
Abstract
Background:
The aim was to compare survival for incidental gallbladder cancer (IGBC), respectively, preoperatively suspected gallbladder cancer (GBC), subjected to surgery for different pathological tumour (pT) stages and in different treatment groups in a national cohort.
Methods:
Data were collected and crosslinked from two national quality registers, SweLiv (2009–2019) and GallRiks (2009–2016). Survival was estimated using Kaplan–Meier analysis. The log-rank test and Cox regression analyses were used to compare groups.
Results:
In total, 466 IGBC patients, including 225 who only underwent simple cholecystectomy (SC), and 477 GBC patients were included. Most patients were female, with small differences in mean age between groups. In all IGBC patients compared with GBC patients, an improved 5-year overall survival in pT3 GBC undergoing surgery (GBC 13% vs all IGBC 8%, p < 0.001), was seen. GBC was shown to be an independent predictor for improved survival in pT3 patients (hazard ratio (HR): 0.6; 95% confidence interval (CI): 0.4–0.8, p < 0.001). In addition, in GBC with curative reresection compared with IGBC SC and IGBC with curative resection, an improved 5-year overall survival in pT3 GBC was shown (GBC 20% vs all IGBC 10%, p < 0.001). GBC was an independent predictor for improved survival in pT3 patients with curative resection (HR: 0.4; 95% CI: 0.3–0.7, p < 0.001).
Conclusions:
GBC was shown to be an independent predictor for improved survival in pT3 patients, and patients with GBC may benefit from one-stage resection. It is, therefore, reasonable to recommend that radiological suspicion of malignancy should be evaluated at a liver tumour centre to optimize patient outcomes.
Keywords
Introduction
With early involvement of the surrounding structures, due to the anatomical location and rapid growth through thin layers of the gallbladder, gallbladder cancer (GBC) remains a disease with poor prognosis. 1 Surgical treatment is still the only potentially curative treatment option. 2 Currently, the surgical management of GBC is dependent on the tumour (T)-stage. There is consensus that simple cholecystectomy (SC) is sufficient to treat T1a cancers. 3 The typical surgical strategy in T1b, T2 and T3 disease is liver resection of segment IVB/V, with wedge resection or segmentectomy and lymphadenectomy of regional nodes, including cystic pericholdochal, perihepatic and periportal lymph nodes, and in more advanced tumours, extraregional lymph node resection, including the aortocaval nodes.4,5 Sometimes, more extensive liver and extrahepatic bile duct resections are performed to achieve R0 resection. 6
Internationally, approximately 70% of GBCs are discovered incidentally. These studies are often based on patients planned for reresection who are already referred to a liver tumour centre.3,7 However, data from the Swedish Registry for Cancer in the liver, gallbladder and biliary tract, SweLiv, which includes all categories of GBC patients, indicated that the distribution of incidental versus preoperatively suspected GBC is different. 8 Previous studies have shown that patients with incidental gallbladder cancer (IGBC) on pT-stadium-specific analysis have significantly better survival than GBC patients in certain stages.9,10 However, these studies are based on IGBC patients selected for liver resection and lymphadenectomy after index cholecystectomy. IGBC patients who were not planned for further surgery were excluded from these analyses. An analysis of the patients we intend to treat would be more suitable to address whether there are differences in overall survival between all IGBC patients compared with GBC patients undergoing surgery. With the ability to identify all IGBC and GBC patients in a national cohort, this question can now be addressed using the national registries.
The primary aim of this study was to analyse overall survival, divided into different tumour stages, for all IGBC patients who either underwent cholecystectomy as the only procedure or were subjected to further surgery as one group compared with preoperatively suspected GBC patients who underwent surgery. Both unresectable patients and patients undergoing tumour resection were included. The same comparison was also made with the IGBC SC group excluded.
The secondary aim was to again compare overall survival as in the primary aim, except only including patients undergoing curative reresection/resection.
Methods
All data regarding IGBC and GBC patients from the National Quality Registry for Liver, Bile Duct and Gallbladder Cancer, SweLiv, between January 2009 and December 2019 were collected in March 2020 and crosslinked with the Swedish Registry for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography, GallRiks, between 2009 and 2016 to ensure inclusion of all IGBC patients during this time. The GallRiks data were available for this period from our previous study. 11 The SweLiv registry consists of different chronological forms, including information on registration, tumour intervention, complications, histopathological diagnosis and follow-up. All patients ⩾16 years of age with primary tumours in the liver, gallbladder or bile ducts are registered in SweLiv. Patients with radiologically suspected GBC who were not planned for surgical intervention were registered, as well as patients with histopathologically proven GBC. The American Joint Committee on Cancer, AJCC, TNM staging system is used in SweLiv, and different classifications have been used during the years; version 6 12 was used until 1 January 2011, then version 7, 13 followed by version 8 14 from 1 January 2019. TNM was initially defined during a multidisciplinary team (MDT) meeting based on radiological findings and definitively as pTNM after histopathological examination if surgery was performed. For IGBC patients, the pT-stadium based on the cholecystectomy specimen is registered. The completeness concerning GBC was 97% in SweLiv in 2020 compared with the Swedish Cancer Registry. The registry was last validated in 2014, and the registered data were compared with source data in medical records at all Hepato-pancreato-biliary centres in Sweden. Each year, national reports with open access are published online. 8 The survival status of the patients entered into the registry is updated continuously by linkage to the Swedish national population register.
