
Abstract
Background:
Management of radiation proctitis presents a treatment challenge. Limited data exist on the management of symptomatic hemorrhoids in radiated patients. This study aims to present a practical approach to the management of radiation proctitis, particularly in patients with synchronous hemorrhoids.
Methods:
A total of 52 consecutive cases of radiation proctitis managed between September 1999 and October 2017 were retrospectively reviewed. The primary treatment was formalin application, plus rubber band ligation in conjunction with formalin when hemorrhoids were a significant component of bleeding, and occasionally argon plasma coagulation.
Results:
The primary indication for radiotherapy was for the treatment of prostate cancer (71%), anal squamous cell carcinoma (10%), and gynecological malignancies (18%). More than half of the patients (52%) presented with radiation proctitis and concomitant internal hemorrhoids. The hemorrhoids were managed with rubber band ligation (56%) and stapled hemorrhoidectomy (7%), at the same procedure as formalin application. At a median follow-up of 12 months, no recurrent rectal bleeding occurred, and no further treatment was needed for most patients. One patient experienced a short period of perianal pain, which was treated with analgesics.
Conclusion:
Formalin application has consistently demonstrated an excellent cure rate and safety profile comparable with the published results as a primary treatment for radiation proctitis. The prolapse of irradiated mucosa over the internal hemorrhoids appears to exacerbate bleeding. Local hemorrhoid treatment is often required as an adjunct in the management of these patients.
Background
Radiation proctitis (RP) is a serious complication seen in patients who have received irradiation during treatment for tumors located in the pelvis. The development of this condition varies with the dose of radiation, the delivery method, and the organ being radiated, ultimately resulting in an incidence of chronic RP in nearly 5% of patients (1–3).
The radiation doses delivered to the pelvis generally vary from 45 to 50 Gy for adjuvant or neoadjuvant treatment for prostate or anorectal malignancies, but may be up to 90 Gy for the definitive therapy for gynecological malignancies. Treatment doses less than 45 Gy usually cause few side effects. However, the dosage range for most treatments, which is generally between 45 and 70 Gy, can lead to more complications (1–4). Even higher doses of radiotherapy can result in collateral damage to surrounding organs in the field of radiation. Newer modalities allow for the use of higher doses of radiation for target tissues with less exposure of normal tissues. External beam radiation studies report incidence rates ranging from 2% to 39%, whereas intensity-modulated radiation therapy studies report incidence rates from 1% to 9% and particle radiation therapy in the range of 1% to 2%. The incidence of proctitis in patients treated with brachytherapy alone is 8% to 13% but may be as high as up to 21% when used in combination with other modalities (4).
Treatment of RP has been investigated for several years employing numerous small studies to determine which methods are truly effective. Various medical strategies like steroid sucralfate enemas, antibiotics, 5-aminosalicylic acid derivatives, probiotics, antioxidants, formalin instillation, and hyperbaric oxygen are available for the treatment with variable efficacies (1–3). More invasive treatments including endoscopic-based, focally ablative interventions such as bipolar cautery, argon laser, radiofrequency ablation, or argon plasma coagulation (APC) are also available (1, 3). Currently, there is no gold standard available for the treatment of chronic RP (5). Some therapies have shown only mild efficacy, but others present a promising option for practitioners (1, 3).
Management of rectal bleeding in patients with hemorrhoids and concomitant RP presents a challenge. Surgeons are aptly concerned about using conventional methods of treatment in these patients, such as cauterization of bleeding areas in the rectum, rubber band ligation (RBL), excisional, and stapled hemorrhoidectomy, for fear of poor healing and possible exacerbation of the original problem. There is limited literature reporting head-to-head comparisons of the various treatment options for RP alone via a randomized controlled approach. Also, limited literature exists about the management of symptomatic hemorrhoids in the radiated patient.
The objective of this study is to describe our experience and present a practical approach to the management of RP particularly in patients with coincident symptomatic hemorrhoids.
Materials and Methods
The basis of this approach to RP and hemorrhoids was the senior author’s observation that about half of the patients he was referred with RP also had obvious internal hemorrhoids. In those patients, he observed that formalin application alone was often unsuccessful, and he deemed it necessary to manage the internal hemorrhoids at the same time as the RP was treated. This approach then continued, with formalin application alone being the primary treatment for RP alone, RBL plus formalin application being the primary treatment for RP with obvious internal hemorrhoids, and APC used only after three or four failed attempts with formalin-based treatment.
Study Design and Participants
A total of 52 consecutive cases of RP managed between September 1999 and October 2017 were retrospectively assessed. Full bowel preparation was performed if complete colonoscopy was required. Otherwise, the patients were given an enema and instructed to have a strict, clear diet a day before the procedure. The procedure was performed under general anesthesia with the patients placed in lithotomy position.
