
Abstract
Aim:
The incidence of pancreaticobiliary maljunction is thought to approximate 1:100,000 within Western populations. We aimed to study the significance of pancreaticobiliary maljunction in biliary tract malignancies.
Methods:
Medical records and magnetic resonance cholangiopancreatography images of 252 consecutive patients treated for biliary malignancies during 2005–2016 were reviewed. Patients with other known risk factors for biliary cancers (n = 27) were excluded. A common pancreaticobiliary channel measuring ⩾10 mm outside the duodenal wall was defined as pancreaticobiliary maljunction.
Main Results:
Of the 225 patients, a reliably interpretable preoperative magnetic resonance cholangiopancreatography was available for 73 (32%). Sex (47% vs 57% females) and age at diagnosis (67 vs 66 years) were similar among patients with or without an magnetic resonance cholangiopancreatography (p = ns for both). In magnetic resonance cholangiopancreatography, a pancreaticobiliary maljunction with a median length of 20 mm (range 10–23 mm) was identified in four patients (5.5%, 95% confidence interval 1.6–14), while none had evident accompanying biliary tree dilatation. Pancreaticobiliary maljunction patients were significantly more often females (100% vs 43%, p = 0.043), less likely to have intrahepatic bile duct cancer (0% vs 65%, p = 0.019) while more likely to have gallbladder cancer (75% vs 22%, p = 0.044) compared to the others. Age at diagnosis (66 vs 67 years, p = 0.898), extrahepatic bile duct cancer incidence (25% vs 13%, p = 0.453), and survival status at last follow-up (50% vs 42% alive, p = 1.000) were comparable between the subgroups.
Conclusion:
The prevalence of pancreaticobiliary maljunction is substantially higher in adults with biliary malignancies than one would expect based on its incidence, reinforcing the etiologic role of pancreaticobiliary maljunction especially in females with gallbladder cancer.
Introduction
Biliary tract cancer, including malignancies of bile ducts and the gallbladder (1), is a rare but aggressive disease with a combined incidence varying from 1.8 to 7 per 100,000 in European populations (2, 3). Primary sclerosing cholangitis, inflammatory bowel diseases, and Lynch syndrome are among the ascertained risk factors for biliary tract cancers (4–6). Another factor thought to predispose to biliary malignancies is a pancreaticobiliary maljunction (PBM), defined as a premature confluence of the bile and the main pancreatic duct outside the duodenal wall and forming an abnormally long pancreaticobiliary common channel (7–11). By limiting the effect of the sphincter of Oddi, a PBM allows pancreatic juice to reflux into bile ducts, predisposing to obstructive cholestasis, lithiasis, chronic inflammation, as well as increasing the risk for malignant transformation of the biliary epithelium (10, 12).
Surveys among Asian populations have demonstrated that a PBM accompanied with bile duct dilatation predisposes to biliary tree malignancies, while an isolated PBM seems to associate particularly with gallbladder cancer (13–15). Accordingly, resection of the extrahepatic bile ducts and the gallbladder with a Roux-en-Y hepaticojejunostomy reconstruction is an established management for PBMs with associated bile duct dilatation, whereas no consensus exists on the optimal treatment of isolated PBMs without a dilated biliary tree (8). Surgery during childhood has been advocated by some authors even for asymptomatic PBMs, since biliary malignancies have occasionally been reported in children although most develop in the adult age (11, 13, 15).
So far, the majority of research on PBMs has been carried out in Asia, where their incidence is as high as 1 per 1000. In the Western world, reports on isolated PBMs are few and their exact incidence remains unknown, but it has been estimated to approximate 1:100,000 (16–18). The epidemiology of PBMs and their role in the development of biliary tree cancers in Western populations have not been studied systematically. The aim of this study was to analyze the association between PBM and biliary malignancies in a Caucasian patient sample.
Materials and Methods
Ethics
This study was approved by the Ethical Committee of Helsinki University Hospital.