Definitions
In the present study, according to the AJCC 6th edition, lymph nodes along the common bile duct, cystic duct, hepatic artery and portal vein were defined as regional lymph nodes, and lymph nodes along the coeliac trunk, superior mesenteric artery, renal artery, mediastinum, periduodenal, peripancreatic and pericardial were defined as metastases. GBC diagnosed en passant during surgery for benign gallbladder disease and/or on histopathological examination was defined as IGBC. R0 resection includes complete resection with a microscopically negative margin. R1 resection was defined as a macroscopically negative resection margin, but a positive microscopic resection margin. R2 resection was defined as a macroscopically positive resection margin. 15 All patients were controlled for surgical procedures, and patients undergoing cholecystectomies in the same session as a liver resection were classified as GBC. The Clavien‒Dindo classification was used to illustrate the severity of surgical complications. 16
Exclusion and inclusion criteria
Patients with cholecystectomy performed as part of another procedure, such as liver transplantation, were excluded; patients were also excluded when the registration was inconclusive concerning the primary diagnosis. In addition, seven IGBC patients registered in GallRiks and not registered in SweLiv were included. pTNM was controlled from patients’ records if the diagnosis was unclear for IGBC patients registered in GallRiks between 2009 and 2016. The studied period was split into two equal time intervals, from January 2009 until June 2014 and from July 2014 until December 2019, to evaluate changes over time concerning MDT meetings. Patients diagnosed with pT1b, pT2 and pT3 were included in the overall survival analysis. Patients proven to be unresectable during surgery (or during the second operation for IGBC patients) only underwent explorative laparotomies due to disseminated disease. Patients who died within 30 days of surgery (n = 10) were excluded from all overall survival analyses.
Overall survival analysis 1
Overall survival analysis including IGBC SC and IGBC patients undergoing a second operation versus GBC patients undergoing surgery was performed. For both groups, patients proven to be unresectable during surgery and patients undergoing resection/reresection were included. Thus, patients with R2 resection/reresection and preoperatively discovered metastases (for IGBC patients during the second operation) were included.
Overall survival analysis 2
Overall survival analysis including only IGBC patients undergoing a second operation versus GBC patients undergoing surgery was performed, and the same inclusion criteria were used as in overall survival analysis 1.
Overall survival analysis 3
Overall survival analysis in IGBC SC patients and IGBC patients with curative reresection as one group compared with GBC patients with curative resection was performed. Patients with R2 resection/reresection and patients with preoperatively discovered metastases (for IGBC patients during the second operation) were excluded from these analyses.
Overall survival analysis 4
The same overall survival analysis, as in analysis 3, concerning curative reresection/resection, was performed with the IGBC SC group excluded.
Statistics
Baseline demographics between groups were compared using one-way analysis of variance (ANOVA) for continuous variables, and these data are presented as the means (sd). χ2 tests were used for categorical variables, and these are presented as the numbers with percentages. The Kaplan‒Meier analysis was used to estimate survival, and the log-rank test was used to compare differences between the groups. Survival was evaluated as overall survival and was measured from the date of diagnosis to the date of death or last follow-up. Patients who died within 30 days of surgery were excluded from the survival analysis. Univariable and multivariable Cox regression analyses were performed to calculate the adjusted hazard ratio (HR). p < 0.05 was considered significant. Statistical analyses were performed using IBM SPSS Statistics 26 Windows (IBM Corporation, Armonk, NY, USA).
Ethics
Ethics were approved by the Regional Ethical Committee in Lund (2014/39-31, 2016/408-32).
Results
In total, 1986 patients were registered in SweLiv with radiologically suspected or histopathologically proven GBC between January 2009 and December 2019. Thirty-five patients were excluded due to incidental findings of GBC during liver transplantation or due to unclear diagnosis. A majority (76%) had preoperatively suspected GBC, with 1485 patients compared with 466 (24%) for IGBC (Figure 1).
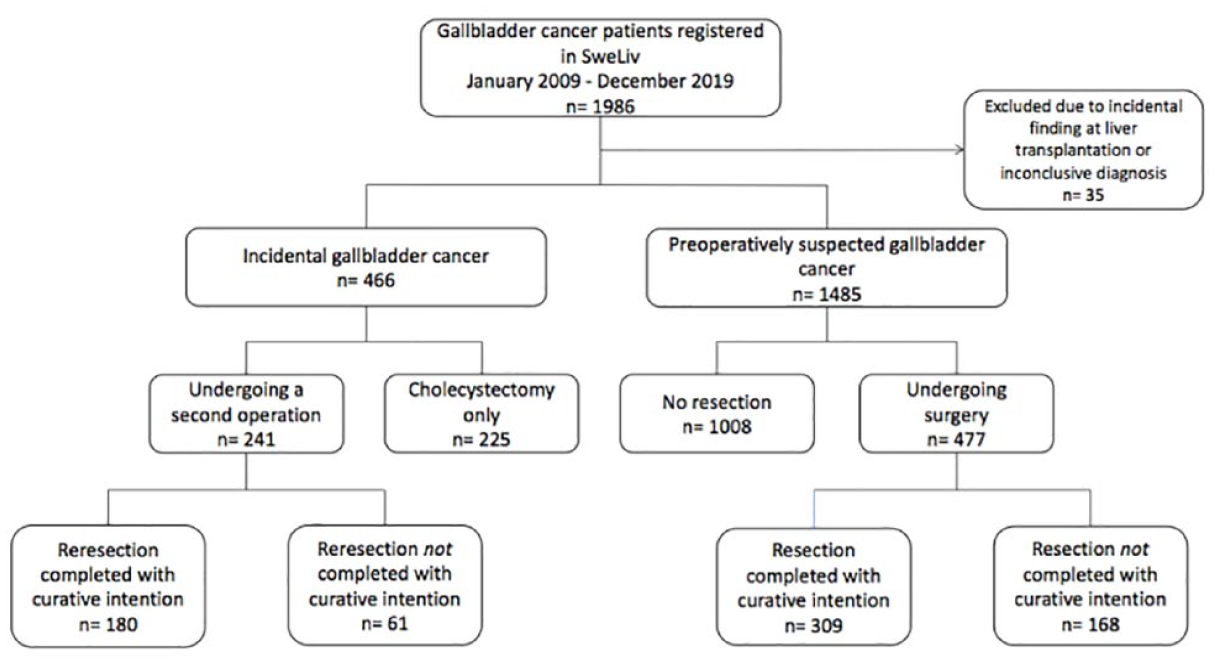
Flow chart, patients with gallbladder cancer registered in SweLiv during 2009–2019.