Details of Patient Management
The appearance of the affected mucosa was numerically graded 0–4 where 0 indicates normal mucosa; 1, mild erythema; 2, diffuse erythema and punctate hemorrhage; 3, frank hemorrhage; and 4, ulceration (6, 7). The length of affected mucosa involvement was determined by endoscopic assessment with distance measured from the anal verge. Only patients with severity of grade 2 and above underwent further treatment. Fig. 1 shows the endoscopic finding in a patient with grade 2 RP.
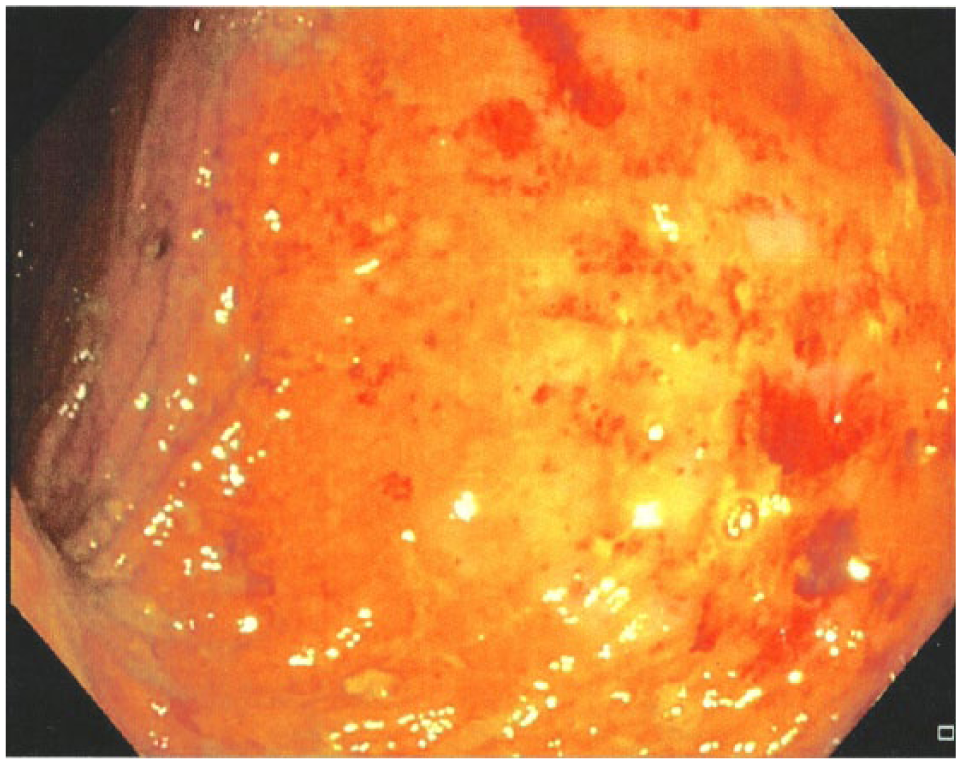
Endoscopic finding in a patient with grade 2 radiation proctitis showing diffuse erythema and punctate hemorrhage.
Formalin 4% Application
With the patient in the lithotomy position, the anus and buttocks are smeared with lidocaine jelly to prevent direct contact with the formalin solution. Direct contact with gauze soaked with 4% formalin applied to each bleeding area of the rectum for 2–3 min is allowed until slight blanching of the mucosa is achieved. At the end of the procedure, the perianal skin is irrigated well with normal saline.
RBL
RBL was performed for the majority of grade 2–3 bleeding internal hemorrhoids at the same procedure as formalin application. Because formalin application changes the elasticity of the hemorrhoidal mucosa, it is necessary to band hemorrhoids first before applying the formalin; otherwise, the mucosa is harder to draw up into the band ligator, and the rubber bands are more likely to be dislodged from the mucosa.
APC
APC was used with the argon glass flow rate ranging between 1.5 and 2 L/min with an electrical power of 60 W. APC was performed with a 2.7-mm probe using the no-touch technique. Telangiectasias were coagulated with pulses of 1- to 2-s duration unless they were particularly confluent.
Patients were discharged the same or the next day. Follow-up was at 4–6 weeks. If rectal bleeding persists, patients were scheduled for another treatment with either of the above-mentioned treatment options.
Variables Measured
Patient age, sex, type of malignancy, the method of treatment, complication, and recurrence of symptoms were obtained from their hospital records and the consulting surgeon’s office.
