
Abstract
Background and Objectives:
The International Study Group of Liver Surgery established the first internationally standardized definitions and grading for posthepatectomy hemorrhage, posthepatectomy liver failure, and bile leakage. We aimed to correlate these definitions and grades of complications with objective parameters of the postoperative course, namely, mortality and length of stay, to assess the usefulness in clinical routine.
Methods:
A total of 415 patients underwent hepatic surgery between 2004 and 2014. Uni- and multivariate analyses were made for correlations of posthepatectomy hemorrhage, posthepatectomy liver failure, and bile leakage with perioperative parameters and mortality.
Results:
Of the total, 25 (6.1%) patients developed a posthepatectomy hemorrhage Grade A, 3 (0.7%) patients a posthepatectomy hemorrhage Grade B, and 1 (0.2%) patient a posthepatectomy hemorrhage Grade C; 23 (5.5%) patients had a posthepatectomy liver failure Grade A, 24 (5.8%) patients a posthepatectomy liver failure Grade B, and 7 patients (1.6%) a posthepatectomy liver failure Grade C. Bile leakage Grade A occurred in 10 (2.4%) patients, bile leakage Grade B in 24 (5.8%) patients, and bile leakage Grade C in 7 (1.6%) patients. Mortality was significantly increased in patients with posthepatectomy hemorrhage Grades B and C and in patients with posthepatectomy liver failure Grades A, B, and C. Three (42.9%) patients with bile leakage Grade C died.
Conclusion:
Our data indicate that the new definitions correlate well with mortality and duration of hospital stay.
Introduction
Advances in perioperative management and surgical techniques, as well as in the management of complications have improved patients’ outcome after liver surgery markedly within the past three decades (1, 2). Along with the improved safety, indications have been widened. Extended resections and resections in patients with underlying liver disease or chemotherapy-related parenchymal injury are routinely performed and therefore complications are still frequent (3). Typical complications of liver resection are posthepatectomy liver failure (PHLF), posthepatectomy hemorrhage (PHH), and bile leakage. Until recently, there were no internationally accepted classifications of PHH, liver failure, and bile leakage. Therefore, the comparison of results from clinical trials is difficult and the assessment of postoperative complications is often based on subjective parameters (4).
In 2010, the International Study Group of Liver Surgery (ISGLS) first published the new consensus definition for PHLF (1) and bile leakage (5), followed by the consensus definition for PHH in 2011 (6). Standardized classification can support the early identification and risk stratification of these complications, enabling better management of these defined events. Unfortunately, these new classifications of PHH, PHLF, and bile leakage lack clinical validation. Therefore, the aim of this study was to provide more evidence regarding the new ISGLS definitions by applying strictly objective parameters, namely, mortality and length of stay. By means of this, we tried to assess the value of these three clinical risk indices as early postoperative predictors of outcome.
Methods
Patients and Data Collection
This retrospective and unicentric study was based on the prospective Mannheim liver database, some of the patients are already part of previous publications (7). All patients with minor or major liver resection at our department between 2004 and 2014 were included. Biopsies, wedge resections, traumatic lesions, or liver resections in the context of other operations were excluded. The variables recorded include patient characteristics, like patients’ age, Child–Pugh score, sex, American Society of Anesthesiologists (ASA) grade, body mass index (BMI), pre-existing cardiac condition, pre-existing pulmonary condition, pre-existing renal condition, arterial hypertension, and diabetes mellitus type 2. Additional, comprehensive preoperative laboratory parameters are listed. Perioperative parameters include the extent of liver resection (minor or major resection), entity of the liver tumor, the amount of perioperatively used packed red blood cells (PRBCs), Pringle maneuver, and laparoscopic surgery. The study was approved by the local ethics committee.
Definitions
Mortality
Perioperative mortality was defined as an in-hospital mortality or 30-day mortality.