Almost half of the IGBC patients underwent SC (n = 225), 241 IGBC patients underwent a second operation and 477 GBC patients underwent surgery. The patient characteristics are presented in Table 1. Most patients were female (IGBC SC 73%, IGBC 72% and GBC 64%, p = 0.017), and there were small differences in mean age between all three groups (71 years vs 67 years vs 68 years, p < 0.001). Most patients were discussed at MDT meetings; however, 20% of IGBC patients with SC were not discussed compared with 15% of IGBC patients undergoing a second operation and 12% of GBC patients undergoing surgery (p = 0.018). MDT meetings were more frequently applied in the later period in all three groups (p < 0.001, Table 1).
Characteristics in IGBC patients with SC, IGBC patients undergoing a second operation and GBC patients undergoing surgery.
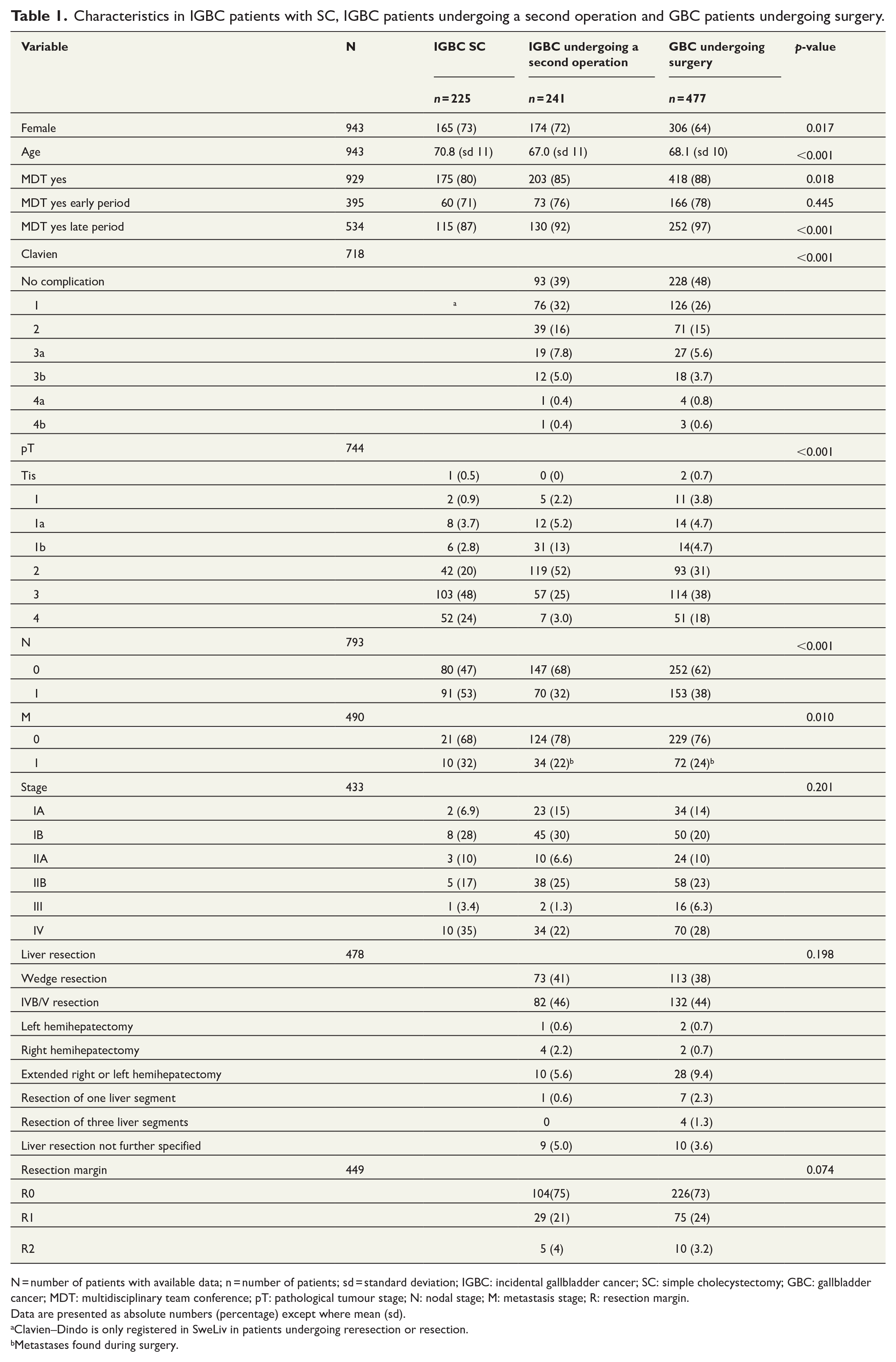
N = number of patients with available data; n = number of patients; sd = standard deviation; IGBC: incidental gallbladder cancer; SC: simple cholecystectomy; GBC: gallbladder cancer; MDT: multidisciplinary team conference; pT: pathological tumour stage; N: nodal stage; M: metastasis stage; R: resection margin.
