
Abstract
Background and Aims:
To evaluate hospital care of children with congenital upper limb defects.
Materials and Methods:
Three hundred and sixty-two children with an upper limb defect, born 1993–2005, and alive after birth admission were identified in the Finnish Register of Congenital Malformations. The data on hospital care, with focus on operative treatment, were collected from the National Hospital Discharge Register, until 31 December 2009. Mean follow-up was 10.2 years (range: 4–17 years). The results were compared with data on the whole children population (1.1 million) in Finland.
Results:
Most children (321, 87%) with upper limb defects had hospital admissions: on average, one admission/year (range: 0–36), and they were treated in hospital 5 days/year (range: 0–150), which is 11-fold compared with an average child in Finland. Four surgical procedures/child were done (range: 0–45), including one hand surgical procedure. The most common procedures were orthopedic (513); gastrointestinal (263); ear, nose, and throat (143); dental (118); thoracic (48); and urologic (44). Of the 513 orthopedic procedures, 326 were directed to upper limbs, 107 to the lower limbs, and 10 to the spine. Median operation age was 2 years 7 months. Altogether, 60% of hospital admissions were non-surgical. Leading causes of non-operative hospital admissions were congenital anomalies (32%), gastroenterological problems (20%), respiratory tract conditions (13%), neurological problems (7%), perinatal conditions (5%), and infectious diseases (5%).
Conclusion:
Treatment of children with upper limb defects is teamwork between pediatric and surgical subspecialties. Burden of hospital care is 11-fold as compared with an average child.
Keywords
Introduction
Birth prevalence of upper limb defects in Finland is 5.3 per 10,000 live births (1). Some upper limb defects, especially radial ray defects, are strongly associated with other anomalies (2). The burden of hospital care among these children, specifically in terms of the number of admissions and total time spent in hospital, is currently unknown. Limb defects are the second most common non-chromosomal subgroup of congenital anomalies after congenital heart defects (3). Upper limb defects are readily visible after birth and thus serve as a warning signal of other malformations. Factors such as the type of the limb defect and whether a child has additional anomalies are likely to influence the number of hospital admissions and the length of treatment. Quantifying hospital care in different patient groups gives useful information for counseling parents and carers as well as for planning health care resources.
In this study, we have analyzed in a population-based manner hospital treatment of children with upper limb defects in Finland, which offers its residents universal health care.
Materials and Methods
Our analysis is based on records of the Finnish Register of Congenital Malformations and Finnish Hospital Discharge Register (FHDR), both maintained by the National Institute for Health and Welfare in Finland (THL). FHDR is one of the oldest individual-level hospital discharge registers covering the whole country. FHDR contains nationwide linkable data on all inpatient hospital discharges with personal identification code since 1969 (4). The validity of FHDR has been examined in 2012, and more than 95% of discharges could be identified in the register. Positive predictive value (PPV) for common diagnoses was between 75% and 99%. Completeness and accuracy in the register varies from satisfactory to very good (4).
Individuals in the Malformations Register and FHDR are coded using the Finnish personal identity code which was introduced in the 1960s (5). Diagnoses in the Register of Congenital Malformations are coded according to the 9th revision of the International Classification of Diseases (ICD-9) of the World Health Organization (WHO). Procedure information in the FHDR was registered using the classification of National League of Hospitals 1983–1996 and from 1996 onward using codes based on Nordic Classification of Surgical Procedures (NCSP) (6).
