
Abstract
Background and Aims:
Laparoscopy in blunt abdominal trauma is challenging because of multiple associated injuries, higher trauma score values and higher morbidity and mortality, as compared with patients with penetrating abdominal trauma. The aim of this study was to investigate the role of laparoscopy in the management of blunt abdominal trauma patients and to highlight related challenges.
Material and Methods:
Over a 4-year period, patients managed laparoscopically for blunt abdominal trauma were retrospectively analyzed. Perioperative details, indications for laparoscopy and conversion, complications, and length of hospital stay were discussed.
Results:
A total of 35 stable patients underwent laparoscopy. The mean Injury Severity Score was 12 (4–38). Therapeutic laparoscopy was performed in 15 (56%) and diagnostic in 12 (44%) patients. Eight (23%) patients were converted to therapeutic laparotomy. Intraoperative bleeding, complex injuries, visualization problem, and equipment failure necessitated conversion. Three (30%) patients with negative computed tomography scan had therapeutic laparoscopy for mesenteric injuries. There were no missed injuries. The mean length of hospital stay was 11 days in both groups.
Conclusion:
Laparoscopy for stable patients is feasible and safe. Multiple injuries make laparoscopy more difficult, and advanced laparoscopic skills are required. The conversion rate is high; however, the non-therapeutic laparotomies were completely eliminated in this study.
Introduction
Laparoscopy for penetrating abdominal trauma (PAT) is increasingly practiced all over the world with the reported sensitivity, specificity, and accuracy of nearly 100% (1–3). The current rate of missed injuries is reported to be below 0.4%, and the conversion rate is ranging from 7% to 47% (4–8).
However, the role of laparoscopy in blunt abdominal trauma (BAT) is not clearly defined (9). Patients with BAT have higher trauma score values and higher morbidity and mortality, compared with patients with PAT (10). BAT is usually associated with other injuries, and clinical examination is not always reliable, due to distracting associated injuries (11). Computed tomography (CT) scan examination is the gold standard, but it is unreliable for detecting hollow viscus injuries. In cases of diagnostic uncertainty, exploratory laparotomy is seen as an innocuous intervention by many investigators (7, 10). However, laparotomy is associated with the morbidity rate as high as 41% (12). Moreover, the rate of unnecessary negative laparotomies is 27% (12).
Laparoscopy is widely applied in patients with PAT and proven to be accurate, associated with low morbidity, faster recovery, and shorter length of hospital stay (LOS) (5, 13, 14). On the contrary, laparoscopy for BAT encounters many challenges and is rarely reported in literature.
The aim of this study was to investigate the role of laparoscopy in the management of patients with BAT and to highlight the challenges encountered with laparoscopic management of these patients.
Material and Methods
This study analyzed the prospectively collected data of hemodynamically stable patients with BAT who were managed laparoscopically at a single academic hospital, from January 2012 to December 2015. Our institution is a tertiary academic hospital providing trauma services for a population of 7.3 million people. Ethics clearance was obtained from our institutional Research Ethics Committee.
Exclusion criteria were as follows: patients managed with initial laparotomy or successful non-operative management, patients with penetrating abdominal injury, cases with incomplete records, and patients under the age of 12.
Patients’ age and gender, mechanism of injury, location of injury, the Injury Severity Score (ISS) and the Penetrating Abdominal Trauma Index (PATI), CT scan findings (64 multislice system), indications for surgery, intraoperative findings, and procedures performed and reasons for conversion were recorded and analyzed. The complications of Clavien–Dindo (CD) grades 3–5 were considered significant and were analyzed (15).
This study included converted-to-laparotomy patients in a control group, based on the point that at the time of laparoscopy all patients were considered stable and similar in the intent to complete operation laparoscopically.
The patients with the systolic blood pressure below 90 mm Hg and the mean inspiratory pressure greater than 30 mm Hg were considered unstable and offered laparotomy.
Details of the patients were summarized descriptively by mean, median, minimum, and maximum values for continuous variables and by frequency count and percentage calculations for categorical variables. Fisher’s exact test was used for comparisons of frequency counts/percentages. Median values were compared by the nonparametric Wilcoxon rank-sum test. All statistical procedures were performed with SAS software (SAS Institute, Cary, NC). A value of p < 0.05 was considered significant.