Statistical Analysis
The Pearson chi and Fisher’s exact tests were used to test for significance of differences between groups. All analyses were conducted using SPSS version 23 (SPSS Inc., Chicago, IL, USA), and p < 0.05 was considered statistically significant. This study was approved by the Sydney South West Area Health Service Ethics Review Committee (RPAH Zone).
Results
Demographics
Between September 1999 and October 2017, 52 RP cases were managed by a single surgeon. Patient demographics and summary of treatment received for RP are shown in Table 1. The median patient age was 72 years (range 43–89, standard deviation (SD) 9.5) and the majority (75%) were males. The median interval from the conclusion of radiotherapy to the onset of symptom was 2 years (range 1–24; SD 4.5). The primary indication for radiotherapy was for the treatment of prostate cancer (71%), anal squamous cell carcinoma (10%), cervical cancer (10%), endometrial cancer (8%), and bladder carcinoma (2%). The most common primary presenting symptom was bleeding (63%), followed by rectal mucus discharge (17%), diarrhea (8%), fecal urgency (8%), and rectal pain (4%).
Demographics of patients undergoing treatment for radiation proctitis (n = 52).
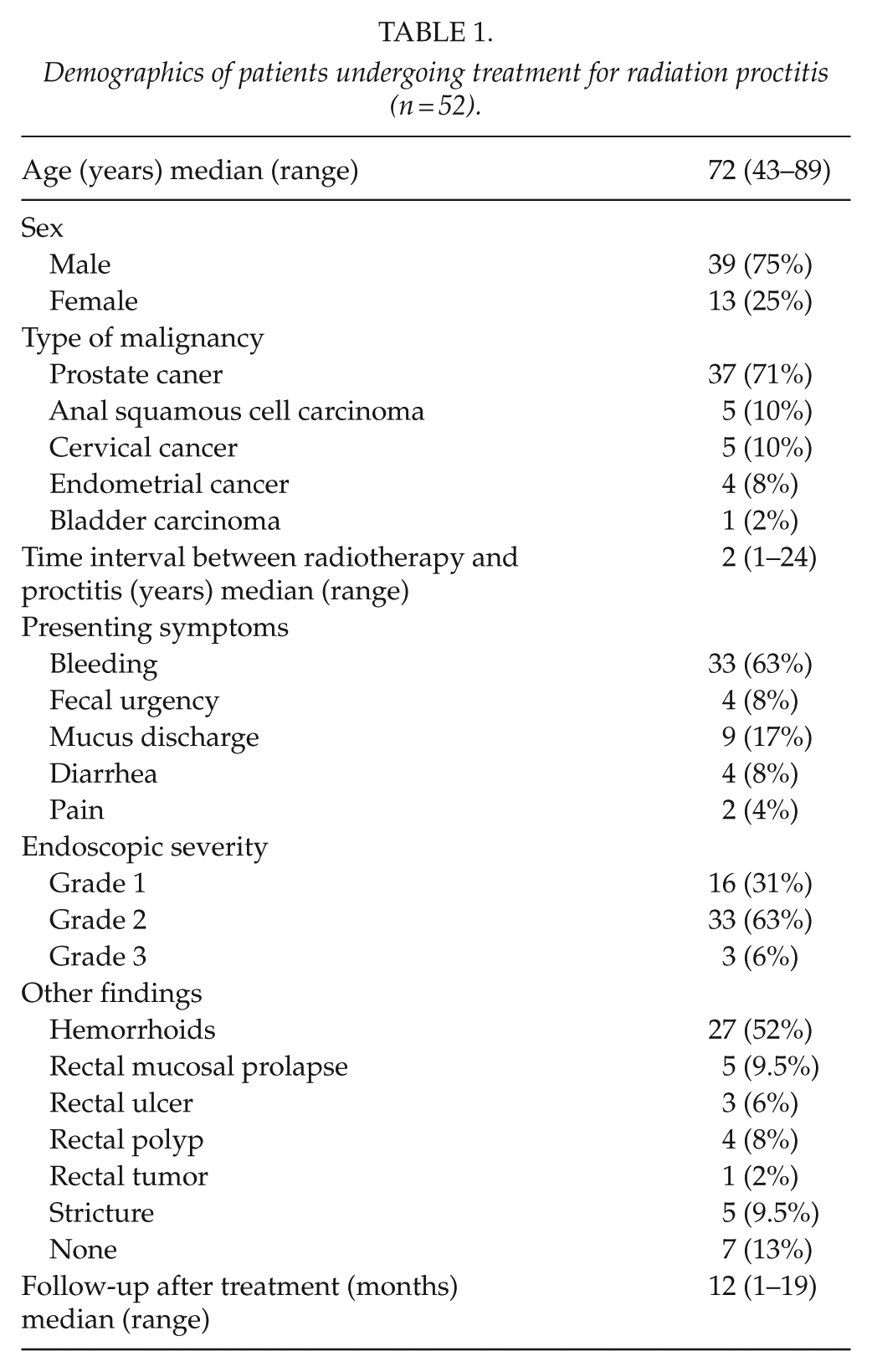
The majority of the patients had either grade 1 (31%) or grade 2 (63%) severity of RP. Only three (6%) patients had grade 3 severity at the time of the procedure. The majority of the patients had rectal involvement starting from 4 to 8 cm from the anal verge, with the mean length of rectal involvement at 5 cm (range 4–13; SD 1.9). Other associated findings with RP include internal hemorrhoids (52%), stricture (9.5%), rectal mucosal prolapse (9.5%), rectal polyp (8%), rectal ulcer (6%), and rectal tumor (2%).
