
Abstract
Background:
The benefits of laparoscopic hemi-hepatectomy compared to open hemi-hepatectomy are not clear.
Objective:
This study aims to share our experience with the laparoscopic hemi-hepatectomy compared to an open approach.
Methods:
A total of 40 consecutive laparoscopically started hemi-hepatectomy (intention-to-treat analysis) cases between August 2012 and October 2015 were matched against open cases using the following criteria: laterality of surgery and pathology (essential criteria); American Society of Anesthesiologists score, body mass index, pre-operative bilirubin, neo-adjuvant chemotherapy, additional procedures, portal vein embolization, and presence of cirrhosis/fibrosis on histology (secondary criteria); age and gender (tertiary criteria). Hand-assisted and extended hemi-hepatectomy cases were excluded from the study. The two groups were compared for blood loss, operative time, hospital stay, morbidity, mortality, and oncological outcomes. All complications were quantified using the Clavien–Dindo classification.
Results:
Two groups were well matched (p = 1.00). In the two groups, 10 patients had left and 30 had right hemi-hepatectomy. Overall conversion rate was 15%. Median length of hospital and high dependency unit stay was less in the intention to treat laparoscopic hemi-hepatectomy group: 6 versus 8 days, p = 0.025 and 1 versus 2 days, p = 0.07. Median operative time was longer in the intention to treat laparoscopic hemi-hepatectomy group: 420 min (range: 389.5–480) versus 305 min (range: 238.8–348.8; p = 0.001). Intra-operative blood loss was equivalent, but the overall blood transfusions were higher in the intention to treat laparoscopic hemi-hepatectomy (50 vs 29 units, p = 0.36). The overall morbidity (18 vs 20 patients, p = 0.65), mortality (2.5%), and the positive resection margin status were similar (18% vs 21%, p = 0.76). The 1- (87.5% vs 92.5%, p = 0.71) and 3-year survival (70% vs 72.5%, p = 1.00) was also similar.
Conclusions:
We observed lower hospital and high dependency unit stay in the laparoscopic group. However, the laparoscopic approach was associated with longer operating time and a non-significant increase in blood transfusion requirements. There was no difference in morbidity, mortality, re-admission rate, and oncological outcomes.
Introduction
Laparoscopic liver surgery has seen rapid growth globally over the past decade with over 10,000 cases now reported in the literature (1). The benefits seen across other specialities such as less post-operative pain, reduced blood loss, and shorter hospital stay with faster overall recovery could be some of the reasons for this growth. For patients with cancer, this may allow the earlier initiation of adjuvant treatment (2, 3). However, the uptake of laparoscopy, particularly for major liver resections has been slower than many other surgical specialities with its dissemination making only slow progress globally (4). Furthermore, The Second International Consensus Conference on Laparoscopic Liver Resections concluded that laparoscopic surgery for major hepatectomy is an innovative procedure that is still in the learning phase (4, 5). To a large extent, this relates to the lack of clear consistent and robust evidence, with few studies demonstrating those clear benefits identified across many of the other specialities.
Much of the literature, which has documented laparoscopic liver resections, has focused on resections involving three segments or less and also excluded patients who had a conversion to an open operation (6). Besides, formal comparison trials, particularly those involving major liver resection, have tended to be heterogeneous, regarding the extent and variation of surgical resection despite using the propensity scoring technique (7). Besides, the conversion to open procedure could also affect the outcomes of the laparoscopic approach. It is essential not to exclude these patients in order to evaluate the actual benefits of the laparoscopic approach more accurately. This study aims to evaluate our experience with the laparoscopic approach (intention to treat analysis) hemi-hepatectomies compared to open cases with particular focus on peri-operative outcomes.
Materials and Methods
A total of 40 consecutive laparoscopically started hemi-hepatectomy cases (intention-to-treat-ITT LHH) between August 2012 and October 2015 were included in the study. Laparoscopic extended hepatectomy with or without biliary reconstruction, hemi-hepatectomy patients with biliary reconstruction, and hand-assisted cases were excluded from the study. All laparoscopic cases were matched with an equivalent open hemi-hepatectomy case from a prospectively maintained database.
Matching was agreed based upon a series of essential (primary), required (secondary), and preferred (tertiary) criteria. Essential criteria included laterality of surgery and nature of the pathology. Secondary criteria included the patient’s American Society of Anesthesiologists (ASA) score, body mass index (BMI), pre-operative bilirubin, neo-adjuvant chemotherapy, and additional procedures such as radiofrequency ablation (RFA), non-anatomical liver resections, and portal vein embolization. Secondary criteria also included the presence of cirrhosis/fibrosis on post-operative histology. Tertiary criteria included age, gender, number of lesions, and size of a tumor. Each laparoscopic case was matched with an open case independently by three of the authors (J.C., V.K.M., and B.L). Matching was based solely upon the pre-agreed criteria, and any disagreements between individuals were discussed and scrutinized as a group. Until all appropriate matches were found and agreed, the outcome metrics were not made available to the authors.