Results
Over the study period, 318 trauma patients were managed with laparoscopy (Fig. 1). All the patients were resuscitated along the Advanced Trauma Life Support (ATLS) principles and were stable at the beginning of laparoscopy. PAT were recorded in 283 (89%) patients. A total of 35 (11%) patients had BAT and were analyzed. Of the 35 patients with BAT, 27 (77%) were managed with laparoscopy, 15 (56%) of them underwent therapeutic intervention, while 12 (44%) patients had diagnostic laparoscopy. The laparoscopic-assisted approach was utilized for therapeutic procedures in six patients with hollow viscera injuries (Table 1).
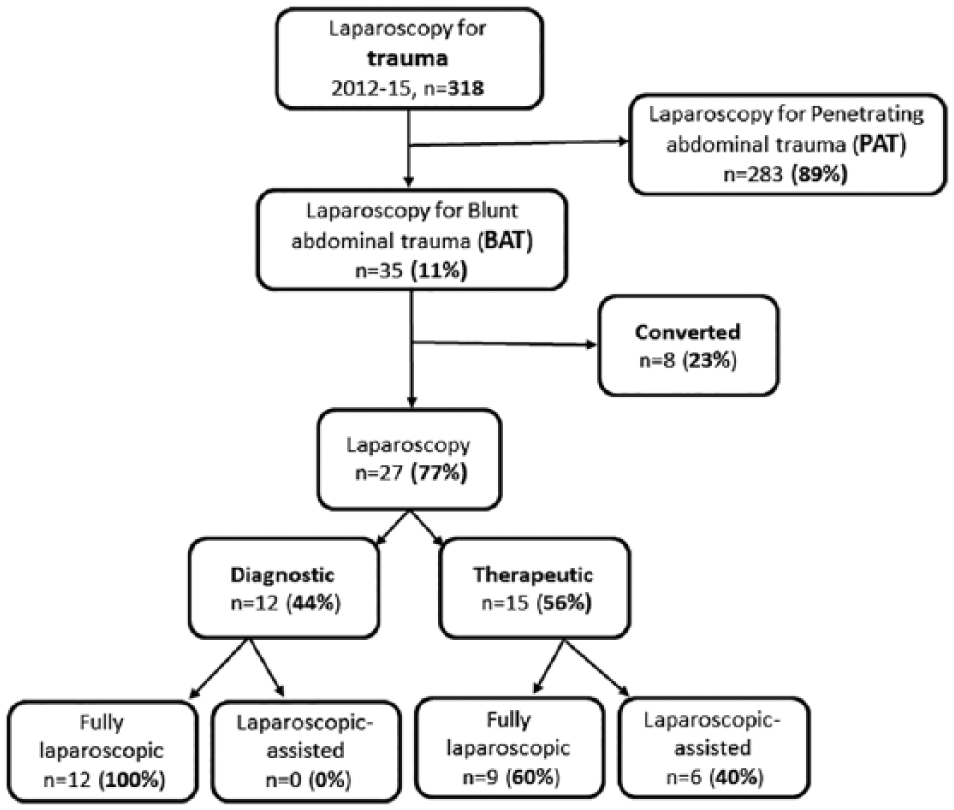
Study population.
Characteristics of patients.