Data are presented as absolute numbers (percentage) except where mean (sd).
Clavien–Dindo is only registered in SweLiv in patients undergoing reresection or resection.
Metastases found during surgery.
Information regarding pT was available in 774 patients of 943 undergoing either SC (IGBC, missing n = 11), second operation (IGBC, missing n = 10) or surgery (GBC, missing n = 178). In IGBC patients undergoing a second operation, the pT2 category was the most common (n = 119, 52%), followed by pT3 (n = 57, 25%) and pT1b (n = 31, 13%). In GBC undergoing surgery and in IGBC SC, the pT3 group was the most common (n = 114, 38% and n = 103, 48%, respectively; Table 1). Most patients were proven to be N0 in IGBC undergoing a second operation group (n = 147, 68%) and in GBC undergoing surgery group (n = 252, 62%), with the highest amount of N1 in the IGBC SC group (n = 91, 53%). Most patients in all three groups were M0. The Clavien–Dindo classification and TNM stages according to AJCC 6th edition was distributed as shown in Table 1. IVb/V segmentectomy with lymphadenectomy was the most common procedure, both in reresected IGBC and resected GBC patients, and the second most common procedure was wedge resection with lymphadenectomy. The majority of IGBC/GBC patients who underwent reresection/resection had a radical (R0) procedure according to histopathological diagnosis; 15 patients had an R2 resection, and 106 patients were presented with preoperatively found metastases (Table 1).
Overall survival analysis 1 – IGBC SC and IGBC patients undergoing a second operation compared with GBC patients undergoing surgery
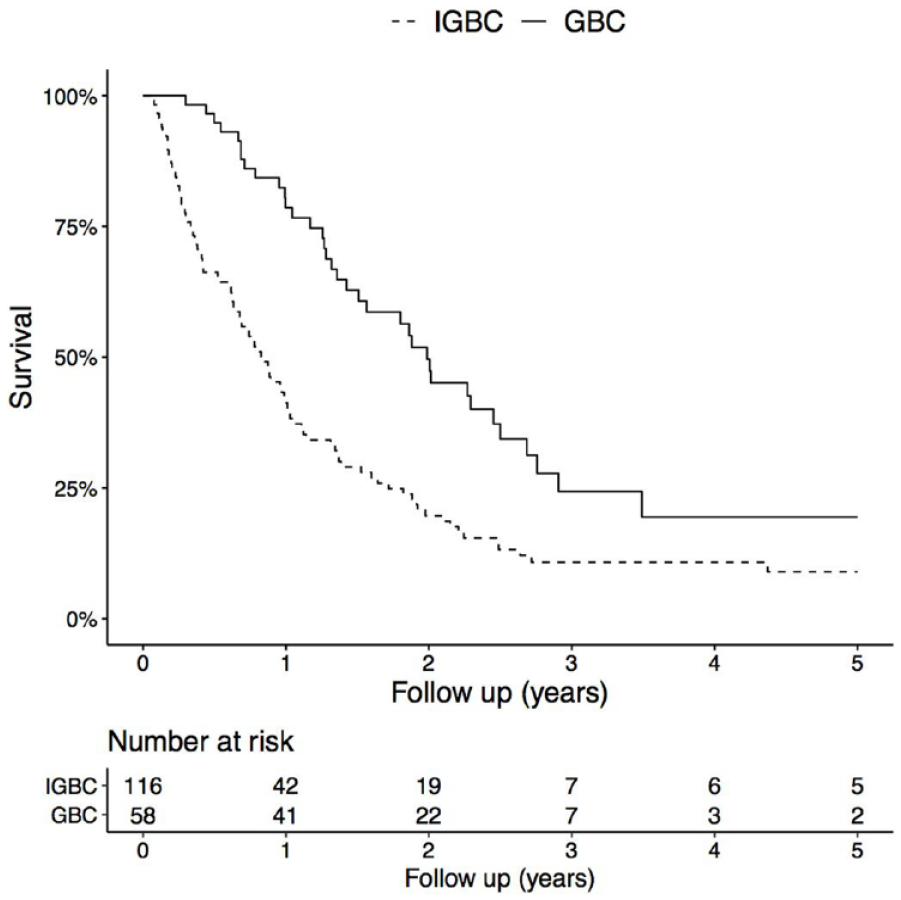
The overall survival in all IGBC patients compared with GBC patients undergoing surgery showed no difference in overall survival in pT1b patients (5-year overall survival 65% in IGBC and 79% in GBC, p = 0.383). In pT2 patients, a tendency toward improved 5-year overall survival in GBC patients was observed (GBC 45% vs all IGBC 40%, p = 0.112) (Figure 2). In pT2 patients, N1 status was shown to impair overall survival on multivariable analysis (HR: 2.0; 95% confidence interval (CI): 1.4–2.9, p < 0.001). In pT3 patients, a significant difference in 5-year overall survival was observed, with improved survival in the GBC group (GBC 13% vs all IGBC 8%, p < 0.001) (Figure 3). GBC was shown to be an independent predictor of improved survival in pT3 patients, adjusted for sex, age and N-status (HR: 0.6; 95% CI: 0.4–0.8, p < 0.001; Table 2).