Management of RP
All 16 patients (31%) with grade 1 RP and minimal symptoms were managed conservatively. Meanwhile, patients with grade 2 and grade 3 RP were managed with either surgery (4%) or endoscopic-based treatments (65%). Formalin 4% application, combined formalin 4% application and APC, and APC alone were performed for the latter (Table 2).
Summary of management received by patients undergoing treatment for radiation proctitis (n = 52).
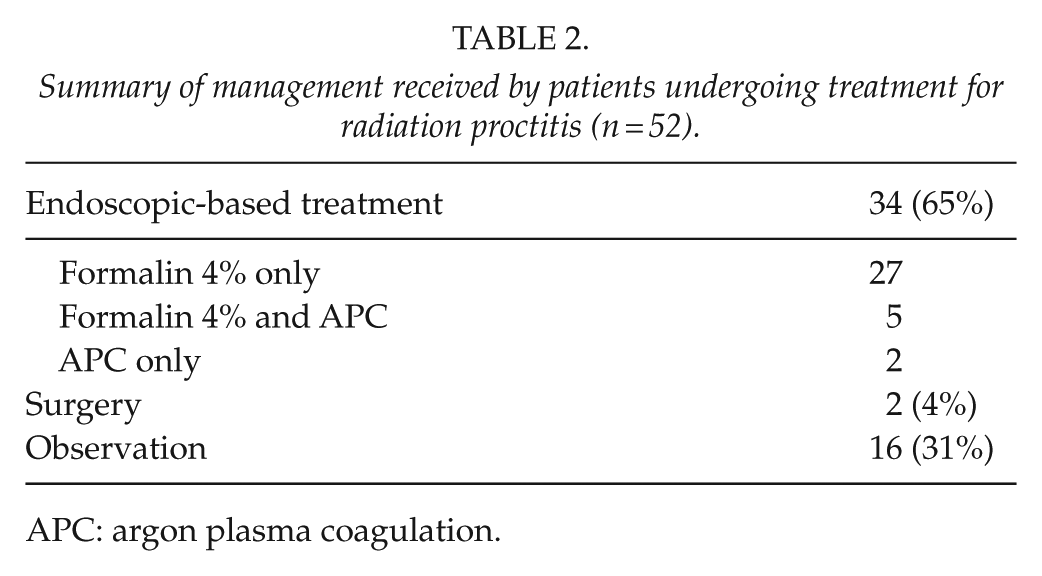
APC: argon plasma coagulation.
In 70% (19/27) of the patients who underwent formalin 4% application alone, the bleeding stopped after a single treatment. The other 30% (8/27) of the patients required two to four treatments before cessation of bleeding. In five patients who needed a combination of formalin and APC treatments, three required only one treatment session, while the other two patients required two treatment sessions to control bleeding fully. Meanwhile, the two patients who underwent APC treatment alone only needed one session to control bleeding. There was no significant difference between the endoscopic-based treatment modality used and the number of treatment sessions required to control bleeding (p = 0.902) (Table 3).
Comparing endoscopic-based treatment used to manage radiation proctitis and number of sessions required to control bleeding (n = 34).