Preexisting pulmonary, renal, and cardiac conditions
These conditions are defined as any pulmonary and cardiac disease that needed regular medication or therapeutic intervention. In the case of pulmonary disease, this means asthma, emphysema, and chronic obstructive pulmonary disease (COPD). In the case of cardiac disease, this means the presence of a defibrillator or pacemaker, significantly reduced cardiac function, or the presence of stents or an artificial cardiac valve. In the case of renal diseases, this means dialysis or significantly reduced renal function. Bilirubinemia was defined as serum bilirubin level higher 2.0 mg/dL. A routine laboratory workup for bilirubin levels in abdominal drains was only performed in cases with suspicion of bile leakage. Serum albumin level lower than 32 mg/dL was defined as hypoalbuminemia. Based on the existing data, we categorized postoperative hemorrhage, liver failure, and bile leakage according to the ISGLS consensus definition.
ISGLS definitions
PHLF, PHH, and bile leakage were defined according to the ISGLS definition (Tables 1S, 2S, and 3S in Supplemental data) (1, 5, 8). All parameters necessary for the assessment of the definitions were stored in our database. The grading was performed retrospectively.
Operations
Within the liver database, procedures are named according to the definition of the Brisbane Terminology (9): Major hepatectomy was defined as the resection of two or more segments. Minor hepatectomy is the resection of less than two segments (10). Central hepatectomy was defined as anatomical segment 4, 5, 8 ± 1 liver resection. Indications for surgery included primary and secondary malignant liver tumors and benign tumors.
Statistical Analysis
The statistical analyses were performed using SPSS for Windows, version 15.0 (SPSS Inc., Chicago, IL, USA). All clinical and pathological characteristics were stratified to build categorical or nominal variables. The thresholds used for categorization were based on previously described thresholds in the literature (11) and/or normal cut-off values in the case of laboratory values. Ordinal scaled variables were compared using the chi-square test. Factors significant (at p < 0.10) at the univariate level were entered into the multivariate model. Cox regression analysis with stepwise backward elimination based on the likelihood ratios was employed to test for independent predictors of survival. A p-value <0.05 was considered to be significant. Missing data never exceeded 10%.
Results
Patient Cohort
Of the 415 patients who met our inclusion criteria, we identified 196 (47.2%) major resections and 219 (52.8%) minor resections (Fig. 1). The patient group consisted of 247 men (59.5%) and the average age was 60.1 years (Table 1). Most patients were classified as ASA grade II (n = 170, 41%). Of the patients, 115 (27.7%) had a pre-existing cardiac condition and 72 (17.3%) had a pre-existing pulmonary condition; 18 patients (4.3%) had bilirubinemia. A low albumin level was present in 53 cases (12.8%). The mean Model for End-Stage Liver Disease (MELD) score was 7.5 (standard deviation (SD) 2.4). Furthermore, we assessed a Child–Pugh Grade A for 30 (7.2%) patients and Grade B for 6 (1.4%) patients. One patient had Child–Pugh Grade C liver cirrhosis. In this 54-year-old female patient, we performed a segment 5 resection for cholangiocellular carcinoma (CCC). Due to the size of the tumor, nearly no functional liver tissue was lost. The operation was performed after extensive information from the patient and because the patient insisted on being operated. Postoperatively, 19 patients died, resulting in a perioperative mortality of 4.5%.

Patient cohort.
Characteristics of the patient cohort.
