
Abstract
Background:
Parastomal hernia is common, but there are few population-based studies showing the frequency and outcome of parastomal hernia repair in routine surgical practice. The aim of this study was to identify patients undergoing surgery for parastomal hernia in Sweden and to define risk factors for complication and recurrence.
Methods:
A broad search of the Swedish National Patient Register 1998–2007 for all possible parastomal hernia repairs using surgical procedure codes. Records of all patients identified were reviewed and those with a definite parastomal hernia procedure were included and analyzed.
Results:
A total of 71 patients were identified after review of the records. The most common reason for surgery was cosmetic and the most frequent method was relocation of the stoma. Parastomal hernia recurrence rate was 18% during follow-up of a minimum 2 years. Overall, a surgical complication occurred in 32%. Possible risk factors were analyzed including emergency surgery versus planned, gender, age, indication for surgery, and method of surgery; none of which was significant.
Conclusion:
The frequency of parastomal hernia procedures was much lower than suggested by previous studies. The number of procedures per surgeon was even lower than expected. No specific risk factor could be identified. Parastomal hernia auditing in the form of a nationwide quality register should be mandatory. Centralization should be considered.
Introduction
Parastomal hernia (PSH) is common among patients with a stoma. The reported incidence varies from a few up to 78% (1–3).
Population-based studies on incidence and prevalence of PSH are rare, and studies on rate of PSH repair are even rarer (4, 5). However, there is an abundance of studies describing outcome of elective PSH repair, though these are often from a single center, describing a specific method of repair often with specific prosthetic material (6–8). Recurrence rates after PSH surgery in modern studies range from 3% to 22% (7–10).
Furthermore, there are few studies on emergency PSH repair, and these have shown high complication rates, including a 13.2% reoperation rate and 6.3% mortality rate, both at 1 month (4–6).
The most common indications for surgical treatment are incarceration, leakage, pain, discomfort, and cosmetic dissatisfaction (10). Emergency repair is most often due to incarceration. The frequency of these problems is not entirely known and might also vary depending on the socioeconomic and cultural background of the patient (5, 6, 9). According to population-based data from the Danish Hernia Register, 5%–10% of patients with PSH known to the healthcare provider, undergo surgical repair (4) corresponding to 60–70 cases annually or approximately 1.5 per 100,000 inhabitants per year (4, 5), indicating that very few PSHs are repaired. Of these, about one-third is emergency procedures due to incarceration, while two-thirds are elective procedures. According to the Danish Hernia Register, mortality is high; 25% following emergency procedures and 2.1% after elective procedures (5).
In Sweden, approximately 1000 stomas are created annually after cancer surgery alone (11), and approximately 35,000 individuals live with a stoma (12). Based on previous incidence figures, up to one-third of these patients are at risk for PSH (2, 4, 5, 13). Sweden has a long tradition of register studies utilizing comprehensive population-based data. The only country as yet to provide nationwide results after PSH surgery is Denmark, and their register data serve as the basis for this study.
Our expectation was that the frequency of PSH surgery in Sweden is similar or lower than that in Denmark, and that data on outcome are sparse in comparison, since no nationwide register exists.
The primary aim of this study was to determine the frequency of PSH surgery in Sweden, and recurrence and complication rates. A secondary aim was to identify any risk factors for complication and recurrence and to map the methods used for repair.
Material and Methods
Study Design
This is a descriptive study on PSH surgery in Sweden. All admissions to Swedish hospitals are registered in a national hospital register (the National Patient Register) administered by the Swedish Board of Health and Welfare, and coded according to International Statistical Classification of Diseases (ICD 10-SE). Both codes for diseases (ICD 10-SE) and for surgical procedures (NOMESCO Classification of Surgical Procedures, version 1.9, from 1997 revised 2004) are registered. The completeness of the register is 99% and readily available for extraction of data such as gender and main and secondary diagnoses, using the patient’s personal identity number and operation date (14, 15).
All patients operated for PSH during the period 1998–2007 were identified by searching the register for the procedure codes listed in Fig. 1. There were no specific codes for repair or treatment of PSH, as these were introduced in 2012. Hence, we began with a broad search covering all procedures that may have involved repair of a PSH. All patients’ personal identity numbers and the hospitals at which they were operated were extracted from the register.