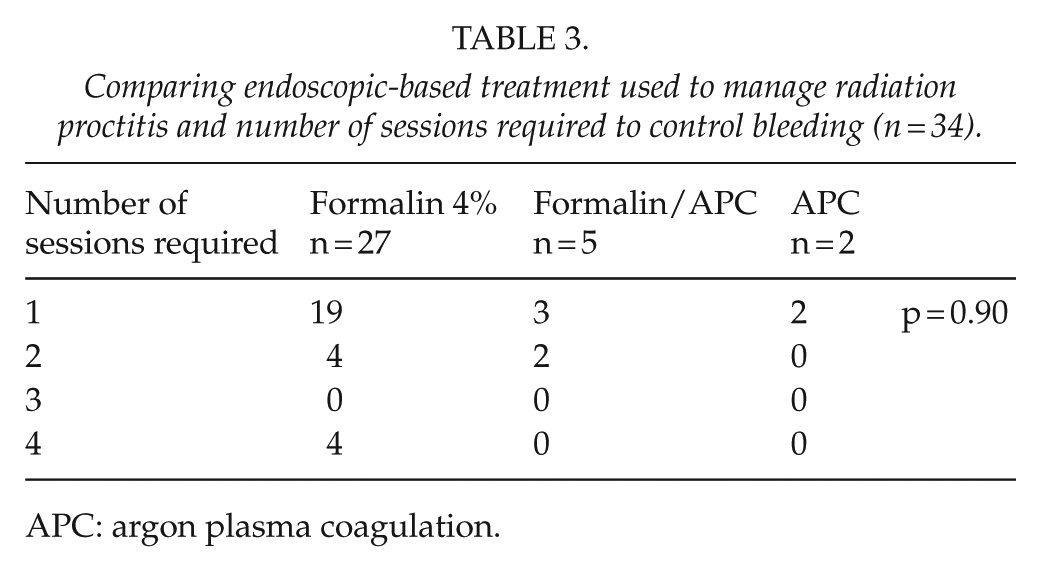
APC: argon plasma coagulation.
One patient had an abdominoperineal resection for persistent bleeding and chronic anemia despite multiple previous attempts to control bleeding with formalin. Fig. 2 shows the resection specimen in this patient demonstrating mucosal atrophy and numerous dilated superficial blood vessels. One patient who initially presented with pain and obstruction from a high-grade rectosigmoid stricture had a low anterior resection.
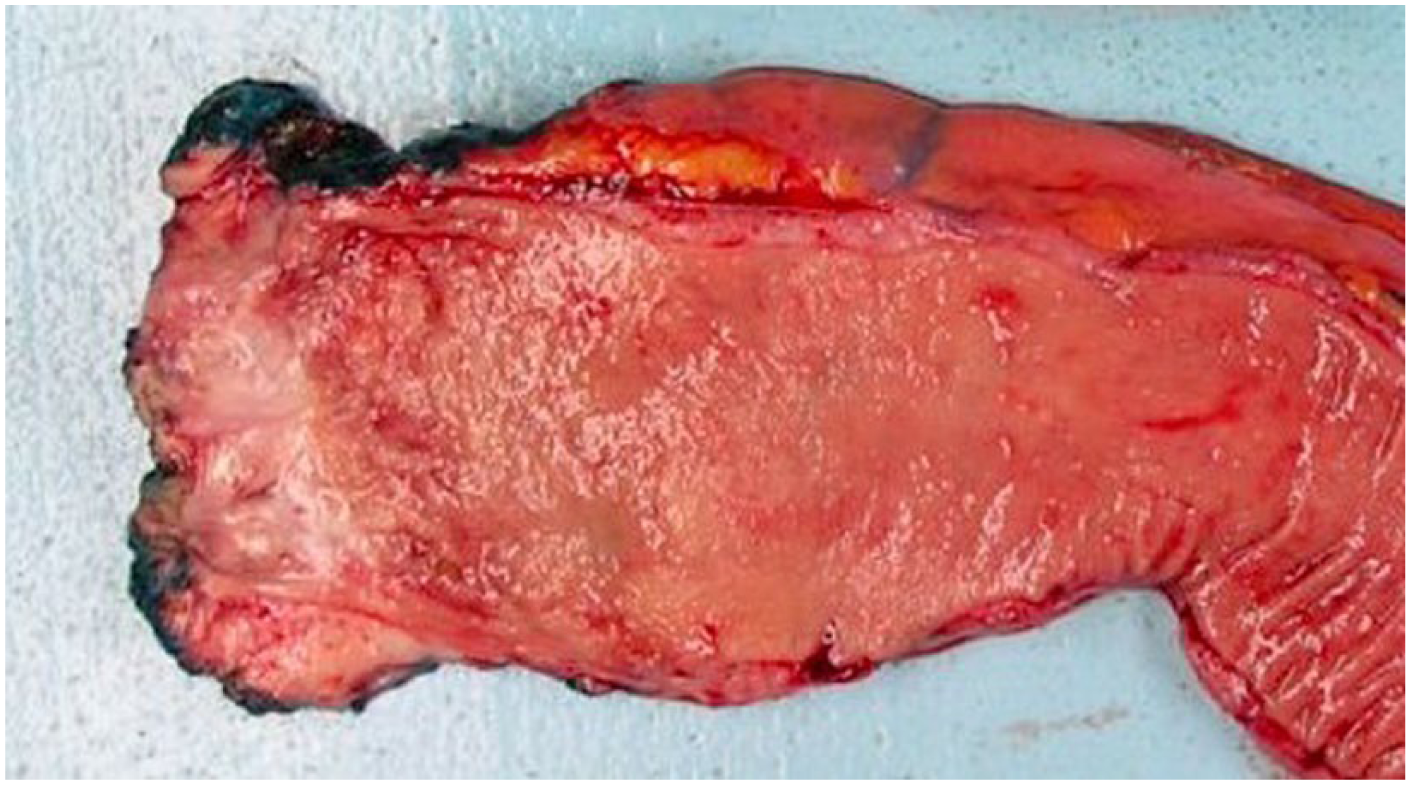
Abdominoperineal resection specimen in a patient with radiation proctitis who presented with persistent bleeding and chronic anemia despite multiple previous attempts to control bleeding with formalin. The rectum shows mucosal atrophy with dilated superficial blood vessels.