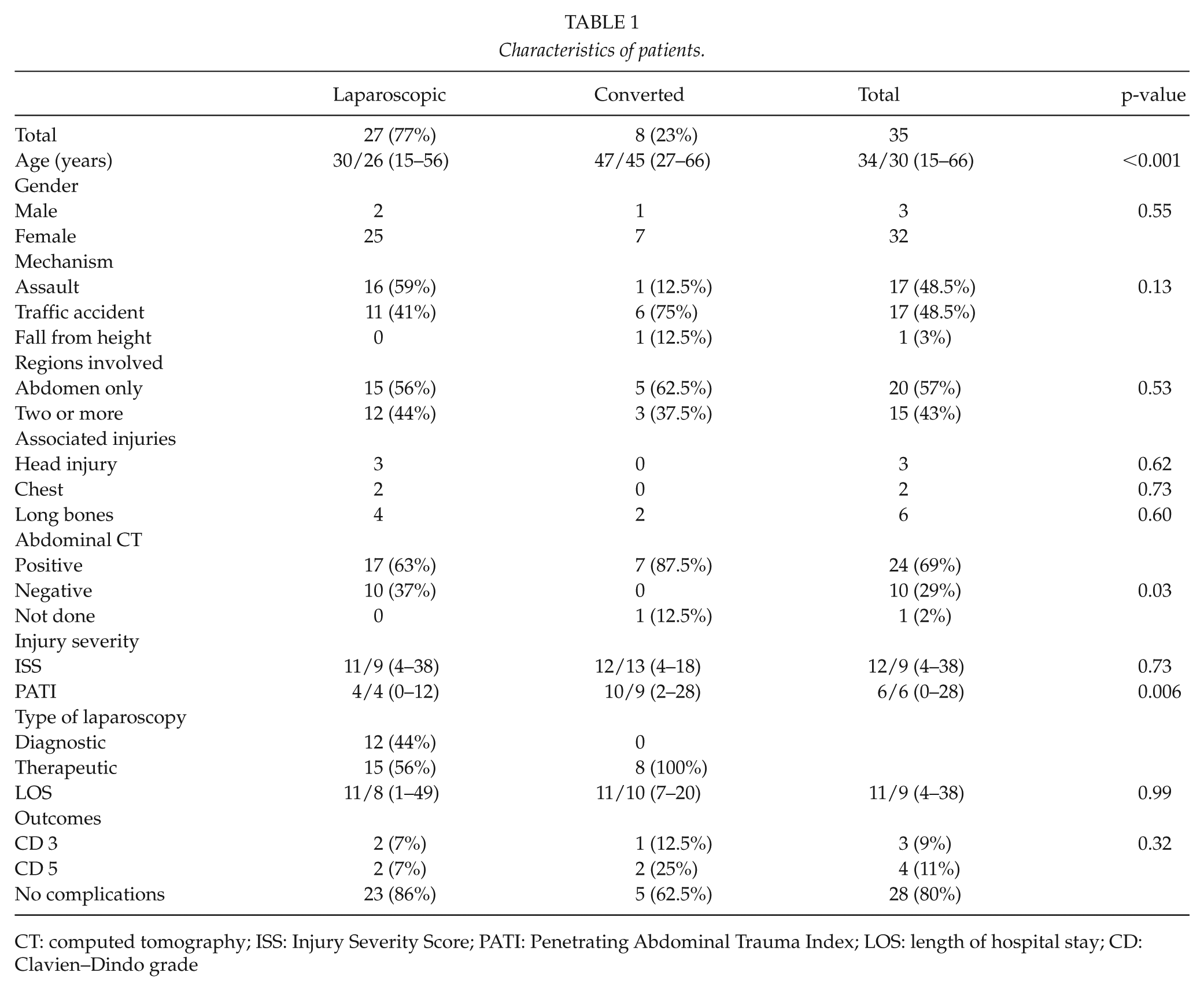
CT: computed tomography; ISS: Injury Severity Score; PATI: Penetrating Abdominal Trauma Index; LOS: length of hospital stay; CD: Clavien–Dindo grade
The most common mechanism of blunt trauma was assault in the laparoscopic group and traffic accident in the converted group. Two or more anatomical regions were involved in 15 (43%) of the patients. The ISS did not differ between the groups; however, the PATI was significantly higher in the converted group.
Only one patient (1 of 35, 2%) did not have preoperative abdominal CT scan. A total of 10 (37%) patients in the laparoscopy group had negative findings on abdominal CT scan; however, three (30%) of them had therapeutic laparoscopy for grade 2 mesenteric injuries requiring repair. The indications for laparoscopic exploration were the following: peritoneal irritation, abdominal tenderness, suspicious of hollow visceral injuries on abdominal CT, and unequivocal signs on physical examination.
