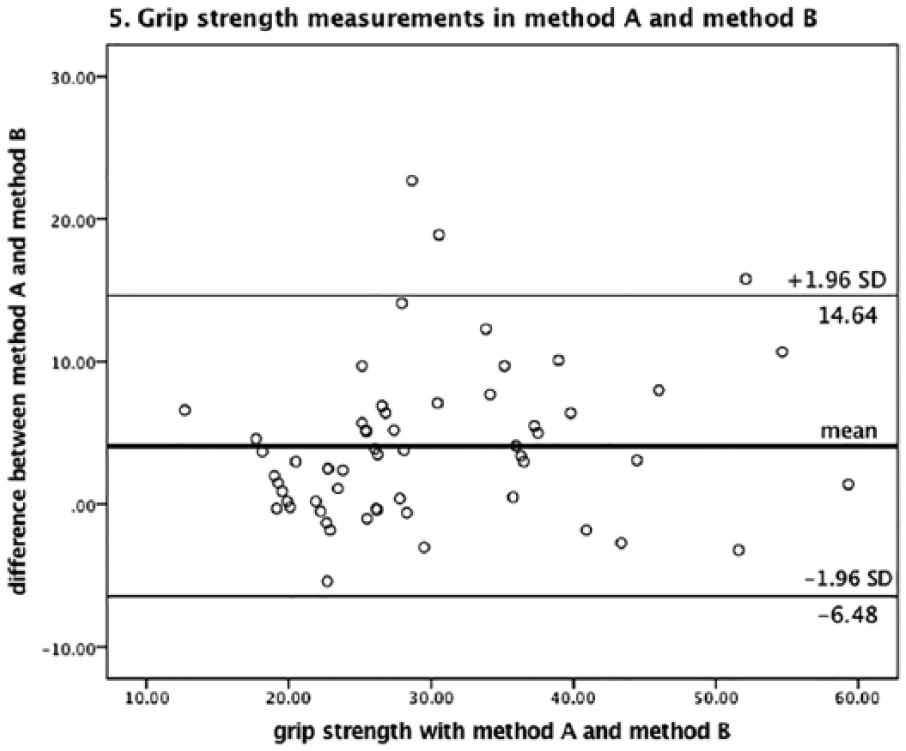
The graphical representation of the level of agreement between measurements A (hydraulic traditional dynamometer) and B (computer-assisted dynamometer) by Bland–Altman’s plot. Vertical lines (Y-axis) represent the mean difference and the standard deviation of the difference between the measurements. Horizontal lines (X-axis) represent the true value of each quantitative measurement result (plots).
Grip strength
To measure grip strength with any dynamometer, each patient was asked to grip the dynamometer with maximal press power and with his or her upper arm adducted against the torso. Shoulders were neutrally rotated, the elbow was flexed at 90°, and the forearm and wrist were neutrally positioned during the testing procedure.
The computer-assisted goniometer (E-Link) illustrated measurements immediately, and the illustrative graphs could be drawn based on the measurement results. The results were ready to be transferred onto the patient’s hospital charts without delay, being instantly available for the healthcare professionals. However, for this study’s purpose, the results were printed out to a separate file and were combined in the electronic research database.
Both investigators independently performed a random selection of 25 measures on the same day using the same technique to evaluate interrater reliability between the two investigators (A.H. and J-J.S.). The investigators were blinded during the revealing of their findings.
Statistical Analysis
The mean differences between the ROM and the strength, measured by the computer-assisted device and the free-hand method, were analyzed by paired t tests. The limits of agreement for the ROM and grip strength were examined using the Bland–Altman plot (25–27). The difference between the two measurements (Y-axis) for each patient was plotted against the mean of the same two measurements (X-axis). The limits of agreement were derived from the mean difference ± 1.96 SD. In the presence of agreement, most data points should have been contained between these intervals. If the two methods were congruent, the mean of the differences was zero. The statistical significance of bias—the gap between the mean of the differences and zero—was tested using a one-sample t test. The data were analyzed as differences of units rather than percentages. A linear trend among data points was evaluated using a linear regression analysis (26).
Intraclass correlation coefficient (ICC) was calculated based on the mean rating (k = 2), absolute agreement, and a two-way mixed effect model to evaluate interobserver validity. Values greater than 0.90 indicated excellent reliability (28).