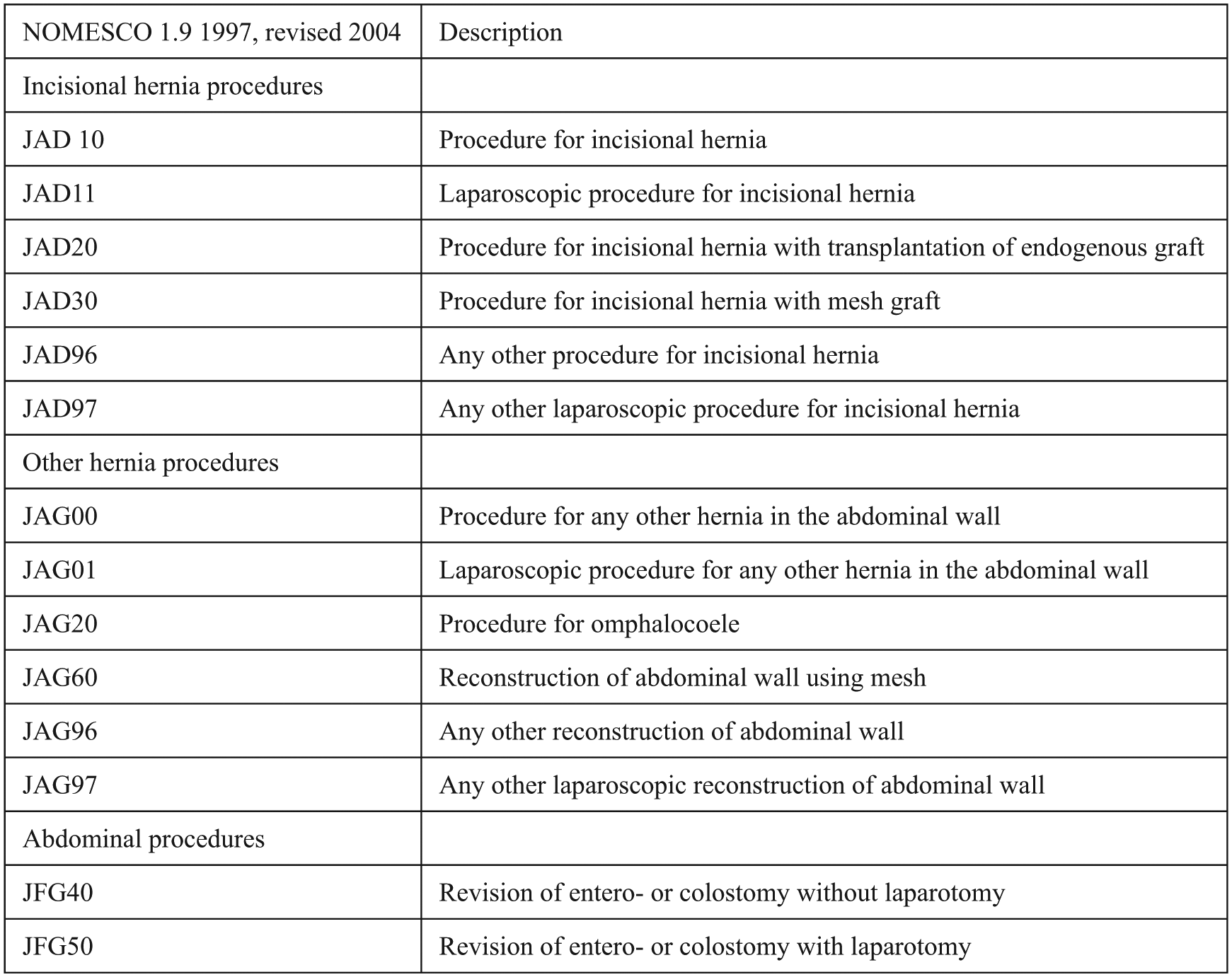
Parastomal hernia in Sweden 1998–2007; explanations of NOMESCO (Nordic version) Classification of Surgical Procedures, version 1.9, from 1997 revised 2004.
Medical records covering the first 2 years after the procedure, of all patients identified in the first broad search, were requested from the hospitals involved and reviewed. Hospitals not responding were sent a second request. The records were reviewed by an accredited colorectal surgeon. Actual procedures of repairing a PSH were identified and included in the study, all other records were discarded. Basic data were extracted from the records of all patients that had been operated due to PSH and entered in a study register. The procedure codes registered were validated by cross-checking against LÖF, the National Health Providers’ mutual insurance company, where all cases of healthcare injuries reported by the patients themselves are registered, including those involving PSH. Procedure codes from cases involving PSH during the relevant time period were extracted. The codes used here were found to correspond with those used in the search of this study.