Laparoscopic inspection of all intraperitoneal organs were performed in all patients, retroperitoneal organs were mobilized and inspected when indicated. Repair of the small bowel and mesentery were commonly performed procedures. Intraoperative findings and performed procedures are listed in Table 2. Eight (23%) patients were converted to therapeutic laparotomy. The conversion to laparotomy was necessary in four patients with intraoperative bleeding which could not be quickly controlled; one patient was converted because of complex injuries, two due to poor visualization, and one due to equipment failure.
Intraoperative findings and therapeutic procedures.
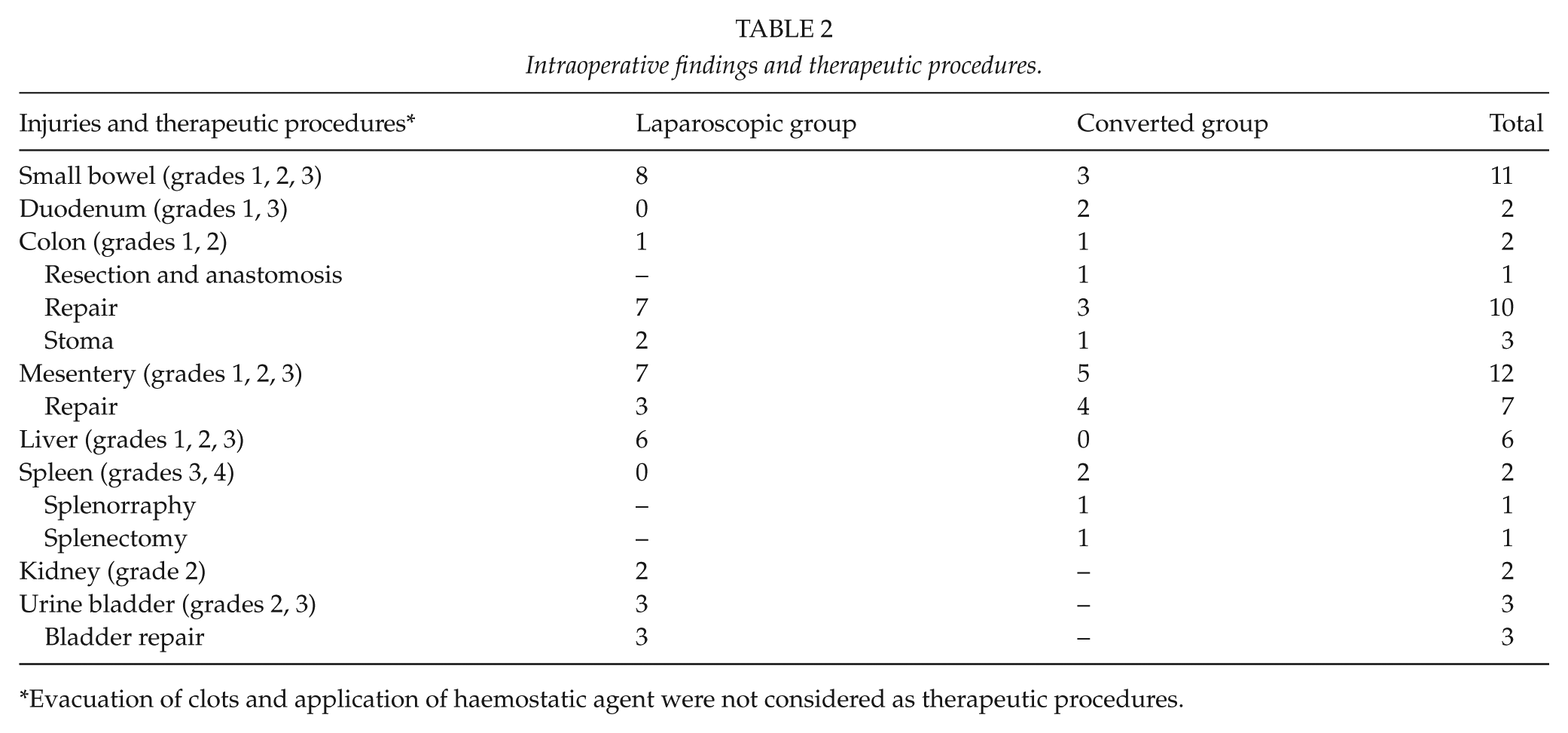
Evacuation of clots and application of haemostatic agent were not considered as therapeutic procedures.