Results less than 5% were considered to be statistically significant (p < 0.05). Statistical analyses were performed using SPSS Statistical Software Package, version 24 (SPSS Inc., USA).
Ethical Approval
Ethical board approval was previously achieved by the Hospital Ethics Committee of Vaasa Central Hospital as part of an upper extremity fracture study (5/2008) that was approved as an amendment by the Northern Finland Hospital District Ethical Committee. The Helsinki Declaration of human research was complied with, and institutional approval was acquired prior to the study’s execution.
Results
Measurement Values
The elbow flexion was measured as 138° using the study method (E-Link) and 146° using the reference method (universal goniometer). Regarding elbow extension, measurements were −8.8° and −9.8° using the study method and reference method, respectively. Pronation was measured as 87° and 85° using the study method and reference method, respectively. Supination was measured as 93° and 85° using the study method and reference method, respectively. Furthermore, the grip strengths were measured at 28 and 31 Nm using the study method and reference method, respectively. All mean values except for that of elbow extension differed statistically significantly (Table 1), and ICC was identified as excellent (ICC = 0.999).
The range of motion of the elbow and forearm was measured by universal and computer-assisted goniometer in degrees, and the grip strength was measured by hydraulic dynamometer and computer-assisted dynamometer (E-link) in children patients with a former supracondylar humerus fracture.
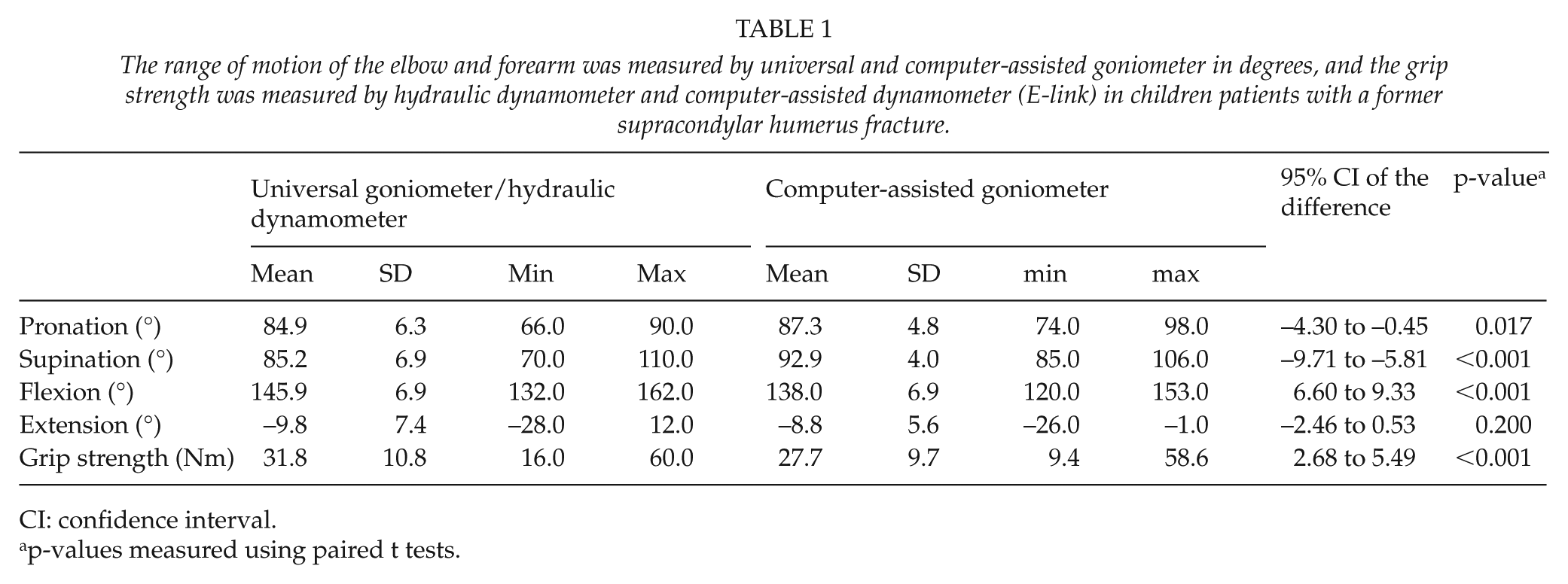
CI: confidence interval.
p-values measured using paired t tests.
