
Abstract
Background and Aims:
Previous studies have reported lower implant survival rates, residual pain, and higher patient dissatisfaction rates following knee arthroplasty in younger knee arthroplasty patients. We aimed to assess the real-world effectiveness of knee arthroplasty in a prospective non-selected cohort of patients aged 65 years or less with 2-year follow-up.
Material and Methods:
In total, 250 patients (272 knees) aged 65 years or less were enrolled into this prospective cohort study. Patient-reported outcome measures were used to assess the outcome.
Results:
The mean Oxford Knee Score and all Knee Injury and Osteoarthritis Outcome Score subscales increased significantly (p < 0.001) from preoperative situation to the 2-year follow-up. Significant increase (p < 0.001) in physical activity was detected in High-Activity Arthroplasty Score and RAND-36 Physical Component Score (PCS). Pain was also significantly (p < 0.001) relieved during the follow-up. Total disappearance of pain was rare at 2 years. Patients with milder (Kellgren–Lawrence grade 2) osteoarthritis were less satisfied and reported poorer patient-reported outcome measure than those with advanced osteoarthritis (Kellgren–Lawrence grade 3–4). There was no difference in the outcome (any patient-reported outcome measure) between patients who underwent total knee arthroplasty and those who received unicondylar knee arthroplasty.
Conclusion:
We found that measured with a wide set of patient-reported outcome measures, both total knee arthroplasty and unicondylar knee arthroplasty resulted in significant pain relief, as well as improvement in physical performance and quality of life in patients aged 65 years or less. Real-world effectiveness of these procedures seems to be excellent. 15% of patients still had residual symptoms and were dissatisfied with the outcome at 2 years after the operation.
Keywords
Introduction
Younger patients have high expectations for the outcome of total knee arthroplasty (TKA), and this may predispose them to dissatisfaction after the operation (1–3). Furthermore, younger age is associated with higher rates of complications and an increased risk for revision surgery (4, 5). Arthroscopic surgery of the degenerative knee has been shown to be ineffective (6), and the incidence of high tibial osteotomy has also steadily decreased (7, 8). Hence, increasing number of younger patients with mild knee osteoarthritis (OA) are being offered knee arthroplasty. In the Nordic countries, the incidence of TKA has grown especially rapidly among patients younger than 65 years of age (9). As both young age (4, 5) and mild knee OA (10) are known to be risk factors for revision surgery, it is of critical importance to assess the outcome of knee arthroplasty within this demanding patient group.
Only a few recent studies have reported the outcome of TKA measured with patient-reported outcome measures (PROMs) in younger patients (1, 11, 12). Only one (12) of these previous trials was a true prospective observational study. Furthermore, patient activity was not assessed with a specific activity score in any of these studies. All of them reported an overall positive effect of TKA on symptoms, activities of daily living (ADL), and quality of life (QoL). However, a variable proportion of patients (11%–25%) were dissatisfied with the outcome of their surgery. Scott et al. (1) reported that dissatisfaction was also related to a low grade of radiographic OA, previous surgery, and obesity.
Randomized controlled trials (RCTs) provide the least biased information of the efficacy of surgical interventions (13). However, RCTs mostly assess effectiveness of interventions in ideal settings. Their ability to assess effectiveness of the whole clinical pathways is limited. Thus, there is an obvious need for valid observational (real-world) data on actual performance in routine settings (14).
The aim of our study was to assess the real-world effectiveness contemporary knee arthroplasty in patients aged 65 years or less. To achieve this goal, we conducted a prospective observational study with 2-year follow up. This study report outcomes measured comprehensively using various PROMs to provide information on the effect of knee arthroplasty on physical activity, ADL, QoL, pain, and satisfaction.
Materials and Methods
For this 2-year prospective cohort study, 250 patients were enrolled between 1 March 2012 and 30 October 2014 at our high-volume academic tertiary referral center. PROM data and other study questionnaires were collected preoperatively, at 2 to 3 months and at 1 year (10 to 14 months) and at 2 years (22 to 26 months) postoperatively.
All patients were treated in their local health centers by general practitioners before they referred the patients for consultation to our institution. The inclusion criteria were as follows: (1) age 65 years or less and (2) scheduled for either TKA or unicondylar knee arthroplasty (UKA). The exclusion criteria were as follows: (1) rheumatoid arthritis or other inflammatory diseases; (2) unwilling to provide informed consent; (3) physical, mental, or neurological conditions that could compromise the patient’s ability and compliance with postoperative rehabilitation and follow-up (e.g. drug or alcohol abuse, serious mental illness, and general neurological conditions such as Parkinson’s disease and multiple sclerosis); and (4) known sensitivity to materials in the devices.
A total of 373 recruitment letters were sent consecutively to patients of 65 years or less who were sent for consultation for knee arthroplasty, and the first 250 patients (272 knees) who returned written informed consent to participate were recruited on the study. As 5 (2%) patients canceled surgery, 6 (2.4%) were revised, 5 (2%) were lost to follow-up, and 2 (0.8%) died during the follow-up; 232 patients (93%; 254 knees) were available for the 2-year follow-up visits, and the analysis of the final results was based on these patients. If the patient had isolated antero-medial OA in the plain radiographs, then demiarthroplasty was considered. While simultaneous bilateral TKAs were performed for 22 patients, none of the patients received bilateral UKAs. The final patient population comprised 227 TKAs and 27 UKAs. Patient demographics are shown in Table 1.