Management of RP and Hemorrhoids
Table 4 summarizes the management received by the 27 patients who presented with RP and concomitant internal hemorrhoids. The majority of the hemorrhoids were managed with RBL (56%). Three (range 2–4) hemorrhoidal piles were banded at the same time per treatment. Stapled hemorrhoidectomy was performed in two (7%) patients with circumferential hemorrhoids. In all, 10 patients (37%) with small internal hemorrhoids were managed conservatively (Fig. 3).
Summary of management received by patients undergoing treatment for radiation proctitis and internal hemorrhoids (n = 27).
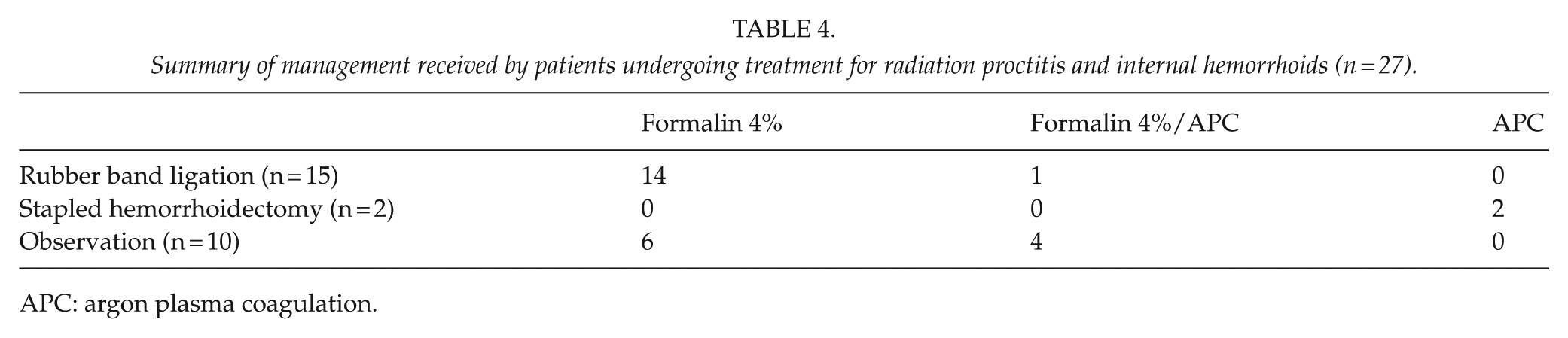
APC: argon plasma coagulation.
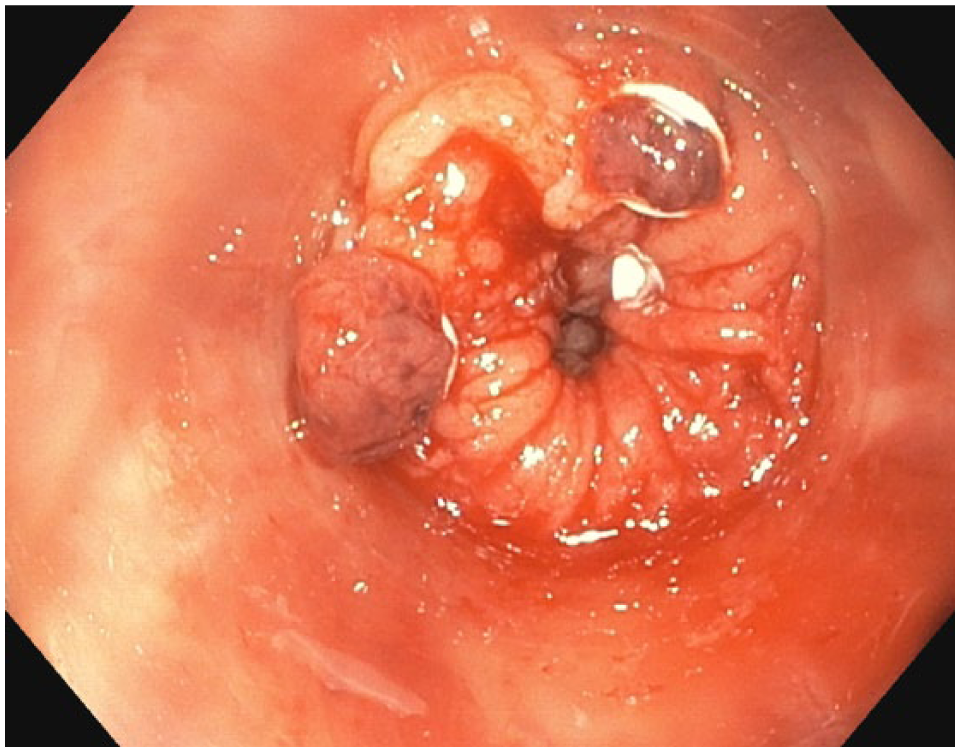
Endoscopic finding in a patient with radiation proctitis and hemorrhoids after rubber band ligation and formalin 4% application.