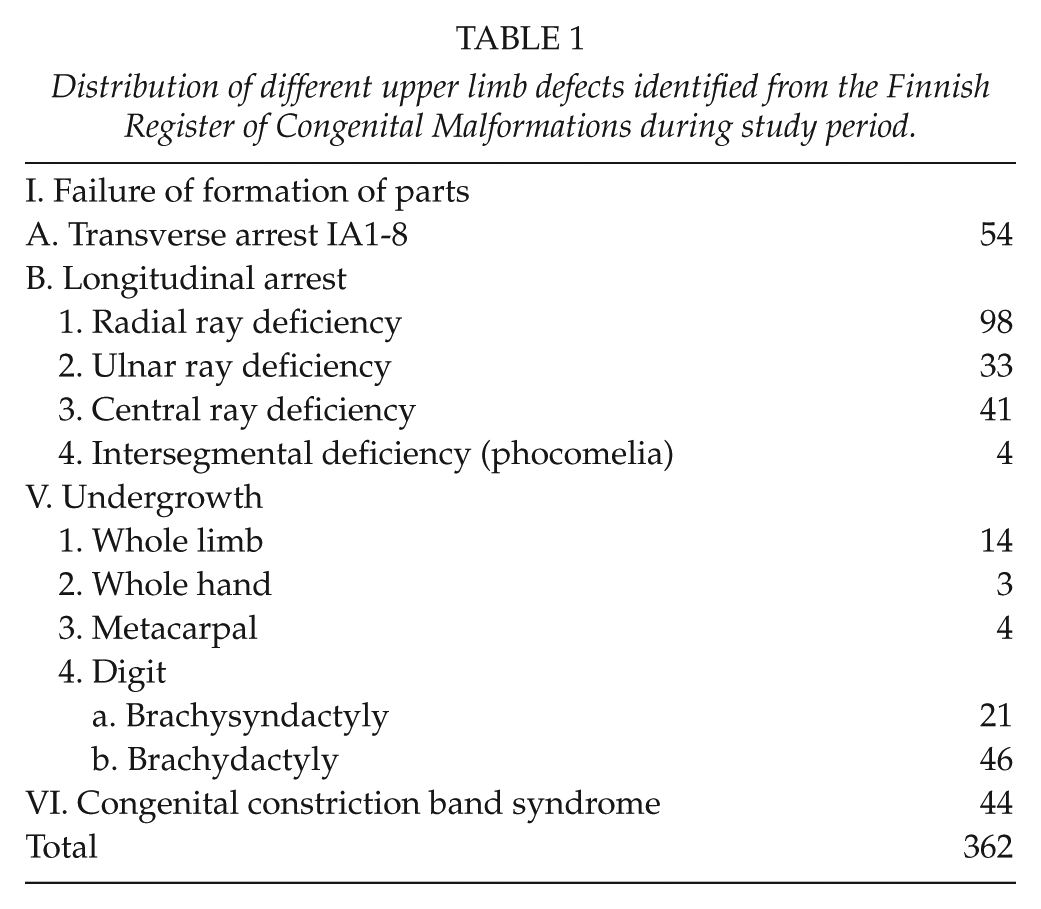
We reviewed upper limb defects among 753,342 births in Finland between 1 January 1993 and 31 December 2005. The national incidence of upper limb defects was 5.56 per 10,000 births (1). All patients coded with ICD-9 codes 75XXX, a total of 430 children from the registry, were re-evaluated by a pediatric orthopedic surgeon and an experienced medical geneticist. Fifty-two of these children had imprecise information on absent skeletal parts in the register. Additional information was therefore requested from the hospitals to supplement data. Patient records, X-ray pictures/radiologist’s opinions on X-ray pictures, family history, and clinical photographs, when available, were reviewed to allow accurate classification. On the basis of the information thus gathered, 11 patients were removed from the study because no upper limb deficiency was observed. PPV of the Register of Congenital Malformations was thus 97%. The remaining (419) children with upper limb defects were classified using the International Federation for Societies for Surgery of the Hand (IFSSH) classification modification introduced by Ezaki et al. (7) in 1993. Stillbirths (25) and children who died during their birth admission (30) were excluded from the analysis of FHDR. Two cases had major anomalies and no hospital admissions. When double-checking these two patients, they revealed to be elective terminations due to fetal indications and were excluded from the study. Three hundred and sixty-two children born alive between 1993 and 2005 with an upper limb defect were included in the FHDR analysis (Table 1).
Distribution of different upper limb defects identified from the Finnish Register of Congenital Malformations during study period.