Agreement between the Methods
There were discrepancies between the two methods in all categories except elbow extension. The measures achieved by the computer-assisted method were approximately 8.0° less (95% confidence interval (CI) = 6.6°−9.3°, p < 0.001) in elbow flexion and 1.0° less in elbow extension (95% CI = −2.5° to 0.5°, p = 0.200) than those achieved using the traditional method (Fig. 2). The bias in pronation and supination between the two methods was 2.4° (95% CI = −4.3° to −0.4°, p = 0.017) and 7.8° (95% CI = −9.7° to −5.8°, p < 0.001), respectively. The computer-assisted method revealed greater values, wherein grip strength was 4 Nm less when evaluated using the computer-assisted method rather than the traditional, hydraulic dynamometer (95% CI = 2.7–5.5 Nm, p < 0.001). Therefore, all measures except elbow extension lacked agreement between the methods (Fig. 2).
There was a positive linear trend between data points in all categories except elbow flexion and grip strength. The regression coefficients β in elbow flexion and extension were 0.069 (95% CI = −18.72 to 15.24, p = 0.256) and 0.332 (95% CI = 0.09–0.57, p = 0.008), respectively. The regression coefficients β in forearm supination and pronation were 0.895 (95% CI = 0.49–1.30, p < 0.001) and 0.485 (95% CI = 0.03–0.94, p = 0.036), respectively. Finally, the regression coefficient β of grip strength was 0.11 (95% CI = −0.03 to 0.25, p = 0.120) (Fig. 2).
Discussion
Supracondylar humerus fractures are the most usual elbow fractures in children. Their complications occur not only because of the fracture itself but also due to insufficient treatment (29, 30). In general, restoration of coronal, sagittal, and rotatory alignment of the distal humerus and osteosynthesis with at least two pins, which fix both fracture fragments and do not cross at the fracture line, are recommended in treatment (5, 31–33). Any deviation from this appreciated practice should be avoided, when treating supracondylar humerus fractures, in general. Nevertheless, there is a risk for impaired recovery. Decreased ROM and grip strength are potential short-term findings. There is also a risk for residual morbidity in long-term follow-up, while 7.7% showed decreased ROM of the elbow (5) and 15% had decrease in grip power in 10 years’ mark (1).
It is important that the methods of measuring these clinically essential outcome variables are both feasible in use, accurate and congruent with each other. Therefore, we performed a clinical research, in which the ROM of elbow and forearm and grip strength were measured with a modern computer-assisted tool and with the traditional, transparent goniometer and hydraulic dynamometer. Both methods are currently used at the study institution. The idea was to support or oppose the use of modern measuring method in performing follow-up of the patients with former upper extremity fracture.
The mean values of each motion of elbow and forearm were compared, and the differences were found to be statistically significant regarding all motions except elbow extension. The rotational ROM values were larger when measured with the computer-assisted tool. Flexion–extension ROM of the elbow and hand grip strength, in contrast, seemed to be smaller when measured with the computer-assisted tool. Thus, there were discrepancies between these two methods. Furthermore, scattering around the bias line increased larger as the average elbow extension and forearm pronation and supination increased; this means that the difference increased along with greater measurement values.
Nevertheless, the difference between the two measuring methods of ROM was 8° at its highest, which seemed to be under minimum clinically significant difference and therefore not clinically important (34). Furthermore, this difference is also in line with the natural variation of the traditional free-hand measurements (35). Analyzing the difference between the studied methods with Bland Altman’s method, by defining the statistical intervals of agreement (25, 26), a statistically significant differences were found. However, despite the incongruence and lack of agreement between the study and reference methods, those findings may be beyond clinical significance. The loss of forearm rotational ROM > 30° (4, 36) and the loss of > 15°–10° in the flexion–extension ROM in the elbow have been defined as clinically relevant and unsatisfactory findings (2, 36, 37). In addition, normal pronation–supination movement in the forearm was > 160° in healthy, uninjured cases (37). In this regard, it seems clear that both computer-based modern measuring method and traditional measurements can be used to investigate the motion capacity of the elbow and forearm in children, during follow-up in clinical practice.