Patient demographics.
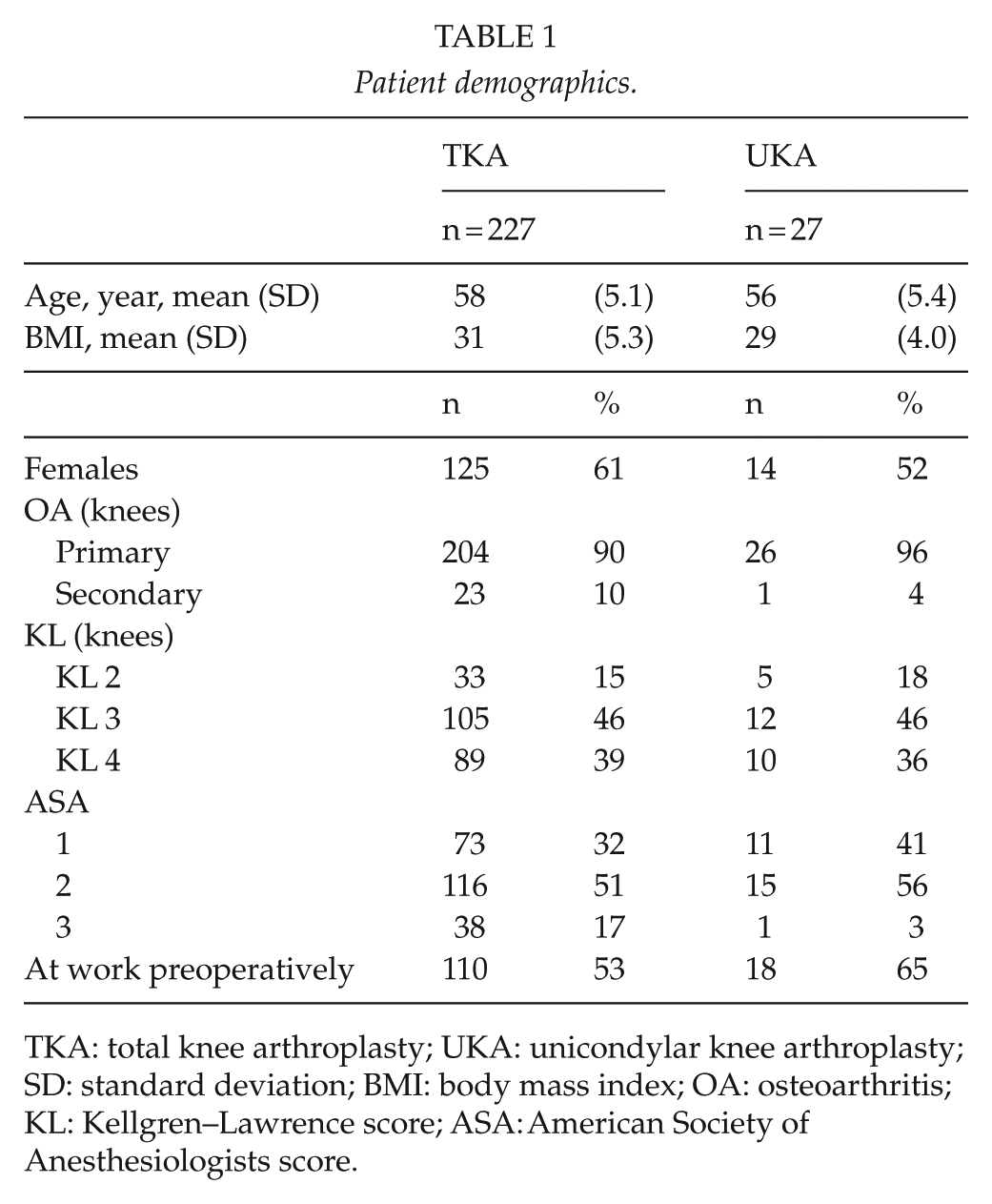
TKA: total knee arthroplasty; UKA: unicondylar knee arthroplasty; SD: standard deviation; BMI: body mass index; OA: osteoarthritis; KL: Kellgren–Lawrence score; ASA: American Society of Anesthesiologists score.
All operations were performed by senior orthopedic surgeons, and all patients were treated with the same routine postoperative rehabilitation and pain management protocol.
Of the 232 patients (254 knees), 227 knees (89%) underwent cemented TKA using either press-fit condylar (PFC; 182 knees; DePuy Synthes, Warsaw, IN, USA) or Nexgen (45 knees; Zimmer Biomet, Warsaw, IN, USA). In 12 (5.3%) of the TKAs, patella was resurfaced. Of the 227 TKAs, 218 (96%) were cruciate retaining (CR) and the rest 9 were posterior stabilized (PS). UKA was performed for 27 patients using the uncemented Oxford phase 3 (Zimmer Biomet) prosthesis.