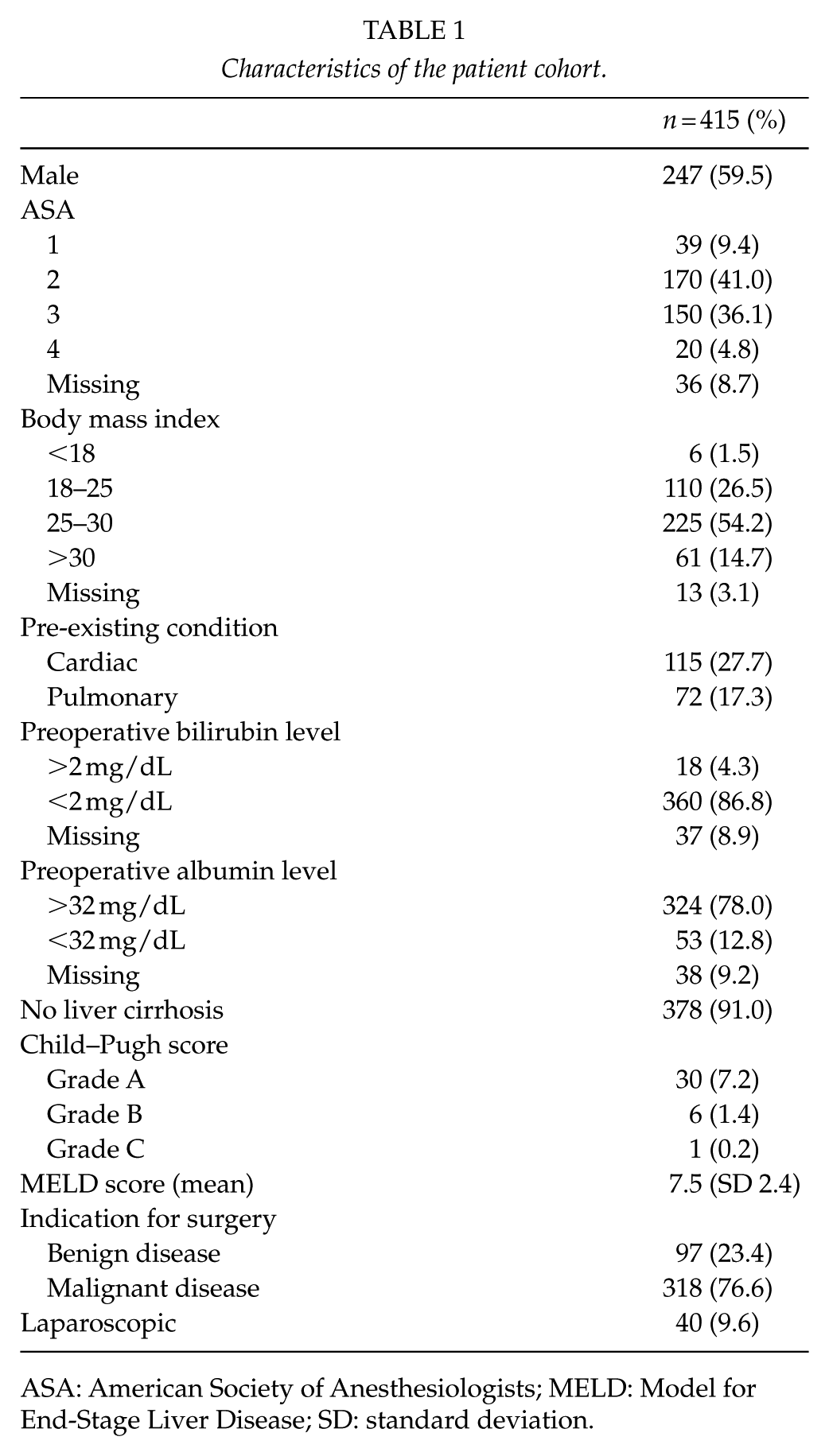
ASA: American Society of Anesthesiologists; MELD: Model for End-Stage Liver Disease; SD: standard deviation.
Procedures Performed
Patients with major liver resections received the following procedures: 44 (11.0%) right hemihepatectomies, 29 (7.3%) left hemihepatectomies, 27 (6.8%) extended right hemihepatectomies, 10 (2.5%) extended left hepatectomies, 14 (3.5%) central hepatectomies, 26 (6.5 %) left lateral sectionectomies, and 46 (11.0%) anatomical resections of more than two segments. In 37.1% of the cases, the Pringle maneuver was applied. In total, 40 (9.6%) of the procedures were laparoscopic. The mean length of the operation was 218.7 min (SD 102.9), and the mean blood loss was 729.7 (SD 1098.4) mL. Pathological examination showed a neoplasm in 318 (76.6%) patients and benign liver disease in 97 (23.4%) patients (Table 1). In this cohort, histopathological findings of malignancies were as follows: 223 metastases (53.7%), 53 (12.8%) with hepatocellular carcinoma (HCC), 24 (5.8%) with CCC, and 18 (4.3%) with Klatskin tumor or gallbladder cancer.