Patients
This was a retrospective study including all patients treated for a biliary tract malignancy at Helsinki University Hospital between the years 2005–2016. The patient records were reviewed for relevant medical history, cancer characteristics, details of surgical treatment, survival and preoperative magnetic resonance cholangiopancreatography (MRCP) findings. Patients with known risk factors, such as primary sclerosing cholangitis, ulcerative colitis, Crohn’s disease, and Lynch syndrome, were excluded.
MRCP
First, two experienced radiologists individually assessed all available MRCP images using preset criteria. Then, the MRCP findings of the two radiologists were compared with each other, and if the individual findings differed, the images were reanalyzed until consensus was achieved. A common channel measuring ⩾10 mm outside the duodenal wall was defined as a PBM (Fig. 1).
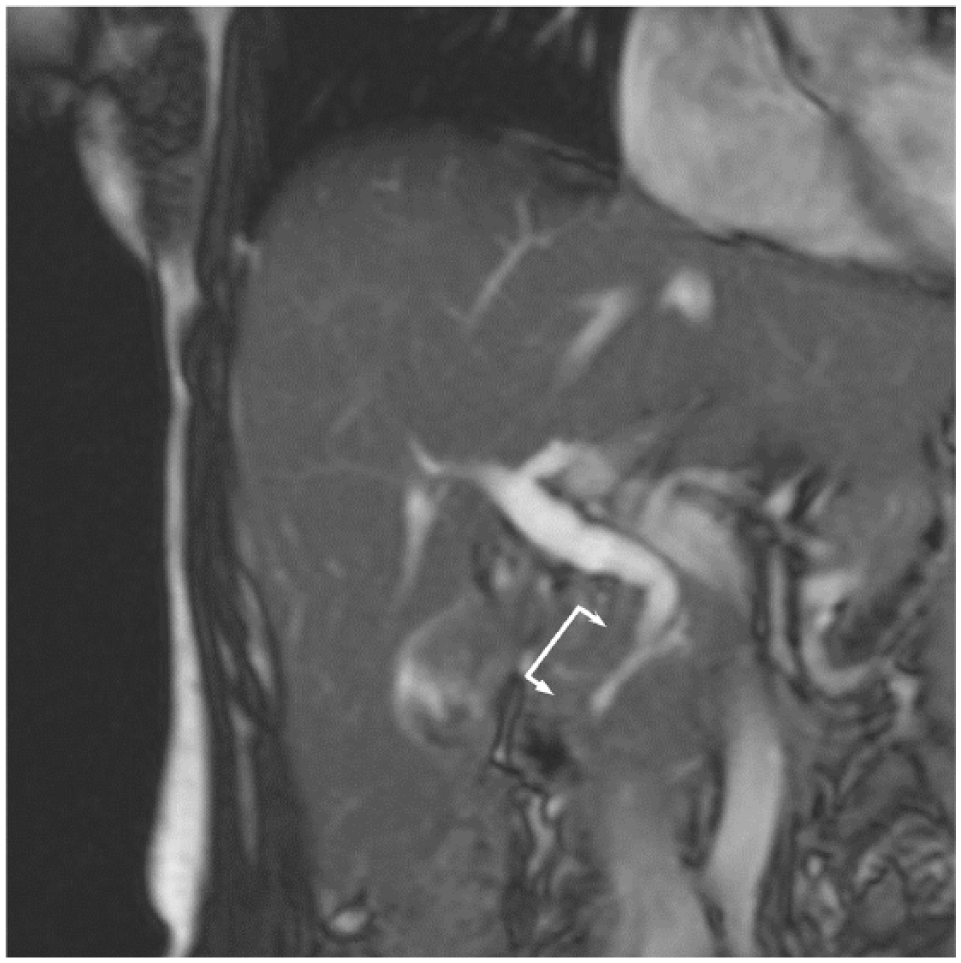
Magnetic resonance cholangiopancreatography findings of a patient with a pancreaticobiliary maljunction of 23 mm (pointed by arrows).
Statistical Methods
The data did not exhibit normal distribution. Continuous data are given as median with interquartile range (IQR) or percentages. Fisher exact test was used to compare categorical outcome variables between subgroups, and continuous variables were compared with the Mann–Whitney U test. 95% Confidence intervals (CIs) for PBM prevalence were defined with the Clopper–Pearson method. The level of significance was set at p < 0.05 and all analyses were performed with SPSS version 24.