The outcomes included the following: intra-operative and overall blood loss; operative time; length of high dependency unit (HDU) and hospital stay; 90-day mortality and morbidity including bile leak, re-operations, and re-admissions; oncological margins (R1 resection taken as a presence of malignant cells within 1 mm from the surgical resection margin); and overall survival at 1 and 3 years. The total operative duration was calculated from skin incision time to the time of neuromuscular blockade reversal recorded on the anesthetic chart. Intra-operative blood loss was calculated using numerous variables including the mean hemoglobin drop, recorded as the difference between the immediate pre-operative level and the lowest recorded level during the post-operative period, as well as the blood transfusion requirement, both intra- and post-operatively. Length of hospital stay was measured from the date of surgery to the discharge date, and intensive care unit stay was measured from the time of admission to HDU until the time of discharge to the ward. All complications were quantified using the Clavien–Dindo classification (8) after going through every patient’s hospital records to make sure every relevant complication data were collected. All patients were followed up for a minimum period of 36 months.
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPPS, Inc., Chicago, IL, USA) version 16. Qualitative data were compared using a χ2 test with Yates’ correction or a Fisher’s exact test when necessary. Normally distributed data are presented as the mean ± standard deviation (SD), and other data are presented as median and range. The independent t-test was employed to compare the means of the two normally distributed groups. Non-parametric tests were used to examine the difference between the two samples when the data had