Number of hospital admissions (excluding the birth episode), days spent in hospital, and number and type of surgical operations were picked up from FHDR from 1 January 1993 until 31 December 2009 concerning these 362 children. Average follow-up time was 10.2 years (4–17 years). Population of children (0–17 years) in Finland during the period 1994–2009 was on an average 1,126,353/year (range: 1,088,456–1,167,822). Data on hospital admissions and days spent in hospital in this census population were also obtained from FHDR from 1 January 1993 until 31 December 2009.
Statistics were calculated by mean t-test. The values of p < 0.05 were considered statistically significant.
This register-based study involved data from the Finnish Register of Congenital Malformations and FHDR. According to the Finnish legislation, informed consent was not required, as the study objects were not contacted. Permission to use the register data in this study was granted by the Ministry of Social Affairs and Health and approved by the data protection authority.
Results
Hospital Treatment
Of all 362 children with upper limb defects, 321 (87%) had hospital admissions. There were altogether 3726 hospital admissions and 19,522 days spent in hospital during the 17-year-long study period. Median of hospital admissions was 4/child. Annually, the mean number of hospital admissions was 1.01 (range: 0–36 admissions)/child and days spent in hospital 5.28 (range: 0–150 days). The length of a hospital treatment period varied from 1 to 388 days/admission (Table 2).
Number of hospital admissions and days spent in hospital during study period.
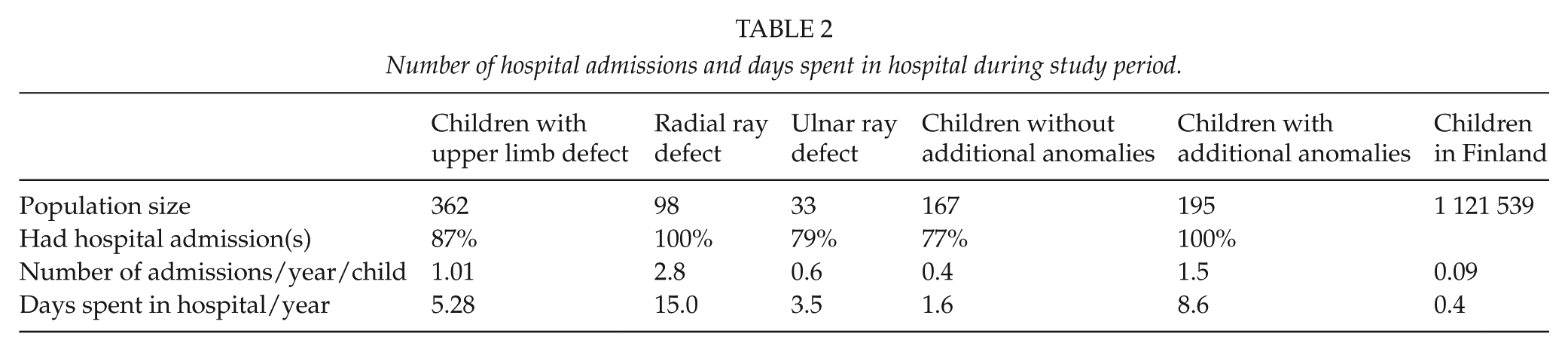
The general pediatric population had altogether 126,243 hospital admissions/year (range: 112,325–140,981), on an average 0.09 admissions/child/year. They spent in hospital 563,245 days/year (range: 501,502–594,610), on an average 0.4 days/child/year. Thus, the number of hospital admissions was 11-fold in patients with an upper limb defect as compared with general population (p < 0.001; crude rate difference: 0.92; crude rate ratio: 11.2) and the time spent in hospital 13-fold (p < 0.001; crude rate difference: 4.88; crude rate ratio: 13.2).