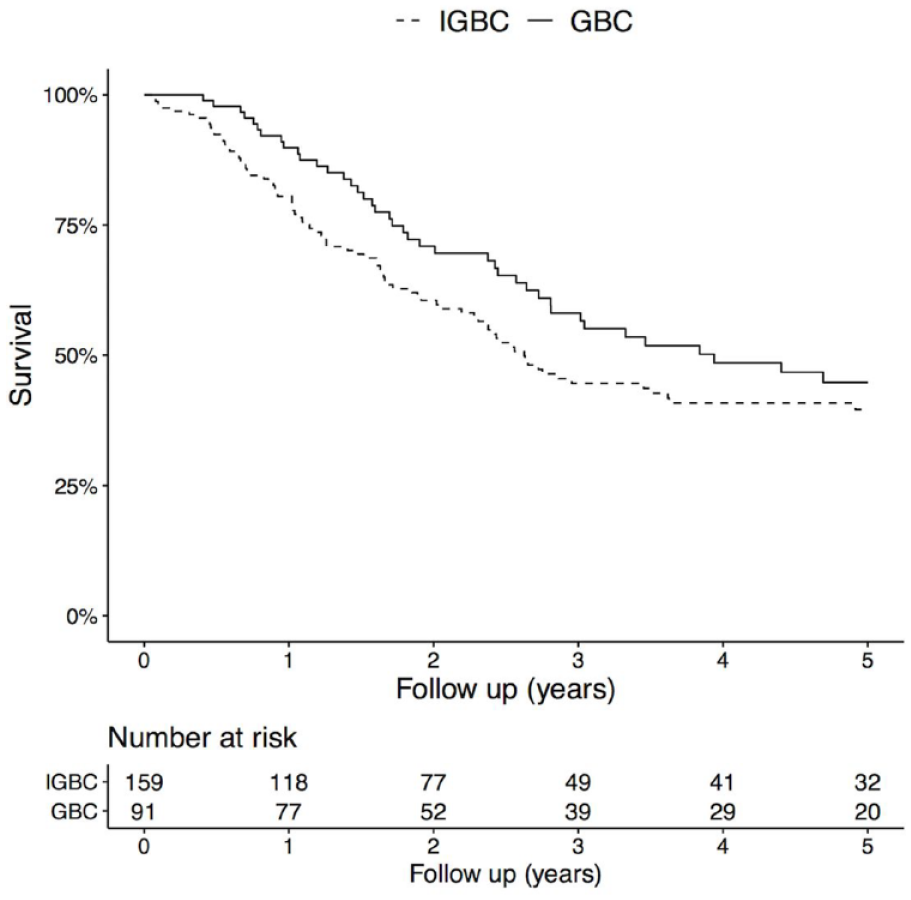
Overall survival in IGBC SC and IGBC patients undergoing a second operation compared with GBC patients undergoing surgery, pT2. p = 0.112 (log-rank test).
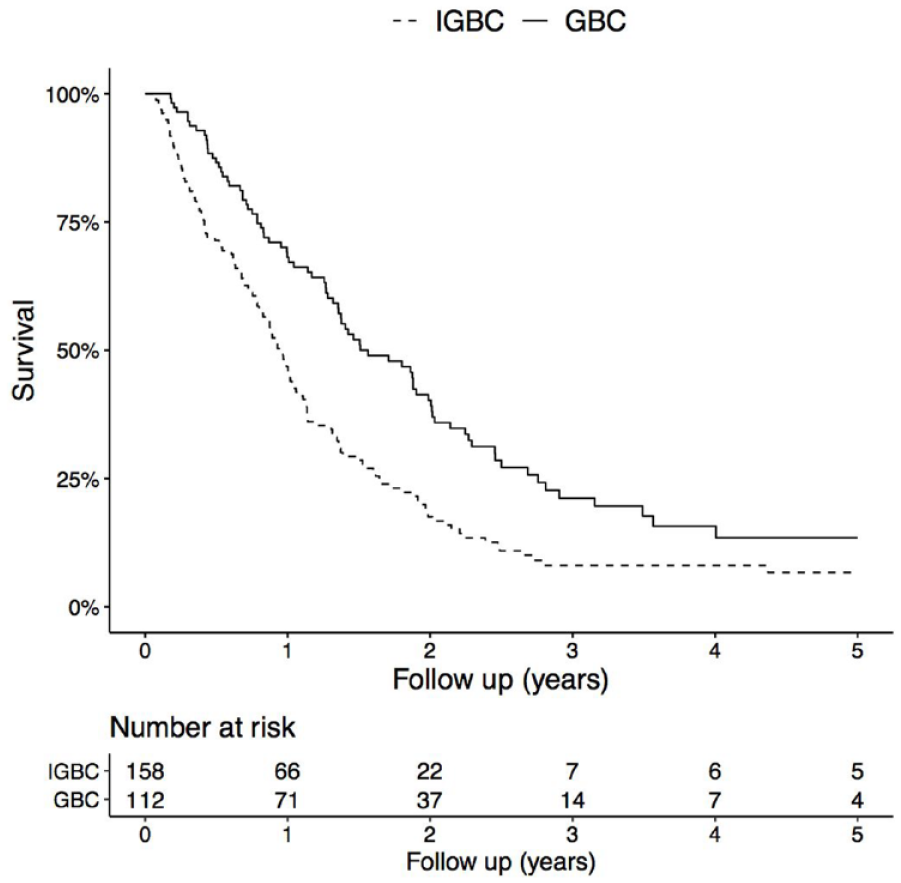
Overall survival in IGBC SC and IGBC patients undergoing a second operation compared with GBC patients undergoing surgery, pT3. p < 0.001 (log-rank test).
Univariable and multivariable analysis in IGBC SC patients and in GBC patients undergoing a second operation compared with GBC patients undergoing surgery (a), and in IGBC SC and IGBC patients with curative reresection compared with GBC patients with curative resection (b), pT3.