a highly skewed distribution. Kaplan–Meier survival curves were plotted at 1 and 3 years after surgery, and the differences between the two groups were estimated using Wilcoxon log-rank test. All p-values were two-tailed, and p < 0.05 was considered to indicate statistical significance.
Results
A total of 40 patients, of which 16 were males, with a median age of 66 years (range: 59–73) in the ITT-LHH group were matched with 40 open cases according to the pre-determined criteria as described. The details of matching by primary, secondary, and tertiary criteria and demographics of both groups are described in detail in Table 1. Both groups were matched for the laterality of surgery (10 left and 30 right hepatectomy) and histology (malignancy in 34 patients). The most common indication for liver resection was colorectal metastasis (n = 23) in both groups.
Case-matched demographics.
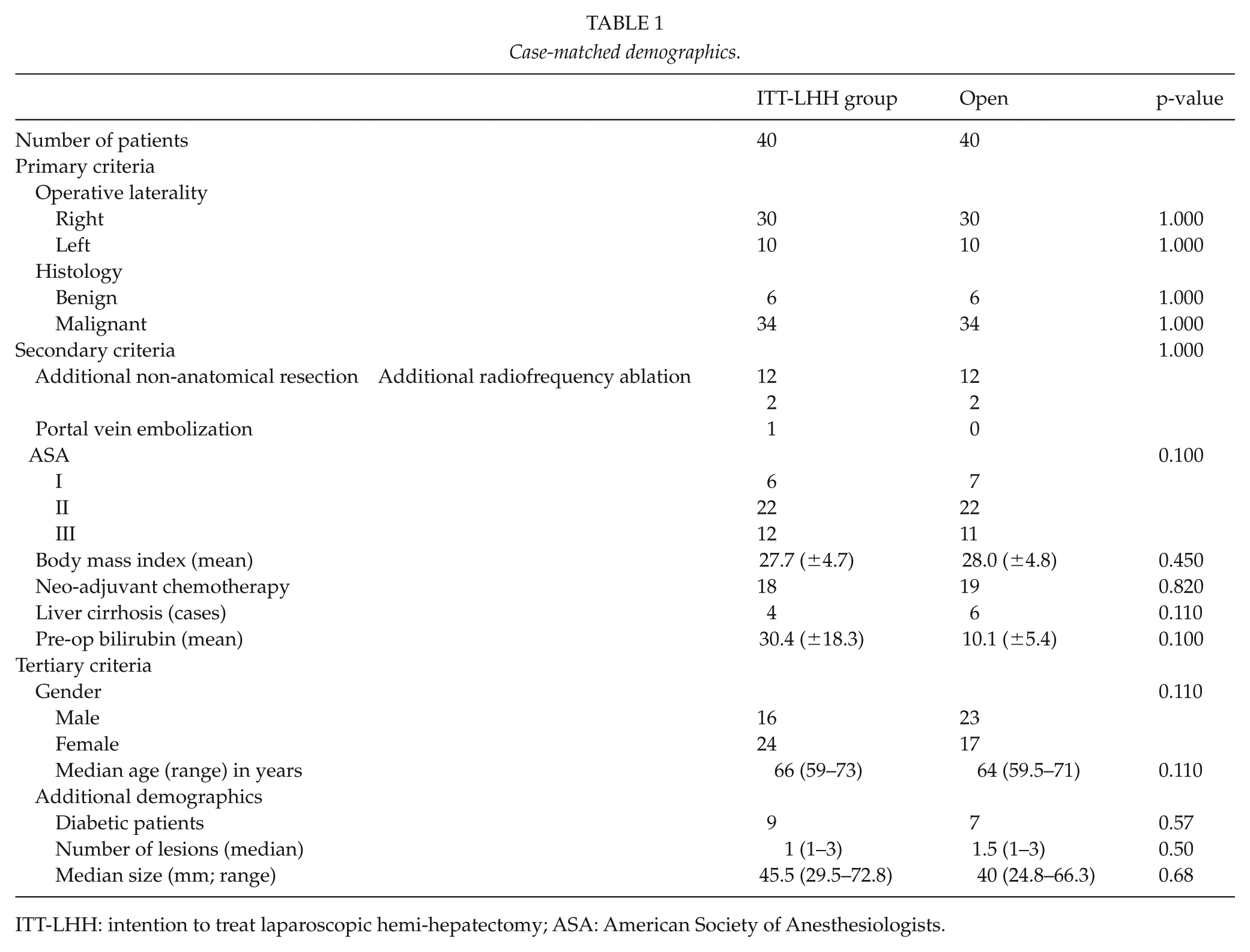
ITT-LHH: intention to treat laparoscopic hemi-hepatectomy; ASA: American Society of Anesthesiologists.
Six patients (15%; left, n = 3 and right, n = 3) had laparoscopic converted to an open operation. The majority of conversions occurred in the first 6 months of the program. The details of the total number of attempted laparoscopic liver resections and the number of procedures that were converted to open are provided in Figs 1 and 2. The main reason for conversion was bleeding (n = 5) and limited access (n = 1) due to body habitus (BMI: 46). In one of the six patients, the laparoscopic procedure was converted to open because of bleeding from non-anatomical resection of a colorectal metastasis after completion of laparoscopic left hepatectomy.
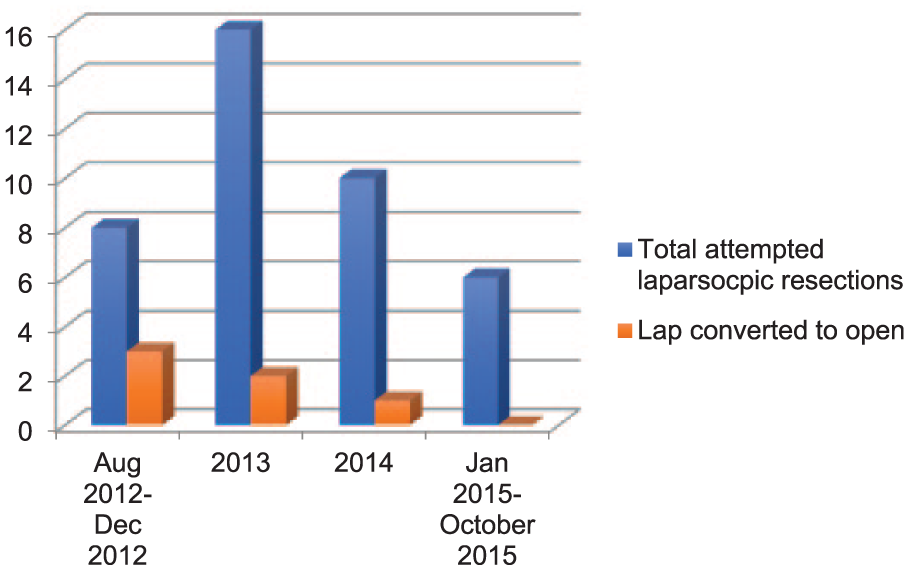
Details of total attempted laparoscopic hemi-hepatectomies and number of patients that had a conversion to open operation.