Outcome Measures
Four different PROMs were used to measure the effectiveness of knee arthroplasty in these patients: Oxford Knee Score (OKS), Knee Injury and Osteoarthritis Outcome Score (KOOS), High-Activity Arthroplasty Score (HAAS), and the RAND-36 general QoL questionnaire. Primary outcome was defined as the effect of knee arthroplasty on pain and function as measured with OKS and KOOS. Secondary outcomes were as follows: the effect of knee arthroplasty on QoL (RAND-36), physical activity (HAAS), and satisfaction. A background questionnaire included information on working status and physical activities. The Visual Analog Scale (VAS) was measured with scale from 0 to 100 and it was used to evaluate pain and satisfaction caused by knee arthroplasty both before and after surgery. The VAS satisfaction scale was divided into four sections: 0 to 25, dissatisfied; 26 to 50, unsure; 51 to 75, satisfied; and 76 to 100, very satisfied as proposed previously by Scott et al. (1).
The severity of knee OA was assessed from preoperative standing fixed flexion view (FFV) radiographs using the Kellgren–Lawrence (KL) classification.
Questionnaires
The OKS score comprises 12 items regarding pain and ADL. Scores vary from 0 to 48, with 48 being the best possible score. The minimal clinically important difference (MCID) for the OKS score is 3 to 5 points.
KOOS comprises five subscales: pain, other symptoms, ADL, function in sport and recreation (sport/rec), and knee-related QoL. A normalized score (100 indicating no symptoms and 0 indicating maximal symptoms) is calculated for each subscale. The MCID is suggested to be 8 to 10.
The HAAS was specifically developed to assess the subtle variations in functional ability after lower limb arthroplasty with particular regard to highly active individuals. The score covers the four domains: walking, running, stair climbing, and general activities. Possible score ranges from 0 to 18 points. The MCID has not been defined for HAAS.
The RAND-36 comprises 36 items that assess eight health concepts. The Physical Component Scale (PCS) and the Mental Component Scale (MCS) are also derived from the eight RAND-36 scales. Scores range from 0 (lowest) to 100 (best). The MCID for the subscales is suggested to be 3 to 5 points.
Ethics