Inclusion Criteria
The criteria for inclusion were as follows: age over 18 years and operated for PSH. The initial wide search was made according to the surgical procedure codes listed in Fig. 1, during the study period 1998 until 2007. See Fig. 2 for a schematic view of the inclusion process.
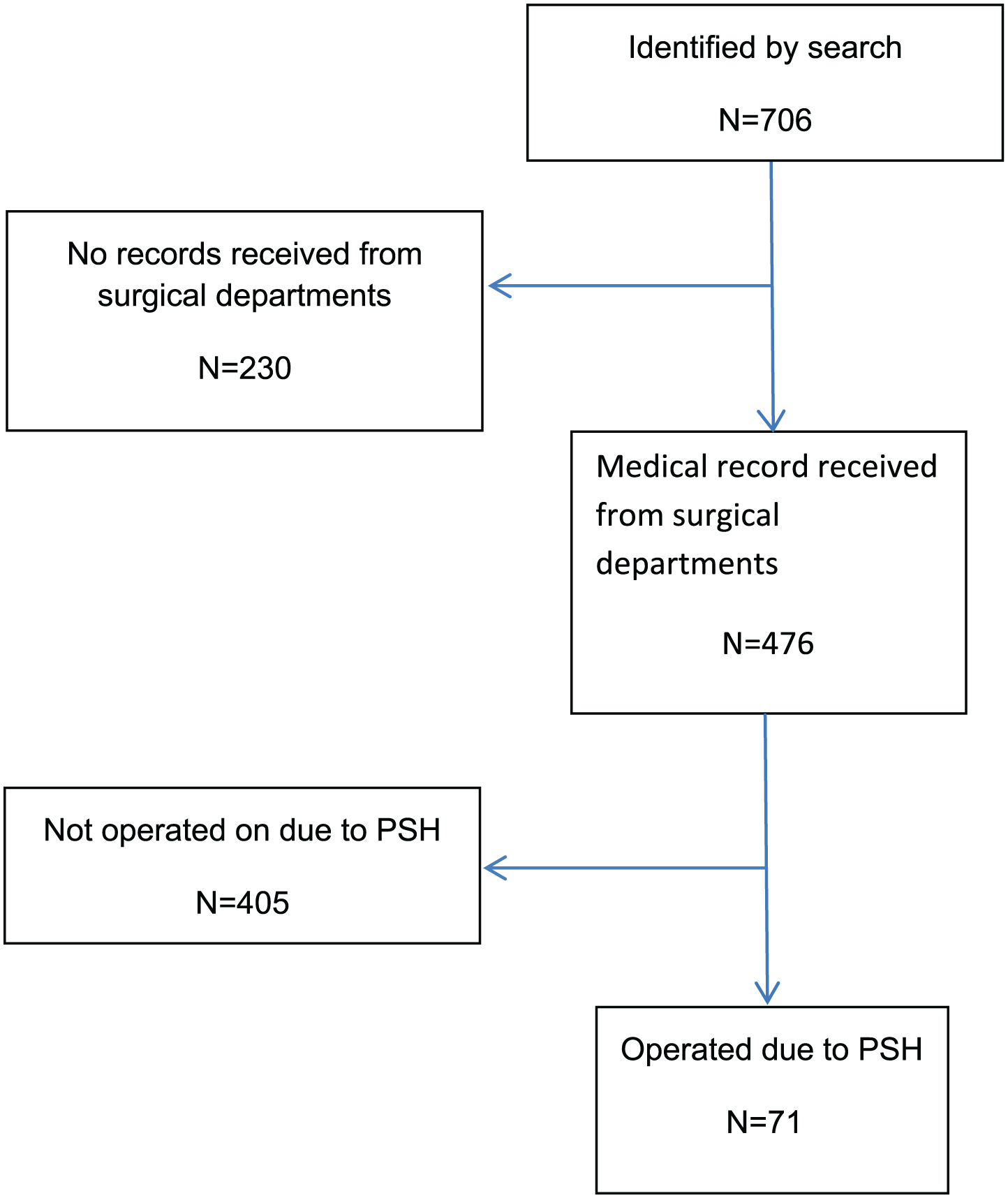
Parastomal hernia (PSH) repair in Sweden 1998–2007; consort diagram.