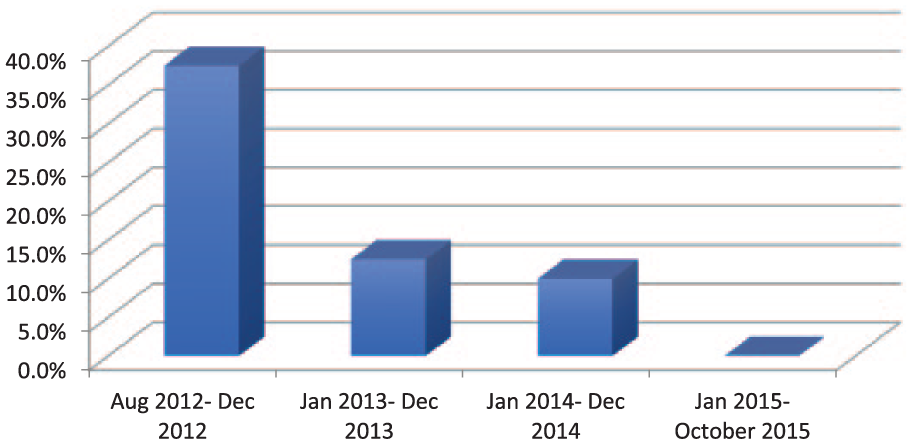
Illustrating the overall conversion rate since the program started in August 2012.
The details of peri-operative outcomes are described in Table 2. The median operating time was shown to be significantly longer in the laparoscopic group compared to the open group (420 min (interquartile range: 389.5–480) versus 305 min (238.8–348.8); p = 0.001). The mean hemoglobin drop was equivalent for the two groups (26.3 and 24.9 g/dL; p = 0.61), with similar hematocrit falls (0.080 and 0.083). In total, 11 patients in the laparoscopic group required a blood transfusion totalling 50 units. In comparison, nine patients received a total of 29 units within the matched open group (p = 0.32).
Details of peri-operative outcomes.
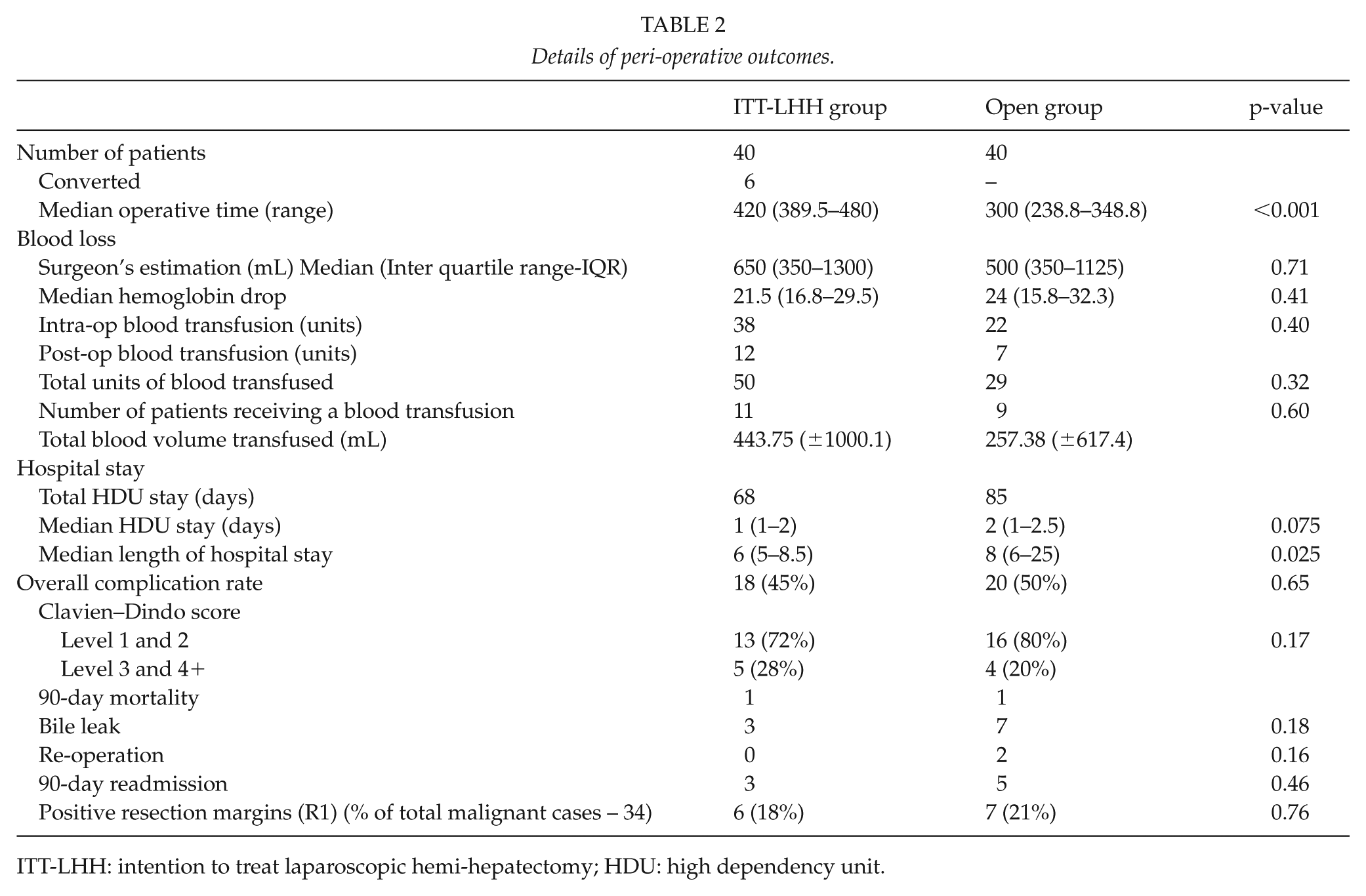
ITT-LHH: intention to treat laparoscopic hemi-hepatectomy; HDU: high dependency unit.