The study protocol (R11178) was approved by the Ethics Committee of our hospital district. The study was registered with ClinicalTrials.gov (NCT03233620). All patients gave written informed consent to participate in the study.
Statistical analysis
Data were presented as median with quartiles (Q1 to Q3) or as mean (SD) or (95% confidence interval (CI)). The Wilcoxon signed rank test and paired t-test for paired data were used to compare preoperative and postoperative values. The differences in distributions in the three measured time points were calculated with Friedman test. A p-value less than 0.05 was considered statistically significant. Data were analyzed using the SPSS (version 23) statistical package (IBM, Armonk, NY, USA.)
To prevent potential bias with TKA and UKA, the results were analyzed for both TKA and UKA together and also separately for TKA and UKA only (Table 2).
Patient-reported outcome measure (PROM) scores preoperatively and at 2 years analyzed separately for TKA (n = 227) and UKA (n = 27).
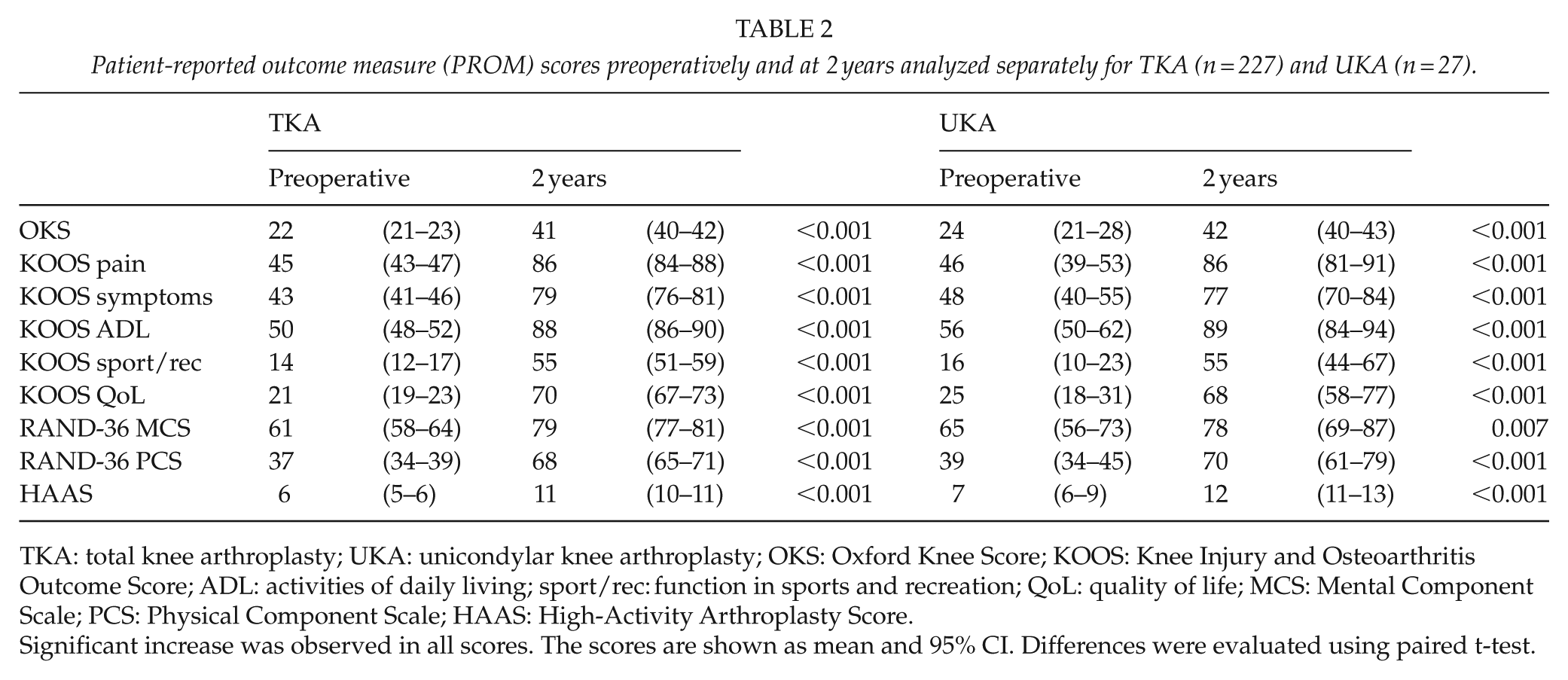
TKA: total knee arthroplasty; UKA: unicondylar knee arthroplasty; OKS: Oxford Knee Score; KOOS: Knee Injury and Osteoarthritis Outcome Score; ADL: activities of daily living; sport/rec: function in sports and recreation; QoL: quality of life; MCS: Mental Component Scale; PCS: Physical Component Scale; HAAS: High-Activity Arthroplasty Score.
Significant increase was observed in all scores. The scores are shown as mean and 95% CI. Differences were evaluated using paired t-test.
Results
Mean OKS increased both statistically (18 points, CI = 17–19, p < 0.001; TKA and UKA together) and clinically (exceeding MCID) significantly from the preoperative situation to the 2-year follow-up. The mean increase did not differ between TKAs and UKAs (Table 2).
Significant increase (p < 0.001) was also observed in all KOOS subscales, all of which also exceeded MCID. The mean increase in scores between preoperative and 2-year follow-up (TKA and UKA together) was as follows: KOOS pain 41 (CI = 39–43), KOOS symptoms 35 (CI = 32–37), KOOS ADL 37 (CI = 35–40), KOOS sport/rec 40 (CI = 37–44), and KOOS QoL 48 (CI = 45–51) (Table 2; Fig. 1).
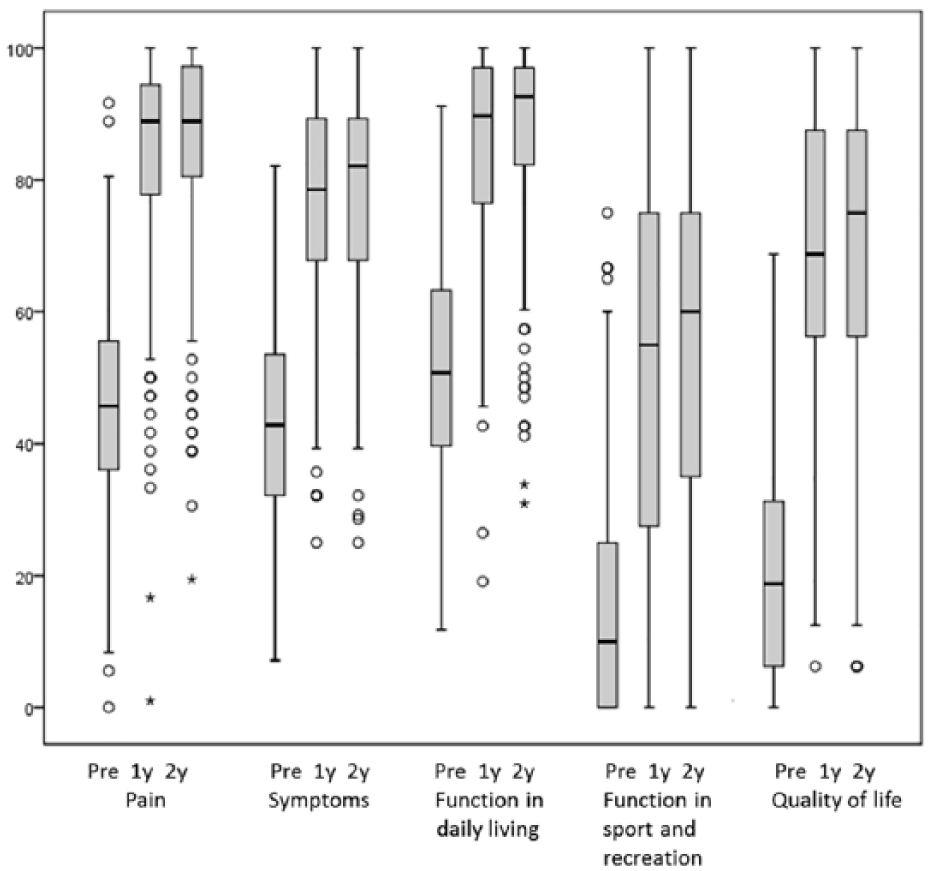
Outcome measured with KOOS subscales (n = 254). Scores presented as median (Q1 to Q3). All differences between the preoperative and 2-year results were significant (p < 0.001 for all comparisons). Differences were evaluated using Friedman test.
