
Abstract
Purpose:
Three-dimensional printing has evolved into a cost-effective and accessible tool. In orthopedic surgery, creating patient-specific anatomical models and instrumentation improves visualization and surgical accuracy. In pediatric orthopedics, three-dimensional printing reduces operating time, radiation exposure, and blood loss by enhancing surgical efficacy. This review compares outcomes of three-dimensional printing–assisted surgeries with conventional surgeries for upper and lower extremity pediatric surgeries.
Methods:
A complete search of medical literature up to August 2023, using Ovid Medline, EMBASE, Scopus, Web of Science, and Cochrane Library was conducted in compliance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Broad search terms included “pediatrics,” “orthopedic,” and “3D-printing.” Eligible studies were assessed for intraoperative time, blood loss, and fluoroscopy exposure.
Results:
Out of 3299 initially identified articles, 14 articles met inclusion criteria. These studies included 409 pediatric patients, with ages averaging 9.51 years. The majority were retrospective studies (nine), with four prospective and one experimental study. Studies primarily utilized three-dimensional printing for navigation templates and implants. Results showed significant reductions in operative time, blood loss, and radiation exposure with three-dimensional printing. Complication occurrences were generally lower in three-dimensional printing surgeries, but there was no statistical significance.
Conclusions:
Three-dimensional printing is an emerging technology in the field of orthopedics, and it is primarily used for preoperative planning. For pediatric upper and lower extremity surgeries, three-dimensional printing leads to decreased operating room time, decreased intraoperative blood loss, and reduced radiation exposure. Other uses for three-dimensional printing include education, patient communication, the creation of patient-specific instrumentation and implants.
Level of evidence:
Level III
Introduction
Three-dimensional (3D) printing originated in the 1980s, when one of the first rapid prototyping machines was created. 1 With technological advancements, 3D printing has become more cost-effective, user-friendly, and increasingly accessible. 1 This has opened the door for various fields, including medicine, to embrace and integrate this versatile tool into their practices.1,2 The application of 3D printing in medicine can be traced back to the early 2000s, and started to make significant strides in the realm of orthopedic surgery in the mid-2010s. Orthopedic surgeons started utilizing 3D printing to create higher fidelity replicas of bones and joints from patient imaging data, allowing a better understanding of complex anatomies and facilitating more precise surgical interventions. 3
The 3D-printing patient-specific anatomical models present many advantages. They allow the surgeon to better visualize and understand the complexities of the patient’s anatomy before entering the operating room. They are also useful in educational settings, where they can be used to better inform the patient of their procedure, or even for surgical education of medical students and residents. 4 Another use for 3D printing is to make patient-specific instrumentation (PSI), including customized navigation templates and surgical guides. 3 By using PSI, the surgeon can more accurately make incisions and place implants, which leads to a more efficient operation. 5 To further increase surgical efficiency, 3D printing can also be used to create patient-specific implants, uniquely tailored to each patient’s anatomy, as well as specific instrumentation. 6
In pediatric orthopedics, the use of 3D printing is particularly invaluable due to the distinct challenges posed by the child’s compact anatomy and their specific developmental needs. Allowing the surgeon to analyze patient deformities on a 3D-printed model preoperatively provides a major advantage by reducing necessary operating time, reducing radiation exposure, and reducing intraoperative blood loss.7 –10 It also serves as a valuable educational resource for both the patients and their parents, which fosters increased confidence and reassurance for everyone involved. 11
This literature suggests that 3D printing is a useful strategy for increasing surgical efficacy, however, previous reviews largely grouped adult and pediatric populations together,8,9,10,12 or focused on spinal orthopedic surgeries. 13 This review aims to compare specific outcomes (operative time, radiation exposure, and intraoperative blood loss) in pediatric orthopedic upper and lower limb surgeries. Operations that used 3D printing for preoperative planning were compared with conventional surgeries. Comparing these quantitative outcomes allows us to identify if there’s a difference in surgical efficacy when using 3D printing in pediatric orthopedics, which can lead to better postoperative outcomes and other potential benefits for this patient population.
Methodology
Search strategy
A complete search for medical literature was executed through August 2023 using Ovid Medline, EMBASE, Scopus, Web of Science, and Cochrane Library in compliance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Given that the concept of 3D printing is still emerging in the field of orthopedic surgery, the search strategy was kept intentionally broad. Search terms included the following Medical Subject Headings and keywords: “infant,” “child,” “adolescent,” “pediatrics,” “orthopaedic,” “musculoskeletal,” “bones,” “fracture,” “sports medicine,” “joints,” “osteotomy,” “3D-printing,” “additive manufacturing,” “rapid prototyping,” and “stereolithography.” Boolean operators (OR, AND) as well as asterisks for truncation were used to optimize the search results (see Appendix 1).
Search results from all databases were uploaded to Covidence, and duplicates were automatically removed. Articles were initially screened independently by two reviewers based on title and abstracts. The remaining articles were screened based on the full text. Disagreements were discussed between the two reviewers to reach a consensus, and conflicts were resolved by the senior author, a pediatric orthopedic surgeon.
Eligibility criteria
This systematic review focuses on the operative efficiency of upper and lower limb orthopedic pediatric surgery when 3D printing is used. Inclusion criteria required that studies (1) used 3D printing as the primary intervention; (2) were upper or lower limb orthopedic procedures; (3) reported intraoperative time, blood loss, or fluoroscopy exposure; (4) provided results for pediatric patients (defined as < 18 years old). All available publication years were included.
Studies were excluded if: (1) 3D printing was not used; (2) the intervention was not an upper or lower limb orthopedic procedure (e.g. spine, skull, teeth, heart, etc.); (3) the outcomes of the study did not include intraoperative time, blood loss, or fluoroscopy exposure; (4) the study was not in English or French; (5) the study was a review, editorial, technique article, methods article, conference proceeding or incomplete (e.g. only abstracts available); (6) the study used animals; (7) the study used cadavers; (8) or the study used bioprinting.
Data extraction
Included studies were compiled in a database and the following information was extracted: study title, author list, year of publication, sample size, mean age, sex, underlying condition, the type of surgical procedure, the type of 3D-printed implant used, primary objective, total operative time, blood loss volume, fluoroscopy time, reported complications, other outcomes of interest, and final conclusions by authors. Studies were further categorized by their level of evidence (LOE), with prospective studies having an LOE II, retrospective studies with an LOE III, and experimental studies/case series having an LOE IV. For prospective and retrospective studies, data for both control and experimental groups were compared and summarized. Data regarding costs of production and manufacturing relating to 3D-printing implants for surgical use was disregarded from comparisons, and descriptive statistics of patient outcomes were used to assess the efficacy of 3D printing in comparison to conventional pediatric orthopedic surgery.
Statistical analysis
Figures 1–3 present paired data from conventional and 3D-printing groups of each study. Mean values from the 3D-printing group were pooled and compared to pooled mean values from the conventional group. GraphPad Prism version 8 was used to prepare graphical representations of patient outcome data.