Surgical Treatment
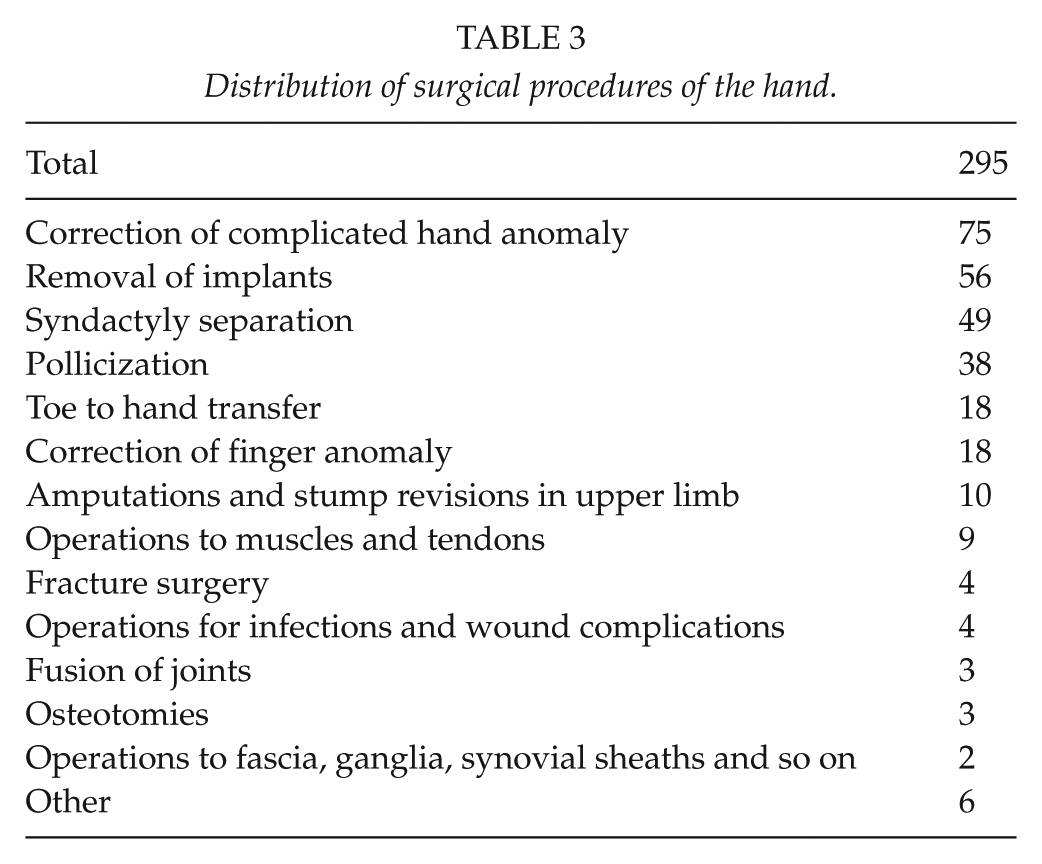
The majority of the children (72%, 262/362) had surgical hospital admissions. Altogether, 1535 surgical procedures were done, on average 4 procedures/child (range: 0–45). The most common procedures were orthopedic (512); gastrointestinal (263); ear, nose, and throat (143); dental (118); thoracic (48); and urologic (44) (Fig. 1). Of the 512 orthopedic procedures, 326 were directed to the upper limb (shoulder, upper arm, elbow, lower arm, and hand), 107 to the lower limbs, and 10 to the spine. The most common surgical operations of the hand were syndactyly separation (49), pollicization (38), and second toe to hand transfer (18) (Table 3).
Distribution of surgical procedures of the hand.