Results
Patient Characteristics
Altogether 252 patients (females n = 130, 52%) with biliary tract malignancies treated in Helsinki University Hospital between 2005 and 2016 were identified. A flow chart of the study population is shown in Fig. 2. Other known risk factors for biliary malignancies were recognized in 27 patients (11%), who were excluded from further analyses. Of the remaining 225 patients, 91 (40%) had undergone a preoperative MRCP, and 73 of them (80%) were considered representative allowing reliable assessment for PBM with adequate imaging (Table 1). Overall, location of biliary cancer was intrahepatic in 62%, extrahepatic bile duct in 14%, and the gallbladder in 25%. Apart from a higher incidence of intrahepatic bile duct cancer and a lower incidence of gallbladder cancer among patients with an interpretable MRCP, baseline characteristics were comparable between the two subgroups (Table 1).
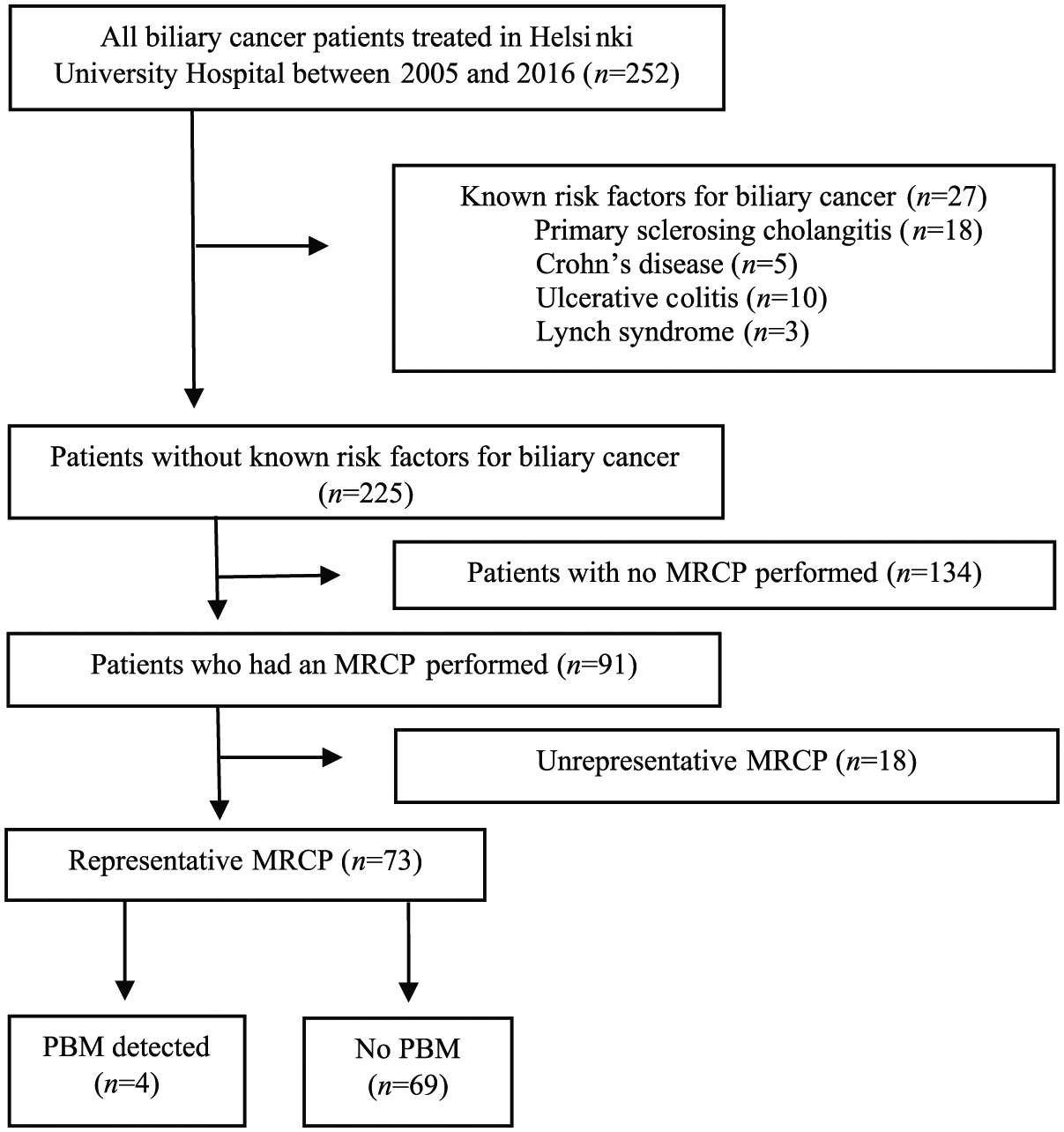
Selection of study patients.