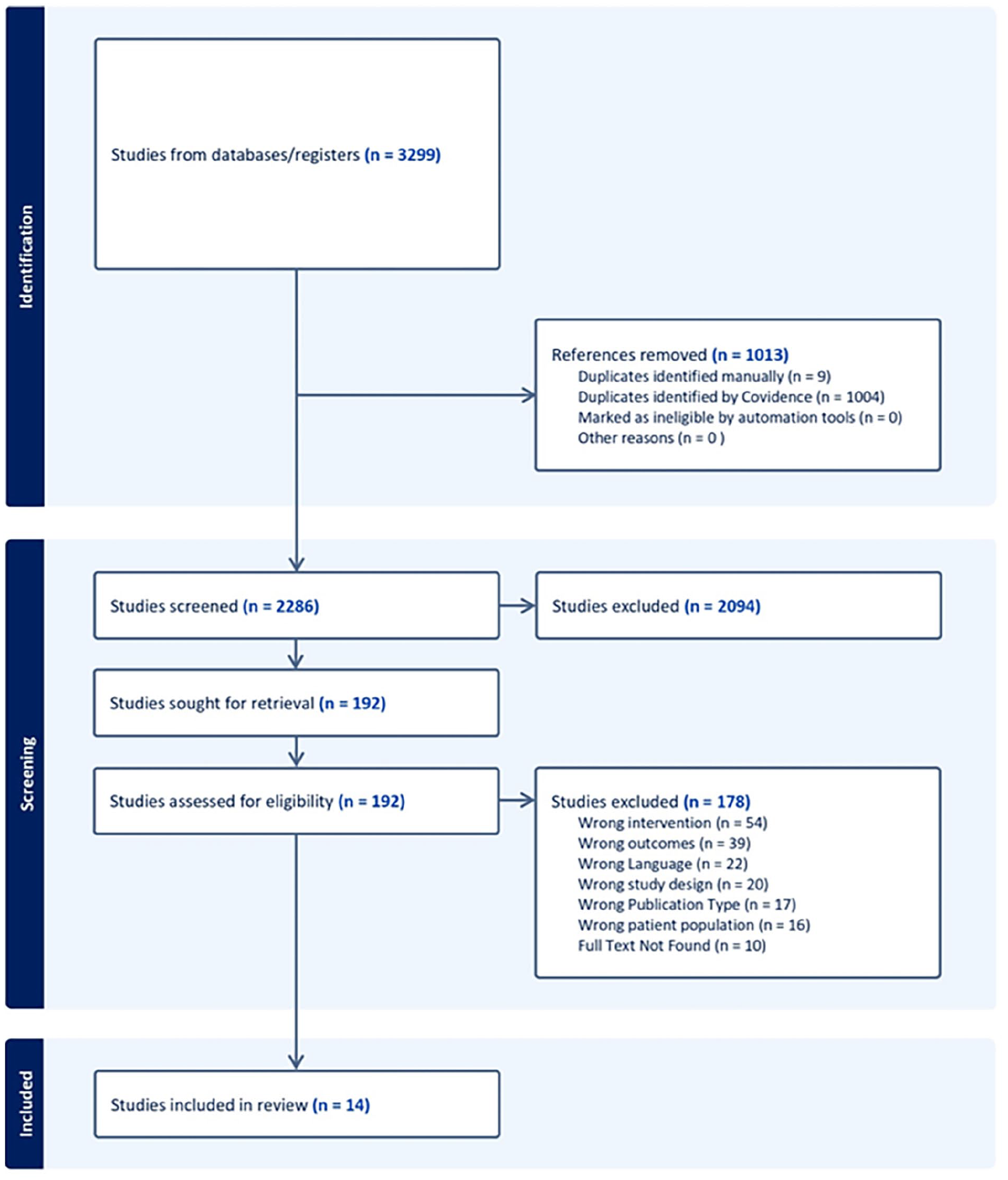
PRISMA flow chart.
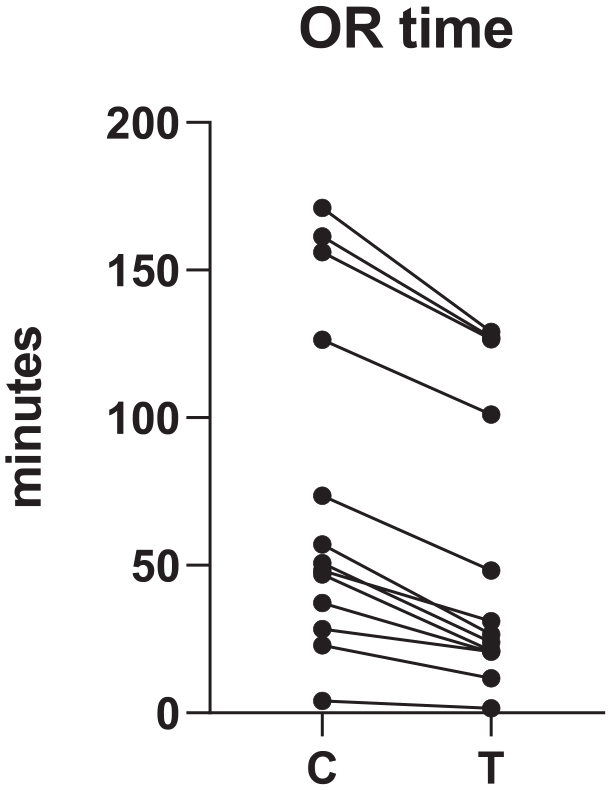
The use of 3D printed navigation templates shows a general trend of reduced operating room time in comparison to control surgeries.
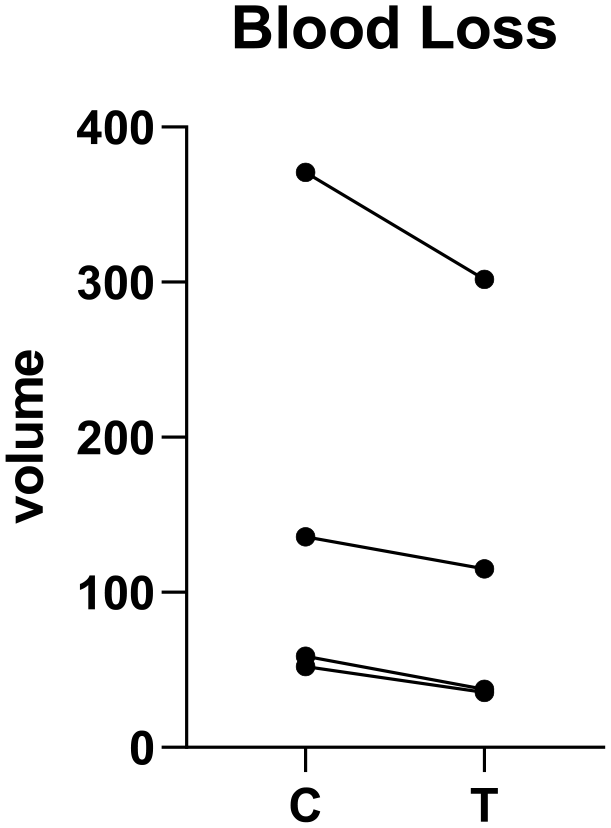
Effect of 3D-printed navigation templates on blood loss.