The preoperative baseline (mean) in physical activity according to HAAS was moderate: 6/18 in patients in the TKA group and 7/18 in the UKA group, respectively. The increase in mean HAAS (TKA and UKA together) was 5 points (CI = 4.6–5.5) over the 2-year follow up, and the improvement was significant (p < 0.001) (Table 2).
RAND-36 score was analyzed with mental (MCS) and physical (PCS) subscales. Over the 2-year follow up, the mean MCS (TKA and UKA together) increased 18 points (CI = 15–20) and the mean PCS 31 points (CI = 28–34). The change seen in both subscales was significant (p < 0.001) and also exceeded MCID (Table 2).
Pain relief was measured with the VAS (exercise and rest). A significant positive change of median value (in exercise: 80 (72,90) versus 13 (4,32), p < 0.001; in rest: 49 (26,71) versus 3 (0,7), p < 0.001) from the preoperative situation to the 2-year follow-up was detected (Fig. 2). In 16 (7%) patients, all of whom had undergone TKA, severe knee pain (VAS > 30) was still reported 2 years after knee arthroplasty.
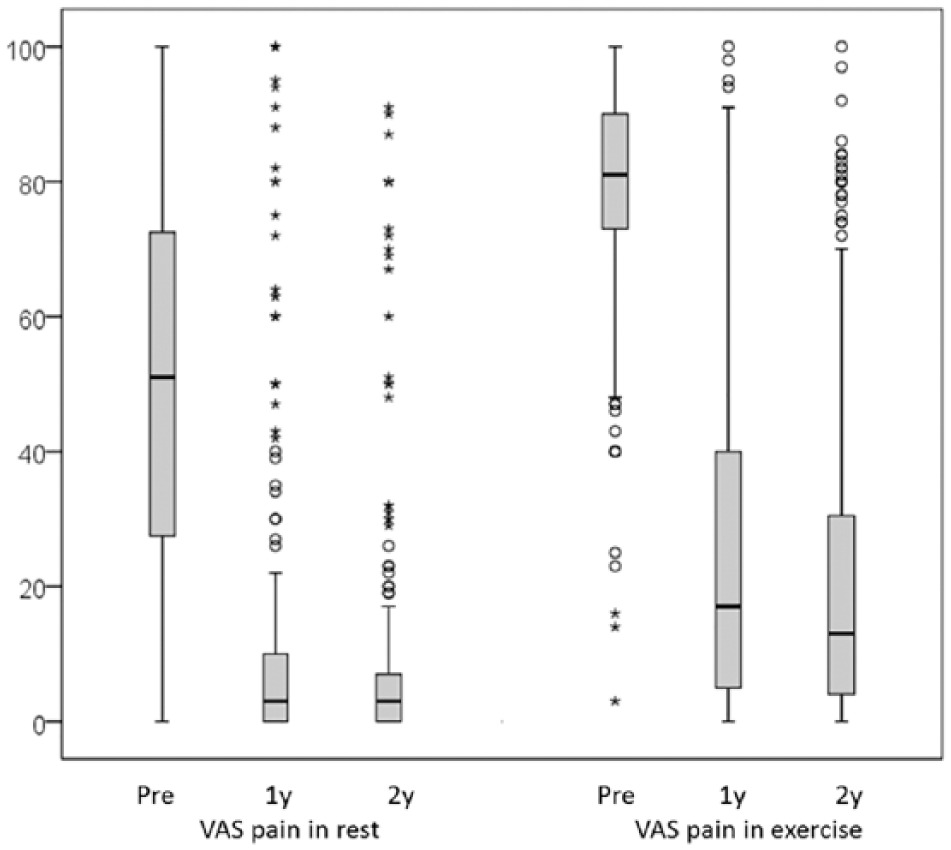
Pain in rest and exercise assessed with VAS scores (n = 254). Values presented as median (Q1 to Q3). All differences between the preoperative and 2-year results were significant (p < 0.001 for all comparisons). Differences were evaluated using Friedman test.
At the time of the 2-year follow-up visit, 85% of patients were either satisfied (9%) or very satisfied (76%) with the outcome of their knee arthroplasty. Between 1- and 2-year follow-up evaluations, 16 patients (6.7%), who had been either unsure or satisfied with the outcome at the 1-year visit, had become more satisfied by the 2-year follow-up evaluation. The number of patients who were dissatisfied with the outcome did not change between the 1- and 2-year follow-up evaluations (Table 3). At the 2-year follow-up visit, 98% of all patients reported that they would choose to undergo knee arthroplasty again, and 96% reported that they would recommend this operation to their best friend. Regarding satisfaction, there was no difference between patients in the UKA and TKA groups.
Satisfaction Visual Analog Scale (VAS) preoperatively, 1- and 2-year follow-ups.