There was a significant reduction in the median length of hospital stay in the ITT-LHH group ((5–8.5) versus 8 (6–10) days; p = 0.025). Overall HDU requirement for the laparoscopic group was 68 days, with patients requiring a median stay of 1 (1–2) day. For the open group, it was 85 days with a median HDU stay of 2 (1–2.25) days, with the difference being not statistically significant, p = 0.075 (Table 2).
Across both study groups, 38 patients (47.5%) experienced a complication as a result of the surgery: 18 (45%) in the laparoscopic and 20 (50%, p = 0.654) in the open group. In total, 55 independent complications were recorded: 33.7% (n = 26) in the laparoscopic group and 36.2% (n = 29) in the open group. A higher percentage of these complications were graded as grade 1 or 2 in the open group compared to the laparoscopic group although it did not reach statistical significance (p = 0.17). Both the open and the laparoscopic groups had nine grade 3 and 4+ complications. Fewer bile leaks were seen in the laparoscopic group (3 vs 7, p = 0.18) with no laparoscopic case requiring a re-operation (Table 2). Two patients in the open group required surgical re-intervention. One of the patients was re-admitted 9 days after discharge with pleural empyema and ultimately required a video-assisted thoracoscopy and washout. The second patient required a re-laparotomy for washout of bile leak and eventually died as a result of sepsis and liver failure. The details of all post-operative complications are described in Table 3. Across the whole study, two patients died (2.5%) at 90 days, one from each group. In the laparoscopic