Results
Of the 3299 articles identified via our combined search strategy, 1013 duplicates were automatically removed in Covidence prior to screening. Titles and abstracts of the remaining 2236 articles were screened using the above-mentioned inclusion and exclusion criteria. During title and abstract screening, 2094 articles were excluded, yielding 192 articles progressing to full text retrieval. Of the 192 articles, 178 articles were further excluded following full text review, yielding 14 articles that fully satisfy our preset inclusion and exclusion criteria. Of the 169 articles excluded, the most frequent reasons for exclusion were: wrong intervention (n = 54), wrong patient outcomes (n = 39), and language of publication (n = 22). Other reasons included wrong study design, unretrievable full texts, and patient populations above the age of 21. Figure 4 presents the PRISMA diagram detailing the flow of study selection.
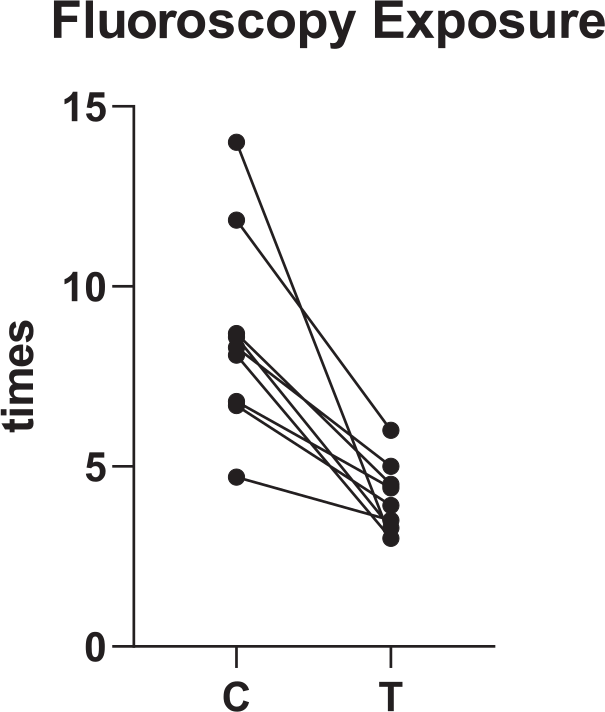
The 3D-printed navigation templates reduced fluoroscopy exposure.
Included articles were published between 2017 and 2023, of which four were prospective studies, nine were retrospective studies, and one experimental study. One article included three patients above the age of 18. 14 The rest consisted exclusively of pediatric data. The sample size totaled to n = 409 patients, with 170 males and 239 females, and an average age of 9.51 years.
Effect of the use of 3D printing on operating room time
Prospective studies included the surgical management of cubitus varus deformity,
15
leg length discrepancy,
16
developmental dysplasia of the hip (DDH),
17
and slipped capital femoral epiphysis
18
in pediatric populations. While all these studies used 3D printed navigation templates, medical-grade poly-
Study characteristics and operating room time.
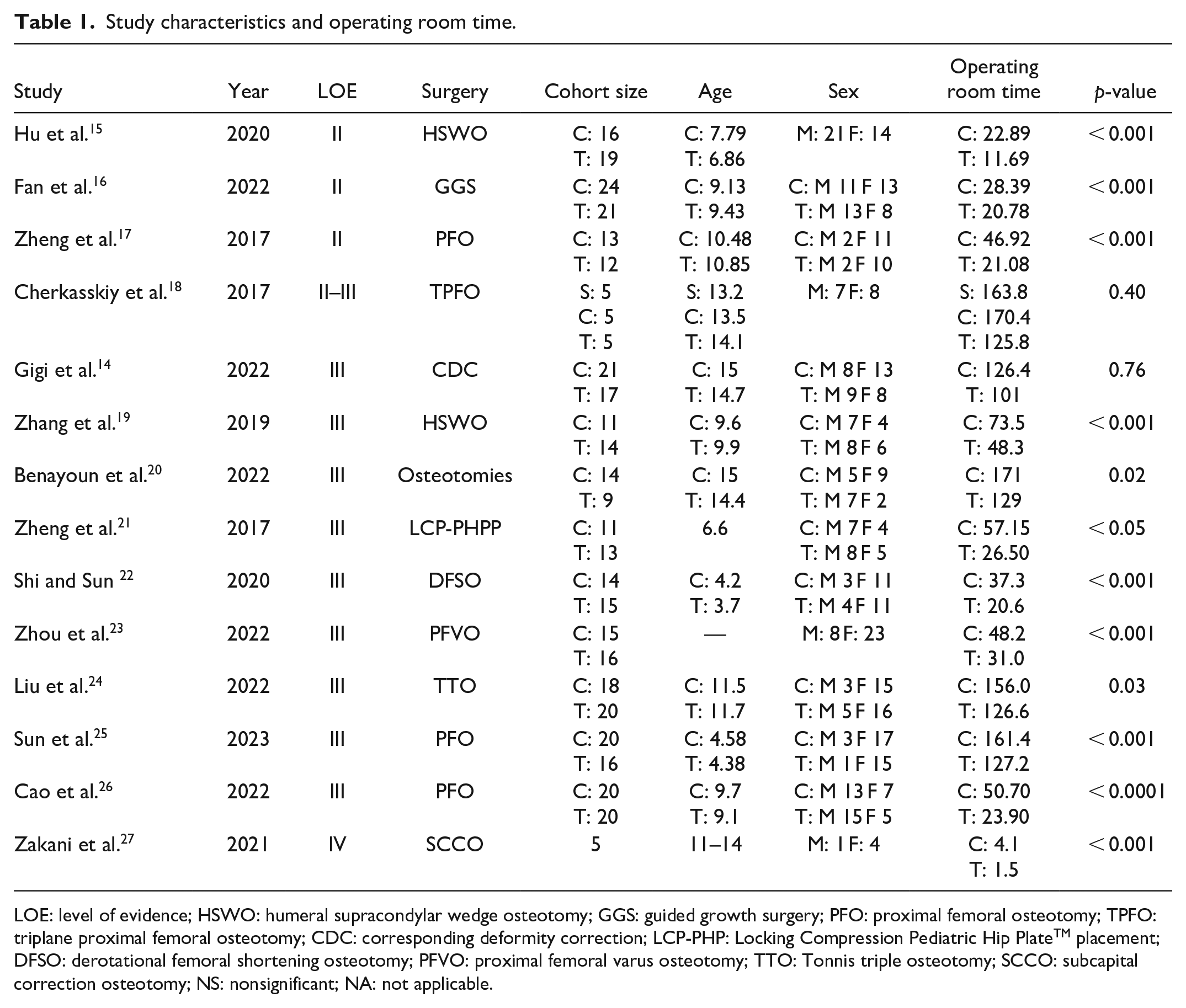
LOE: level of evidence; HSWO: humeral supracondylar wedge osteotomy; GGS: guided growth surgery; PFO: proximal femoral osteotomy; TPFO: triplane proximal femoral osteotomy; CDC: corresponding deformity correction; LCP-PHP: Locking Compression Pediatric Hip PlateTM placement; DFSO: derotational femoral shortening osteotomy; PFVO: proximal femoral varus osteotomy; TTO: Tonnis triple osteotomy; SCCO: subcapital correction osteotomy; NS: nonsignificant; NA: not applicable.