Study Variables
The registered parameters are as follows: age, gender, date, number of procedures, elective or emergency surgery, type of procedure, indication for surgery, complications (surgical site infections, stenosis of stoma, skin problem, and recurrent PSH), and mortality. PSH at the new site was registered as a recurrence, whereas incisional hernia at the former stoma site was excluded. We opted to have four separate age groups analogous to the study by Helgstrand et al. (4). We also decided to sub-divide operation methods between elective or emergency surgery.
Ethics
The study protocol adhered to the Helsinki Declaration and was approved by the Regional Ethics Committee in Umeå, Sweden (approval ids.: dnr 09-021M and dnr 2017-165-32).
Statistical Analyses
SPSS, version 24TM was used for all statistical analyses. Analyses of group variables were performed using the chi-square test; a p-value <0.05 was considered significant. When numbers were too few for chi-square to be valid, Fishers Exact Test was used.
Results
The preliminary broad search identified 706 patients who had possibly been operated for a PSH. After one or two requests, 67.4% (476/706) of these patients’ medical records were received.
Review of those records identified 71 patients who had definitely been operated for PSH, by 61 different surgeons at 35 surgical departments.
Patient characteristics and data describing the surgical procedures are presented in Table 1. The material was equally distributed between men and women. The most common reason for surgery was cosmetic, that is, ugly hernia (Table 1). Furthermore, relocation of the stoma (Table 1) was