Characteristics of all patients without known risk factors for biliary cancer.
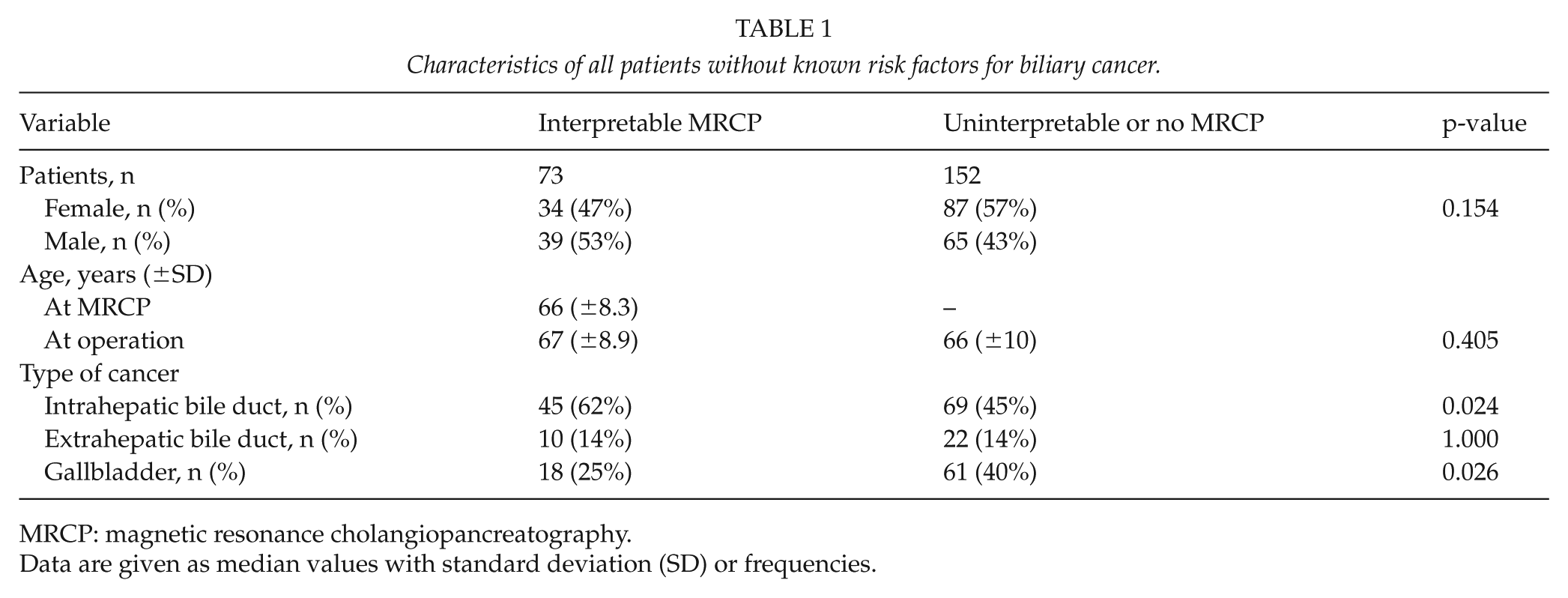
MRCP: magnetic resonance cholangiopancreatography.
Data are given as median values with standard deviation (SD) or frequencies.