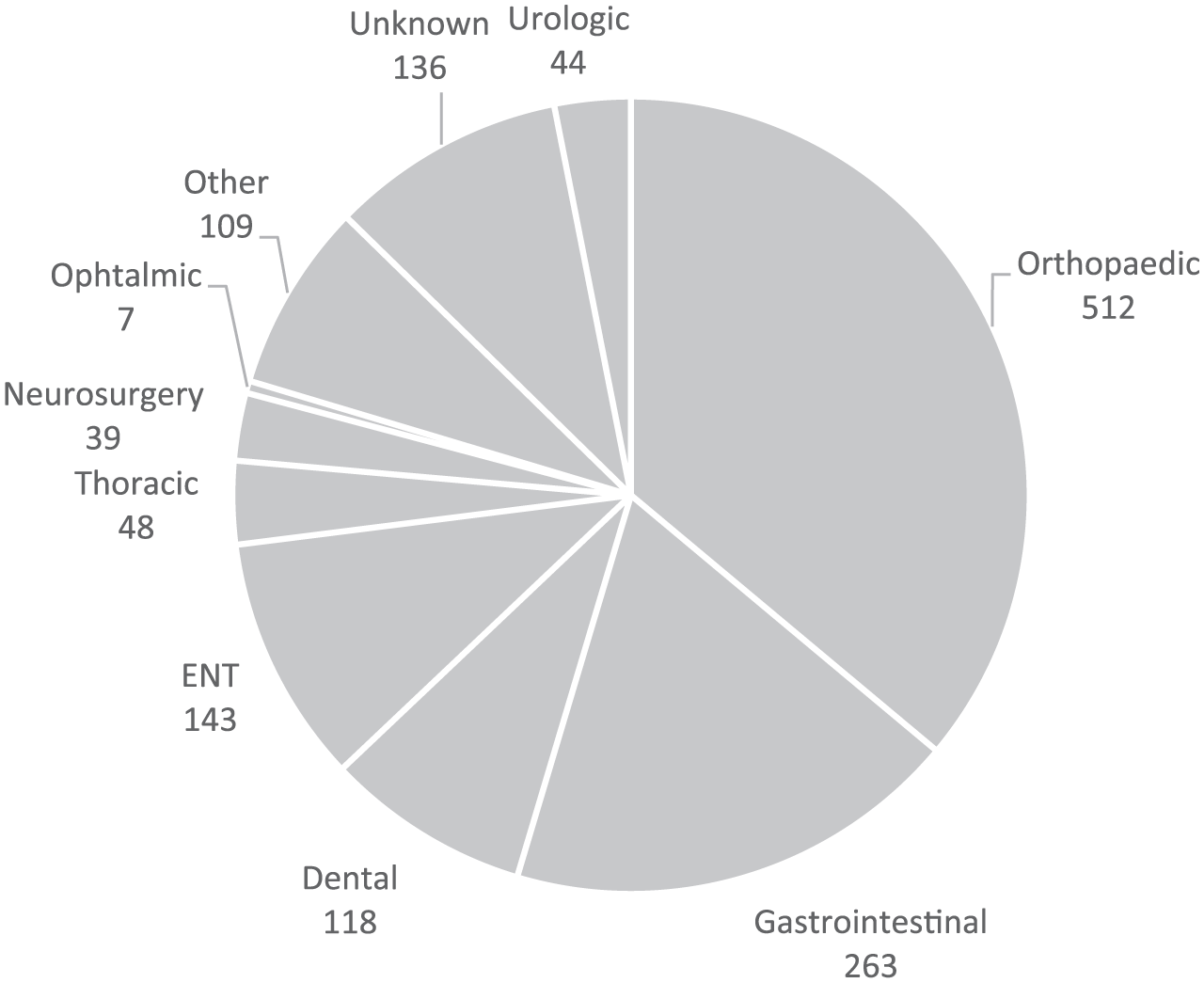
Distribution of surgical procedures within study population.
Median operation age was 2 years 7 months (range: 0–15 years 4 months), mean age 3 years 5 months. Of all procedures, 67% (1021/1535) were done before 4 years of age, 22% (338/1535) within the first year of life, and 86% (1332/1535) before school age (7 years) (Table 4).
Timing of surgery.