group, one patient died due to a cerebrovascular event on day one. This patient had laparoscopic converted to open procedure due to intra-operative bleeding from the middle hepatic vein. In the open group, one patient died as a result of sepsis and liver failure. Of the 34 malignant cases, 6 in the laparoscopic group (equal left and right hepatectomies) and 7 in the open group had R1 resection margin status.
Details of all post-operative complications.
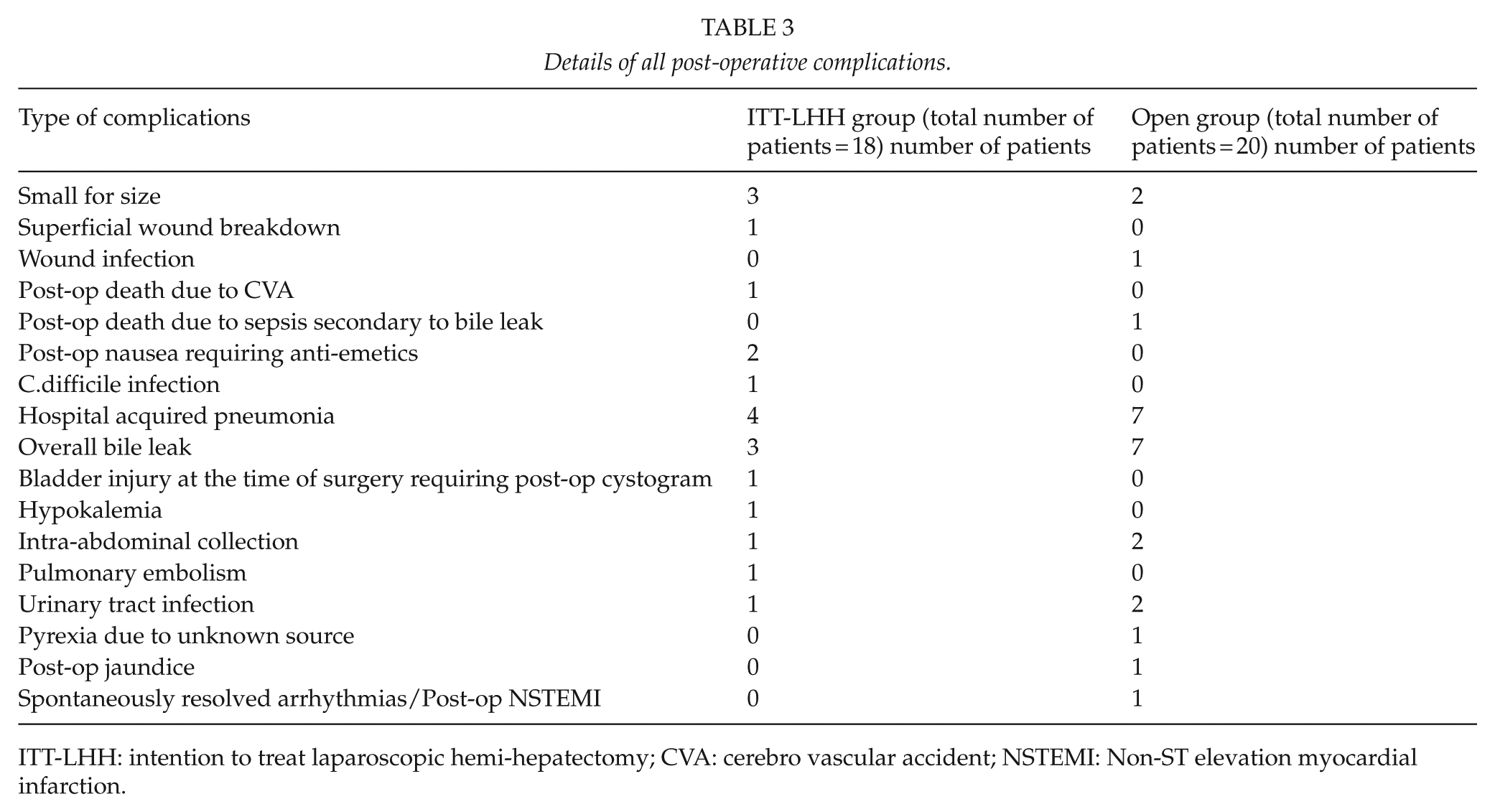
ITT-LHH: intention to treat laparoscopic hemi-hepatectomy; CVA: cerebro vascular accident; NSTEMI: Non-ST elevation myocardial infarction.
There was no difference in the overall survival at 1 and 3 years between the two groups. Patients in both groups were followed up for a minimum period of 36 months. The median follow-up for the total of 80 patients is 54 months (range: 0–163). The median follow-up for the ITT-LHH group is 47.5 months (range: 0–78) and for the open group is 65 months (0–163). The 1-year survival for the whole group is 90%. The 3-year survival for the whole group is 70%. The 1-year survival was not significantly different between the two groups (ITT-LHH: 87.5% vs Open: 92.5%, p = 0.71). The 3-year survival also was not significantly different between the two groups (ITT-LHH: 70% vs Open: 72.5%, p = 1.00). Kaplan–Meier survival estimates revealed no significant association between the type of surgical approach and survival at 1 and 3 years (p = 0.48 and p = 0.62, respectively; Fig. 3).
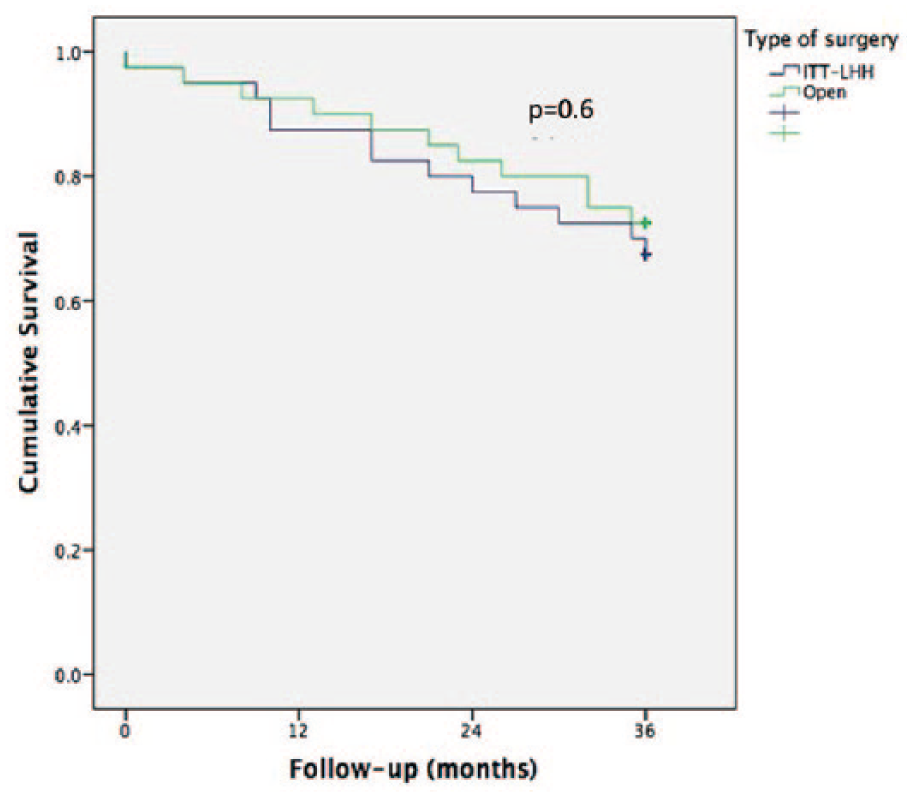
Kaplan–Meier survival curves comparing overall survival for both groups.