the most commonly used method. The overall surgical complication rate was 32.4% and the recurrence rate 26.8% (Table 2) after a follow-up of at least 2 years. In some cases, the patient was dismissed from the department in shorter time than 2 years, and if no more entries were to be found in the records, this was regarded as no recurrence. Mean time from the surgery to the last entry in the records was 361 days (range: 11–2470 days). Totally four patients had a second operation due to recurrent PSH after the index PSH operation. Meshes used were different kinds of polypropylene meshes in 18 cases; in 2 cases, a PTFA mesh; and in 8 cases, the prosthetic material was not defined in the record. The most common placement of the mesh was in sublay position (16 cases), the second most common position was intraperitoneal onlay (4 cases), the third most common position was an onlay position (3 cases), and in 5 cases the position was not was not defined in the record. Finally, possible risk factors for complications and recurrence (emergency surgery vs planned, gender, age, indication for surgery, and type of operation) were analyzed, but none of these was found to be significant (Table 3).
Parastomal hernia (PSH) repair in Sweden 1998–2007; basic demographics and characteristics.
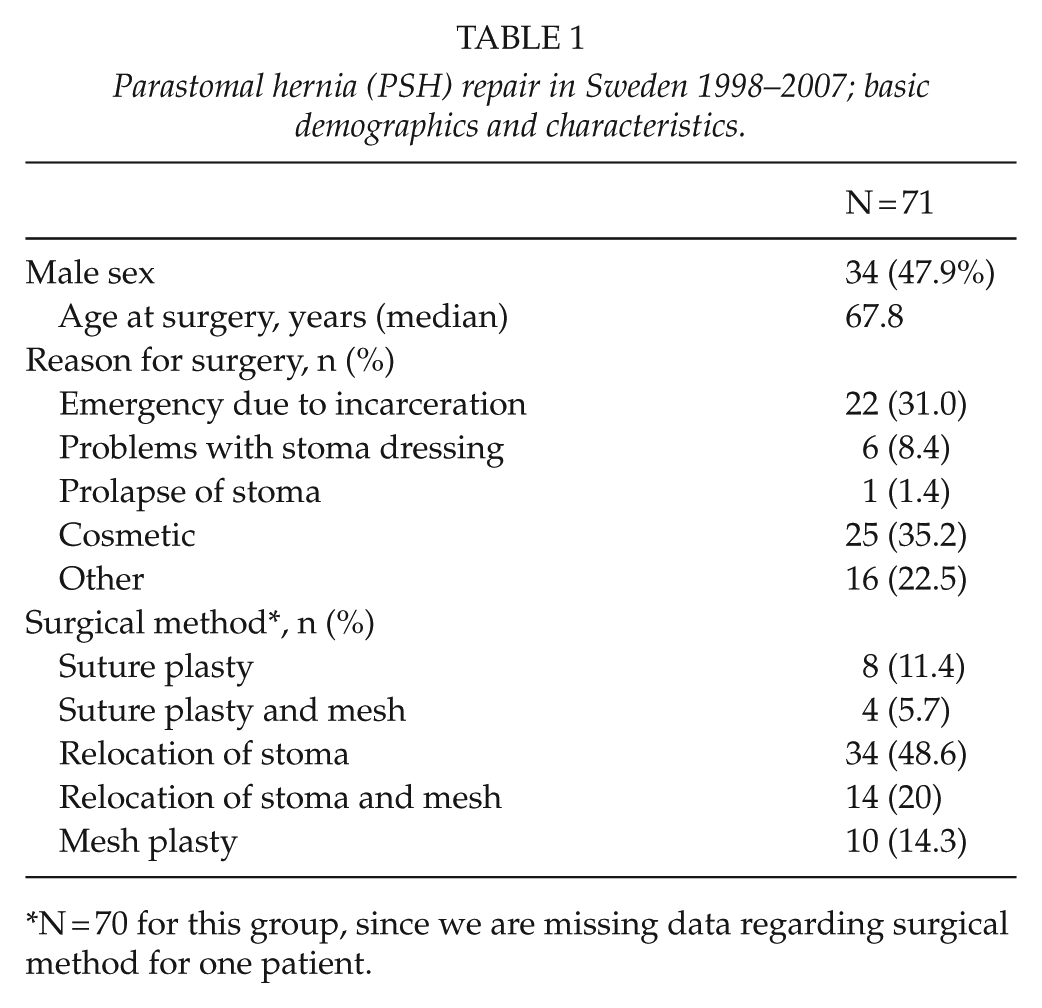
N = 70 for this group, since we are missing data regarding surgical method for one patient.
Parastomal hernia repair (PSH) in Sweden 1998–2007; outcome and complications.
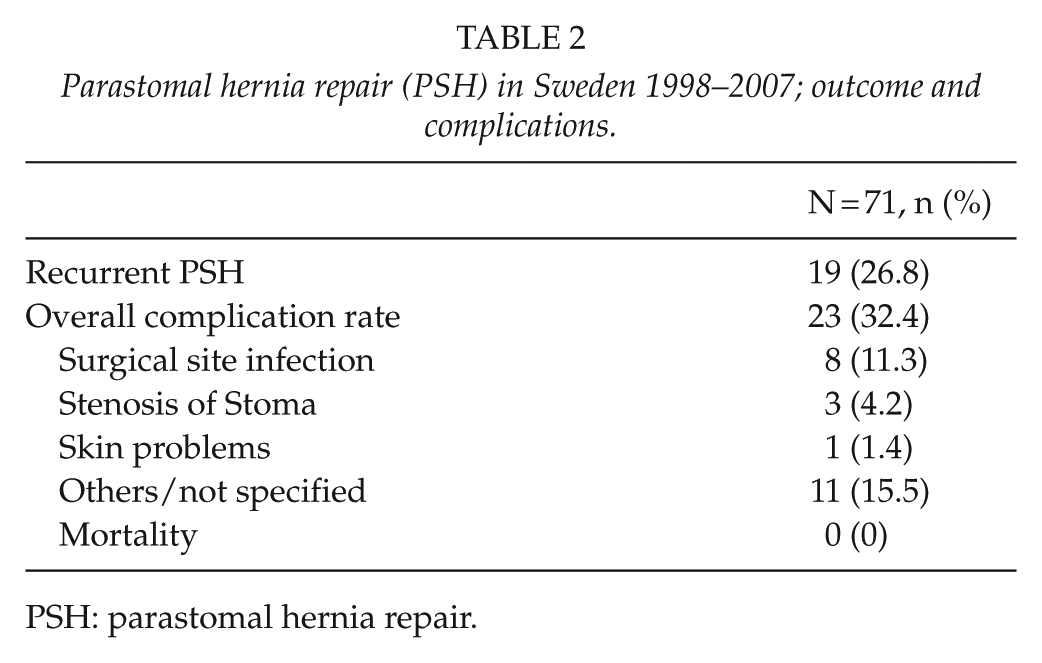
PSH: parastomal hernia repair.
Parastomal hernia repair in Sweden 1998–2007: analysis of risk factors.