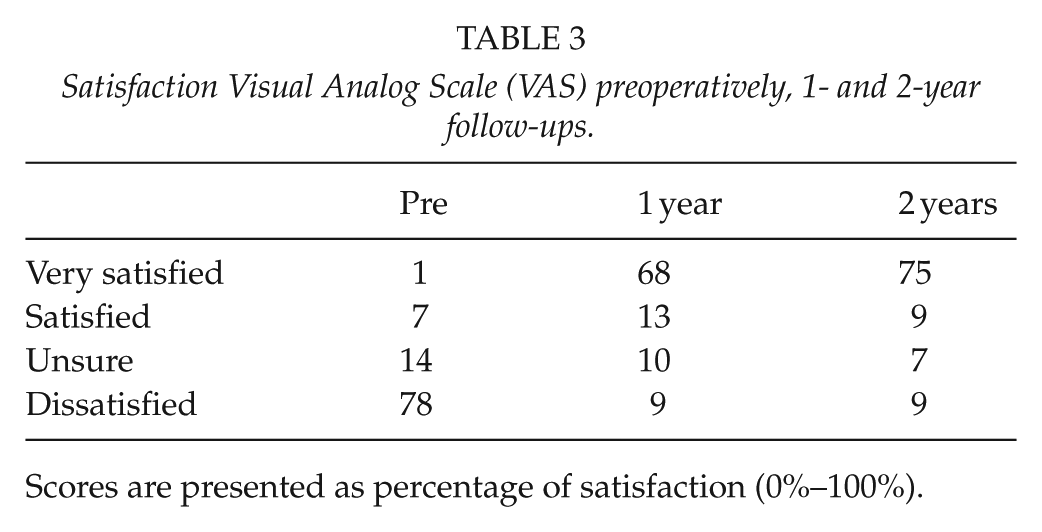
Scores are presented as percentage of satisfaction (0%–100%).
Preoperative KL-grade significantly affected both satisfaction and PROM outcomes measured at 2 years. The median VAS satisfaction was significantly poorer in patients with preoperative KL grade 2 OA compared to both patients with KL 3 (85 (51,97) versus 94 (80,100) points, p = 0.006) as well as those with KL 4 OA (85 (51,97) versus 91 (81,99) points, p = 0.015) at the time of the 2-year follow-up visit (Fig. 3). Furthermore, there was a significant difference in median OKS between the groups at the time of the 2-year follow-up visit: median OKS was worse in the KL 2 group than both in the KL 3 group (41 (36,44) versus 44 (38,46) points, p = 0.015) and in the KL 4 group (41 (36,44) versus 43 (40,45) points, p = 0.037). However, this difference fulfilled the MCID criteria only when the KL 2 and KL 3 groups were compared. Similarly, patients with KL 2 OA preoperative, ended up with significantly poorer median subscale scores than those patients with more advanced radiographic OA (KL 4) at the time of the 2-year follow-up visit: KOOS symptoms (75 (61,89) versus 86 (78,93), p = 0.001), KOOS ADL (88 (76,96) versus 93 (85,97), p = 0.041), and KOOS sport/rec (40 (25,75) versus 60 (38,75), p = 0.028). However, the significant improvements between preoperative and 2-year follow-up were observed in all PROMs and also in the KL 2 patients (p < 0.001).
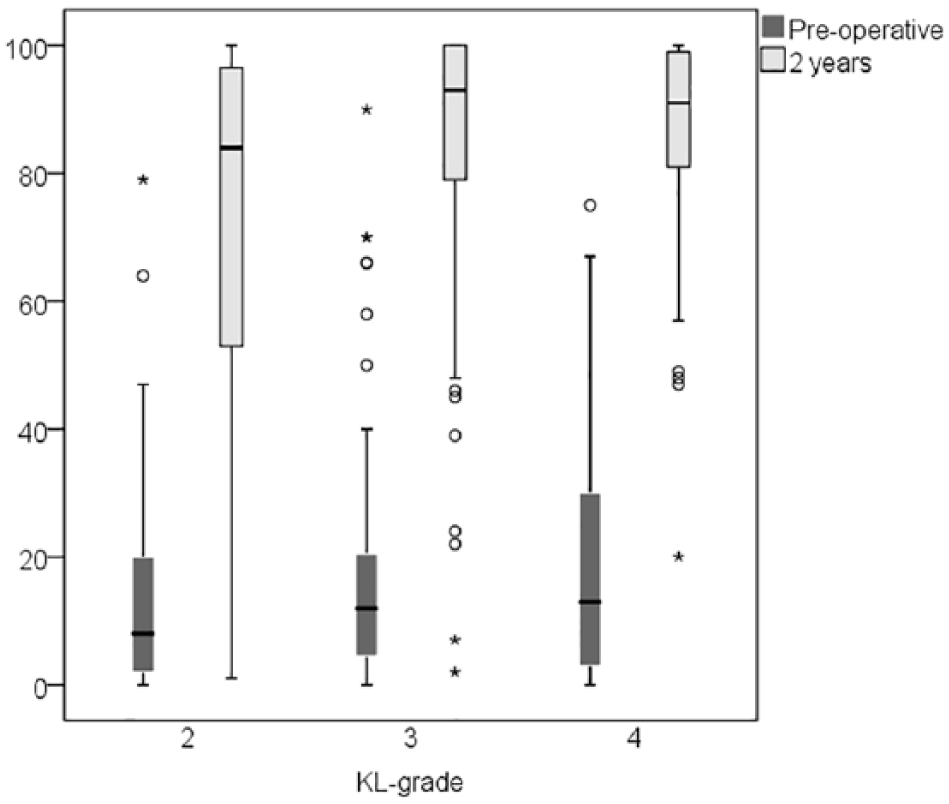
VAS satisfaction in different Kellgren–Lawrence groups (n = 254). Scores presented in median (Q1 to Q3). All differences between the preoperative and 2-year results were significant (p < 0.001 for all comparisons). Differences were evaluated using Wilcoxon signed rank test.