Discussion
In this study, we compared the peri-operative and oncological outcomes of laparoscopic hemi-hepatectomy (LHH) with an open approach. In order to find out the extent of benefits the patients received during the laparoscopic procedure, we included all cases that were converted to open. We decided not to use propensity score matching method due to the small sample size and to avoid potential bias associated with propensity score matching method (9). Instead, we chose to match each laparoscopic case with an open case on 15 separate variables by three independent authors.
There are very few published series like our series that compared pure LHH cases with open hemi-hepatectomy cases (10–12). Ratti et al. (10) compared 49 laparoscopic major hepatectomies with 585 open hepatectomies on 1:3 ratio and found that there was decreased blood loss, early functional recovery, and increased operative time in the laparoscopic group. Our results are similar to this study except that we found a minor increase in blood loss and higher blood transfusion requirements in the laparoscopic group.
In a study of 159 consecutive laparoscopic major hepatectomies, Van der Poel et al. (11) observed longer median operative time and lower median blood loss in the laparoscopic group. Lau et al. (13) evaluated the outcomes of all laparoscopic cases including the ones that were converted to open and did not find any difference with the open group with regard to overall complication rate, mortality, morbidity, blood loss, operating time, and length of hospital stay. Yoon et al. compared laparoscopic right hepatectomy with open right hepatectomy for hepatocellular cancer using propensity score matching method. They found decreased morbidity, decreased length of stay, and increased operation time in the laparoscopic group. However, there was no difference in blood loss and oncological outcomes between the two groups (12). Nomi et al. compared the outcomes of laparoscopic major hepatectomies with an open group in patients over the age of 70 years. They did not observe any difference in duration, blood loss, transfusion rate, morbidity, and mortality (14). The overall bile leak rate of 12.5% for the whole group is comparable to the published literature (15–17). We observed a non-significant higher bile leak rate in the open group (17.5% vs 7.5%). In a study by Cauchy et al. (15), the bile leak rate was 13.5%. In another study by Braunwarth et al.(16), the overall bile leak rate was 11%. In a systematic review and meta-analysis of studies comparing bile leakage test group versus no bile leakage test, Wang et al.(17) observed 9.6% bile leak rate in the untested group.
The control of bleeding is much more challenging in the context of the laparoscopic approach. Unfortunately, lack of specific laparoscopic training and skills to control bleeding in a timely fashion can result in conversion to open operation. Although conversion to open procedure is not a failure, it can affect the overall outcomes of the laparoscopic approach and can put surgeons off taking up (18). In the published series, conversion rates ranged from 0% to 36% (11, 13, 18). In our series, the overall conversion rate was 15%, which is similar to the published series. The majority of conversions in our series were in the first 12 months of the program with a conversion rate of 37.5% compared to 0% in 2015. Within this series, except one, all other conversions were due to bleeding. Cai observed that in 45.9% of cases, the conversion to open operation was due to bleeding (19). Conversion to an open operation will affect the overall outcomes: in a retrospective review of 400 laparoscopic liver resections performed between 2006 and 2017, Goh et al.(20) found an increased operative time, blood loss, blood transfusion rate, and post-operative morbidity and mortality in the group that had conversions. In our series, 76% of total blood transfusion requirements were for patients that had laparoscopic converted to open procedure.