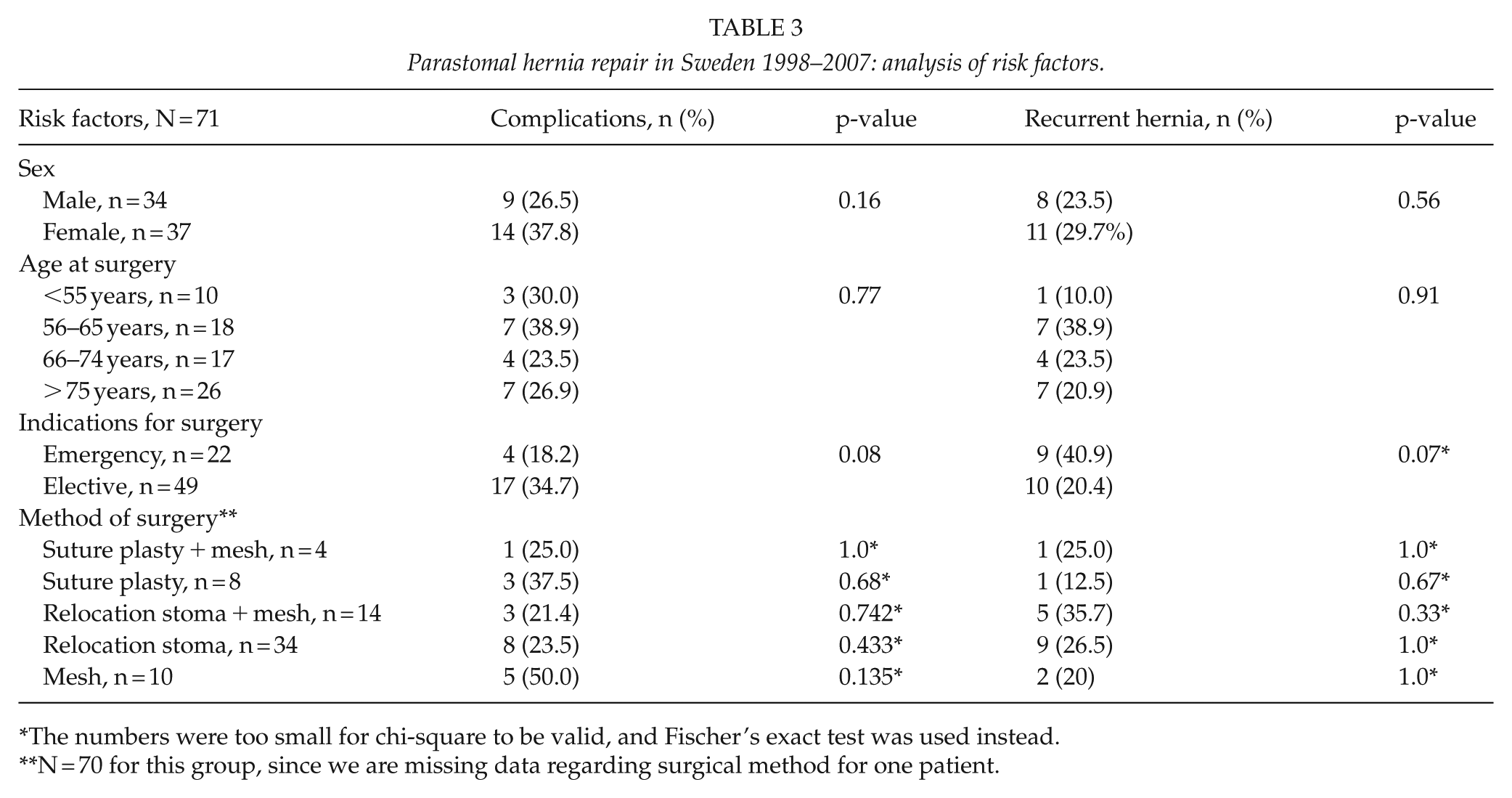
The numbers were too small for chi-square to be valid, and Fischer’s exact test was used instead.
N = 70 for this group, since we are missing data regarding surgical method for one patient.