Revisions
Of the 254 knee replacements originally operated, 6 (2.4%; 4 TKAs and 2 UKAs) had to be revised during the 2-year follow-up period. Two patients in the TKA group underwent secondary patellar resurfacing because of persistent anterior knee pain, one TKA was revised for prosthetic joint infection, and one TKA for stiffness due to arthrofibrosis. Of the two UKAs that underwent revision surgery, one was revised for dislocation of the polyethylene insert and the other for impingement. Revised patients were excluded from the final outcome assessment.
Discussion
Earlier research on the success of knee arthroplasty has tended to focus on the survival of the implant. The functional outcome of knee arthroplasty has traditionally been measured using surgeon-driven clinical scores, such as the Knee Society Score (15–17). Recently, however, there has been an increasing demand for the subjective, patient-originated evaluation of the outcome (11). In practice, however, only a few such studies have been published so far (2, 11, 12). In this study, we utilized a wide set of PROMs to assess the real-world effectiveness of knee arthroplasty in a prospective non-selected cohort of patients undergoing TKA or UKA at our institution.
The increasing incidence of TKA also raises the question as to whether the financial resources invested in this treatment provide sufficient beneficial results in the face of the intensifying need for cost containment (9). Although we know that young age slightly increases the risk of revision, implant survival has been shown to be acceptable also in younger patients. Therefore, TKA is also a viable option for the treatment of end-stage OA in this patient population (18). Younger patients form a specific group with longer life time expectancy and also often with high demands for the outcome of surgery (19). In this study, we found that patients aged 65 years or less benefited significantly from knee arthroplasty in terms of pain relief, as well as in terms of improved physical activity and QoL. However, the total disappearance of knee symptoms was rare.
There have been earlier studies on functional gain following TKA in young patients but these have lacked true prospective follow up. These studies have used the upper age limits of 50 (11) or 55 (1) years of age. In everyday clinical practice, however, these subgroups are marginal. Instead, the rising incidence of TKA has occurred especially in patients aged 50 to 59 years (20), which is among the target group of our study. In our study, 85% of patients were satisfied or very satisfied with the outcome at 2 years postoperatively, and an even higher proportion of patients (98%) reported a willingness to undergo knee arthroplasty again. In other recent studies, the subgroups who are dissatisfied with their surgery have been reported to range from 10% to 20% (1, 2, 11). In this respect, knee arthroplasty is clearly inferior to total hip arthroplasty, and the topic of dissatisfied knee arthroplasty patients clearly needs further research. Previous studies have shown that persistent pain after knee arthroplasty is strongly associated with psychological aspects and young age (21, 22). In our study, knee arthroplasty resulted in significant pain relief, and most of this effect was seen already during the first postoperative year. Moreover, between 1 and 2 years postoperative, the number of patients with persistent knee pain continued to decrease (Fig. 2). Thus, some patients experienced a clearly delayed recovery, but the small subgroup (7%) of patients who reported severe knee pain persisted at the time of the 2-year follow-up.
Scott el al. (1) divided the satisfaction scale into four categories: very satisfied, satisfied, dissatisfied, and as the fourth group they included those patients who were unsure about their satisfaction. We found that a small proportion of patients who were “unsure” at the time of the 1-year follow-up reported being satisfied at the time of the 2-year follow-up (7 patients, 2.9%). Thus, in some patients, complete recovery after knee arthroplasty may take up to 2 years. Dissatisfied patients, however, still held the same view at the time of the 2-year follow-up. Satisfaction is clearly a multidimensional experience, as 98% of patients reported being willing to undergo knee arthroplasty again despite the fact that 15% of patients were dissatisfied or unsure with the outcome of their surgery. The patient’s own perspective of the preoperative symptoms and functional disability may partly explain this difference, that is, they may still have considered the outcome of knee arthroplasty to be better than the preoperative situation despite their residual knee symptoms. The proportion of patients in our study who were satisfied with the outcome was in accordance with other recent studies on the subject (23–25).
Scott et al. (1) reported high (59%) dissatisfaction rate of TKA in patients with KL 1–2 grade OA preoperatively. Also, in our study, satisfaction at 2 years was significantly lower in the KL 2 group, both when compared to the KL 3 and the KL 4 groups. Significant improvement, however, was achieved in all KL subgroups as compared to the preoperative situation (Fig. 3). As there was no difference in KOOS pain subscale between the KL subgroups at 2 years, it seems that despite their higher dissatisfaction rate, also patients with milder OA (KL 2) achieved good pain relief. In patients with mild radiographic knee OA, there may be other factors than pain, such as depression or catastrophizing behavior, that would explain higher dissatisfaction rates despite good pain relief achieved with surgery.