Whether overall better patient selection or general technical improvement will minimize the conversion rate is difficult to identify from this study. The majority of converted cases occurred within the first year of the learning curve; the implication of this is that a long learning curve should be expected with the laparoscopic technique. Many studies have explored the learning curve in an attempt to formalize a figure upon which to meet proficiency, but as always it has proved difficult to accurately predict, with up to 190 cases being proposed (21, 22). In our own experience, we noted an essential reduction in conversions to open surgery after an acquisition of a 2-year experience with 20 cases. Goh et al.(18) observed decreased mortality, morbidity, and length of stay after acquiring experience with 20 major hepatectomies. Nomi et al.(14) noted that 45 major liver resections were required for reducing operative time. Yamada et al. noted decreased blood loss and conversion rate in their unit where there was a stepwise training program and standardization of the procedure. They found no difference in the blood loss and operative time between the young and senior surgeon group (23). However, from the literature review, we have not found any studies that found a definite number beyond which the conversion rate, operative time, blood loss, and post-operative complications go down significantly. The Southampton Consensus Guidelines for Laparoscopic Liver Surgery have suggested that learning curve for major hepatectomies is 55 for surgeons with expertise in performing minor liver resections (24). The learning curve will depend on several factors including the case-load, experience of surgeons in other areas of laparoscopic surgery, and the availability of a structured training program. In a recent study, Halls et al.(25) showed that with specific training, early adapters could overcome the learning curve much faster than the self-taught pioneers, emphasizing the importance of structured laparoscopic training.
The oncological safety of the laparoscopic operation is well established. Similar to the published literature, we did not find any difference in the R1 resection margin status between the two groups (18% vs 21%) (26). In a review of 9000 laparoscopic cases, Ciria et al.(1) reported that an adequate tumor-free margin was obtained in 82%–100% of cases. In a study by Pencovich et al., the overall R1 resection rate was 20.3%. They also noted that the long-term outcomes of colorectal liver metastasis patients with R1 resection were not inferior to patients who had R0 resection (27). In another large series by Hosokawa et al.(28), the overall R1 resection rate was 49%. We did not find any difference in the overall 1- and 3-year survival between both groups. We could not compare our overall survival figures with the published literature as we included both benign and malignant cases in both groups. We feel that a subset analysis would be inappropriate as it would defeat the purpose of the study, that is, comparing outcomes of laparoscopic technique with an open approach.
One of the main concerns with laparoscopy in this setting, not dealt with in this study, is the cost. Although for minor resections the evidence supports the cost-saving benefit over the open resection, there remains little data in the literature that convincingly addresses this issue for major resections. However, a single study, which reviewed the cost analysis comparing open and laparoscopic right hepatectomies from the United States, concluded that the laparoscopic right hepatectomy was cost neutral to the open equivalent, although the cases in the study were not stringently matched (29). The remaining evidence suggests that there are higher operating room costs with equivocal in-patient hospital-related costs, although the evidence was not generated using appropriate health care economic analysis, which would include the indirect cost benefits (30).
There are limitations to our study that need to be addressed. It is a small single-center, retrospective study. We decided only to evaluate the outcomes of laparoscopic hepatectomies and excluded hand-assisted and all other laparoscopically performed liver resections. Laparoscopic hemi-hepatectomy is not a commonly performed operative procedure across many centers in the United Kingdom. Even in the centers that are providing this service, only a few surgeons are performing this procedure. In our unit, only one surgeon (S.A.) performs laparoscopic major hepatectomy, which explains the limited sample size. Although this is a retrospective study, the data are collected prospectively, and the matching technique issue has already been addressed.
We can, therefore, conclude that the laparoscopic major hepatectomy is a safe operation with similar mortality and morbidity compared to an open approach. The laparoscopic approach reduces overall hospital and HDU stay. However, we cannot forget the additional 2 h of operating time and its cost implications. The benefits of reducing blood loss, evident across other specialities which have adopted the laparoscopic technique, have not been demonstrated in this series. There is no clear evidence from this study, which could either categorically denounce or promote the introduction of the laparoscopic technique for major liver resections. However, in concordance with the results of previous studies, it appears that the acquisition of experience over time leads to improvement of the operative outcomes. The outcomes from the ongoing Orange II Plus trial are anticipated, in the hope that they may answer some of these outstanding questions and confirm whether there is indeed a role for laparoscopy for major liver resection and to what extent that may be (31).
Footnotes
Acknowledgements
This work has been presented in part as a poster presentation at the GBIHPBA 3rd Annual Scientific Meeting 2016, The Chesford Grange Hotel, Leamington Spa, Warwickshire, UK, 17–18 March 2016, and as an oral presentation at the 12th Biennial E-AHPBA Congress 2017, 23–26 May 2017, Mainz, Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.