PBM Prevalence and Related Characteristics
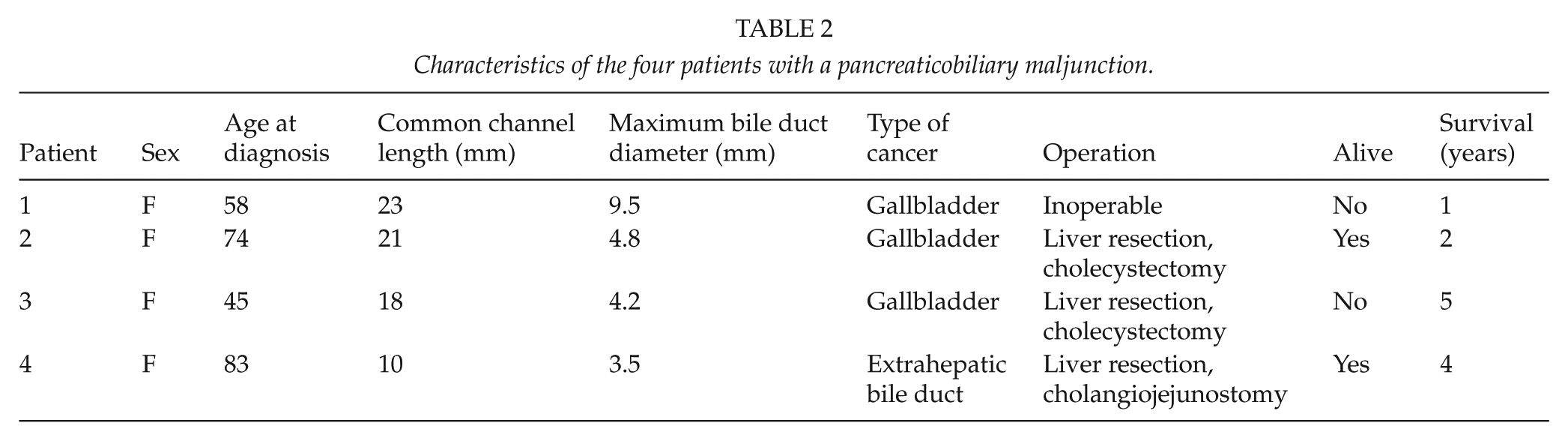
MRCP revealed a PBM in 4 out of the 73 patients (5.5%, 95% CI 1.6–14) with representative MRCP imaging (Table 2). Median length of the common channel was 20 mm (range 10–23 mm). None had distinct biliary tree dilatation, while the median maximum diameter of the extrahepatic bile duct was 4.5 mm (range 3.5–9.5 mm). All patients diagnosed with a PBM were females, and two of them ⩽58 years of age at diagnosis (Table 2). Three out of the four patients had gallbladder cancer whereas the fourth patient suffered from extrahepatic bile duct cancer. The estimated prevalence of PBM in gallbladder cancer was 17% (95% CI 3.6–41). Two patients are currently alive after 2 and 4 years postoperatively, while the other two died 1 and 5 years after the diagnosis (Table 2).
Characteristics of the four patients with a pancreaticobiliary maljunction.
Comparison of Patients with and without a PBM
Patients with a PBM were significantly more often females (100% vs 43%, p = 0.043) and were less likely to have intrahepatic bile duct cancer (0% vs 65%, p = 0.019) while they more likely presented with gallbladder cancer than others (75% vs 22%, p = 0.044) (Fig. 3). Age at diagnosis (66 vs 67 years, IQR 48.25–80.75 vs 61.5–72 years, p = 0.898), the incidence of extrahepatic bile duct cancer (25% vs 13%, p = 0.453), and survival status at last follow-up (2/4 vs 29/69 patients, p = 1.000) were comparable between patients with and without a PBM. Age at diagnosis was also similar when gallbladder cancer patients with or without a PBM were compared (58 vs 65 years, IQR 45–74 vs 59–76 years, p = 0.301). Three out of the four patients (75%) with a PBM had an operable malignancy compared to 36 out of 69 (52%) patients without a PBM (p = 0.618).