Prevalence of PHH and Grading
Of the 415 patients, 29 (7.6%) developed PHH: 25 (6.1%) of these patients were classified as PHH Grade A, 3 (0.7%) as Grade B, and 1 (0.2%) as Grade C. Among the three patients with Grade B PHH, we could observe a significantly prolonged duration of hospitalization (length of hospital stay (LOS)) of 46.7 (SD 57.5) days, whereas patients without PHH stayed only 13.4 (SD 8.7) days (p < 0.001; Table 2 and Fig. 2). The patient with PHH Grade C stayed 12 days; due to the small sample size, we could not perform statistical analysis. The mortality was significantly increased in patients with PHH Grade A (n = 3, 12%), PHH Grade B (n = 1, 33.3%), and PHH Grade C (n = 1, 100%) compared to patients without PHH (n = 14, 3.9%, p < 0.001; Table 3 and Fig. 3).
Association of complications with length of stay (LOS) in hospital.
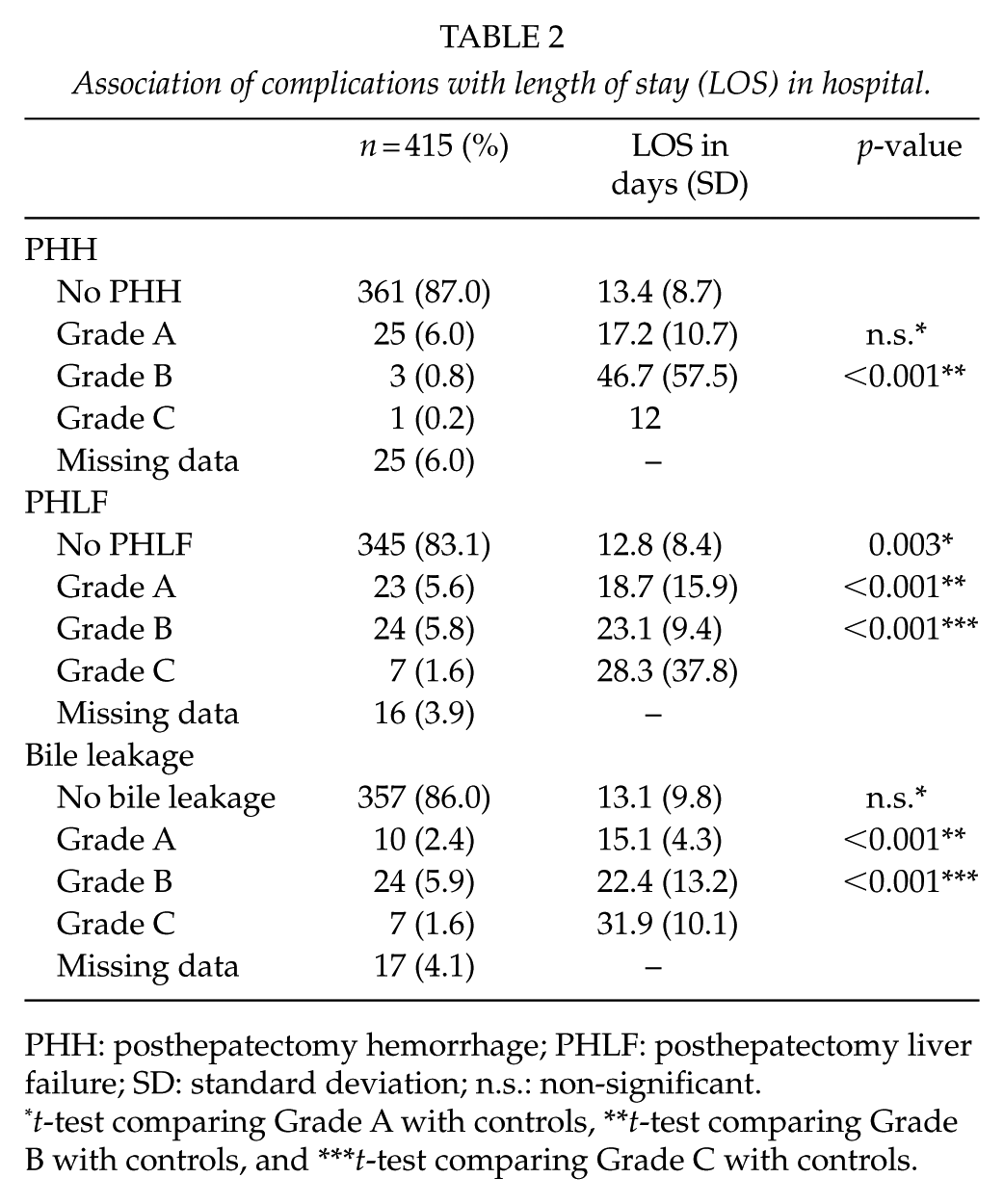
PHH: posthepatectomy hemorrhage; PHLF: posthepatectomy liver failure; SD: standard deviation; n.s.: non-significant.
t-test comparing Grade A with controls, **t-test comparing Grade B with controls, and ***t-test comparing Grade C with controls.