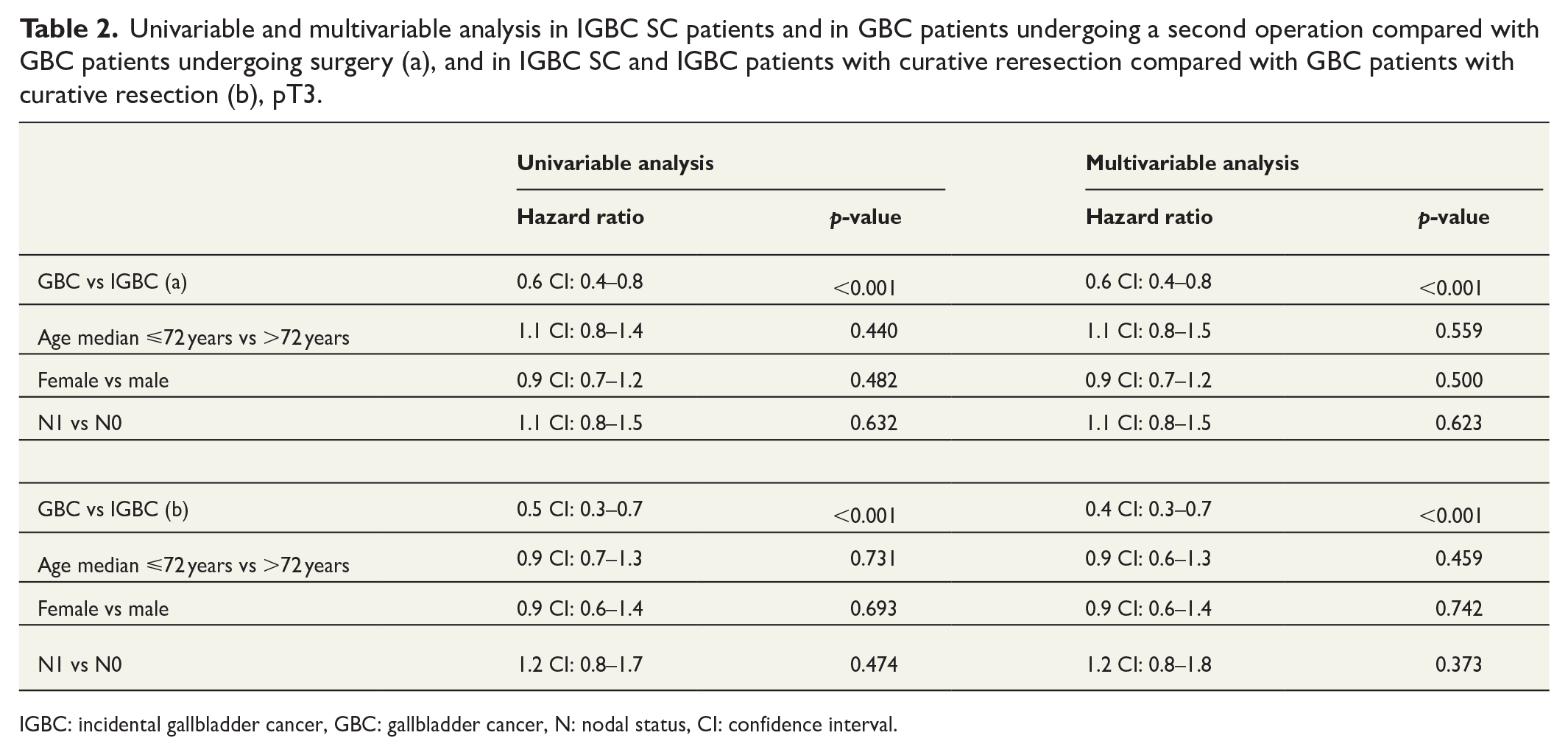
IGBC: incidental gallbladder cancer, GBC: gallbladder cancer, N: nodal status, CI: confidence interval.
Overall survival analysis 2 – IGBC patients undergoing a second operation compared with GBC patients undergoing surgery
No significant difference was shown in overall survival on pT-stage specific analysis (pT1b, pT2 and pT3) in IGBC patients undergoing a second operation compared with GBC patients undergoing surgery. The 5-year overall survival was 79% in pT1b GBC and 76% in IGBC (p = 0.581). In pT2 GBC and IGBC patients, the 5-year overall survival was 45% in both groups (p = 0.456). In pT3 patients, the 5-year overall survival was 13% in the GBC group versus 19% in the IGBC group (p = 0.665). On univariable and multivariable analysis, no difference in survival was seen in pT1b or pT3 concerning sex, age and N-status. In pT2 patients, N1 status was shown to impair survival (HR: 1.7; 95% CI: 1.1–2.5, p = 0.017).