Effect of the use of 3D printing on intraoperative blood loss
Of the four prospective studies, three studies did not collect data on intraoperative blood loss, except the study assessing the use of 3D printing in TPFO for slipped capital femoral epiphysis, which did not denote any statistical significance (Senior group vs C vs T, 981.5 ± 534.4 vs 962.6 ± 276.1 vs 979.8 ± 316.2 mL, p = 0.3; see Table 2). 18 Five out of ten retrospective studies recorded intraoperative blood loss,14,19,24 –26 and four of the five stated they found a statistically significant decrease in blood loss during 3D printing surgeries compared to control surgeries.19,24 –26
Study characteristics and blood loss.
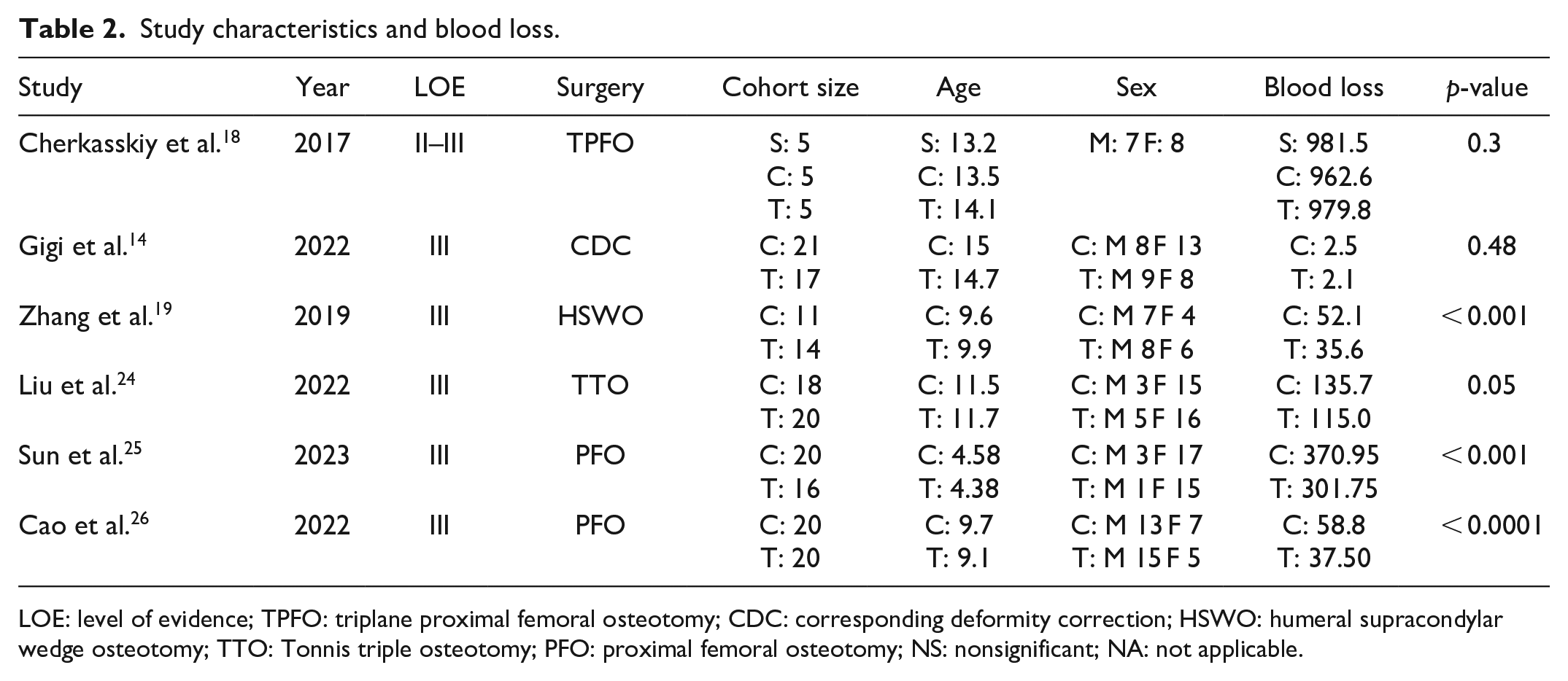
LOE: level of evidence; TPFO: triplane proximal femoral osteotomy; CDC: corresponding deformity correction; HSWO: humeral supracondylar wedge osteotomy; TTO: Tonnis triple osteotomy; PFO: proximal femoral osteotomy; NS: nonsignificant; NA: not applicable.
Effect of the use of 3D printing on fluoroscopy exposure
Three prospective studies recorded the frequency of fluoroscopy exposure, and two studies stated they found a statistically significant decrease in radiation exposure during surgeries that used 3D printing,16,17 while one study did not find any statistically significant difference in fluoroscopy time. 18 Seven out of ten retrospective studies recorded the frequency of fluoroscopy exposure, and all noted a statistically significant decrease in X-ray exposure in the 3D printing groups compared to control cohorts (see Table 3).20 –26 One experimental study also mentioned a statistically significant difference in X-ray exposure during simulated surgeries with 3D printed drill guides compared to control simulations. 27
Study characteristics and X-ray exposure.