Patients were followed-up for a median duration 12 months (1–19; SD 5.1). At the final follow-up, no recurrent rectal bleeding occurred, and no further treatment was needed for most patients. There was no major complication or mortality in this series. One patient experienced a short period of perianal pain, which was abated quickly when treated with analgesics.
Discussion
RP is a relatively common and potentially devastating consequence of modern radiation therapy (3, 7). It can be classified as acute or chronic depending on the temporal relationship to the course of radiotherapy. The clinical picture of RP varies from asymptomatic to potentially life-threatening. Acute proctitis presents more commonly with diarrhea, urgency, or pain, while bleeding and fecal incontinence occur less frequently (8, 9). Chronic RP can include any of the acute symptoms that persist past 3 months after the initiation of treatment or develop independently at a later time. Also, it presents more frequently with rectal bleeding as a symptom compared to acute proctitis. Finally, chronic RP can also include the development of symptoms that are generally not seen in acute proctitis, such as stricture, obstruction, or fistula formation (8, 9).
The reported incidence of any transient acute RP is thought to range from 50% to 100%, while the incidence of chronic RP is considerably less common with estimates ranging from 2% to 20% of all patients treated with radiation for pelvic malignancy (10, 11). The median time for the development of chronic symptoms after radiation treatment is between 8 and 13 months in the majority of the series (1, 6). Although, a few series do report a considerably longer latent period, with initial symptoms developing more than 30 years after completing radiation (1). The median time to symptom occurrence in our series is 2 years and the longest latent period we recorded is 24 years after radiotherapy. These observations highlight the burden of this disease on our patients with a previous history of radiation. Hence, they should be informed of these possibilities and the potential need for long-term follow-up.
Formal diagnosis of RP involves direct visualization of the suspicious post-radiated tissues. Mucosal features indicative of RP include pallor, friability, and telangiectasias (1). Biopsy of the area is not always necessary, though this can help rule out other causes for symptoms like inflammatory bowel disease or malignancy. In our series, one patient presenting with rectal bleeding developed an irradiation-induced rectal tumor after 24 years of completing radiotherapy for prostate cancer. Radiotherapy for prostate cancer has been linked to the late occurrence of second malignancies due to low-dose radiation scatter (1, 6). Although these cases are rare, it should always be considered in a patient being managed for RP.
Formalin scleroses and seals fragile neo-vasculatures in radiation-damaged tissues to prevent further bleeding through chemical cauterization. The half-life of a systemically absorbed formalin is known to be 90 min, and the initial histological change after treatment is limited to the mucosal layer (12, 13). Formalin therapy is simple yet results in a significant improvement of the hemoglobin levels and the requirement of blood transfusion in patients with rectal bleeding from RP (14). It has been one of the most studied applications for chronic RP. It is being used in several different preparations including 2%, 4%, 5%, and 10% concentrations, used as irrigation versus formalin-soaked gauze, and performed either in the office or the operating room (15, 16). The results using either technique have similar success rates ranging from 75% to 100%, mostly in one or two treatments (14, 16). A canine model showed that a lower concentration with lesser contact time is essential to decrease systemic toxicity (13). Some studies suggest that a solution of less than 4% can successfully be used without significant toxicity (15, 16). Formalin concentration and method of application are crucial for the treatment success since these factors directly affect the risk of the formalin side effects. Among the reported acute treatment side effects include anal pain, transient incontinence, diarrhea, fever, and colitis. The majority of these side effects occur because of the difficulty in stopping the formalin from extending proximally or distally outside the treatment area, particularly with the instillation technique (12, 13). Direct application of formalin allows for the more accurate application of treatment and possibly fewer strictures, but it may not be feasible with large mucosal areas affected and could lead to fistula formation. Although formalin application has been regarded as generally safe, significant complications including bleeding, strictures, and fistulas, worsening of radiation stricture, worsening of incontinence, and severe pain have been reported (14–17). Therefore, patients with pre-existing symptoms, or those arising from radiation injury, should carefully be evaluated before treatment.