Discussion
The main finding of this study was that the frequency of PSH surgery in Sweden is much lower than we expected. Complication rates were acceptable, and no particular risk factors could be identified. We conclude that the frequency of elective PSH repair is very low; only 49 elective procedures were identified over a 9-year period (of 71 procedures identified, including emergency surgery). This extrapolates, considering the missing data to 71*706/476 equals 105 procedures over a 10-year period. Even so, assuming that around 1000 ostomies are created each year, 10,000 ostomies of all forms should have been created during the period investigated. If one assumes a PSH frequency of 50%, this would have resulted in 5,000 PSH repairs if all had been repaired. The 49 (73 cases with extrapolation) cases actually repaired electively thus represent only a very small proportion of all PSHs that should have occurred. Our findings suggest that the frequency of elective PSH repair procedures in Sweden is far less compared to Denmark, 0.12 per 100,000 inhabitants compared to 1.5 per 100,000 inhabitants. This is indicating that Swedish surgeons, for several reasons, are restrictive in performing PSH repair. Reasons for the low frequency of PSH surgery in Sweden might be the well-known high recurrence and morbidity rates and local tradition embracing more reactionary and old fashioned methods (4, 5, 9). There are no specialized or leading centers for PSH surgery in Sweden or a national register as, for example, in Denmark. A specific nationwide quality register would probably increase the quality of PSH surgery, as has been the case with other procedures such as inguinal hernia surgery (16).
Short-term results regarding complications and recurrent PSH were better than anticipated (9) and mostly of minor character (4, 6, 13, 17). Retrospective studies, however, tend to produce lower complication rates than prospective studies. However, the number of cases in this study was low, and prospective studies evaluating specific repair techniques show far higher complication rates (4, 9). One possible reason for the low complication rate in this study is that the procedures used were usually reactionary without mesh, that is, relocation of the stoma or reducing the opening in the abdominal wall with sutures, all of which have poor long-term results.
The strength of this study is that it is based on a well-defined population of patients, whose records have been thoroughly scrutinized, thus representing surgical outcome in routine practice nationwide.
One obvious weakness is that there was no specific surgical procedure code for repair of PSH during the period of the study. This means that any number of patients might have escaped identification despite our broad search including a wide spectrum of procedure codes that could have represented PSH repair, for example, emergency procedures involving a PSH might be coded as an exploratory laparotomy, but including this in the search would have generated an unmanageable number of records. The low number of elective PSH procedures could be explained by coding bias, but we have tried to address this by comparing registers though and the codes used in the different registers matched, so this is less likely. Another possibility is that among missing data, a high volume center is hidden, and the percentage of actual PSH procedures are much higher in the missing material.
There were no differences in complication or recurrence rates according to gender or age group. Unfortunately, the statistical power was limited by the dwindling number of patients operated on, so these results must be interpreted with caution. Even so, our results indicate from the risk analyses that age and gender are not risk factors for complications and recurrence. The frequency of complications was higher in patients operated with a mesh, and even though this difference was not significant, it may be prudent to properly inform the patients about the risks associated to the use of mesh, since there are few studies published on the long-term results of PSH repair with mesh. European Society of Hernia recommends mesh when repairing a PSH but does not comment particularly on the long-term effects. Some studies of both the use of mesh when repairing PSH and the use of mesh when repairing incisional hernias have shown high reoperation and complication rates related to mesh; problems that may develop many years after surgery (18–20).
In this survey, the commonest reason for PSH repair was cosmesis. Arguably, the overall price in terms of risk for reoperation, morbidity, and mortality, for correcting a cosmetically disturbing PSH is potentially high for the individual patient. On the other hand, inability to bathe in public or to wear clothes of preference impairs a person’s quality of life. Recent research has shown that many complaints arising from a PSH can be addressed non-surgically, but there is a lack of information regarding the efficiency and results of conservative management (10).
In view of the low number of procedures performed each year, it would seem logical to centralize PSH repair to a few centers of excellence, so as to gain higher volumes and provide better opportunities for research. Hopefully, dedicated centers should also lead to better access for Swedish patients and also provide higher quality of surgery. Unfortunately, this leaves the problem of emergency surgery which must also be addressed. It seems reasonable that all elective procedures should be performed as part of clinical trials preferably randomized trials comparing different methods and materials, and all procedures should be entered in a nationwide register regardless.
In conclusion, this study shows that the frequency of PSH procedures in Sweden is low; much lower than anticipated from a previous population-based study (4). Furthermore, the number of procedures per surgeon is very low. The complication rate was in line with previous reports, but the rate of recurrence was high. No specific risk factors could be identified.
Footnotes
Acknowledgements
The authors thank research nurse Lisa Eskilsson, Department of Surgery, Sunderby hospital, Region Norrbotten, and Robert Lundqvist, statistician, Region Norrbotten, and all hospitals participating.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Regional Ethics Committee in Umeå, Sweden (approval ids.: dnr 09-021M and dnr 2017-165-32).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication ofthis article: This work was funded by the Department of Research and Development, Region Norrbotten.