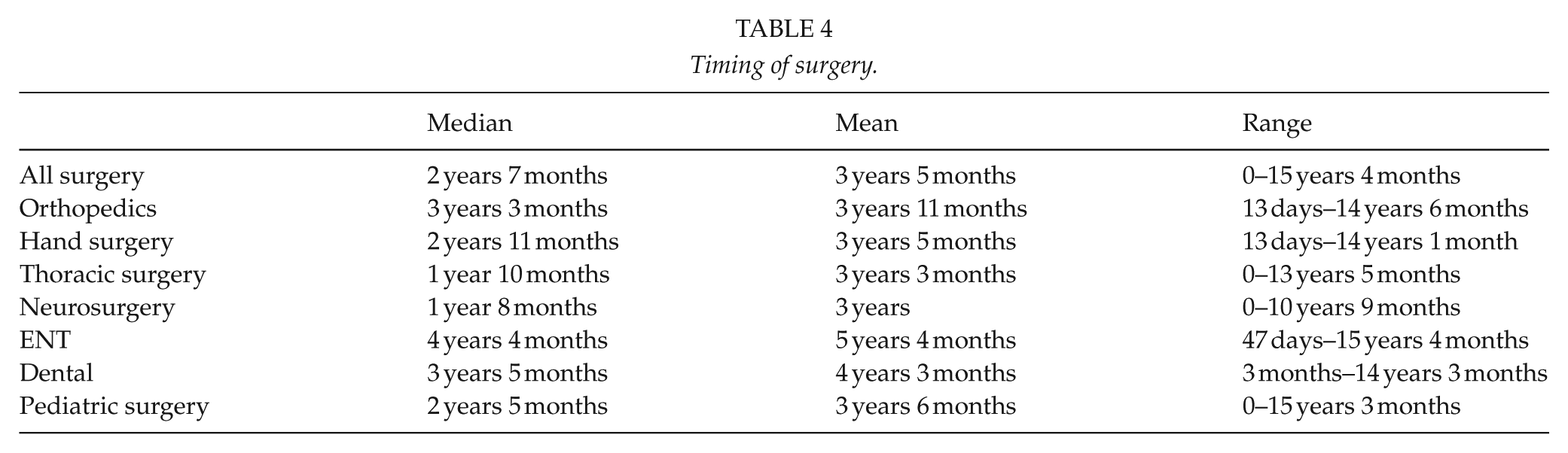
Roughly one-third of the children (36.7%, 133/262) had surgery directed to the upper limb. On average, one hand surgical procedure/child was done (range: 0–9). Almost half of these children (46.6%, 62/133) went through several hand surgical procedures. Syndactyly separation was done at mean age of 20 months (range: 1 month–9 years) with most patients (33/49) operated between 1 and 3 years of age. Pollicization was done at mean age of 44 months (range: 14 months–7 years), and most patients (23/38) were operated before the age of 4 years. Toe to hand transfer was performed at mean age of 45 months (range: 18 months–6 years) with most transfers done (12/18) before the age of 4 years.
Non-Surgical Hospital Admissions
Altogether, 60% (2191/3663) of hospital admissions were non-surgical (no surgical procedures done during the hospital stay). Based on number 1 diagnosis registered by the discharge of the patient, the leading cause to non-surgical hospital admissions was congenital anomalies (32%), followed by gastroenterological problems (20%), respiratory tract conditions (13%), neurological problems (7%), perinatal conditions such as low birth weight (5%), and infectious diseases (5%) (Fig. 2).