There were no missed injuries in this study. The mean LOS was 11 days in both groups. Two patients died in each group. These patients were severely injured polytrauma patients (ISS, 16–38). Three patients suffered Clavien–Dindo grade 3 complications. In the laparoscopy group, one had percutaneous drainage of intra-abdominal abscess and second had drainage/debridement of assisted access site for wound sepsis. One patient in the converted group had re-look laparotomy for intra-abdominal abscess (Table 3).
Patients with significant complications.
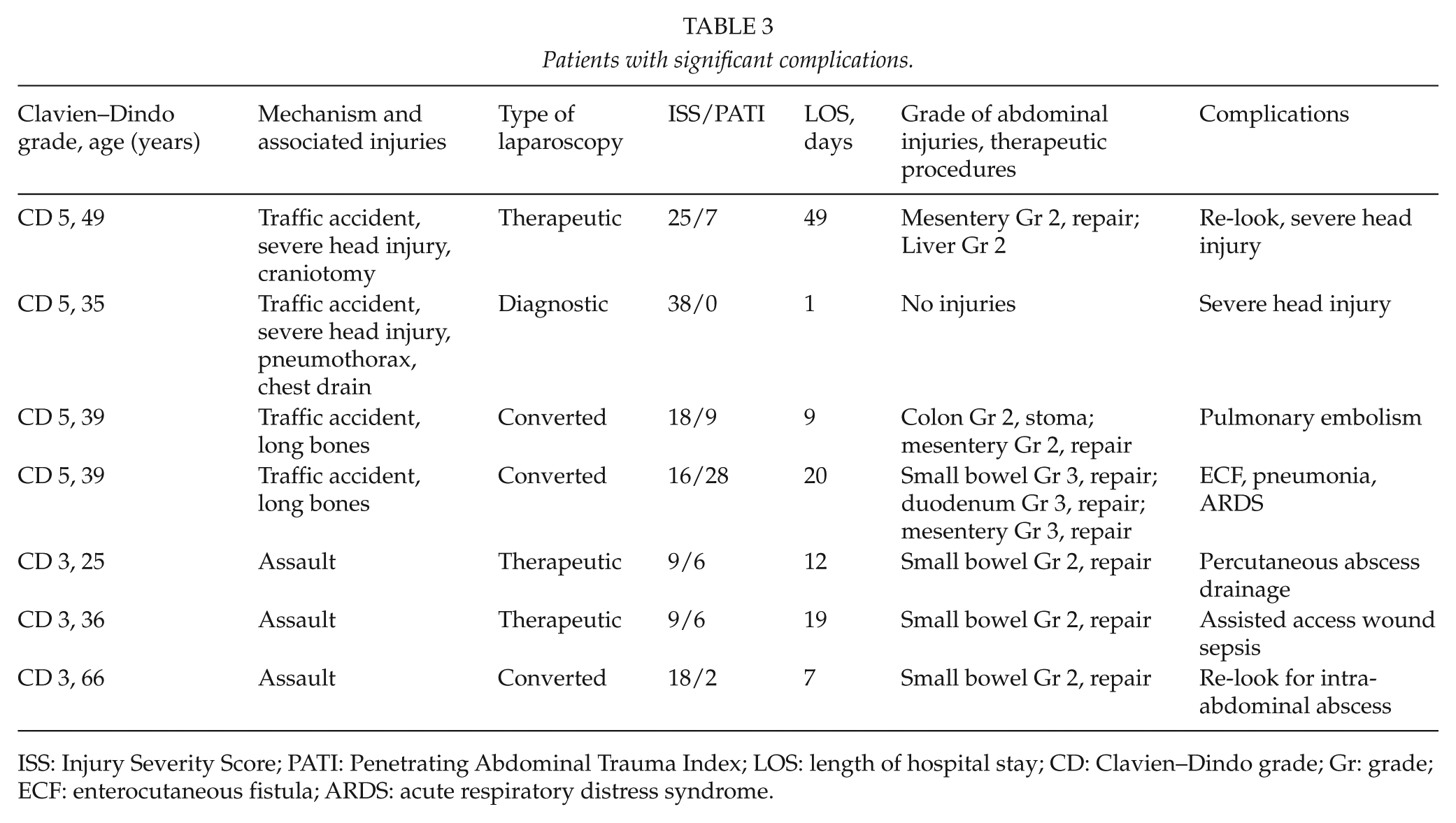
ISS: Injury Severity Score; PATI: Penetrating Abdominal Trauma Index; LOS: length of hospital stay; CD: Clavien–Dindo grade; Gr: grade; ECF: enterocutaneous fistula; ARDS: acute respiratory distress syndrome.
