
Abstract
Background and Aims:
Chronic radiation proctitis is a disease associated with radiotherapy of cancer in the pelvic region. The main symptom is rectal bleeding. Several treatment modalities have been attempted, but few have demonstrated satisfactory effects. We present our experience with formalin applied locally to the rectal mucosa in the treatment of chronic radiation proctitis. Furthermore, we assess possible complications, the gravest suggested being cancer. Previous studies on the subject have reported good results, but often with a somewhat vaguely defined follow-up. Our evaluation of the treatment was based on both subjective symptoms and proctoscopic findings.
Material and Methods:
A small study (N = 11) was conducted retrospectively. All patients treated for chronic radiation proctitis with formalin in our clinic were identified, and data concerning effect and complications were collected by studying the patients’ records, with a questionnaire and a follow-up interview and proctoscopy.
Results:
The study showed a marked decrease in bleeding and objective signs of proctitis in all patients. Complete cessation of bleeding was achieved in five patients. Possible complications to the treatment detected in our study were the following: anorectal pain, tenesmus, incontinence, diarrhea, and mucous rectal discharge. No signs of neoplasia were found.
Conclusions:
The formalin treatment had a very good effect on chronic radiation proctitis. Possible complications were detected. Except in the case of anorectal pain, these are all of a questionable nature and can possibly be attributed to chronic radiation proctitis itself rather than the formalin treatment. Further study is warranted to confirm long-term effects of the formalin and to exclude possible complications, especially secondary anorectal cancer.
Introduction
Radiotherapy is an increasingly common component in the management of cancers in the pelvic region. A side effect to pelvic irradiation is inflammation in the rectum, proctitis. In most cases, this acute proctitis is self-limiting (1–7), but a chronic variant, chronic radiation proctitis (CRP), can develop either following the acute state or even several years after treatment completion. The relation between the acute and chronic forms is not entirely established (2–4, 6, 7), neither is the frequency with which CRP occurs. Thus, incidences ranging from 1%–20% are proposed in different publications (2, 5, 8–12). Suggested predisposing factors include technical details concerning the radiation treatment, such as radiation dose and duration, obesity, diabetes, hypertension, atherosclerosis, adjunctive chemotherapy, history of abdominal surgery, age and sex (2, 4, 6, 13).
Histologically, the disease is characterized by subintimal fibrosis and obliterating endarteritis with thrombosis and thereby relative ischemia, which leads to vascular proliferations and telangiectasias. This makes the vessels in the rectal wall fragile and prone to bleeding, which explains the main symptom of CRP: rectal bleeding, occasionally necessitating blood transfusions. Other symptoms include anorectal pain, diarrhea, mucous rectal discharge, tenesmus, incontinence, ulcerations, fistulae, strictures/stenoses, and perforation (2–7, 11, 13, 14).
Several treatment modalities have been attempted, but few have demonstrated satisfactory results. Medical treatments, including steroids administered both orally and locally, local 5-aminosalicylic acid (5-ASA) derivatives, oral and local sucralfate, oral metronidazole, local short chain fatty acids, and combinations of these, have been shown to be of limited or no effect (2–6, 13, 15). Hyperbaric oxygen therapy has shown promising results, but the treatment is extremely time consuming, very expensive, and restricted to highly specialized centers (2–6, 13). Endoscopic treatments are numerous and are generally effective in treating the bleeding. Unfortunately, most are associated with a risk of damaging the rectal wall (1, 2, 4, 6, 7, 13, 15–18). The best endoscopic treatment seems to be argon plasma coagulation, both with respect to achieving effect and minimizing complications. There is broad consensus that surgery should be considered a last resort due to its high morbidity and mortality (4, 6–8, 12, 13, 15, 17–19).
The use of formalin in the treatment of radiation-induced inflammation is well known. It was introduced in 1969 as a treatment for radiation cystitis (20) and in 1986, attempted on a CRP-patient as an enema (21). In 1993, the first multipatient study with longer follow-up periods was published (15), this time employing local application of formalin to affected tissue. The mechanism by which formalin works is a matter of debate. It probably relies on coagulation necrosis limited to the mucosa with the ischemia caused by thrombosis of the fragile neovascularisations (1, 5, 16, 18, 22). Another theory proposes cross-linking or hydrolysis of the tissue proteins as a key process (1, 10).