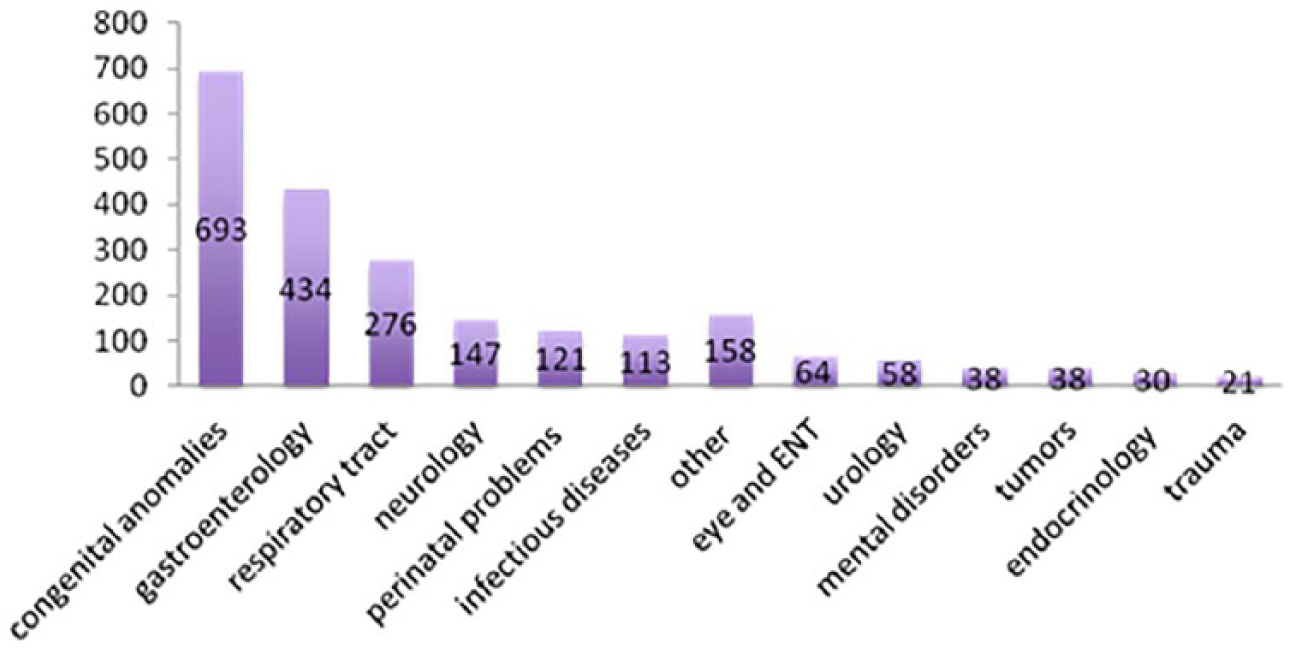
Distribution of non-operative hospital admissions based on number 1 diagnosis of the hospital stay.
Children with No Admissions
Forty-one children of the study population (41/362, 11%) had no hospital admissions. They had no other anomalies than an upper limb defect. The most common diagnoses in these children without registered hospital treatment were absent ulnar finger(s), Poland’s syndrome, terminal defects of fingers, and constriction band syndrome.
Subgroup Analysis
Most children with an isolated upper limb defect had hospital admissions. There were altogether 646 hospital admissions, on average 0.4/child/year. Children with an isolated upper limb defect spent in hospital altogether 2453 days, 1.6 days/child/year (Table 1).
All children with either some kind of a syndrome or multiple major organ anomalies (195) had hospital admissions. They had altogether 3080 hospital admissions, on an average 1.5/child/year. Children with multiple anomalies spent in hospital 8.6 days/year (Table 1).
There were 98 infants with a radial ray defect. All of them had hospital admissions, on average 2.8/child/year, which is 31-fold compared with the whole child population. Children with a radial ray defect spent in hospital on an average 15 days/year (Table 1).
Thirty-three live born infants had an ulnar ray defect. Twenty-six (79%) had hospital admissions, on an average 0.6 admissions/child/year. Children with an ulnar ray defect spent in hospital 3.5 days/year. Seven children with no admissions during the follow-up period had no other malformations than the defect in their upper extremity.
Discussion
Upper limb defects (especially radial ray defects, phocomelia, and amelia) are known to be associated with other anomalies, leading to increased morbidity and mortality (8, 9). Congenital malformations are a significant component of the global burden of disease (GBD) among children, accounting for 25 million disability-adjusted life years (DALYs) worldwide (10, 11). Congenital anomalies are the cause of death in 6.7% of deaths in the neonatal period in the world (12). In western countries, where infant mortality is low, congenital anomalies are the most common cause of death in the neonatal period (13).