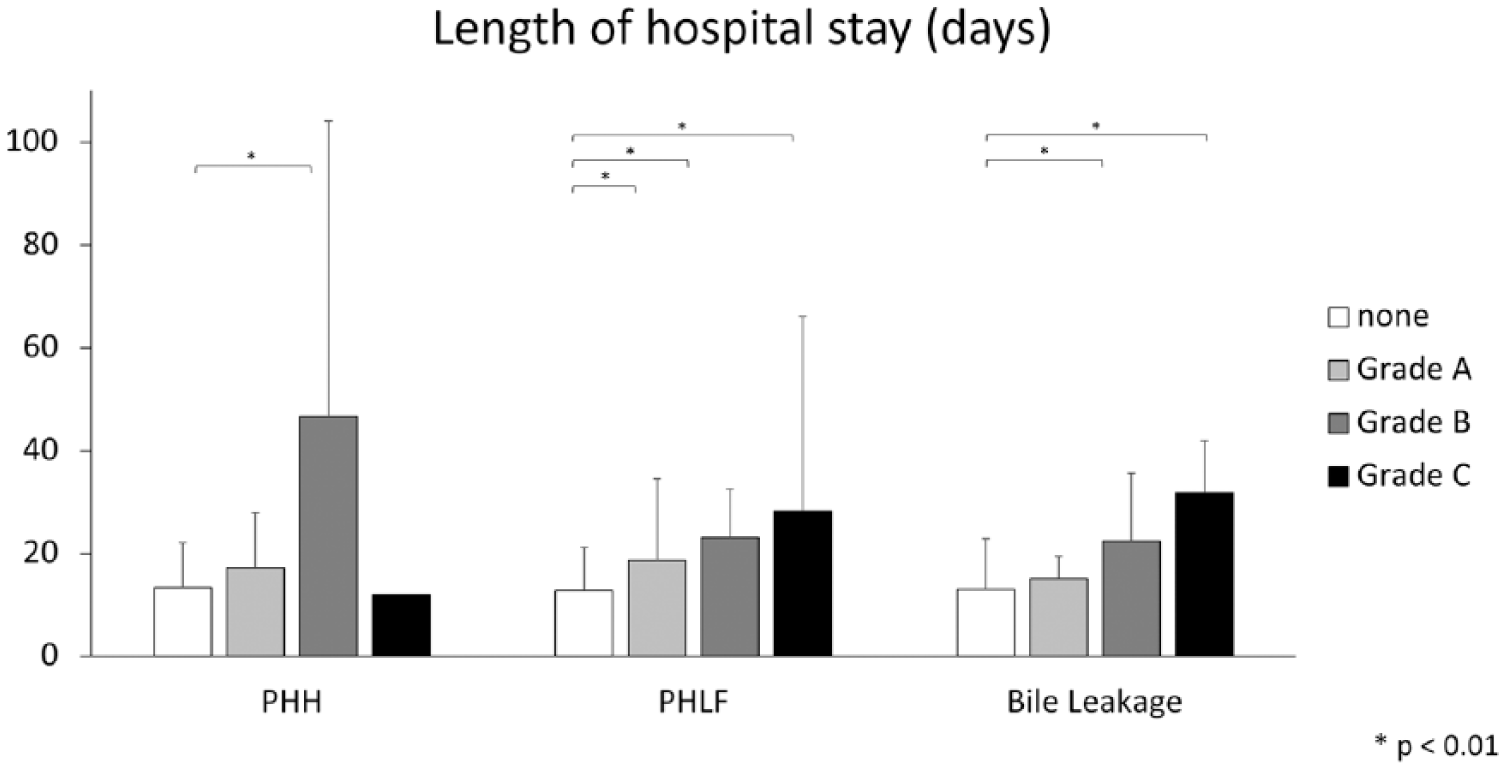
Length of hospital stay (LOS) in days: distribution of LOS (mean) was displayed by severity grading of PHH, PHLF, and bile leakage according to ISGLS definitions. Bars indicate standard deviation. Significant values are marked by *p < 0.01.