Overall survival analysis 3 – IGBC SC and IGBC patients with curative reresection compared with GBC patients with curative resection
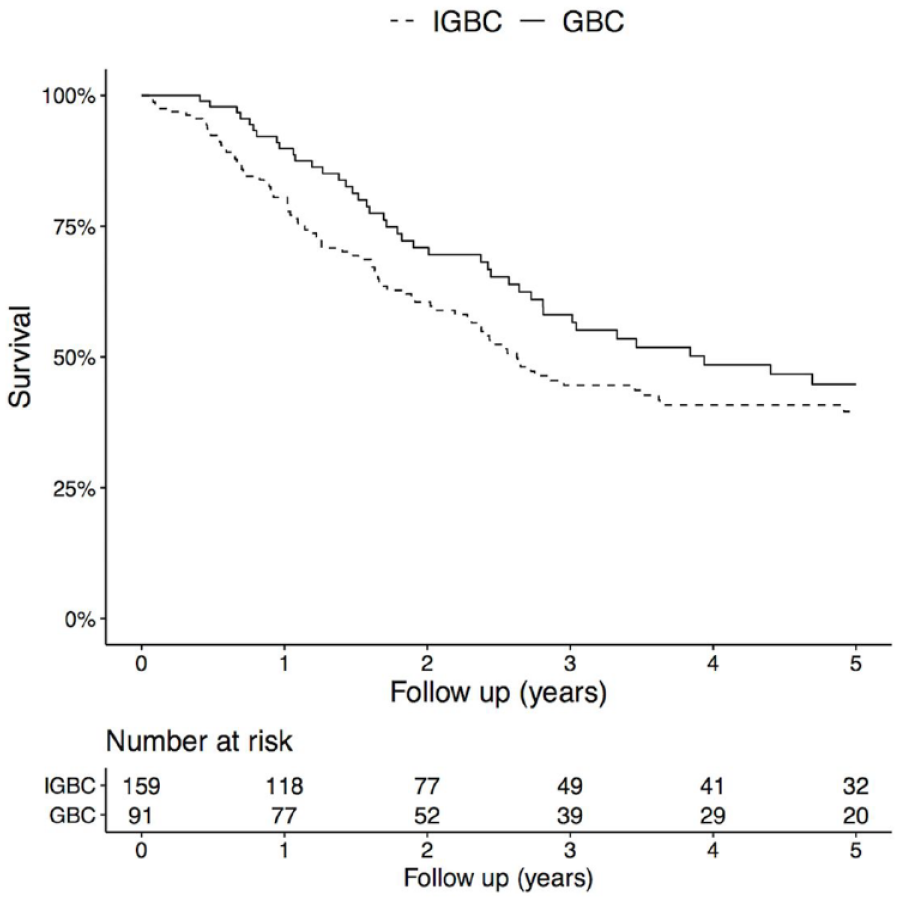
In the pT1b category, no difference was seen in overall survival in all IGBC patients (SC and curative reresection) compared with GBC patients with curative resection (70% vs 87% p = 0.275), and sex, age and N-status did not significantly affect survival. In pT2 GBC patients, a tendency toward improved overall survival was seen (50% 5-year overall survival) with curative resection compared with IGBC SC and IGBC patients with curative reresection (42% 5-year overall survival) (p = 0.051), and N1 status impaired survival (HR: 2.0; 95% CI: 1.3–3.1, p < 0.001). Improved 5-year overall survival was observed in pT3 GBC patients with curative resection compared with IGBC SC and IGBC patients with curative reresection (20% vs 10% p < 0.001) (Figure 4). GBC was shown to be an independent predictor of improved survival in pT3 patients, adjusted for sex, age and N-status (HR: 0.4; 95% CI: 0.3–0.7, p < 0.001; Table 2).
Overall survival in IGBC SC and IGBC patients with curative reresection compared with GBC patients with curative resection, pT3, p < 0.001 (log-rank test).
Overall survival analysis 4 – IGBC patients with curative reresection compared with GBC patients with curative resection
Overall survival in IGBC patients with curative reresection compared with GBC patients with curative resection according to pT-stage showed no significant difference in overall survival in pT1b (5-year overall survival IGBC: 80% GBC: 87%, p = 0.748) or pT2 (5-year overall survival IGBC: 50% GBC: 50%, p = 0.896) patients. In pT3 patients, a significant difference in overall survival was seen, with a 5-year overall survival of 50% in IGBC patients compared with 20% in GBC patients (p = 0.023, Figure 5). IGBC was proven to be an independent predictor of improved survival in pT3 patients undergoing curative reresection, adjusted for sex, age and N-status (HR: 0.4; 95% CI: 0.2–0.8, p < 0.019).
Overall survival in IGBC patients with curative reresection compared with GBC patients with curative resection, pT3. p = 0.023 (log-rank test).
Discussion
To our knowledge, this is the first study to include a full national cohort of patients with incidental and preoperatively suspected GBC. Our results showed an improved overall survival in patients with GBC compared with patients with IGBC in pT3 and a tendency toward improved overall survival in pT2. Because of the rarity of the disease, 17 studies investigating survival in this patient category are often limited to small cohorts.18,19 We managed to include a large number of patients due to two well-established registries in Sweden: SweLiv and GallRiks.
In all pT3 GBC patients undergoing surgery, an independent improvement in 5-year overall survival was observed compared with all IGBC SC and IGBC patients undergoing a second operation, including both resected and unresectable patients. The same finding was registered for pT3 GBC patients undergoing curative resection compared with IGBC SC and IGBC patients undergoing curative reresection. This may indicate that pT3 patients benefit from one-stage resection. These findings are contradictory compared with previous studies. Ethun et al. 10 showed an improved independent overall survival in IGBC patients undergoing radical (R0, R1) reresection compared with radically resected GBC patients in Stage III, 28.6 versus 11.6 months (p < 0.001). IGBC SC patients were not included, and the GBC cohort was smaller than that in the present study. This finding is in line with our results concerning curative reresection in pT3 IGBC patients compared with GBC patients. No other recent studies have investigated the difference in survival in IGBC and GBC patients, and previous studies were limited by small cohorts 20 and by non-pT- or stage-specific survival analysis.21 –23
The large difference in 5-year overall survival in pT3 IGBC with curative reresection compared with GBC with curative resection may show that curatively reresected pT3 IGBC patients are an extremely select group, since they qualified for surgery despite the time interval from index cholecystectomy.