Reviews on the subject (3, 6, 7, 23) tend not to distinguish between topical treatment and enemas when reporting effect and possible complications. There is, however, some indication that topical application of the formalin could result in fewer complications due to its briefer and more controlled contact with the mucosa (4, 5, 14), sparing the more proximal parts of the intestine as well as the anal canal, which is somatically innervated by the inferior rectal nerves and thus highly sensitive to pain. All studies have generally produced good results with regard to effect. One of the more recent studies (1) treated a study population of N = 100 with 10% topical formalin, instead of the more frequently used 4% solution, and reported an impressive response rate of 93%. In this study, however, as with the majority of studies published to date (9–12, 17, 19, 24, 25), follow-up regimes are unclearly defined, particularly with respect to posttreatment proctoscopy. Stern and Steinhagen (11) have raised the concern that the formalin treatment could possibly cause cancer. Based on above-mentioned aspects, we chose the topical application modality with 10% formalin as treatment, using a proctoscope instead of anal retractors, as these seem to be associated with increased morbidity (5, 7, 14, 18). The purpose of this study was to evaluate the treatment by adhering to a strict posttreatment program fusing subjective symptoms with proctoscopic findings, producing clear endpoints for both effect and complications. In addition, the proctoscopic examinations were performed with thought to the proposed risk of cancer.
Material and Methods
We conducted a retrospective study on patients who had been treated with formalin for CRP in the outpatient clinic of the abdominal surgery ward, Aarhus University Hospital, Tage Hansens Gade, since the introduction of this treatment in 2007. The patients were identified by thorough scrutiny of the outpatient clinic’s appointment records. The patients’ medical records were obtained and specific information concerning the patients’ baseline symptoms and the physician’s observations was extracted. Possible complications related to the formalin treatment were also noted. Follow-up consisted of a questionnaire sent to the patients, an interview, and a proctoscopic examination. In the questionnaire and the interview, we investigated the patients’ view on the effect of and possible complications related to the treatment. The proctoscopic examination (focusing on the signs of proctitis: erythema, pallor with friability, telangiectasias, and ulcerations) was conducted to add objectivity to the subjective symptoms reported by the patients and to screen for neoplasia. Data from these sources were combined to form the follow-up results presented below.
The treatment itself consists of a varying number of sessions. The patient is placed in the lithotomy position, and a cotton applicator soaked in 10% formalin is inserted via a rigid proctoscope. The areas of fragile/bleeding mucosa are identified by proctoscopy, and the cotton applicator soaked in formalin is gently pressed against the area under visual guidance. The formalin effect can be immediately assessed by cessation of bleeding and mucosal blanching. No anesthesia is required, and the treatment can be performed in an outpatient clinic with intervals of around 1 month between treatments.
Results
A total of 11 patients, 7 male and 4 female, were initially identified. Patient age at first treatment session was between 53 and 82 years (median = 71). The patients had a previous history of undergoing radiotherapy for prostate cancer (n = 7), cervical cancer (n = 3), or vaginal recurrence of endometrial cancer (n = 1). The time interval from termination of radiotherapy to commencing the formalin treatment was between 10 and 47 months (median = 18), implying CRP and not merely acute radiation proctitis. Four patients had low hemoglobin levels prior to initiation of formalin treatment, and two of them had required blood transfusions. Six patients had experienced other symptoms related to CRP than bleeding before treatment, specifically anorectal pain (n = 1), diarrhea (n = 2), mucous rectal discharge (n = 3), tenesmus (n = 1), and incontinence (n = 3). Six patients had received some other form of treatment for CRP beforehand, specifically local steroids (n = 6), 5-ASA derivatives (n = 1), sucralfate (n = 1), and short chain fatty acids (n = 3). All these had limited or no effect. One patient was being treated with an anticoagulant agent (warfarin). Follow-up period for our patients was calculated from completion of treatment to follow-up and was between 1 and 34 months (median = 19).
Table 1 shows results for each patient with respect to response and complications. Bleeding before treatment is graded as persistent when an everyday occurrence is reported, or intermittent when occurring once, or several times, a week. Complete response (CR) represents complete cessation of bleeding and no proctoscopic signs of proctitis at follow-up, while partial response (PR) denotes marked decrease in symptoms but where patients now and then may experience bleeding of a milder character with or without minor proctoscopic signs of proctitis persisting.
Patient data, response and complications.