In this study, we linked a population-based national registry of birth defects to population-based hospital admission data. This approach made it feasible to gain a true picture of hospital care because admission records were linked for each child with an upper limb defect. Our results showed an 11-fold number of hospital admissions and a 13-fold number of days spent in hospital for each child each year, compared with children and the youth population on the average. Previous population-based studies focusing on hospital care of children with upper limb defects have not been done. A study in England analyzed hospital admissions in the first 2 years of life among children with cleft lip and/or palate. Those who had additional anomalies had a 5-fold number of hospital admissions and an 11-fold number of days spent in hospital compared with all children (14). A study from Western Australia describes hospital care of children with the Down syndrome, finding fivefold numbers compared with the general population (15). Another study from Western Australia clarifies the amount of hospital admissions of all children with birth defects and they found threefold numbers in the age group up to 1 year compared with normal child population (16). It seems that children with upper limb defects need a considerable amount of hospital care compared not only with general population but also with children with other congenital anomalies based on data from these other studies mentioned above (14–16).
The impact of multiple anomalies on the burden of disease has been scarcely analyzed in the literature. There is one study from Kenya, where the burden of selected congenital anomalies (club foot, hypospadias, hydrocephalus, spina bifida, cleft lip, bladder exstrophy, imperforate anus) was examined in a resource-limited region (17). The GBD has been extensively studied and discussed (18). It has been recognized as a crucial input into debates, intervention organization, and health technology planning. However, data on the burden of multiple anomalies are scarce. These data are central for the same causes as is the study on the GBD, although the focus is pinpointed to a smaller scale. Our study reveals that children whose upper limb defects are not associated with perinatal lethal anomalies undergo considerably more medical examinations and interventions than children on the average. These surgical interventions are more often related to the associated anomalies rather than to upper limb problems.
The timing of syndactyly separation is usually recommended at 12 months or later (19). Some authors recommend pollicization ideally before 1 year of age and reconstructive surgery for hypoplastic thumb between 1 and 2 years (20, 21). Others recommend that hand reconstruction should be completed by approximately 4 years of age (22). The actual timing of hand surgery is influenced by other anomalies needing treatment, often more urgently. In our material, syndactyly separation was in 67% done between 1 and 3 years and in 92% before 4 years. In 14%, separation was done before 1 year. Pollicization was never done before 1 year, but in the majority (61%) of cases before 4 years and in 95% by school age (7 years). Toe to hand transfer was in the majority of cases done before 4 years and always before school start. It seems that praxis in our country meets recommendations quite well.
Diagnosis of an upper limb defect is usually quite straightforward, since the defect is often clearly visible. Precise classification needs expertise, however. This study is based on a national database including nearly all children with upper limb defects in Finland. The main disadvantage of register data is its secondary nature: the data have not been collected primarily for the purposes of a specific research question. In a hospital material from Cleveland (USA), an underlying disorder with a significant genetic component was found in 71% of children admitted to a children’s hospital (23). If we could have compared hospital care of children with upper limb defects, with a population of healthy children, we would most probably have found a greater difference. Our result of an 11-fold burden of hospital care is thus an underestimate, since our study is a comparison with a “normal population” that includes all children in Finland, as well as those with congenital anomalies and genetic disorders.
The average follow-up time in our study was 10.2 years (4–17 years). Most surgery for congenital anomalies is done ideally in the first years of life and almost all before school age. Our figures of operative treatment are an underestimate because in some children the follow-up was only 4 years.
The quality of life of these patients cannot be assessed from register data. However, identifying patients who need hospital care and surgical treatment aids in the discussion on the prognosis, thus helping to prepare the parents for the future. Similar surveys to those done for spina bifida, quantifying the economic and psychosocial effects of upper limb defects, should be performed (24).
In Finland, the burden on hospitals is at least 11-fold in children with congenital upper limb defects. With the accumulation of health care visits, health care professionals should try to deal with as many problems as possible during one hospital admission.
Conclusion
Children with upper limb defects need not only hand surgery but also teamwork of many specialists. The burden of hospital care is at least 11-fold compared with an average child.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This register-based study involved data from the Finnish Register of Congenital Malformations and FHDR. According to the Finnish legislation, informed consent was not required, as the study objects were not contacted. Permission to use the register data in this study was granted by the Ministry of Social Affairs and Health and approved by the data protection authority.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.H. received funding as Consultant: Medtronic; Funding for Institute: Medtronic; K2M via Innosurge As. E.K.-V., N.P., and Y.N. received no financial support for the research, authorship, and/or publication of this article.