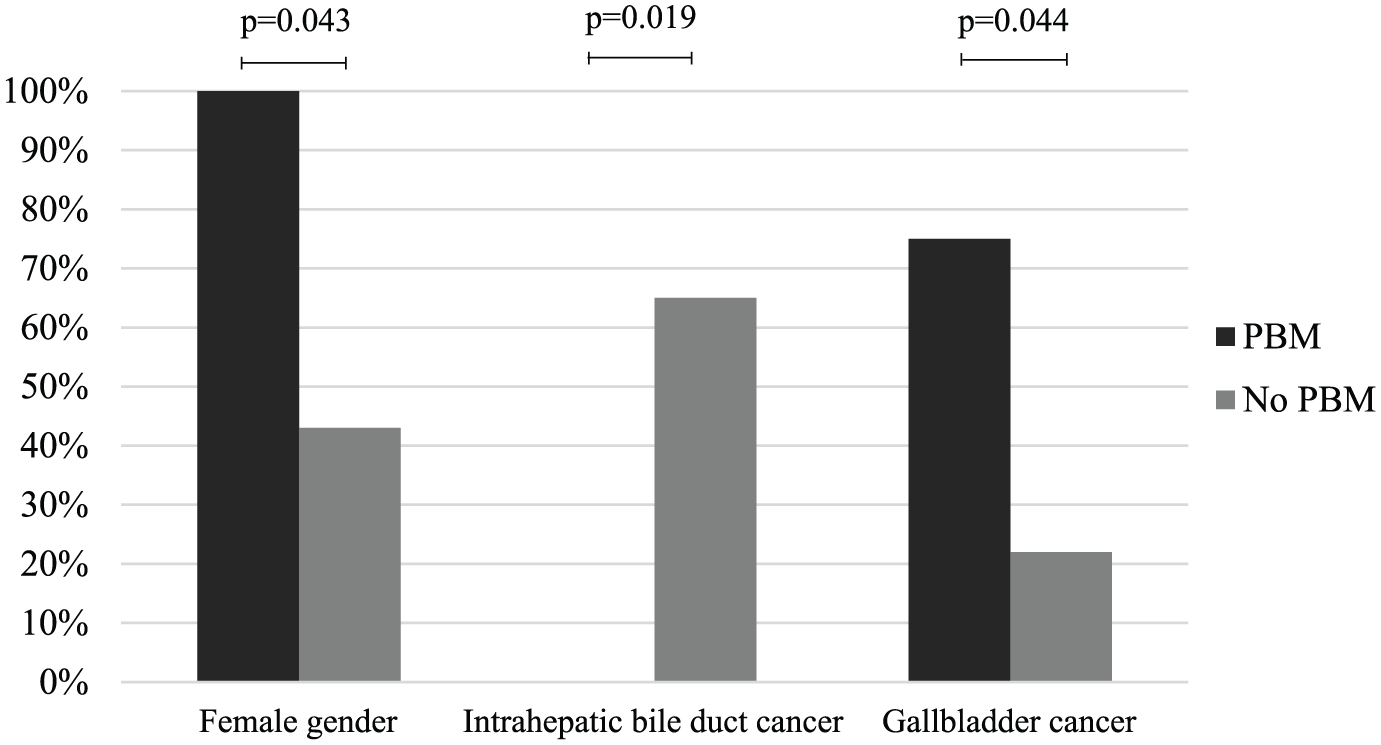
Comparison of patients with and without a pancreaticobiliary maljunction (PBM).
Discussion
This is one of the first studies evaluating the role of PBM as a risk factor for biliary tract malignancies in a Caucasian population. A PBM without a distinctly dilated biliary tree was identified in 5.5% of patients with biliary malignancies, clearly exceeding the previous PBM incidence estimates in the Western world and supporting the concept that PBM is a premalignant condition. Compared to other patients with biliary cancer, those with a PBM developed gallbladder cancer more often and were more frequently female, suggesting similar PBM pathogenesis and sex distribution than previously reported in Asian populations.