Discussion
The management of patients with BAT poses significant challenges to the treating physicians. Only 5%–10% of blunt trauma patients will have significant intra-abdominal injuries requiring surgical intervention, and 10% of them will present with negative clinical examination (16). Severe “occult” intra-abdominal injuries requiring specific treatment were described in BAT patients even without distracting injuries and abdominal pain (17). In this scenario, abdominal imaging improves diagnostic yield; however, it is still not an entirely accurate approach.
The Focused Assessment with Sonography in Trauma (FAST) is non-invasive bedside imaging modality to identify free fluid in the abdominal cavity; however, it is highly operator dependent. It is commonly used as an adjunct to the primary survey according to the ATLS guidelines. However, Dolich et al. (18) reported that 1.7% of patients with negative FAST had organ injuries, and 23% of them required exploratory laparotomy. In the recent study from the United States, the authors discovered that the sensitivity of FAST in stable patients with BAT was 22%, and they proposed, where possible, to bypass FAST exam and go directly to CT scan (19). CT scan is the imaging of choice in BAT; however, it also has limitations. Hollow viscus injuries are not easily demonstrated on abdominal CT scan. In most patients, only indirect signs of injuries can be identified, this can lead to missed injuries and delayed surgical treatment (20). A delay in surgical treatment of hollow viscus injuries in as little as 5 h may increase morbidity and mortality (21–23). Despite its limitations, CT remains standard imaging of hemodynamically stable patients with BAT (8, 24–27), and this study confirmed it. Abdominal CT scan was performed preoperatively in 98% of patients, and only one patient did not have a scan for an unknown reason. All patients in the converted group had positive findings on CT scan; however, in the laparoscopic group, 37% of patients had negative CT scan. The possibility of the false-negative CT findings was highlighted in this study. Three (30%) patients with negative CT scan had therapeutic laparoscopy for mesenteric injuries. Although physical examination and CT scan findings will identify most injuries, there are still a sizable group of patients who will have false-negative findings, and necessary treatment will be delayed. Laparoscopy in these cases will accurately identify and offer therapeutic options for occult intra-abdominal injuries. The question on when to offer laparoscopy and whether to engage in a trial of non-operative management still remains unanswered.
The combination of radiographic, laboratory, and physical examination findings was utilized in the Bowel Injury Prediction Score (23, 28). The score of 2 or greater is highly suggestive of bowel injuries and may suggest early diagnostic laparoscopy; however, it was not used in this study and needs prospective validation.
Diagnostic peritoneal lavage (DPL) in BAT was discouraged due to over-sensitivity and relatively low specificity (29). However, the concept of DPL can be modified to the laparoscopic assessment in surgical trauma (LAST) under local anesthesia in the trauma resuscitation area (30). LAST appears a promising screening tool, but needs validation.
In our institution, all stable trauma patients requiring surgical exploration will undergo laparoscopy and be converted to laparotomy when conversion criteria are met. There are no doubts that BAT patients with signs of peritonitis, positive findings on imaging, or with high suspicions for injuries (like seatbelt sign) require surgical exploration and our choice for stable patients is laparoscopy. Equivocal or worsening abdominal examination in most cases warrants surgical exploration. Our indications for surgical exploration are in agreement with other studies (26, 29, 31–33). A high index of suspicious for hollow viscus injuries is reasonable, as in this study, the most common injuries were small bowel and mesenteric injuries; the same is reported in the literature (34). More studies are needed to draw the line between indications for diagnostic laparoscopy and non-operative management.