Most patients, including all stages, presented with GBC (76%); this result contrasts with previous studies where IGBC was described as far more common. However, these studies were often based on data from liver centres, where patients are referred when reresection is already planned. 24 The IGBC incidence was lower (20%–50%) in studies based on data from hospitals performing cholecystectomies for benign indication.25 –27
More patients were discussed at MDT meetings in the later period in all three groups. However, for both time periods, IGBC SC patients were less discussed than IGBC patients undergoing a second operation and GBC patients undergoing surgery. These IGBC SC patients were not evaluated properly concerning reresection and may not have been selected for surgery for this reason. In the IGBC SC group, most patients were diagnosed with pT3 and did not undergo further resection. These results are in line with our previous study, 11 in which more IGBC pT2 patients were selected for reresection than pT3 patients. The reasons for not proceeding with surgery in the present study in the IGBC SC patients were not studied, but these patients were likely disqualified for surgery because of disseminated disease at re-evaluation, indicating that pT3 patients benefit from one-stage resection. In our previous study, 11 including patients with IGBC between 2007 and 2016, the most common reasons for not performing reresection in pT2 disease were that the index cholecystectomy was considered a radical procedure and comorbidity. In pT3 disease, the most common reasons were advanced tumour stage and patient comorbidity.
In Sweden, wedge resection and lymphadenectomy are recommended for pT1b–pT3 GBC patients. 28 Most patients in our study underwent IVb/V segmentectomy, followed by wedge resection. When investigating the extent of liver resection in pT2 GBC, no advantage has been seen of anatomical hepatectomy of segments IVb and V over wedge resection.29,30 Xu et al. 31 concluded that liver resection is not mandatory for pT1b upon analysis of data from the Surveillance, Epidemiology and End Results (SEER) database. These results are in line with Yuza et al., 32 who found no difference in 10-year overall survival between patients with SC and patients with extended surgery. Nevertheless, recent studies agree31,33,34 that regional lymphadenectomy in pT1b should be performed. The lymph node metastasis rate has been described to be as high as 14.8% in pT1b patients. Lymphadenectomy also adds useful information regarding prognosis and when planning adjuvant chemotherapy. 33
In our study, positive lymph nodes were proven to impair survival in pT2 patients in different treatment groups. It has previously been shown that, lymph node excision in pT2 patients improves survival 35 and positive lymph nodes at reresection/resection are a well-known negative prognostic factor. 36 The distribution of pT status in the IGBC reresection group was in line with our previous study, 11 with most patients in the pT2 category, followed by pT3 and pT1b. However, the distribution in the GBC resection group showed most pT3 cases.
Since a new distinction was made in the 8th edition of the American Joint Committee on Cancer (AJCC) concerning T2 tumours, 37 several studies6,19,29 have investigated survival in T2a (peritoneal side) and T2b (hepatic side) IGBC and GBC patients. We were unable to perform an overall survival analysis considering this distinction due to few pT registrations according to the 8th edition of the AJCC. The location of the T2b tumour in the dissection plane of a cholecystectomy may be a disadvantage in IGBC patients. A disruption of the natural layers and barriers between the tumour and the lymphovascular structures in the liver may lead to dissemination of tumour cells in the liver bed, leading to locoregional recurrence.29,38
Intraoperative perforation of the gallbladder during index cholecystectomy is because of the surgical intention and approach more common in IGBC patients, who are initially operated on for a benign indication as compared with GBC patients. 39 Bile spillage at index cholecystectomy has been shown to be a risk factor for decreased survival in patients with pT1b-T3 tumours. 18 In addition, higher rates of peritoneal dissemination and decreased chances of radical reresection have been shown. 40 These results further demonstrate the advantage of one-stage resection in IGBC patients. In a previous study from our group, 11 accidental perforation at index cholecystectomy tended to decrease resectability among patients planned for reresection, and perforation during index cholecystectomy was as high as 43% in patients planned for reresection. In this study, we were unable to study the occurrence of intraoperative perforation of the gallbladder during index cholecystectomy.
As in previous studies,3,7 most patients were not suited for reresection in the group with IGBC or resection in the group with GBC. In our study, most patients were in Stage IV (AJCC 6th edition), and metastases were found during reresection/resection in 22% of IGBC and in 24% of GBC patients. Nevertheless, most IGBC/GBC patients who underwent surgery had a radical resection (R0) according to histopathological diagnosis.
Limitations
Original data were collected from two prospective registers, and the limitations of this study are mostly inherent to registry data, for example, the quality of the source data and the amount of missing data. The studied period covers 11 years, and the SweLiv forms have been changed several times during these years, which could have affected the interpretation of the data. In addition, we were unable to cross-link SweLiv data with GallRiks during the entire study period; however, the completeness of the registry has improved in recent years. 8 We did not have access to personal data concerning GBC patients and could not collect information regarding histopathological results when TNM was incomplete, meaning that these patients could not be included in the survival analysis. Also, data concerning the use of chemotherapy were incomplete and missing in many patients in SweLiv and this variable could therefore not be included in the analysis.
Conclusion
Our results show that pT3 IGBC patients and possibly pT2 IGBC patients may benefit from one-stage resections. GBC was proven to be an independent predictor of improved survival in pT3 patients. It is reasonable to recommend that radiological suspicion of malignancy should be evaluated at a liver tumour centre to optimize patient outcomes.
Footnotes
Acknowledgements
The authors thank all surgeons in Sweden for reporting data to GallRiks and SweLiv and to all persons involved in maintaining these registries.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research work was supported by PhD Regional research grant Region Skåne, and the Erik and Angelica Sparres research foundation, Dr Carolina Muszynska and the Bengt Ihre foundation and government grant for clinical research (![]() ), Dr Bodil Adersson, and was used for salary and statistician support. No other funding from other organizations has been received.
), Dr Bodil Adersson, and was used for salary and statistician support. No other funding from other organizations has been received.
Informed consent
Informed consent has been given by all patients registered in SweLiv and GallRiks.