Association of complications with mortality.
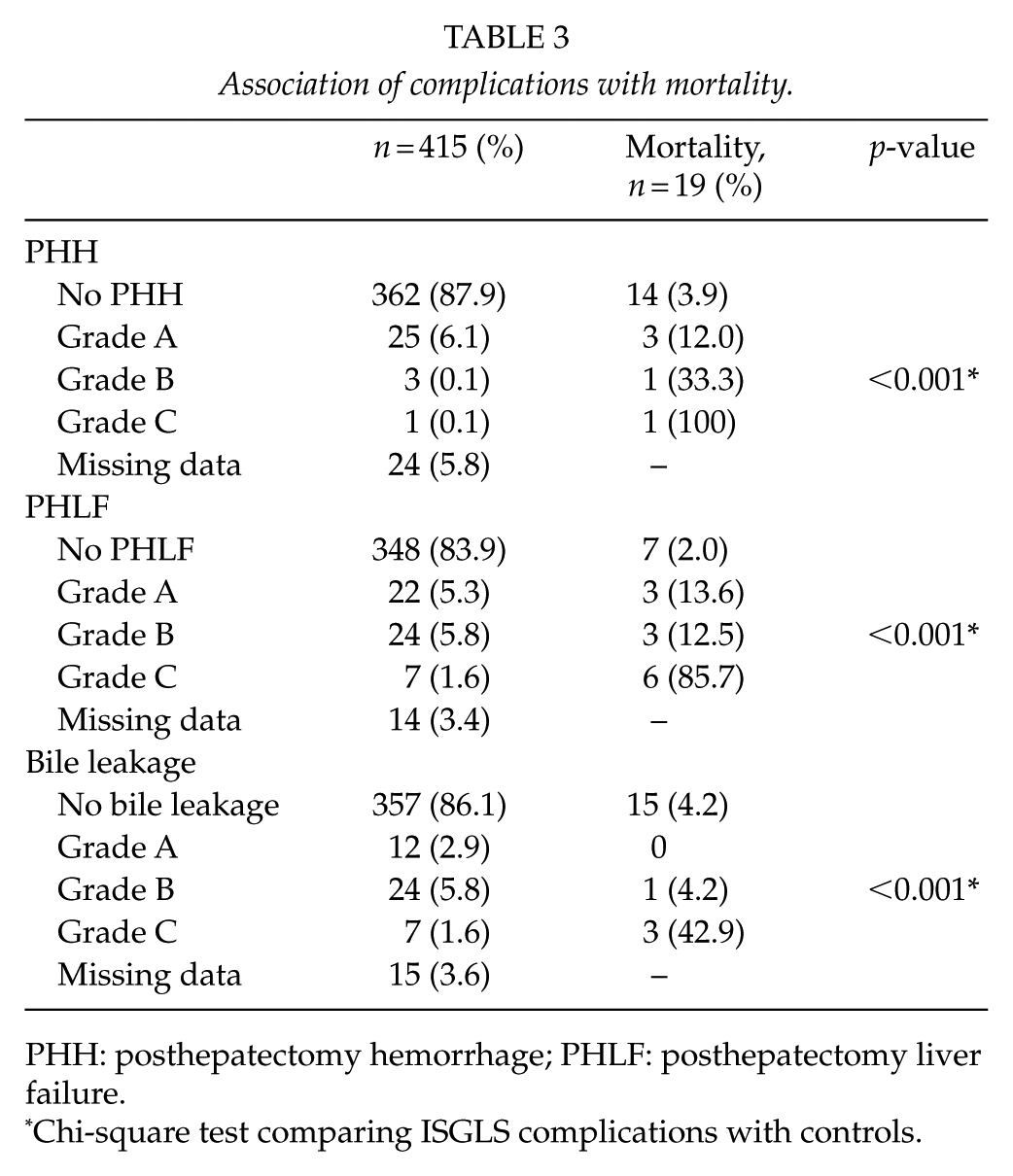
PHH: posthepatectomy hemorrhage; PHLF: posthepatectomy liver failure.