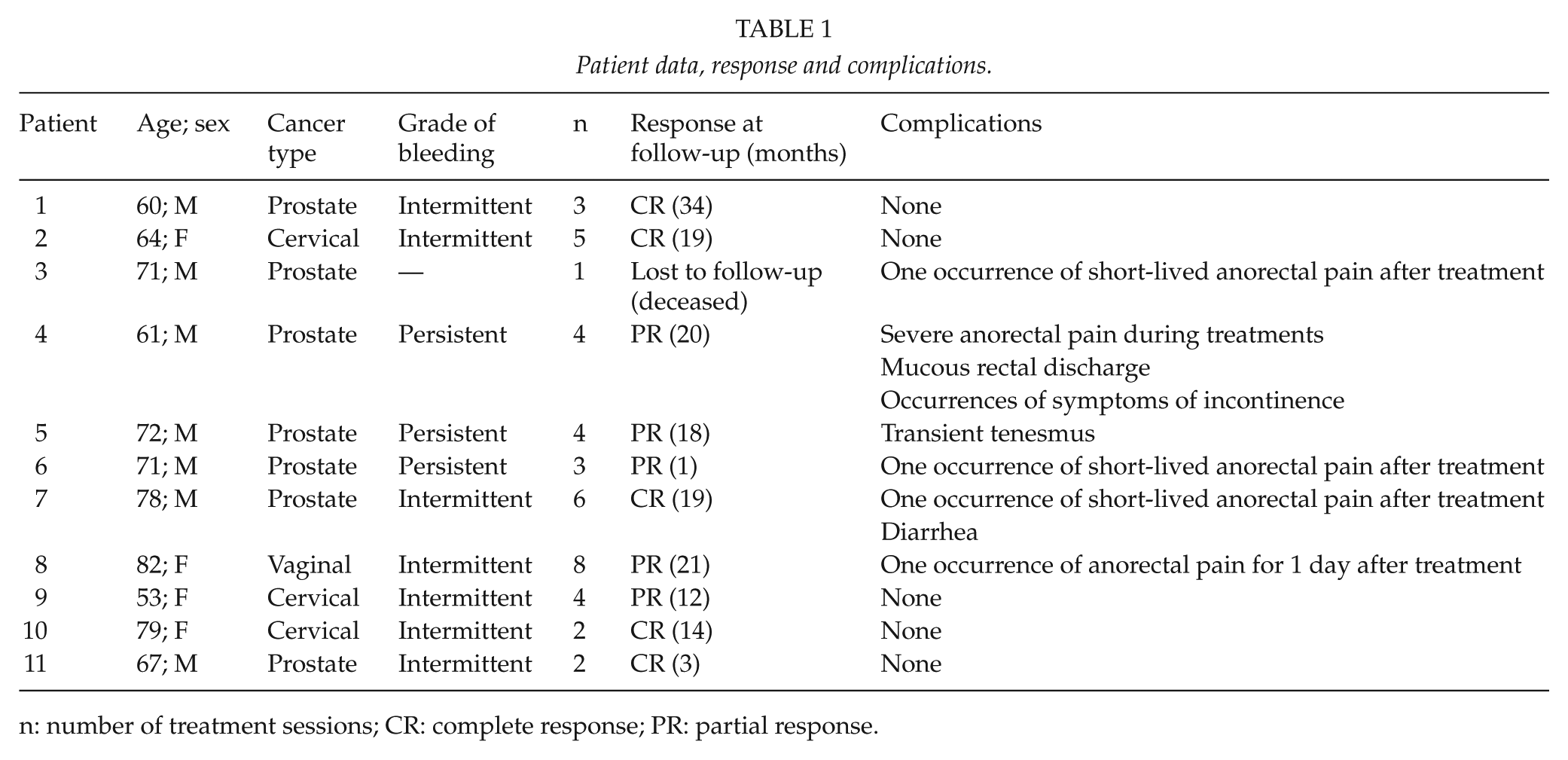
n: number of treatment sessions; CR: complete response; PR: partial response.
All patients had a marked reduction in both symptoms and objective findings at follow-up. Five patients experienced complete cessation of bleeding and no proctoscopic signs of proctitis (CR) while five showed a PR. One patient was lost to follow-up. His death was unrelated to both CRP and the formalin treatment. The following is a brief look at the partial responders individually.