APC is a safe, well-tolerated, and effective treatment option in extensive chronic RP that is refractory to medical management. It is easy to perform and efficacious and has a good safety profile if performed correctly (7, 17). APC has minimal tissue penetration, making it attractive for treatment of superficial bleeding. Brief pulses of 1–2 s should be used to minimize the depth of thermal penetration to reduce the risk of perforation, excessive ulceration, and stricture (7, 17). Five small series, each with 20–40 patients, examined the efficacy of APC in patients with bleeding from chronic RP (7, 17). Single sessions have been reported to improve symptoms significantly, but on average, two to three treatments are needed to achieve this result. Most of the complications reported are mild and included cramps, mucus discharge, and stricture. However, significant complications including large ulcers, perforations, and rectourethral and rectovaginal fistulas have also been reported (7, 17).
Formalin application is not always effective, particularly in large areas. In some cases, we combined formalin with APC in managing moderate to severe RP to successfully stop the bleeding. Formalin application was used initially to address large areas of rectal mucosal involvement, which was complemented by the use of APC to treat localized remnant bleeding lesions precisely.
The management of hemorrhagic RP is challenging because of the necessity for repeated intervention. There is some controversy regarding the factors that correlate with the number of interventions required to achieve hemostasis. Some studies have reported that the endoscopic grade of RP correlates with the severity of bleeding and the number of interventions needed for hemostasis (18). But this has been subjected to scrutiny due to lack of uniformity in the description of endoscopic grading of RP. Previous studies have also identified an association between the extent of the proctitis and the number of treatment sessions required (19). However, in a study done by Siow involving 91 patients with hemorrhagic RP, they found no statistically significant correlation between the length of proctitis and the number of treatment required (7). Similarly, they reported no statistically significant associations between age, gender, ethnicity, and primary disease with the number of treatment sessions.
The main challenges encountered when considering the surgical management of patients with RP are whether or not surgery is indicated and, if so, what surgical intervention is most appropriate. Approximately 2.6% of patients will undergo surgery as a result of complications of RP (10). The decision to proceed with surgery is more straightforward when patients present with high-grade stricture, fistulae, or perforation. While historical data show that surgery is rarely employed for bleeding patients who are refractory to medical treatment, data reported by Yuan support colostomy formation in patients who are transfusion-dependent showing significant improvements in quality of life (20). However, diversion alone does not remove the damaged tissue leaving the patient at risk of continued complications including bleeding, perforation, occlusion, and abscess formation (10). In some instances, proctectomy may be the only option available, although it carries higher risks. A recent meta-analysis demonstrated a 40% lower rate of morbidity with diversion when compared to resectional surgery and, while not statistically significant, also shows a 32% lower rate of mortality in favor of diversion versus resectional surgery (10).
Very limited data exist regarding the management options and outcomes in patients with hemorrhoids and concomitant RP. The prolapse of the damaged mucosa over the internal hemorrhoids in radiated patients seems to exacerbate bleeding. We believe that addressing the hemorrhoids can be a useful adjunct to control bleeding effectively. In a survey-based investigation by Hawkins to get a consensus among colorectal surgeons on the management of these patients, the majority of those who responded treat RP initially as treatment of the patient’s hemorrhoids; however, more than half of the respondents reported that hemorrhoidectomy is the most effective method of treatment after failure of primary RP treatment (21). Although there was no consensus reached, it was noted that treating the RP alone, hemorrhoidectomy, RBL, or injection sclerotherapy is reasonable in treating patients with symptomatic hemorrhoids and coincident RP until more data are available to determine the best therapy.
Limitations
There are limitations to the conclusions that can be drawn from this study because of the number of patients and its retrospective design. We are, however, encouraged by the ease of the procedure, safety, and low morbidity.
Conclusion
Formalin, APC, and the combined method of formalin and APC have consistently demonstrated an excellent cure rate and low morbidity profile comparable with the published results as a primary treatment for RP. The clinical results of this series also show that the addition of RBL is effective in managing the internal hemorrhoids. We believe the key finding of our study is the confirmation that in patients with RP and significant hemorrhoidal bleeding, the hemorrhoids need to be dealt with as well.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.