Most patients with BAT suffer from road traffic accidents and have multiple associated injuries. The prompt diagnosis of all injuries is difficult, and a delay in management may result in the higher complication rate of 25%–65% (35). In this study, associated injuries were present in both groups and accounted for 43%. The mechanism of injury did not affect the laparoscopic management.
The ISS score was higher in the converted group, but the difference was not statistically significant. However, the PATI score was significantly higher in the converted group. These findings suggest that more complex intra-abdominal injuries were eventually managed with the open approach.
Patients with BAT frequently have major physiologic derangements or associated severe injuries, often making them unstable and not suitable for laparoscopy. The recovery of patients depends mostly on associated injuries convalescence and that seems to mitigate the potential benefits of laparoscopy, such as LOS and ventilator-free days (36). In this study, associated injuries were the main reason why LOS was similar in both groups. The similar LOS stay for BAT patients was reported by Johnson et al. (9). The complications were higher in the converted group, but it may be related to more complex intra-abdominal injuries. All four patients who died were severely injured polytrauma patients. In the laparoscopy group, two patients died from severe head injury; it was expected and was unrelated to laparoscopy. Although it is controversial, we believe that laparoscopy benefits of less operative trauma and faster recovery outweigh the potential increase in intracranial pressure during laparoscopy. However, some investigators suggest head injury as a relative contraindication to laparoscopy (26). Further studies are needed to investigate this issue.
Our policy is to offer initial laparoscopy to all stable patients who need surgical exploration. The algorithm was recently reported by Matsevych et al. (13). Laparoscopy for BAT requires a thorough inspection of all intra-abdominal organs in order not to miss injuries. Camera navigation skills, mobilization of all organs in the abdominal cavity, bowel run, and laparoscopic suturing were recently reported as the critical laparoscopic skills needed for trauma laparoscopy (37, 38).
Our conversion rate (23%) for BAT was higher than the reported rate for PAT (11.7%) (13). The higher conversion rate for blunt trauma reflects the severity and multiplicity of intra-abdominal injuries. In literature, the conversion rate varies from 8.5% to 37% depending on the selection criteria (29, 34, 39, 40). The reasons for conversion in this study were bleeding, multiple complex injuries, visualization problem, and equipment failure. Although it was not observed in this study, the respiratory and hemodynamic deterioration of patient should lead to conversion (13).
Benefits of laparoscopy over laparotomy in patients with abdominal trauma are well documented. The decrease or even elimination of non-therapeutic laparotomies, reduction in the incidence of postoperative morbidity and mortality, decrease of postoperative pain, enhanced recovery, and shorter LOS were reported (2,9, 41, 42).
Our study has some limitations. The study was a retrospective, had small sample size, and follow-up was not accurately documented. The result of this study strongly depends on the level of operating surgeon’s laparoscopic skills and, therefore, can be reproduced only in centers with similar expertise. The groups comparison should be taken with caution because of heterogeneity and small numbers. The overall LOS was calculated, and it does not accurately represent LOS after laparoscopy. Nonetheless, the study gives an insight into how laparoscopy could be used for blunt trauma, and it highlights the challenges encountered during laparoscopy.
Conclusion
In conclusion, laparoscopy for stable patients with BAT is feasible, accurate, and safe; however, it faces multiple challenges. Pre-operative abdominal CT scan can help to select patients for non-operative management, although, the low accuracy of CT scan in detecting hollow viscus injuries should be taken into consideration. Laparoscopy cannot replace CT scan or non-operative management, but it can accurately identify and manage hollow viscus injuries in cases of uncertain findings on physical examination and imaging. Multiple intra-abdominal injuries make laparoscopic exploration more difficult, and advanced laparoscopic skills are required. Associated extra-abdominal injuries contribute to the severity of patients and prolong the convalescence by masking the benefits of laparoscopy. The conversion rate is high; however, the non-therapeutic laparotomies were eliminated in this study. More studies are needed to confirm our findings with the laparoscopy for blunt trauma patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Sefako Makgatho University Research Ethics Committee (SMUREC; reference number: SMUREC/M/32/2016: IR) by O.Y.M. (on behalf of all authors).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.