When economic effect of the study method and the reference method are considered, it is obvious that the purchase cost of the computer-assisted measuring method is higher. However, there is no difference in operating expenses of the instruments; low additional cost may be needed for hardware or software updates in the long term. In turn, by improving the accuracy, avoiding errors in typewriting and calculations, and contributing in job sharing, the study method may have positive financial effect on patient care.
Furthermore, there are limitations in traditional goniometer measuring. In cadaveric studies, the free-hand measurements generally differed up to 7° in flexion and 10° in extension, when they were compared with the measurements by fluoroscopy (35). For this reason, some studies have recommended that surgeons should use radiographic measuring rather than the goniometer as a gold standard to measure joint movements (14, 38, 39). However, radiographic measuring of ROM—particularly in children—is not acceptable due to its radiation. Neither is it feasible due to high time consumption. Thus, despite its limitations, traditional goniometer measuring has previously been defined as a reasonable measuring tool in clinical use (4). Currently, it is the most commonly used method for measuring movements also for study purposes (14, 40).
The final reason for the statistically significant difference between the study and reference methods remains unknown. When using the universal goniometer, the central black line and the circular degree scale are placed along the midline of the patient’s extremity (14). The computer-assisted tool, however, lacks these qualities, which may complicate positioning the sensor along the upper- and lower-arm axis, which hinders the measuring process. Furthermore, there is no visible central point in the computer-based handle, and the hinge area is not transparent; this may be an essential feature for positioning the instrument precisely in the mechanical central point of the movement. We suggest that adjusting the design of the study measure would improve the agreement with the reference method.
This research has several strengths. It was a prospective, comparative, observational study. The patients presented a homogeneous group of adolescents and children who had suffered from a previous upper extremity fracture. Due to this authentic study population comprising real fracture cases, the findings may be generalized for use within injury units. The study cases were not selected according to any characteristics other than previous fracture. All but one of 60 cases participated. The two educated personnel were trained in measuring techniques, and their interobserver reliability was found to be excellent. The study’s purpose was also highly appreciated because upper extremity fractures are the most common fractures in children, and many new methods have been recently developed to improve their treatment (41). However, some modern innovations have been taken into clinical use without wide scientific evidence; for example, the computer-based measuring method used in this research is conventionally used with adults, hence it had been adopted in pediatric patients despite the sparse existing literature.
As a limitation, we recognize that more studies are needed to validate the findings in wider age groups, including younger patients. In this study, the youngest cases were 10 years of age. The feasibility of the method in children aged <10 years—and particularly preschool children—remains unclear. Furthermore, the feasibility of the computer-assisted method should be tested among children with acute injuries.
Conclusions
Joint movements are essential variables when evaluating the outcome of supracondylar humerus fracture, while >10° of change in elbow ROM associates with impaired function. As compared with the gold-standard goniometer, the study method was not congruent. However, all differences were less than 10° and thus probably beyond clinical importance.
Grip strength is a commonly used index to evaluate impairment and treatment outcome for hand function. The computer-assisted study method resulted in slightly lower grip strength, compared with traditional hydraulic dynamometer, but this difference seemed to be beyond clinical importance.
The study method has advantages in recording the outcomes to electronic charts, avoiding the risk of human type-writing error, while it makes the mathematical estimations automatically and is widely used by other experts than medical doctors. Therefore, the studied computer-assisted method is a potential technique in performing the follow-up of pediatric supracondylar humerus fractures.
Footnotes
Acknowledgements
Emil Aaltonen Foundation, Pediatric Research Foundation, and Alma and K.A. Snellman Foundation supported the study. MD Hanna Hyvönen contributed in writing the article.
Author Contributions
L.K. contributed toward the statistical analysis and wrote the article, while T.P. contributed to both the statistical analysis and the writing of the article, A.H. made the measurements and contributed to the study design and writing of the article, W.S. contributed to the study design and methods and helped revised the article, and J-J.S. was a supervisor who also initiated the study and contributed toward the clinical examinations and writing of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical board approval was previously achieved by the Hospital Ethics Committee of Vaasa Central Hospital as part of an upper extremity fracture study (5/2008) and as a registered amendment by the Northern Finland Ethical Committee. The Helsinki Declaration of human research was recognized, and institutional approval was acquired.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The researchers received study grants from both public national funding (VTR-funding) and nonprofit foundations.