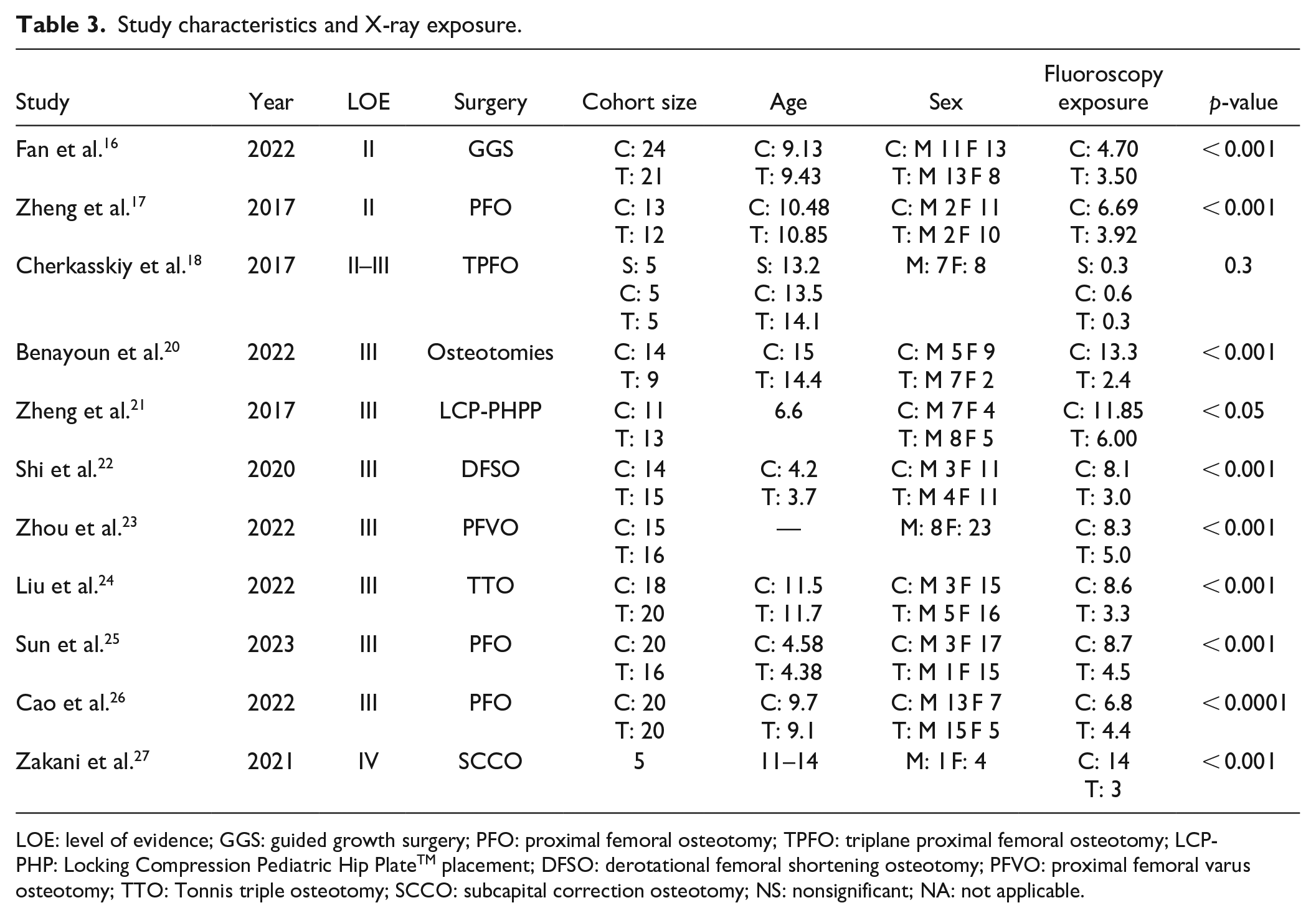
LOE: level of evidence; GGS: guided growth surgery; PFO: proximal femoral osteotomy; TPFO: triplane proximal femoral osteotomy; LCP-PHP: Locking Compression Pediatric Hip PlateTM placement; DFSO: derotational femoral shortening osteotomy; PFVO: proximal femoral varus osteotomy; TTO: Tonnis triple osteotomy; SCCO: subcapital correction osteotomy; NS: nonsignificant; NA: not applicable.
Effect of the use of 3D printing on complication occurrence
Three out of four prospective studies recorded the occurrence of complications,16 –18 and two of the three studies stated they found a statistically significant decrease in complication occurrence in the 3D-printing group (see Table 4).16,17 Seven out of ten retrospective studies compared complication frequency between 3D printing and control surgeries,14,19 –21,23,24,26 and one out of seven studies noted a significant decrease in postoperative complication. 21
Study characteristics and complication occurrences.
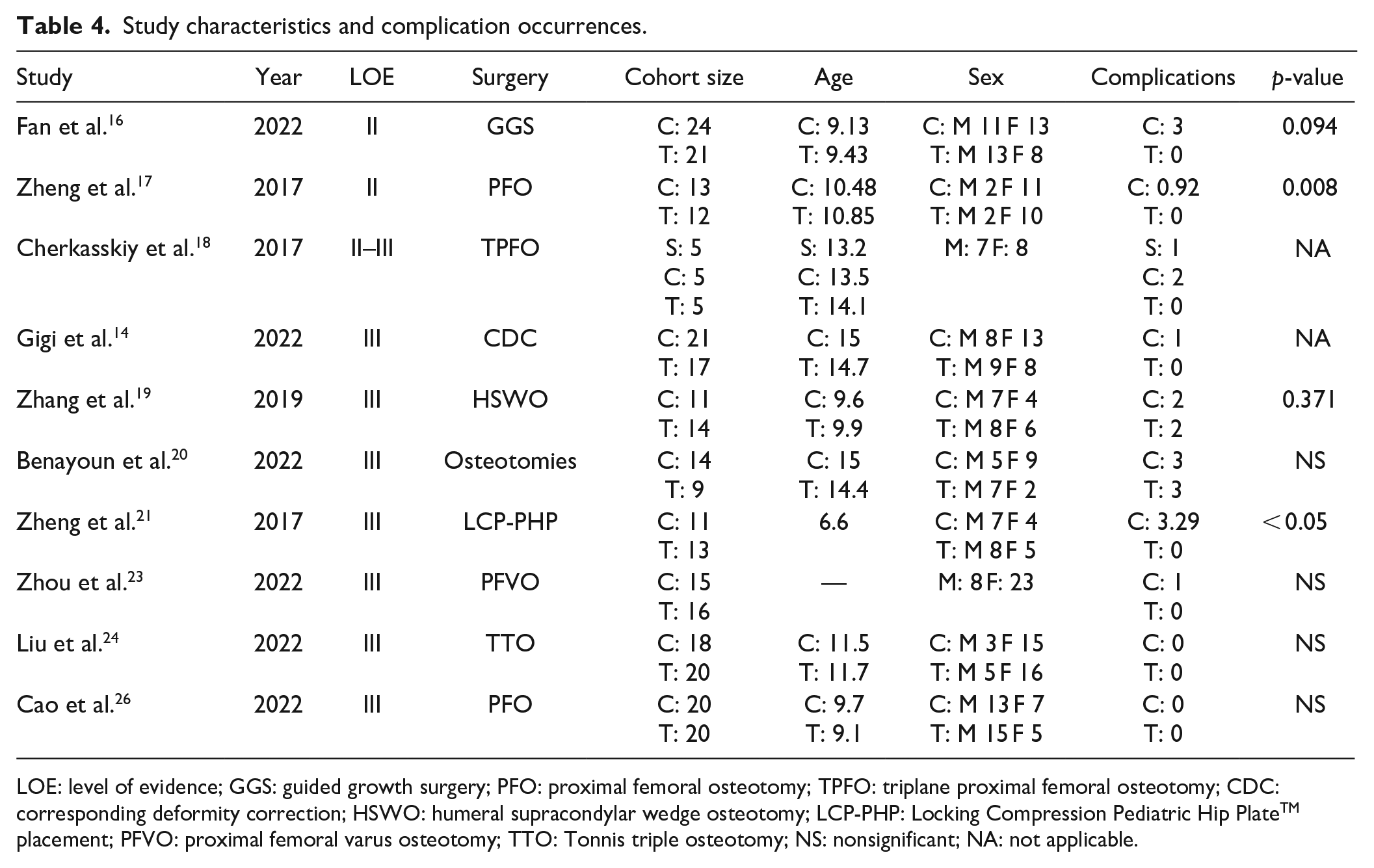
LOE: level of evidence; GGS: guided growth surgery; PFO: proximal femoral osteotomy; TPFO: triplane proximal femoral osteotomy; CDC: corresponding deformity correction; HSWO: humeral supracondylar wedge osteotomy; LCP-PHP: Locking Compression Pediatric Hip PlateTM placement; PFVO: proximal femoral varus osteotomy; TTO: Tonnis triple osteotomy; NS: nonsignificant; NA: not applicable.