The clinically significant improvement in physical activity in these younger knee arthroplasty patients is an important finding. Young patients may be self-evidently considered physically active. This may restrict their access to knee arthroplasty because of the fear of compromised implant survival. A recent study by Keeney et al. (26) showed that preoperatively there was no difference in physical activity levels between younger (55 years or less) and older patients (65 to 75 years), and that physical activity increased in both groups after knee arthroplasty. In our study, only 42 (17%) patients reported a preoperative activity level of over 50% according to the HAAS scale. Respectively, the preoperative physical activity level points were less than 50% when also measured with the KOOS (93% of patients) and 36-Item Short Form Health Survey (SF-36; 76% of patients) subscales (Table 2). However, significant improvement was seen postoperatively in physical activity in the HAAS as well as in the KOOS and SF-36 physical activity subscales. Thus, the ability to exercise can also be improved with knee arthroplasty in younger patients. To the best of our knowledge, our study is the first to assess the effect of knee arthroplasty on patient activity levels using a specific activity score in a prospective observational (real-world) study.
Scott et al. (27) reported that patients undergoing TKA consider climbing stairs, ability to walk, and kneeling to be especially important activities in their daily living. Because the preoperative physical activity of patients undergoing TKA has been shown to be low, more demanding activities, such as cycling or carrying heavy objects, have not been so important for them (28). In the working-age population, functions related to daily living are associated with working capability. In our study, 104 (45%) patients were retired or about to retire preoperatively. Of the128 (55%) patients who were working preoperatively, a high proportion (89%) returned to work during the 2-year follow-up, and significant improvements in scores related to daily living supported this finding (Table 2).
Changes in QoL are based on both physical and mental improvements and are also related to pain relief. Even if physical scores improved more distinctly, it is notable that mental scores also improved significantly after knee arthroplasty. The Mental Component Score (MCS) of RAND-36 showed comparable improvement with the Physical Component Score (PCS) of RAND-36, emphasizing comprehensive improvement in outcomes (Table 2). Recently, Goh et al. (11) also reported significant albeit slightly smaller improvements in these scores than the scores we found in this study (PCS 16.9 versus 31.5 and MCS 4.4 versus 17.5).
We recruited younger patients with knee OA who were scheduled for knee arthroplasty at our institution. Our study was an observational intervention study with the focus on effectiveness, and the study setup mirrored everyday clinical practice. This setup has previously been applied only by Klit et al. (12), who conducted a prospective cohort study among patients aged less than 60 years. The difference between the study by Klit et al. and our study was that we included both patients who were listed for TKA and those who were scheduled for UKA. Furthermore, we applied a specific activity score (HAAS) to assess the effect of knee arthroplasty on patient activity levels. In our setup, UKA and TKA yielded similar results. Thus, the theoretical advantages of UKA over TKA (29) did not result in either better clinical outcome in any of the PROMs used or higher satisfaction. This finding warrants further research, and future work should compare the outcome and effectiveness of UKAs and TKAs in RCTs.
Our study is not without limitations. We did not have a specific control group of patients above the age of 65 years which would have enabled the comparison of our results with the older patient population. The UKA group was also markedly smaller than the TKA group. The obvious strength of this study was the evaluation of the outcome using multiple PROM data that have not been included in previous studies, a non-selected real-world cohort of patients, and also the fact that only a very small proportion (7%) of patients was lost to follow-up during the 2-year study period. Our study is also the first to evaluate the real-world effectiveness of TKA and UKA in younger patients utilizing a wide set of PROMs. To the best of our knowledge, our study is the first to assess both actual patient satisfaction and also their willingness to undergo the same surgery again. This approach showed that satisfaction is clearly a multidimensional issue that may not be adequately assessed with a single question about satisfaction.
Conclusion
We found that knee arthroplasty provided patients aged 65 years or less with clinically significant pain relief as well as improvement in ADL and QoL. The patients’ physical activity was low or moderate preoperatively, but improved significantly during the 2-year follow-up. Some pain and functional deficiencies remained after knee arthroplasty, and this should be emphasized in the preoperative guidance given to patients who are considering or scheduled for such surgery. Mild radiographic OA preoperatively is a clear risk factor for patient dissatisfaction with the outcome of knee arthroplasty. Future research is warranted to clarify the preoperative risk factors for severe residual symptoms and dissatisfaction after knee arthroplasty.
Footnotes
Acknowledgements
Peter Heath contributed to language revision; M.N. and A.E. designed the study; H.H. and M.N. analyzed the data and calculated statistics; M.N. prepared the manuscript; and T.M. and A.E. reviewed the results. All authors revised and approved the final manuscript.
Declaration of Conflicting Interests
M.N., T.M., and H.H. have no conflicting interests. A.E. has received research grant (Zimmer Biomet) and lecture fee (DePuy).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from the Finnish Arthroplasty Association and the Finnish Orthopedic Association.
Ethical Approval
The study protocol (R11178) was approved by the Ethics Committee of Pirkanmaa Hospital District.
Informed Consent
All patients gave written informed consent to participate in the study.
Trail Registration
The study was registered with ClinicalTrials.gov (NCT03233620).