Chi-square test comparing ISGLS complications with controls.

Mortality (%): mortality rate (%) was displayed by severity grading of PHH, PHLF, and bile leakage according to ISGLS definitions. Significant values are marked by *p < 0.01.
Prevalence of PHLF and Grading
In total, 23 (5.5%) patients were graded as PHLF Grade A, 24 (5.8%) as PHLF Grade B, and 7 (1.6%) as PHLF Grade C. PHLF Grade A (18.6 (SD 15.9) days, p = 0.003), Grade B (23.1 (SD 9.4) days, p < 0.001), and Grade C (28.3 (SD 37.8) days, p < 0.001) all had a statistically significantly longer LOS compared to controls (12.8 (SD 8.4) days; Table 2 and Fig. 2). A significantly increased mortality rate was observed in patients with PHLF Grade A (n = 3, 13.6%), PHLF Grade B (n = 3, 12.5%), and PHLF Grade C (n = 6, 85.7%) compared to patients without PHLF (n = 7, 2.0%, p < 0.001; Table 3 and Fig. 3).
Prevalence of Bile Leakage and Grading
Among the 415 assessed patients, 43 (10.4%) were classified as having bile leakage: 10 (2.4%) of these had bile leakage Grade A, 24 (5.8%) had bile leakage Grade B, and 7 (1.6%) had bile leakage Grade C. Patients with bile leakage Grade A had no significantly prolonged LOS. The LOS of patients with bile leakage Grade B was 22.4 (SD 13.2; p = 0.001) and 31.9 (SD 20.1; p = 0.001) days for patients with Grade C. Patients without bile leakage stayed on average 13.1 (SD 9.8) days (Table 2 and Fig. 2). In comparison to patients without bile leakage (n = 15, 4.2%), the mortality was significantly increased for patients with bile leakage Grade B (n = 1, 4.2%) and bile leakage Grade C (n = 3, 42.9%, p < 0.001; Table 3 and Fig. 3).
Uni- and Multivariate Analyses
We performed uni- and multivariate analyses to identify the possible risk factors for the incidence of severe complications (Grades B and C). For this purpose, we grouped all complications into mild (none resp. Grade A) and severe (Grades B and C). The following parameters were included for univariate analysis: sex, preoperative comorbidities, ASA grade, histological finding of malignancy, Child–Pugh score, extent of resection, and preoperative serum levels of bilirubin, albumin, and creatinine. Univariate analysis showed that the risk factors for severe PHLF were elevated preoperative bilirubin (p = 0.01), low albumin (p = 0.046), malignant disease (p = 0.05), and the extent of resection (p << 0.001). Multivariate analysis confirmed the preoperative level of bilirubin (odds ratio 8.38; p-value 0.003) and the extent of resection (odds ratio 18.93; p-value >> 0.001) to be significant risk factors for the incidence of severe PHLF.
Univariate analysis showed that the risk factors for PHH were the extent of resection (p < 0.001), elevated creatinine (p = 0.015), and elevated preoperative bilirubin levels (p = 0.003). There were insufficient cases with severe PHH (n = 4) to perform multivariate analysis.
Univariate analysis showed that cardiac disease (p = 0.025), elevated creatinine (p = 0.02), and the extent of resection (p < 0.001) were the risk factors for the occurrence of bile leakage. Multivariate analysis for bile leakage confirmed the extent of resection to be the only significant risk factor (odds ratio 15.82; p-value << 0.001; Table 4S).
Discussion
The complication rate is commonly used to compare the performances of surgical centers but also to compare the results of surgical clinical trials (12). Unclear definitions of complications render the assessment of trials or surgical performances difficult. One solution for better assessment is to refer to objective parameters such as mortality or the LOS. Another possibility is to establish clear definitions for typical surgical complications by consensus conferences. The aim of this study was to provide more evidence regarding the new ISGLS definitions of PHLF, PHH, and bile leakage by retrospectively analyzing the association of these parameters with objective parameters such as mortality and LOS. It is also important to state that mortality in the definitions Grade B are not essentially causally related to the complication itself (which then would be graded as C) but to secondary complications such as pneumonia and myocardial infarction.