Discussion
This systematic review highlights the potential of 3D-printing technology to enter standard practice in the preoperative planning of pediatric orthopedic surgery. Preoperative planning using 3D-printed models provides surgeons with a more precise understanding of patient-specific anatomical structures, which in turn allows them to streamline their surgical approach, reducing operating room time, intraoperative blood loss, and radiation exposure for pediatric patients, thus resulting in a more efficient surgery. Despite certain articles reporting fewer complications and improved clinical outcomes with 3D printing compared to conventional surgeries, a significant proportion of studies reported no notable distinctions. Reported complications include growth plate cartilage or articular cartilage injury, epiphyseal injury, wound infections, and nerve injury.14,16,17,19 It is, therefore, difficult to evaluate the clinical significance of 3D printing since there is insufficient evidence regarding the improvement in patient outcomes. Nevertheless, a decrease in operating room time holds evident advantages, such as from a cost-effectiveness standpoint. 28 Prolonged operating times and increased intraoperative blood loss correlate with elevated risks of complications, both of which could be mitigated by the implementation of 3D printing into standard practice.29,30 In addition, decreasing intraoperative blood loss often enables earlier and safer patient recovery. 30 Moreover, a systematic review and meta-analysis showed that the likelihood of complications increases significantly with prolonged operative duration, approximately doubling with operative time thresholds exceeding two or more hours. 31 While complication rates vary among surgical disciplines, prolonged operative durations generally align with increased complication risks across most specialties. Recognizing the significant impact of surgical complications on patient well-being and healthcare expenses, stakeholders including surgeons, healthcare facilities, and policymakers should prioritize strategies aimed at streamlining operative processes and enhancing workflow efficiency. Nevertheless, this focus on time reduction must be balanced with other critical factors such as patient safety and the identification of additional risk elements for complications. As such, adapting the use of 3D printing could not only improve the overall surgical state of the patient, but could also improve surgical outcomes. Further research is encouraged to explore interventions aimed at reducing operative durations while considering patient outcomes post-surgery.
Finally, pediatric patients are more sensitive to radiation than adults due to their rapidly growing cells, so it is beneficial to minimize radiation exposure when possible. Less fluoroscopy scans also benefit the health of the surgical staff, due to less direct and scatter radiation. 32 In addition, there are significant risks associated with anesthesia on the developing brain. 33 This literature on the use of 3D printing in orthopedic surgery often groups adult and pediatric populations together, however, pediatric patients in particular can benefit from 3D printing due to their unique case-by-case anatomy.
Another emerging use for 3D printing is the creation of personalized implants and prosthetics. 34 Customized prosthetic devices are especially beneficial to pediatric patients because of their rapidly growing bodies. Furthermore, 3D-printed models are useful for clinical training. The brevity of pediatric medicine exposure during medical school results in pediatric subspecialists progressing with insufficient knowledge and experience. This warrants the use of 3D-printed models for more efficient training, as they have been shown to improve medical education and procedural performance in pediatric training.35,36 The synergistic benefits of 3D printing and pediatric orthopedic surgery merit further exploration.
Although this review highlights the outcomes of 3D printing when used for preoperative planning in upper and lower limb pediatric orthopedic surgeries, it has several other medical applications as well. 37 In orthopedic surgery, 3D printing is mostly used for preoperative planning, but it is also often used for creating final implants and PSI. Between 2012 and 2018, trauma and oncology were the orthopedic subspecialities that used 3D printing the most. 12 Across all age groups and subspecialities, 3D printing significantly reduced operative time, intraoperative blood loss, and the number of fluoroscopy shots, which represents important patient benefits. 12 For the surgical treatment of pediatric spinal pathologies, preoperative planning using 3D printing applications show improved screw placement accuracy, but does not identify significant differences in operative time or blood loss. 13 In pediatric orthopedic surgeries involving the upper and lower limbs, notable reductions were observed in operating time, intraoperative blood loss, and radiation exposure. However, the impact on surgical accuracy and patient outcomes remains inconclusive, with varying perspectives in the existing literature.
Since 3D printing is still an emerging technology, the research consists majorly of retrospective and prospective studies, which presents different sources of potential bias. Randomized control trials are necessary to further authenticate the effectiveness of 3D printing in preoperative planning. Moreover, many of the existing studies group adult populations and pediatric patients into a single cohort. Given the major differences in adult and pediatric surgery, more studies exclusively examining the outcomes of pediatric procedures would be beneficial.
The future of 3D printing in orthopedic surgery holds great promise. Advancements in this technology are likely to further refine the customization of implants, enabling orthopedic surgeons to create patient-specific devices with precision and high fidelity. It will continue to allow orthopedic surgeons to optimize their surgical approach before entering the operating room, which is favorable for the patients and can reduce complications. Significant advancements are anticipated in the role of 3D printing within medical education as well. The potential for point-of-care manufacturing of personalized medical devices and anatomical models may foster a paradigm shift, promoting more accessible and cost-effective healthcare solutions. As research and development in 3D printing technologies advance, the future holds exciting possibilities for transforming the way we approach and deliver healthcare across diverse medical disciplines.
Conclusion
Three-dimensional printing is an emerging technology in the field of orthopedics. Among its various applications, it is primarily used for preoperative planning. For pediatric upper and lower extremity surgeries, 3D printing leads to decreased operating room time, decreased intraoperative blood loss, and reduced radiation exposure. Other uses for 3D printing include education, patient communication, the creation of PSI, and patient-specific implants. Additional higher-level studies are required for this patient population and intervention.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241264183 – Supplemental material for Three-dimensional-printing-guided preoperative planning of upper and lower extremity pediatric orthopedic surgeries: A systematic review of surgical outcomes
Supplemental material, sj-pdf-1-cho-10.1177_18632521241264183 for Three-dimensional-printing-guided preoperative planning of upper and lower extremity pediatric orthopedic surgeries: A systematic review of surgical outcomes by Peter Joseph Mounsef, Rachad Aita, Khaled Skaik, Sofia Addab and Reggie Charles Hamdy in Journal of Children’s Orthopaedics
Footnotes
Appendix
Search strategy.