Before starting treatment, Case 4 experienced daily bleeding resulting in anemia. After treatment completion, the bleeding had diminished to about once a month. There were no objective signs of inflammation, and the bleeding was suspected to originate from hemorrhoids. Furthermore, the result might be affected by the fact that the patient was undergoing treatment with warfarin. Prior to treatment, Case 5 also suffered from low hemoglobin levels due to profuse daily bleeding with mucous discharge. The bleeding was reduced to less than once a week at follow-up, and the mucous discharge had subsided. Case 6 went from requiring blood transfusions due to his daily rectal bleeding to minor bleeding about once a week. Case 8 and Case 9 experienced a decrease in bleeding from several times a week to negligible bleeding episodes about once a week and once a month, respectively.
As mentioned earlier, we noted anemia in four of our patients. This condition was reversed in all patients at the end of the study. Besides having the effect on bleeding outlined above, the formalin treatment showed effect on other of the patients’ reported CRP symptoms, specifically improvement of anorectal pain (n = 2), cessation of diarrhea (n = 2), cessation or improvement of mucous rectal discharge (n = 3), and cessation or improvement of incontinence (n = 3).
Complications reported were anorectal pain (n = 5), tenesmus (n = 1), mucous rectal discharge (n = 1), diarrhea (n = 1), and incontinence (n = 1). The complaints of pain during treatment occurred particularly when applying formalin to the lower part of the rectum. The pain was located at the anal region. In one patient, completion of therapy required general anesthesia in one session. In all other patients, the pain was tolerable and subsided shortly after termination of the procedure. No signs of neoplastic lesions were detected.
Discussion
The results presented support the conclusions of previous studies; formalin treatment is highly effective with relatively few and mild complications. All our patients experienced a marked improvement in their disease with respect to both subjective symptoms and proctoscopic findings. Half of the patients completing follow-up were practically cured of their disease. The other half achieved a marked reduction in symptoms. Whether or not patients experiencing PR could have reached a CR with additional treatments is unclear. As shown above, PR denotes a marked improvement of symptoms in every case. The treatments were not continued until complete cessation of bleeding, but terminated after reaching a “satisfying result” was determined in the clinical setting, by the fact that only minor changes remained proctoscopically and from patient contentment, meaning the patients were fully satisfied with the relief achieved. Further treatments might have resulted in CR. The number of treatments needed to achieve this “satisfying result” varied somewhat (from n = 2 to n = 8). This might reflect the diverse severity of patients’ CRP, a varied response to treatment, a difference in the patient’s view on what constitutes such a result, or perhaps a combination of these. While our study reproduces the good results found by Haas et al. (1), both studies using 10% formalin, a final conclusion on whether 10% is more effective than 4% cannot be reached.
Pain was a frequent complaint during treatment sessions. It was mostly of a mild and transient character. One patient experienced severe pain while being treated. Another complained of pain for 1 day after one of her eight treatment sessions. The rest of the reported complications are more difficult to attribute to the formalin treatments. These are all known symptoms of CRP itself and did not occur in more than one patient each. Other patients actually experienced improvement or even cessation of these symptoms, as mentioned earlier. Regarding the effect of formalin on the rectum’s compliance and storage function, Myers et al. (22) conducted a study on canine subjects with formalin enemas and found no compromising effect thereof.
Our study has the drawback of being retrospective. The patients’ medical records are not written with a study in mind, and thus, they are not kept as methodically as would have been desirable. This problem is tackled by employing questionnaires and interviews as sources of information as well. This, however, introduces other problems such as recall-bias. Concerning the various follow-up periods, these seem of an appropriate length with respect to determining the effect of formalin. Complications arising from the treatment should also be detected, at least short-term ones. With regard to any possible long-term complications, the follow-up periods may seem too short. One suggested possible long-term complication of this treatment is secondary cancer. The concern was raised by Stern and Steinhagen (11) who reported two cases of second malignancy. They suggest the radiotherapy itself as a cause but are unable to completely exclude formalin as an etiological factor. No other reports including the present have detected any other cases of second malignancy. With a median follow-up period of 19 months, our study is, however, unable to rule out cancer as a result of the formalin.
In conclusion, we have demonstrated the effectiveness of formalin in the treatment of CRP, as in previous studies. The results are based on not only patient accounts but also objective assessment of the proctitis. All patients in the study showed a marked decrease in symptoms and proctoscopic signs of proctitis. The treatment is inexpensive, easy to carry out, requires limited preparation and equipment, can be performed on an outpatient basis, and is effective with little or no complications. Further studies are warranted to confirm the long-term effect of the formalin and to exclude possible complications, especially secondary anorectal cancer.