The chronic inflammation caused by constant reflux of pancreatic juice into the bile ducts has been thought to be responsible for the malignant transformation occurring in the biliary epithelium of PBM patients (10, 12). Large Asian surveys have shown that a PBM without dilatation of proximal bile ducts associates mainly with gallbladder cancer (13–15) and our results are the first to confirm that a similar risk for malignancy exists in patients with an isolated PBM also in a Western population. Considering the combined incidence of gallbladder cancer and extrahepatic bile duct cancer in Finland (4.04–5.46 per 100,000) (3) as well as the estimated PBM incidence of 1:100,000, PBM prevalence among patients with biliary malignancies should, consequently, be below 1% if these conditions were unrelated to each other. Instead, we found the prevalence of PBM as high as 5.5% and 17% in adults with biliary malignancies and gallbladder cancer, respectively. Compared to the general population, patients with a PBM have been reported to develop gallbladder cancer at younger age (7, 19). In our study, patients with a PBM developed gallbladder cancer 7 years earlier compared to the patients who did not have a PBM; however, possibly due to small sample size, this difference was not statistically significant. All of our patients with a PBM were female, which is in line with previous reports showing that women with PBMs develop gallbladder cancer more frequently than men with a PBM (7).
The established treatment of PBMs combined with choledochal cyst is resection of the extrahepatic bile ducts including the gallbladder with a Roux-en-Y hepaticojejunostomy reconstruction. There is no unanimity when it comes to the treatment of PBMs without clear dilatation or the lower limit of pathological pancreaticobiliary common channel length (20). The high proportion of gallbladder cancers associated with undilated PBMs supports a prophylactic laparoscopic cholecystectomy, which is associated with a low risk of significant operative complications (21). Development of biliary cancer has not been noted in long-term follow-ups among patients who have undergone a prophylactic cholecystectomy for isolated PBMs (21, 22). However, because the K-ras and tumor suppressor gene mutations identified even in the noncancerous biliary epithelium of patients with isolated PBMs suggest an increased risk for bile duct cancer as well (8, 11), some authors recommend a hepaticojejunostomy, which carries a much higher risk for significant postoperative complications (11, 23). If a cholecystectomy is solely performed, a careful long-term follow-up is likely necessary to catch the development of possible biliary tree malignancies early on (24).
The incidence of PBMs in Western populations has been thought to approximate 1:100,000; however, no current evidence on its true epidemiology exists. In a nationwide Japanese survey, 42% of patients with untreated isolated PBMs developed biliary malignancies (13). Although the small number of patients in the present study prevents a reliable estimation of PBM incidence, but by supposing the rate for developing malignancies would be similar among Western and Asian PBM patients, and by taking into account the incidence of biliary tract cancers in Finland (3), the overall incidence of isolated PBMs in Finland should approximate 0.6:100,000. However, larger population-based studies are needed to reliably assess the epidemiology of PBMs in the Western world. Considering that the incidence of choledochal malformations appears to be rising (25), the incidence of PBMs may differ from estimates made decades ago. Since we had a significantly higher proportion of gallbladder cancer patients without representative MRCP available, and we only included patients with a clear pancreaticobiliary common channel ⩾10 mm, it is possible that the true incidence of PBM among cancer patients could be even higher than now observed.
This study had several limitations. Less than half of the patients with biliary malignancies underwent an MRCP prior to treatment and after excluding patients with inadequate MRCP images, only a third of the initial patients could be included in the study. Accordingly, our sample size was too small to evaluate the incidence of PBM reliably and we cannot exclude the possibility that the higher proportion of gallbladder cancer among patients not undergoing MRCP and our strict definition of common channel had underestimated the true incidence of PBM. Nonetheless, this is the first study conducted on this matter in a Western country and provides important information about PBMs as a risk factor for biliary malignancies.
In conclusion, an isolated PBM identified in 5.5% of Caucasian patients with biliary malignancies associated particularly with female gender and gallbladder cancer, suggesting similar PBM behavior than previously reported in Asian studies. Further research in larger patient samples is needed to define the optimal treatment and follow-up of PBM without a bile duct cyst, as well as to characterize the current epidemiology of PBMs in the Western world.
Footnotes
Acknowledgements
The authors want to acknowledge contributions from Dr Heikki Mäkisalo and Dr Antti Koivusalo.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Sigrid Jusélius Foundation, the Finnish Pediatric Research Foundation, and the Helsinki University Central Hospital.