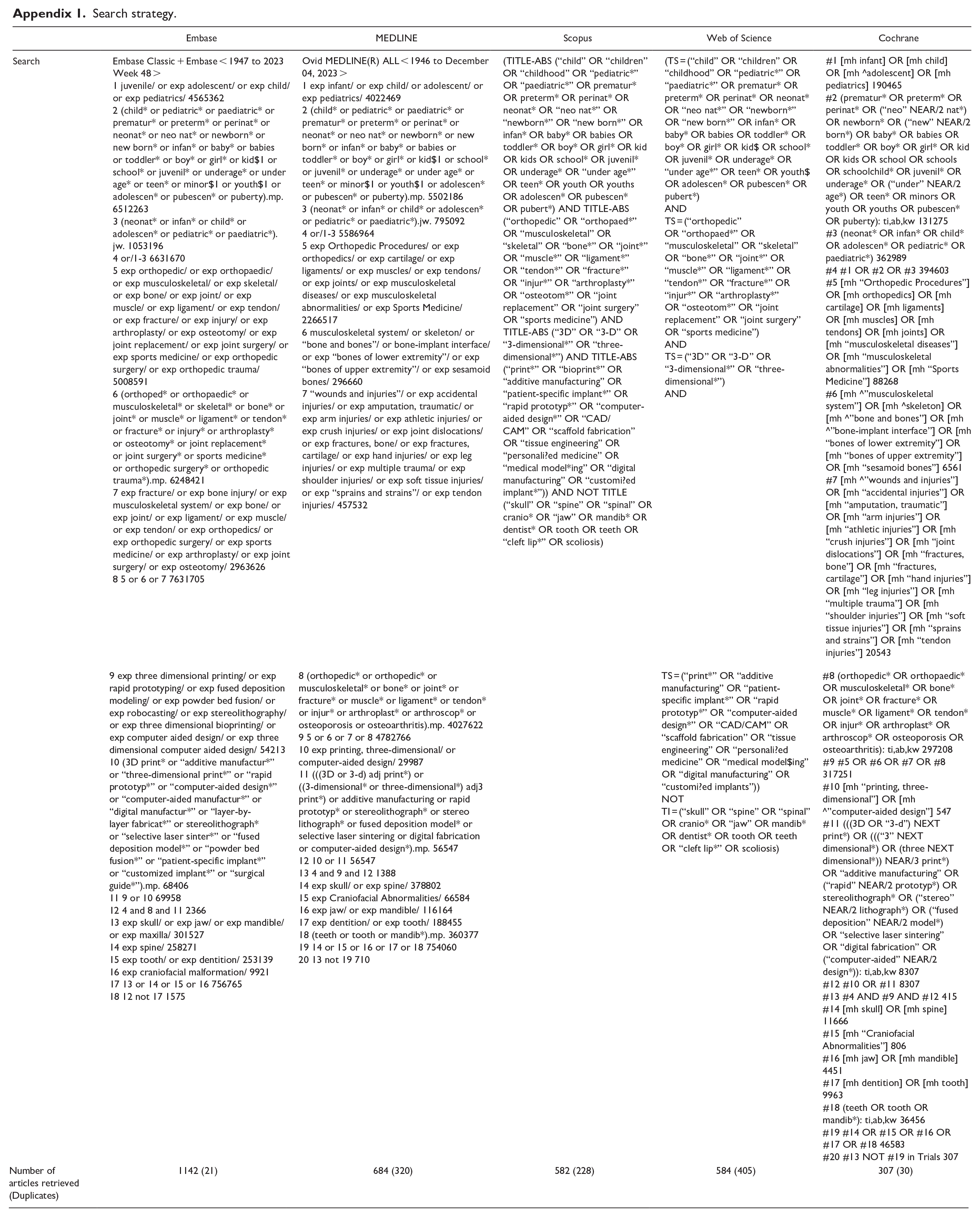
| Embase | MEDLINE | Scopus | Web of Science | Cochrane | |
|---|---|---|---|---|---|
| Search | Embase Classic + Embase < 1947 to 2023 Week 48 > 1 juvenile/ or exp adolescent/ or exp child/ or exp pediatrics/ 4565362 2 (child* or pediatric* or paediatric* or prematur* or preterm* or perinat* or neonat* or neo nat* or newborn* or new born* or infan* or baby* or babies or toddler* or boy* or girl* or kid$1 or school* or juvenil* or underage* or under age* or teen* or minor$1 or youth$1 or adolescen* or pubescen* or puberty).mp. 6512263 3 (neonat* or infan* or child* or adolescen* or pediatric* or paediatric*).jw. 1053196 4 or/1-3 6631670 5 exp orthopedic/ or exp orthopaedic/ or exp musculoskeletal/ or exp skeletal/ or exp bone/ or exp joint/ or exp muscle/ or exp ligament/ or exp tendon/ or exp fracture/ or exp injury/ or exp arthroplasty/ or exp osteotomy/ or exp joint replacement/ or exp joint surgery/ or exp sports medicine/ or exp orthopedic surgery/ or exp orthopedic trauma/ 5008591 6 (orthoped* or orthopaedic* or musculoskeletal* or skeletal* or bone* or joint* or muscle* or ligament* or tendon* or fracture* or injury* or arthroplasty* or osteotomy* or joint replacement* or joint surgery* or sports medicine* or orthopedic surgery* or orthopedic trauma*).mp. 6248421 7 exp fracture/ or exp bone injury/ or exp musculoskeletal system/ or exp bone/ or exp joint/ or exp ligament/ or exp muscle/ or exp tendon/ or exp orthopedics/ or exp orthopedic surgery/ or exp sports medicine/ or exp arthroplasty/ or exp joint surgery/ or exp osteotomy/ 2963626 8 5 or 6 or 7 7631705 |
Ovid MEDLINE(R) ALL < 1946 to December 04, 2023 > 1 exp infant/ or exp child/ or adolescent/ or exp pediatrics/ 4022469 2 (child* or pediatric* or paediatric* or prematur* or preterm* or perinat* or neonat* or neo nat* or newborn* or new born* or infan* or baby* or babies or toddler* or boy* or girl* or kid$1 or school* or juvenil* or underage* or under age* or teen* or minor$1 or youth$1 or adolescen* or pubescen* or puberty).mp. 5502186 3 (neonat* or infan* or child* or adolescen* or pediatric* or paediatric*).jw. 795092 4 or/1-3 5586964 5 exp Orthopedic Procedures/ or exp orthopedics/ or exp cartilage/ or exp ligaments/ or exp muscles/ or exp tendons/ or exp joints/ or exp musculoskeletal diseases/ or exp musculoskeletal abnormalities/ or exp Sports Medicine/ 2266517 6 musculoskeletal system/ or skeleton/ or “bone and bones”/ or bone-implant interface/ or exp “bones of lower extremity”/ or exp “bones of upper extremity”/ or exp sesamoid bones/ 296660 7 “wounds and injuries”/ or exp accidental injuries/ or exp amputation, traumatic/ or exp arm injuries/ or exp athletic injuries/ or exp crush injuries/ or exp joint dislocations/ or exp fractures, bone/ or exp fractures, cartilage/ or exp hand injuries/ or exp leg injuries/ or exp multiple trauma/ or exp shoulder injuries/ or exp soft tissue injuries/ or exp “sprains and strains”/ or exp tendon injuries/ 457532 |
(TITLE-ABS (“child” OR “children” OR “childhood” OR “pediatric*” OR “paediatric*” OR prematur* OR preterm* OR perinat* OR neonat* OR “neo nat*” OR “newborn*” OR “new born*” OR infan* OR baby* OR babies OR toddler* OR boy* OR girl* OR kid OR kids OR school* OR juvenil* OR underage* OR “under age*” OR teen* OR youth OR youths OR adolescen* OR pubescen* OR pubert*) AND TITLE-ABS (“orthopedic” OR “orthopaed*” OR “musculoskeletal” OR “skeletal” OR “bone*” OR “joint*” OR “muscle*” OR “ligament*” OR “tendon*” OR “fracture*” OR “injur*” OR “arthroplasty*” OR “osteotom*” OR “joint replacement” OR “joint surgery” OR “sports medicine”) AND TITLE-ABS (“3D” OR “3-D” OR “3-dimensional*” OR “three-dimensional*”) AND TITLE-ABS (“print*” OR “bioprint*” OR “additive manufacturing” OR “patient-specific implant*” OR “rapid prototyp*” OR “computer-aided design*” OR “CAD/CAM” OR “scaffold fabrication” OR “tissue engineering” OR “personali?ed medicine” OR “medical model*ing” OR “digital manufacturing” OR “customi?ed implant*”)) AND NOT TITLE (“skull” OR “spine” OR “spinal” OR cranio* OR “jaw” OR mandib* OR dentist* OR tooth OR teeth OR “cleft lip*” OR scoliosis) | (TS = (“child” OR “children” OR “childhood” OR “pediatric*” OR “paediatric*” OR prematur* OR preterm* OR perinat* OR neonat* OR “neo nat*” OR “newborn*” OR “new born*” OR infan* OR baby* OR babies OR toddler* OR boy* OR girl* OR kid$ OR school* OR juvenil* OR underage* OR “under age*” OR teen* OR youth$ OR adolescen* OR pubescen* OR pubert*) AND TS = (“orthopedic” OR “orthopaed*” OR “musculoskeletal” OR “skeletal” OR “bone*” OR “joint*” OR “muscle*” OR “ligament*” OR “tendon*” OR “fracture*” OR “injur*” OR “arthroplasty*” OR “osteotom*” OR “joint replacement” OR “joint surgery” OR “sports medicine”) AND TS = (“3D” OR “3-D” OR “3-dimensional*” OR “three-dimensional*”) AND |
#1 [mh infant] OR [mh child] OR [mh ^adolescent] OR [mh pediatrics] 190465 #2 (prematur* OR preterm* OR perinat* OR (“neo” NEAR/2 nat*) OR newborn* OR (“new” NEAR/2 born*) OR baby* OR babies OR toddler* OR boy* OR girl* OR kid OR kids OR school OR schools OR schoolchild* OR juvenil* OR underage* OR (“under” NEAR/2 age*) OR teen* OR minors OR youth OR youths OR pubescen* OR puberty): ti,ab,kw 131275 #3 (neonat* OR infan* OR child* OR adolescen* OR pediatric* OR paediatric*) 362989 #4 #1 OR #2 OR #3 394603 #5 [mh “Orthopedic Procedures”] OR [mh orthopedics] OR [mh cartilage] OR [mh ligaments] OR [mh muscles] OR [mh tendons] OR [mh joints] OR [mh “musculoskeletal diseases”] OR [mh “musculoskeletal abnormalities”] OR [mh “Sports Medicine”] 88268 #6 [mh ^”musculoskeletal system”] OR [mh ^skeleton] OR [mh ^”bone and bones”] OR [mh ^”bone-implant interface”] OR [mh “bones of lower extremity”] OR [mh “bones of upper extremity”] OR [mh “sesamoid bones”] 6561 #7 [mh ^”wounds and injuries”] OR [mh “accidental injuries”] OR [mh “amputation, traumatic”] OR [mh “arm injuries”] OR [mh “athletic injuries”] OR [mh “crush injuries”] OR [mh “joint dislocations”] OR [mh “fractures, bone”] OR [mh “fractures, cartilage”] OR [mh “hand injuries”] OR [mh “leg injuries”] OR [mh “multiple trauma”] OR [mh “shoulder injuries”] OR [mh “soft tissue injuries”] OR [mh “sprains and strains”] OR [mh “tendon injuries”] 20543 |
| 9 exp three dimensional printing/ or exp rapid prototyping/ or exp fused deposition modeling/ or exp powder bed fusion/ or exp robocasting/ or exp stereolithography/ or exp three dimensional bioprinting/ or exp computer aided design/ or exp three dimensional computer aided design/ 54213 |
8 (orthopedic* or orthopedic* or musculoskeletal* or bone* or joint* or fracture* or muscle* or ligament* or tendon* or injur* or arthroplast* or arthroscop* or osteoporosis or osteoarthritis).mp. 4027622 |
TS = (“print*” OR “additive manufacturing” OR “patient-specific implant*” OR “rapid prototyp*” OR “computer-aided design*” OR “CAD/CAM” OR “scaffold fabrication” OR “tissue engineering” OR “personali?ed medicine” OR “medical model$ing” OR “digital manufacturing” OR “customi?ed implants”)) |
#8 (orthopedic* OR orthopaedic* OR musculoskeletal* OR bone* OR joint* OR fracture* OR muscle* OR ligament* OR tendon* OR injur* OR arthroplast* OR arthroscop* OR osteoporosis OR osteoarthritis): ti,ab,kw 297208 |
||
| Number of articles retrieved (Duplicates) | 1142 (21) | 684 (320) | 582 (228) | 584 (405) | 307 (30) |
Author contributions
P.J.M. and R.A. were involved in the screening, data review, article redaction, critical review, and approval. P.J.M. also contributed toward the search. K.S. and S.A. contributed toward data review, article redaction, critical review, and approval. R.H. contributed toward study planning, data review, article redaction, critical review, and final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This review involved human data from previously published studies only. Informed consent was not needed.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.