In the present analysis, we considered 415 patients, among which 219 underwent minor liver resection and 196 underwent major liver resection. This number of patients seems to be sufficient to address the aim of this study, as the number of patients is within the range reported in previous studies (13–15). In particular, a definition for PHLF seems to be important, as an increasing number of patients receive extended liver resections. These patients often have limited function of liver due to neoadjuvant chemotherapy or underlying liver disease. Therefore, the probability of PHLF is high and has to be considered by responsible surgeons. In our patient cohort, PHLF Grade A occurred in 5.7% of the patients, Grade B in 6% of the patients, and PHLF Grade C in 1.7% of the patients. This is within the range reported in previous publications (16, 17). The new classification correlated well with LOS and mortality. Therefore, the score seems to be useful for routine use and for clinical trials. To identify the risk factors for PHLF, we performed uni- and multivariate analyses. Multivariate analysis only confirmed preoperative level of bilirubin and the extent of resection as the risk factors. Both are known risk factors for PHLF (18). The high odds ratios of 8.38 for elevated bilirubin levels and 18.93 for major hepatectomies suggest that both factors are very important. However, both factors are already considered in the perioperative management by specialists and can be explained considering the need for functional liver parenchyma. We hypothesize that the Child–Pugh score was not significant due to the low number of patients with cirrhosis in advanced stages caused by preoperative patient selection.
Postoperative intraperitoneal hemorrhage is a rare complication after liver resection and usually occurs within 48 h. It is perhaps the most difficult complication to assess because the operative setting in liver surgery requires a low central venous pressure. This, in combination with even a limited intraoperative blood loss, causes a drop in the postoperative hemoglobin level when patients receive infusion. Because many patients also have traces of blood in their tubes, it has to be considered on an individual basis if patients really develop PHH or not. This is the first time that the new definition is evaluated in a clinical setting. Only four patients experienced a clinically relevant PHH in our patient cohort, and this low number is in accordance with the previous data (19–21). Interestingly, the new definition of the ISGLS is only infrequently used (19–22). Although only a few patients had PHH Grades A and B, we could assess a significant prolongation of LOS and increase in mortality compared to controls. Therefore, although difficult to assess, the new definition seems to be useful in clinical settings and research. Unfortunately, we could not evaluate the risk factors due to the small number of patients with severe PHH.
According to the new definition of bile leakage, 6.4% of our patients had Grade A, 6% had Grade B, and 1.7% had bile leakage Grade C. While patients with bile leakage Grade A had no significantly prolonged LOS, the patients with Grades B and C had significantly longer LOS. The mortality was also significantly increased for patients with bile leakage Grades B and C. These figures are in the range of the previously published data (23, 24). One point that was already discussed earlier was that Grade A biliary leaks do not constitute a significant leak and should not be part of a definition for bile leak. According to this, our patients with bile leakage Grade A had no prolonged LOS and no increased mortality. One factor was identified that was a risk factor for severe bile leakage: the extent of resection with an odds ratio of 15.82. Bile leakage is exceptional after minor hepatectomy. This circumstance is difficult to understand as the resectional plane after segmentectomies is even or can even be larger than that after major hepatectomy. The underlying physiological explanation might be that the danger of lesions to larger bile ducts is higher in major hepatectomies.
In conclusion, the results of this study are limited due to the small number of patients and the retrospective setting. Furthermore, we could not assess the impact of chemotherapy, particularly on PHLF and PHH, due to wide variations in chemotherapy agents and indications in the patient cohort. However, the new definitions for the occurrence of PHH, PHLF, and bile leakage of the ISGLS correlate well with LOS and mortality. Subsequently, the definitions seem to be suitable for both concepts of quality assurance and clinical trials. Due to the simple application, they are particularly effective for everyday clinical use.
Supplemental Material
supplemental_data_re-re-revision – Supplemental material for Evaluation of the New ISGLS Definitions of Typical Posthepatectomy Complications
Supplemental material, supplemental_data_re-re-revision for Evaluation of the New ISGLS Definitions of Typical Posthepatectomy Complications by E. Birgin, W. Tesfazgi, M. Knoth, T.J. Wilhelm, S. Post and F. Rückert in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
*E.B. and W.T. contributed equally to this work. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.